Amis - tips and tricks
41
AMIS surgical technique tips and tricks SD Koutsostathis
-
Upload
stefanos-koutsostathis -
Category
Healthcare
-
view
72 -
download
0
Transcript of Amis - tips and tricks

AMISsurgical technique
tips and tricks
SD Koutsostathis

MISDefinition
Minimally Invasive Surgery
NOT
Mini Incision Surgery

Training
Learning center
Visit reference centers
Cadaver labs
Expert assistance
Requirements in new techniques

Pre-op planning

Installation
Traction table. Correct positioning

Installation
Anatomic landmarks

Anterior Minimally Invasive Surgery


Rectus femoris
DB LCFA

Approach
Calcar
Iliocapsularis
Gluteus minimus

Break posterior
cortex

RECTUS FEMORIS
CAPSULE

I-I line (depth)Orientation


Parallel to TAL


GT Calcar
Pyriformis




Planning of head-neck length is possible


FAST CLOSURE

?• Is it an evolution?
• Is it safe?
• Is it better for the patient?
OR
• Commercial trick?
• Industry promoted technique?
• Role of media – internet?

different
benefit
profile
different
risks
different
intervals
different
approaches
!!

AMIS® technique - Advantages
• Shorter stays in the hospital.
• Shorter rehabilitation.
• Reduced risk of dislocation.
• Immediate post-operative muscle
tone preservation.
• Decreased post-operative pain.
• Less blood loss.
• Faster return to daily activities.
• Reduction of scar tissues.

Direct Anterior THA
What are the Concerns?
• Exposure
• Equipment and
Resources
• Learning Curve
• Complications

What are the early problems with
Direct Anterior Approach to Hip
• Operative time
• Fluoro exposure
• Blood loss
• Wound complications
• Femur fracture
• Lat. Fem Cutaneous N. Damage
• Ascending branch of the lateral femoral circumflex artery Injury

Is AMIS better than direct lateral ?
• Less muscle damage
Muller et al, Arch Orthop Trauma Surg, Feb 2011
•Better gait symmetry
Lugade et al, Clin Biomech, Aug 2010
•Better SF-36 and WOMAC at 1 yr
Restrepo, et al, JOA, Aug 2010

Is it better than posterior ?
Limited comparative data at this time
Several ongoing prospective randomized studies

Retrospective comparison study of 45 patients who
had DAA on one hip and posterior or lateral approach
on other hip
Shorter LOS with DAA (2.27 vs 3.87 days)
Less PCA usage (11.6 vs 24.6 mg) morphine
Better ambulation POD #1 166 feet vs 49 feet
Gorab, et al, AAOS 2011
Is it better than posterior ?

LEARNING CURVE COMPLICATIONS
?

Recognize or avoid
the LFCN!!
Good preperation of the entry point
femoral nerve palsies
varus positioning of the stem
Suggestions to avoid problems

Check your reaming depth using fluoro
Insert the acetabular prosthesis carefully under fluoro
acetabular implant protrusio
Suggestions to avoid problems

Accurate and complete femoral neck osteotomy
Careful femoral canal preparation and broaching
fracture of the greater trochanter
Suggestions to avoid problems

periprosthetic fracture
• Identify the femoral canal and be careful when broaching
• In the beginning you can use fluoro
Suggestions to avoid problems

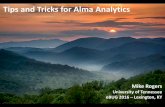
When do complications happen??
0
1
2
3
4
5
0 50 100 150 200 250 300
minor
major
Cases

We suggest that:
There is a learning curve of at least 50
cases for an experienced hip surgeon
Hands on training is necessary
Expect complications but do your best to decrease
their frequency!!

Conclusion
Literature is available to support use of most
surgical approaches
Do not forget the principles of THA
• Long term fixation
• Low wear
Be care about allowing small part (approach)
dictate the whole procedure

5 TIPS for success (5 P’s)
1. Practice
2. Patient Selection
3. Plan
4. Patience
5. Predict Complications

Take home messages
No miracles in approaches!
Learn all of them if you can
Learn mini approaches and use them with caution
Be aware of pitfalls when taking decisions