
Evaluating Induction-Salvage Treatment Regimes in Therapy of AML/MDS

Acute Myeloid Leukemia
Allo HSCT after Low Toxicity CDT A step toward individualized allogeneic
immunotherapy?
Didier Blaise, MDInstitut Paoli Calmettes,
CRCM and Aix Marseille University
Marseille, France
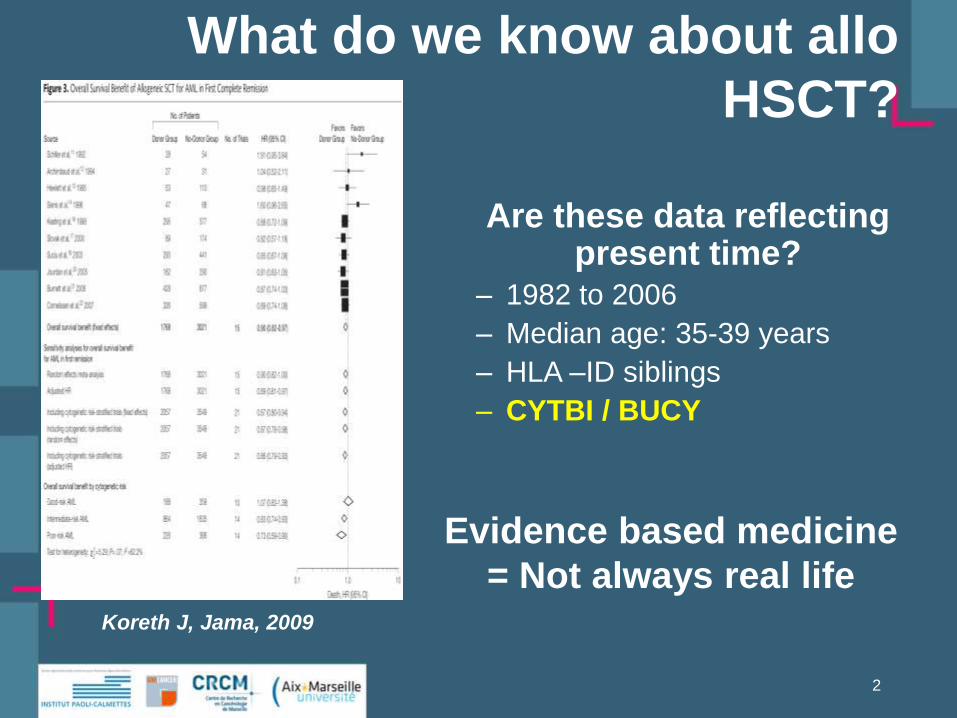
What do we know about allo
HSCT?
2
Koreth J, Jama, 2009
Are these data reflecting present time?
– 1982 to 2006
– Median age: 35-39 years
– HLA –ID siblings
– CYTBI / BUCY
Evidence based medicine
= Not always real life

Donor
T Cell
Donor
mononuclear cell
Host cells
Conditioning regimenDiseaseEndotoxin
IL2
IFN G
IL1
TNF@
IL1
TNF@
CDT is a major factor for
Mortality
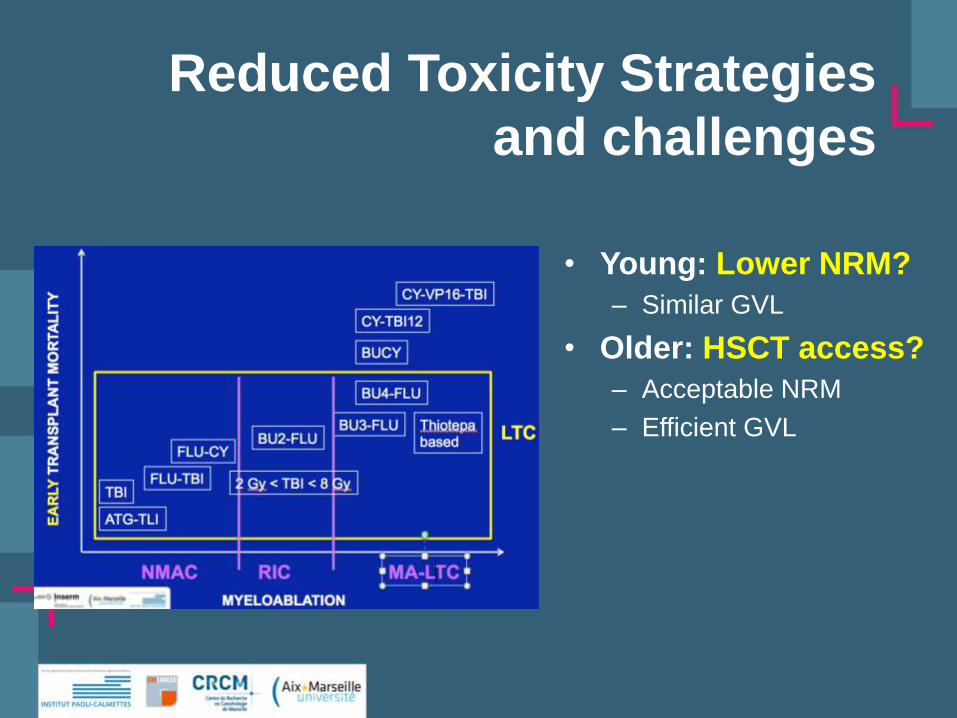
Reduced Toxicity Strategies
and challenges
• Young: Lower NRM?
– Similar GVL
• Older: HSCT access?
– Acceptable NRM
– Efficient GVL

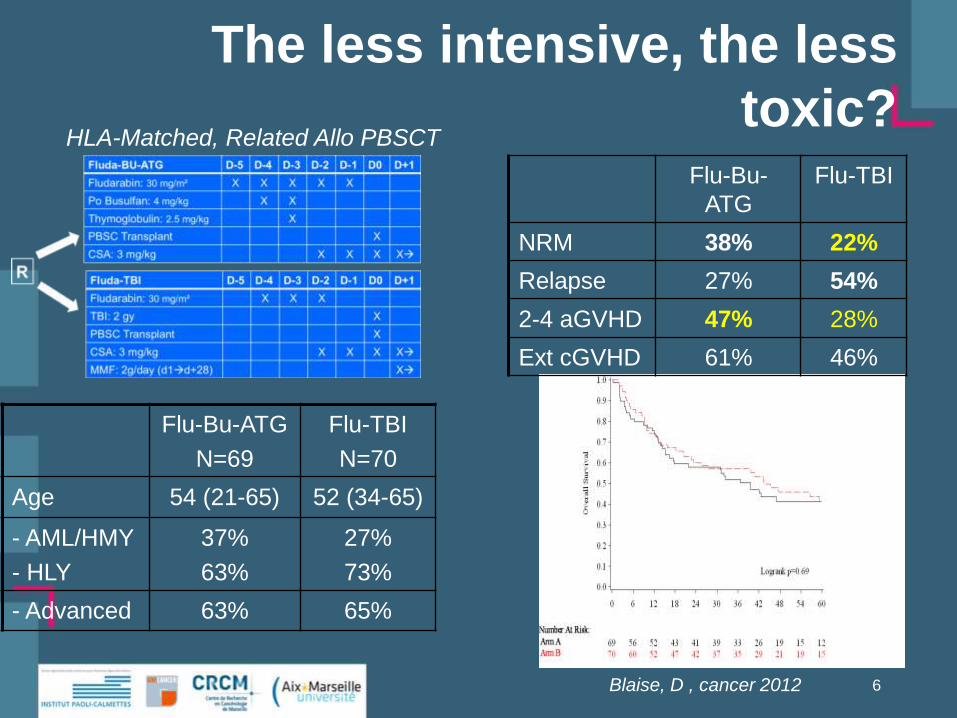
The less intensive, the less
toxic?
Flu-Bu-ATG
N=69
Flu-TBI
N=70
Age 54 (21-65) 52 (34-65)
- AML/HMY
- HLY
37%
63%
27%
73%
- Advanced 63% 65%
Blaise, D , cancer 2012
Flu-Bu-
ATG
Flu-TBI
NRM 38% 22%
Relapse 27% 54%
5
HLA-Matched, Related Allo PBSCT
The less intensive, the less
toxic?
Flu-Bu-ATG
N=69
Flu-TBI
N=70
Age 54 (21-65) 52 (34-65)
- AML/HMY
- HLY
37%
63%
27%
73%
- Advanced 63% 65%
Blaise, D , cancer 2012
Flu-Bu-
ATG
Flu-TBI
NRM 38% 22%
Relapse 27% 54%
2-4 aGVHD 47% 28%
Ext cGVHD 61% 46%
6
HLA-Matched, Related Allo PBSCT

GVHD remains a major cause of
death after RIC
No
n R
ela
pse M
ort
ali
ty
7
p=0.003
17%
31%
41%
12%
Saillard C, Leuk & Lymphoma, 2014

Dose Intensity and Toxicity
• DI is not the only cause of toxicity
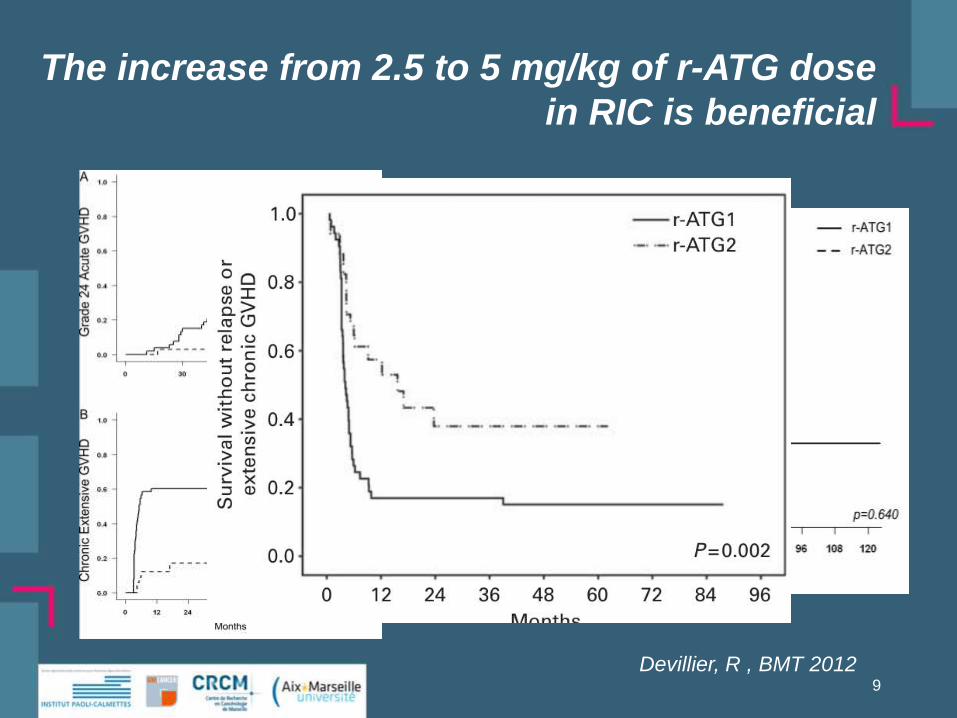
The increase from 2.5 to 5 mg/kg of r-ATG dose
in RIC is beneficial
Devillier, R , BMT 20129
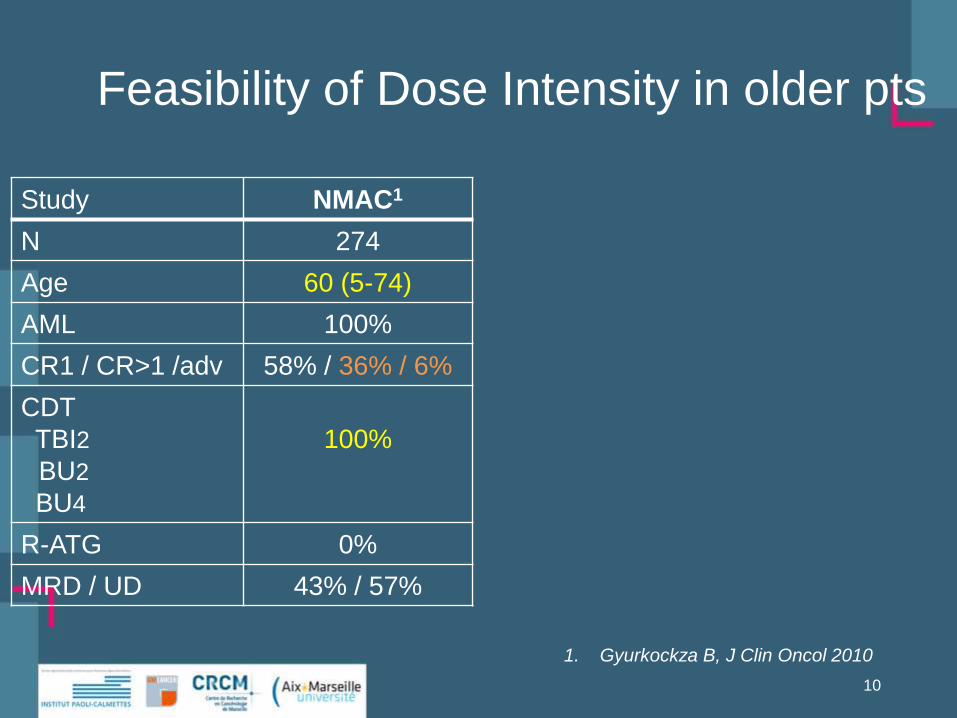
Study NMAC1
N 274
Age 60 (5-74)
AML 100%
CR1 / CR>1 /adv 58% / 36% / 6%
CDT
TBI2
BU2
BU4
100%
R-ATG 0%
MRD / UD 43% / 57%
10
Feasibility of Dose Intensity in older pts
1. Gyurkockza B, J Clin Oncol 2010
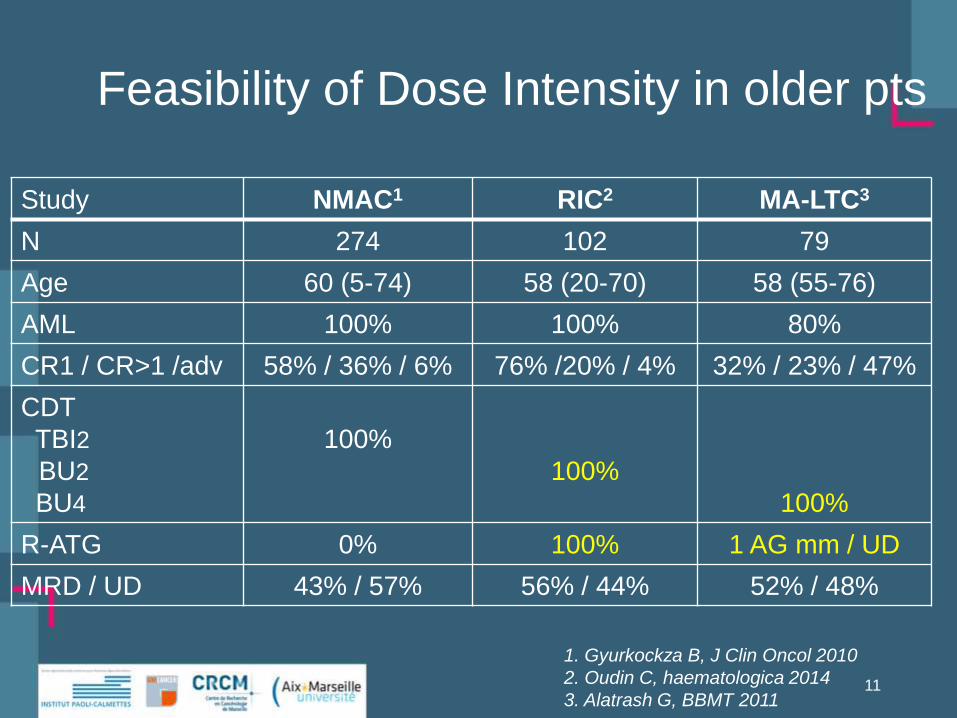
Study NMAC1 RIC2 MA-LTC3
N 274 102 79
Age 60 (5-74) 58 (20-70) 58 (55-76)
AML 100% 100% 80%
CR1 / CR>1 /adv 58% / 36% / 6% 76% /20% / 4% 32% / 23% / 47%
CDT
TBI2
BU2
BU4
100%
100%
100%
R-ATG 0% 100% 1 AG mm / UD
MRD / UD 43% / 57% 56% / 44% 52% / 48%
11
Feasibility of Dose Intensity in older pts
1. Gyurkockza B, J Clin Oncol 2010
2. Oudin C, haematologica 2014
3. Alatrash G, BBMT 2011

Study NMAC1 RIC2 MA-LTC3
N 274 102 79
Graft Failure 12 0 0
100 days NRM 4% 5% 5%
Overall NRM 26% 24% 26%
12
Feasibility of Dose Intensity in older pts
1. Gyurkockza B, J Clin Oncol 2010
2. Oudin C, haematologica 2014
3. Alatrash G, BBMT 2011

Dose Intensity and Toxicity
• DI is not the only cause of toxicity
• DI is not always associated with toxicity

CR1 AML
NMAC
N=160
RIC
N=78
MA-RTC
N= 25
14
Importance of Dose Intensity in Disease
Control?

The less intensive, the less
toxic?
Flu-Bu-ATG
N=69
Flu-TBI
N=70
Age 54 (21-65) 52 (34-65)
- AML/HMY
- HLY
37%
63%
27%
73%
- Advanced 63% 65%
Blaise, D , cancer 2012
Flu-Bu-
ATG
Flu-TBI
NRM 38% 22%
Relapse 27% 54%
2-4 aGVHD 47% 28%
Ext cGVHD 61% 46%
15
HLA-Matched, Related Allo PBSCT
Dose Intensity and Toxicity
• DI is not the only cause of toxicity
• DI is not always associated with toxicity
• DI may contribute controlling disease
17
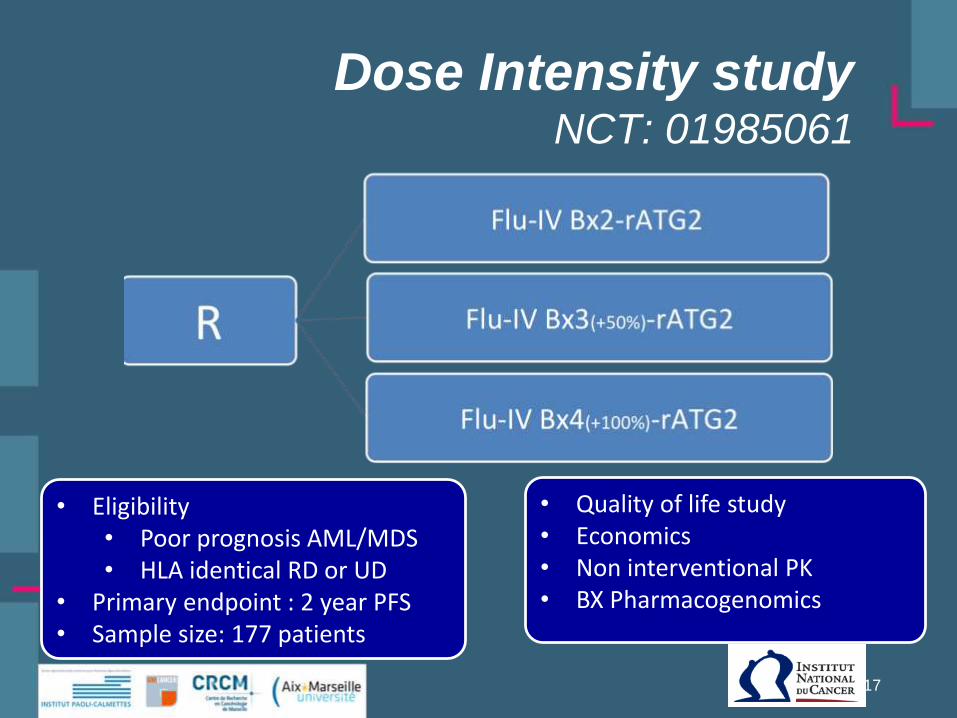
• Eligibility• Poor prognosis AML/MDS• HLA identical RD or UD
• Primary endpoint : 2 year PFS• Sample size: 177 patients
• Quality of life study• Economics• Non interventional PK• BX Pharmacogenomics
Dose Intensity studyNCT: 01985061
Conclusions• Toxicity was (is) a major issue
– Low post-transplant toxicity is achievable• It is critical for some populations: Older/unfit patients
• CDT is an important adjustment variable
– Low toxicity does not mean only reduced intensity
• Disease control is the major issue– Low toxicity is not NO toxicity
• Still some work to do...
– Intensive CDT with low toxicity is achievable• Individualized CDT may be critical for better disease control
– Optimized CDT may not be sufficient to cure some diseases
• Post transplant therapy?
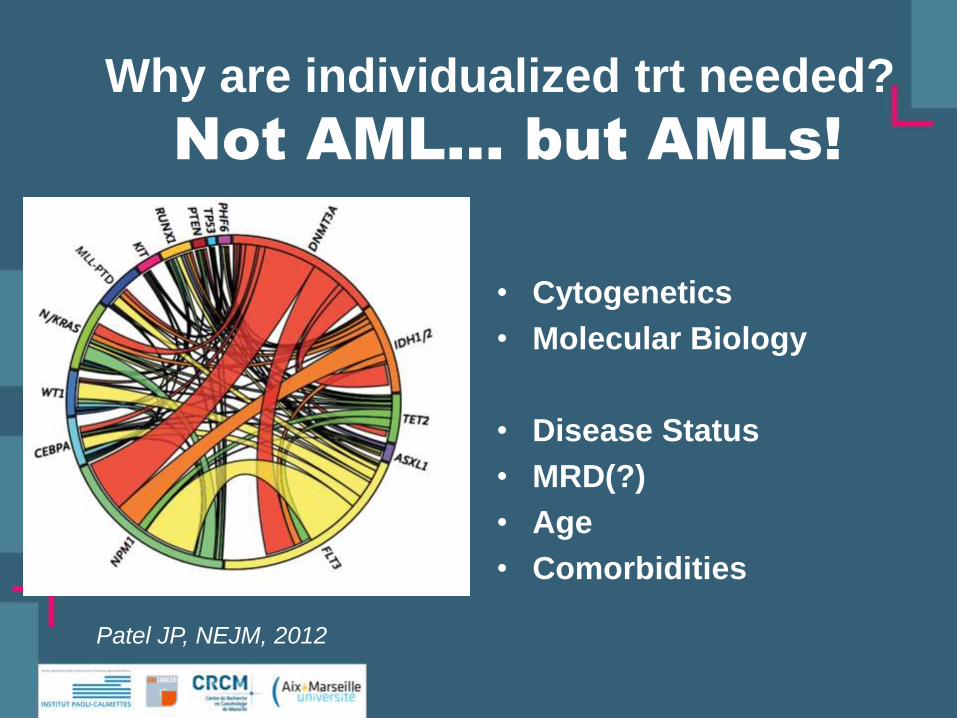
Why are individualized trt needed?
Patel JP, NEJM, 2012
• Cytogenetics
• Molecular Biology
• Disease Status
• MRD(?)
• Age
• Comorbidities
Not AML… but AMLs!

Risk changes with accurate
assessment
Intermediate Risk?
Patel JP, NEJM, 2012
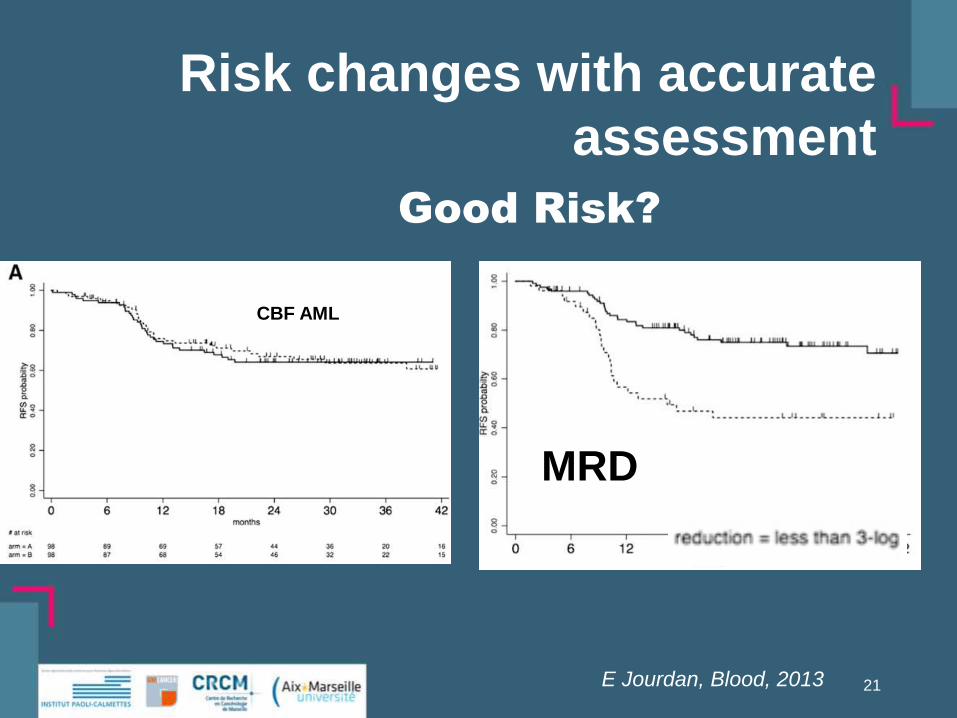
Risk changes with accurate
assessment
E Jourdan, Blood, 2013 21
MRD
CBF AML
Good Risk?

5-year relative survival rates
with respect to age in patients
with AML1
5-y
ea
r s
urv
iva
l ra
te
0
10
20
30
40
50
60
Age, years
<45 45–54 65+55–64
1. Howlader N, et al (eds). SEER Cancer Statistics Review, 2010
2. Appelbaum FR et al, Hematology Am Soc Hematol Educ,2001
OS in patients aged >55 years
(ECOG data from 1973–1997)2
Outcome of AML in the elderly
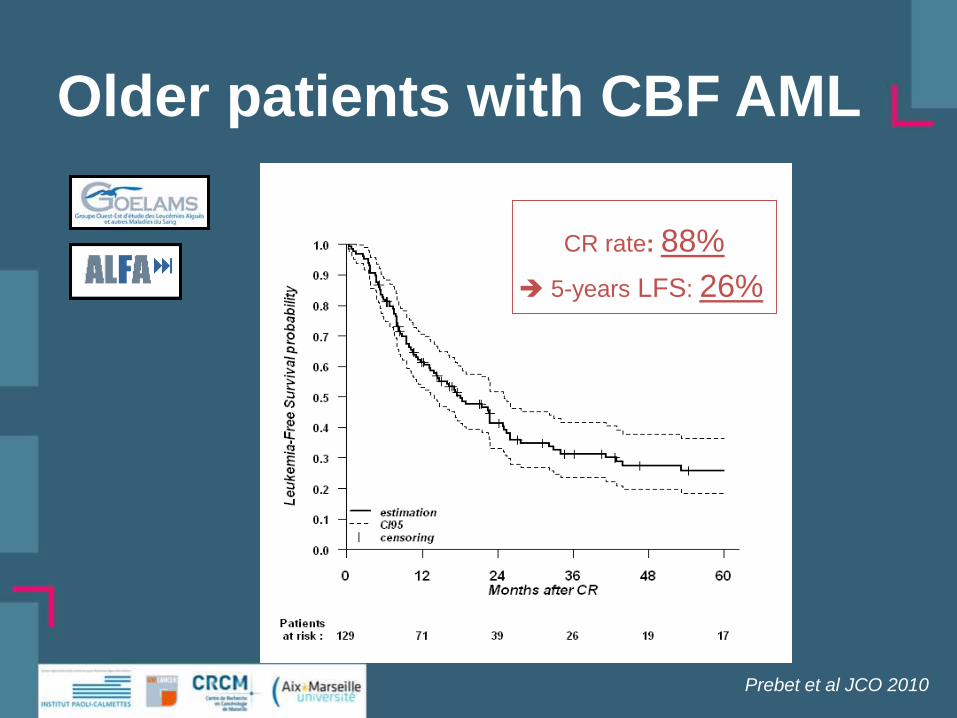
Older patients with CBF AML
5-years LFS: 26%
CR rate: 88%
Prebet et al JCO 2010

Not AML… but AMLs…
and different patients…
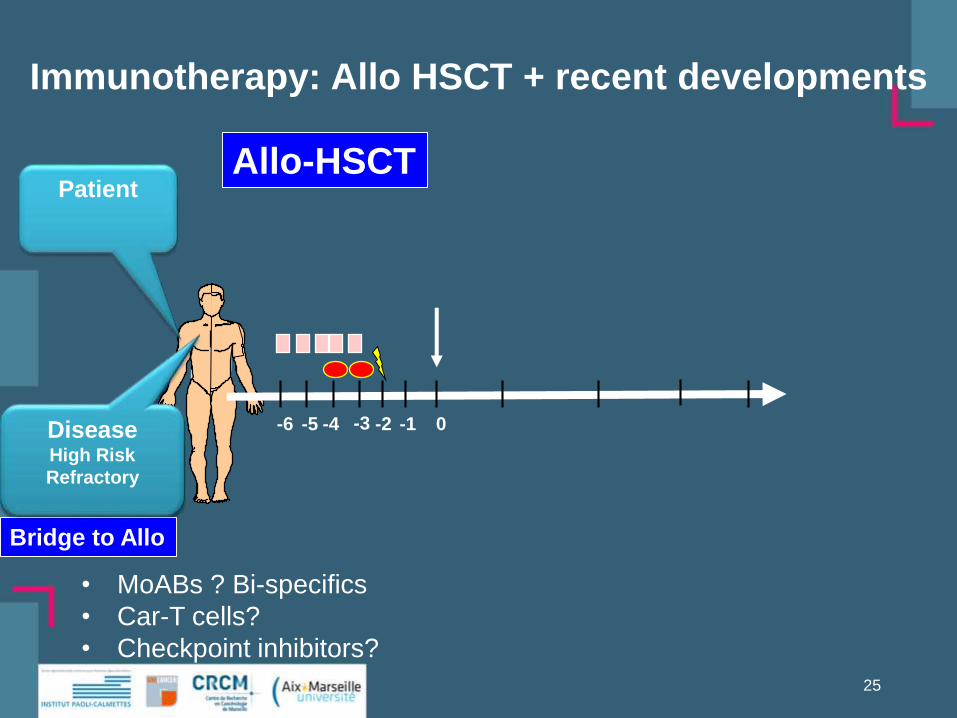
Patient
-3 -2 -1-4-6 -5 0
Immunotherapy: Allo HSCT + recent developments
25
DiseaseHigh Risk
Allo-HSCT
Bridge to Allo
DiseaseHigh Risk
Refractory
• MoABs ? Bi-specifics
• Car-T cells?
• Checkpoint inhibitors?

DonorIndividualized
Conditioning
PatientAge
Comorbidities
-3 -2 -1-4-6 -5 0
26
GVHD prophylaxis
DiseaseStage
Prognostic
Factors
MRD
Allo-HSCT
HLA match vs Alternative DNMAC/RIC vs. MA-RTC
No Post-Graft IS
Long vs. short term
In-vivo T-cell depletBridge to Allo
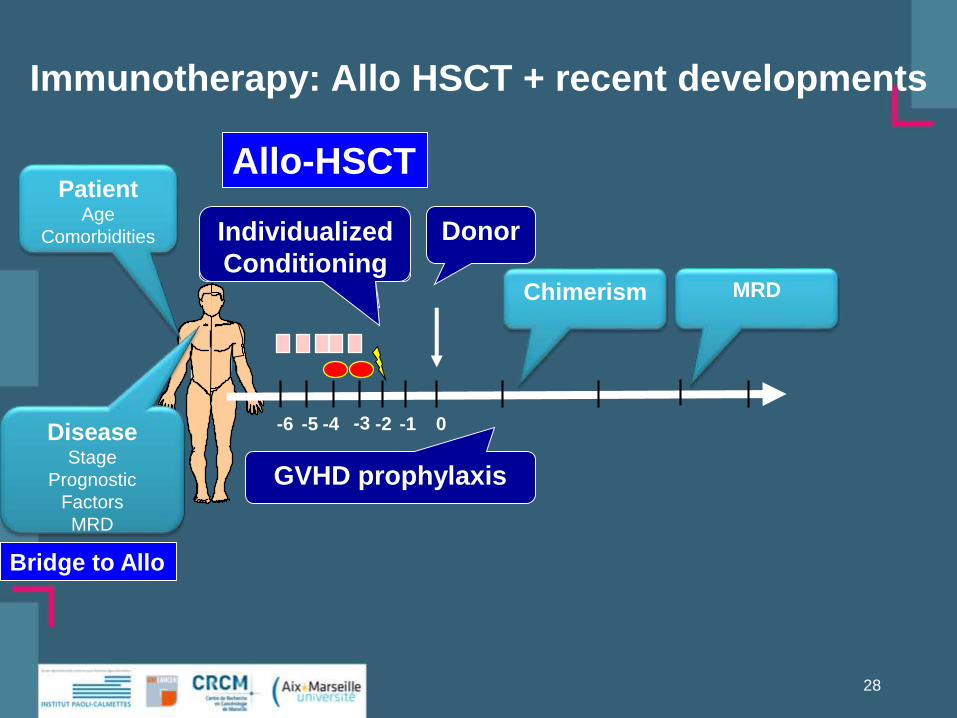
Immunotherapy: Allo HSCT + recent developments

DonorIndividualized
Conditioning
PatientAge
Comorbidities
-3 -2 -1-4-6 -5 0
27
GVHD prophylaxis
Allo-HSCT
Chimerism
DiseaseStage
Prognostic
Factors
MRD
Rela
pse
Immunotherapy: Allo HSCT + recent developments
Bridge to Allo
DonorConditioning
PatientAge
Comorbidities
-3 -2 -1-4-6 -5 0
28
GVHD prophylaxis
Allo-HSCT
Chimerism MRD
DiseaseStage
Prognostic
Factors
MRD
Immunotherapy: Allo HSCT + recent developments
Bridge to Allo
Individualized
Conditioning
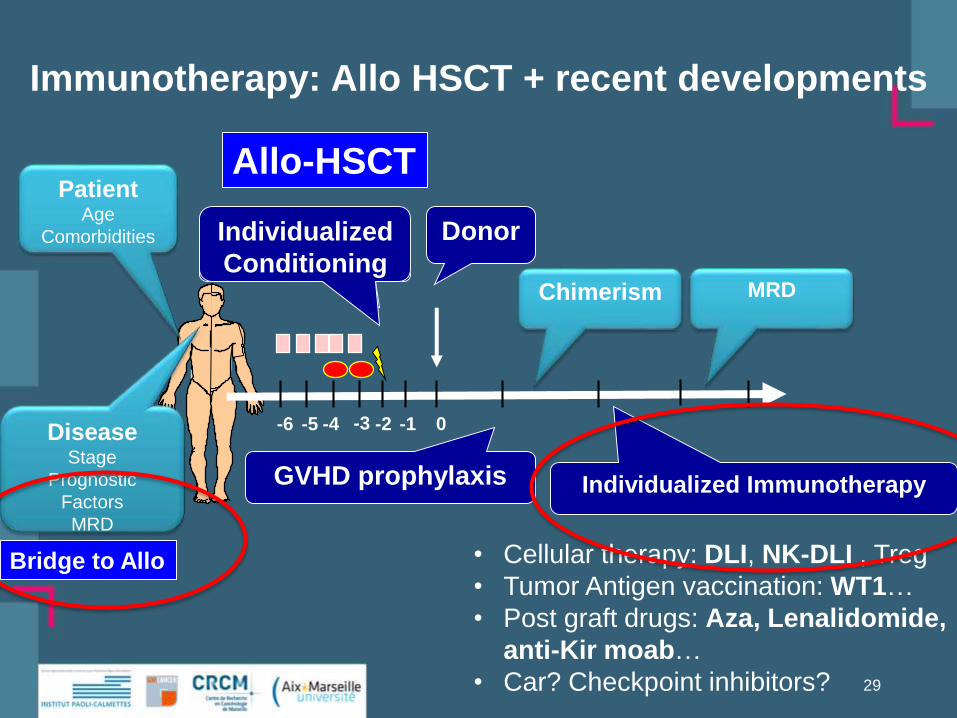
DonorConditioning
PatientAge
Comorbidities
-3 -2 -1-4-6 -5 0
29
GVHD prophylaxis
Chimerism
Individualized Immunotherapy
• Cellular therapy: DLI, NK-DLI , Treg
• Tumor Antigen vaccination: WT1…
• Post graft drugs: Aza, Lenalidomide,
anti-Kir moab…
• Car? Checkpoint inhibitors?
MRD
Allo-HSCT
DiseaseStage
Prognostic
Factors
MRD
Immunotherapy: Allo HSCT + recent developments
Bridge to Allo
Individualized
Conditioning

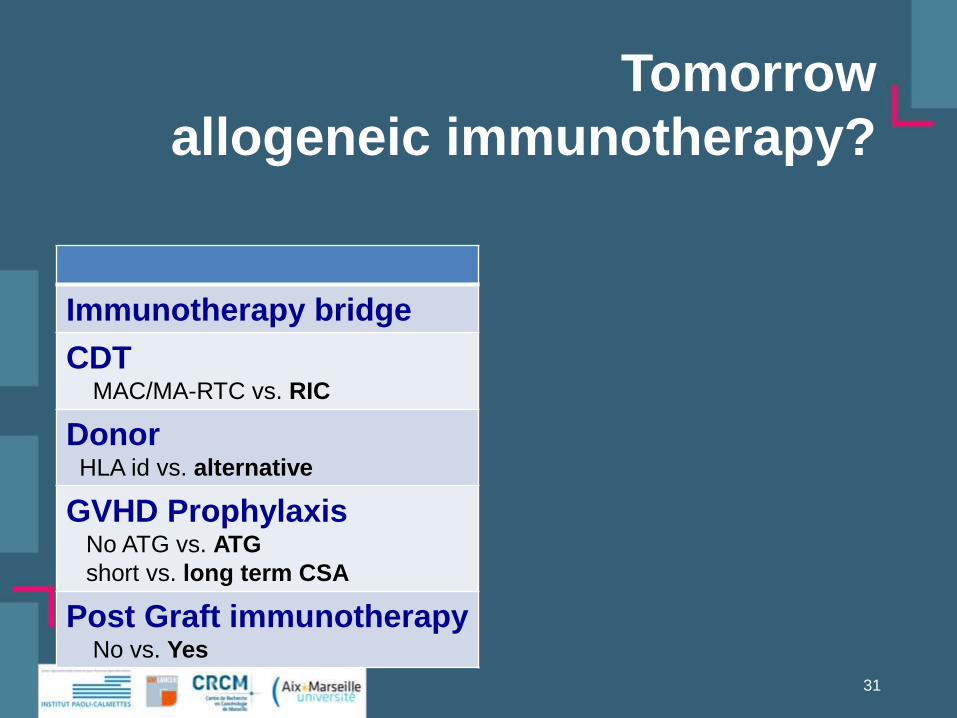
Tomorrow
allogeneic immunotherapy?
Immunotherapy bridge
CDTMAC/MA-RTC vs. RIC
DonorHLA id vs. alternative
GVHD ProphylaxisNo ATG vs. ATG
short vs. long term CSA
Post Graft immunotherapyNo vs. Yes
31

SR CR1
Immunotherapy bridge
CDTMAC/MA-RTC vs. RIC
+++
DonorHLA id vs. alternative
+
GVHD ProphylaxisNo ATG vs. ATG
short vs. long term CSA
++++
Post Graft immunotherapyNo vs. Yes
+
32
Tomorrow
allogeneic immunotherapy?
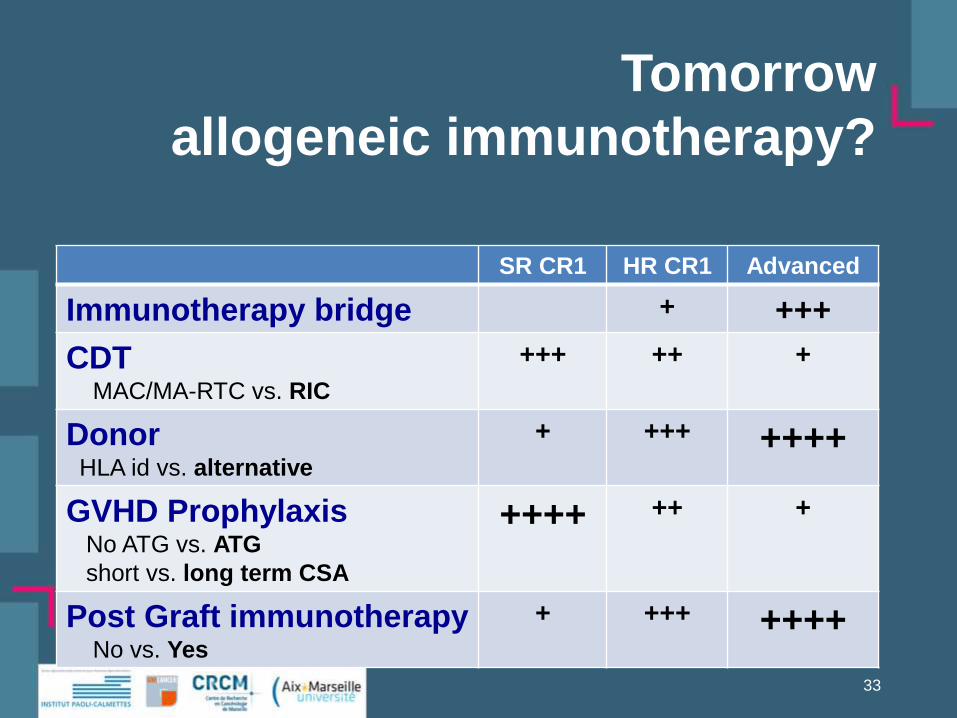
Tomorrow
allogeneic immunotherapy?
SR CR1 HR CR1 Advanced
Immunotherapy bridge + +++
CDTMAC/MA-RTC vs. RIC
+++ ++ +
DonorHLA id vs. alternative
+ +++ ++++
GVHD ProphylaxisNo ATG vs. ATG
short vs. long term CSA
++++ ++ +
Post Graft immunotherapyNo vs. Yes
+ +++ ++++
33
Conclusions
• Allogeneic Immunotherapy is an effective
therapy for AL
• What is essential ?
– Not what has been done so far…
– But what we yet have to do!
34
Ollie,
So much to do…Keep going!
Stan

35












![Risk-adapted therapy of AML in younger adultsSolalettura].pdf · Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010.](https://static.fdocuments.in/doc/165x107/5e2962bb73f8a5419b612bcd/risk-adapted-therapy-of-aml-in-younger-solaletturapdf-risk-adapted-therapy-of.jpg)


