American College of Radiation Oncology · Program to Dr del Regato . . . . 8 Guidelines for Howard...
16
BULLETIN BULLETIN BULLETIN BULLETIN BULLETIN American College of Radiation Oncology Winter 2000 Volume 7 • Number 1 BULLETIN BULLETIN BULLETIN BULLETIN BULLETIN ACRO to Recognize Fellows at 10th Annual Meeting . . . . . . . . . . . . . . . . . . 3 Other Highlights from the ACRO Executive Committee Meeting . . . . . . . . . . . . . . . . . . 3 Radiation Oncology Topics Receive Media Coverage at 85th RSNA Scientific Assembly . . . . . . . . . 4 RSNA President Describes Effect of Managed Care on Radiology . . . . . . . . . . . . . . . . 5 Annual Oration in Radiation Oncology Addresses Inadequacies of Systemic Therapy for Early-Stage Breast Cancer . . . . . . . . . . . . . 6 Limitations of Lung Cancer Diagnosis and Treatment Discussed by Oncodiagnosis Panel . . . . . . . . . . . . . . . . . . . . 7 RSNA Dedicates Meeting Program to Dr del Regato . . . . 8 Guidelines for Howard H. Wong Fellowships in Radiation Oncology . . . . . . . . . 9 Peer Review Goes Online . . . . 10 Melanoma Vaccine Shows Promise in the Most Advanced Cases of Stage III Melanoma . . . . . . . . 11 American College of Radiation Oncology 10th Annual Meeting: Tentative Program . . . . . . . . . . . . . . . . 13 New Members . . . . . . . . . . . . 14 Some 2000 Meeting Dates . . . 16 inside this issue To become a member or to sign up a friend, Please contact the ACRO office at (630) 368-3733. is Your Organization Help it (Continued on next page) Report from the AMA By Dennis Galinsky, MD In a historic vote, the American Medical Association (AMA) House of Del- egates decided to form a national labor organization. The unit that will be formed will embrace employed physicians in negotiations with hospitals, health plans, and universities concerning employment contracts and patient care. Where allowed, the negotiating unit also will represent residents. Esti- mates are that such a union could help up to 17% of the nation’s physicians. More than half the physicians practicing in this country would not be eligible to join because they are self employed and thus barred from collective bar- gaining by federal antitrust laws. Strikes will not be part of the leverage used by the union. Other actions, such as not filling out paperwork necessary for an employer to effectively collect, will be used. The AMA will continue to lobby for federal antitrust relief in the form of the Campbell Bill, which would enable self-employed physicians to bargain collec- tively, or an amendment to the National Labor Relations Act. A resolution that ACRO had submitted at the 1998 AMA annual meeting op- posing the forceful employment or contracting of physicians by hospitals was
Transcript of American College of Radiation Oncology · Program to Dr del Regato . . . . 8 Guidelines for Howard...

BULLETINBULLETINBULLETINBULLETINBULLETINAmerican College ofRadiation Oncology
Winter 2000
Volume 7 • Number 1
BULLETINBULLETINBULLETINBULLETINBULLETINACRO to RecognizeFellows at 10th AnnualMeeting . . . . . . . . . . . . . . . . . . 3Other Highlights from theACRO Executive CommitteeMeeting . . . . . . . . . . . . . . . . . . 3Radiation OncologyTopics Receive MediaCoverage at 85th RSNAScientific Assembly . . . . . . . . . 4RSNA President DescribesEffect of Managed Care onRadiology . . . . . . . . . . . . . . . . 5Annual Oration in RadiationOncology AddressesInadequacies of SystemicTherapy for Early-StageBreast Cancer . . . . . . . . . . . . . 6Limitations of Lung CancerDiagnosis and TreatmentDiscussed by OncodiagnosisPanel . . . . . . . . . . . . . . . . . . . . 7RSNA Dedicates MeetingProgram to Dr del Regato . . . . 8Guidelines for Howard H.Wong Fellowships inRadiation Oncology . . . . . . . . . 9Peer Review Goes Online . . . . 10Melanoma Vaccine ShowsPromise in the MostAdvanced Cases ofStage III Melanoma . . . . . . . . 11American College ofRadiation Oncology 10thAnnual Meeting: TentativeProgram . . . . . . . . . . . . . . . . 13New Members . . . . . . . . . . . . 14Some 2000 Meeting Dates . . . 16
inside this issue
To become a member or to sign up a friend,Please contact the ACRO office at (630) 368-3733.
���� is Your Organization
�����Help it
(Continued on next page)
������������� ������������ � ���������Report from the AMABy Dennis Galinsky, MD
In a historic vote, the American Medical Association (AMA) House of Del-egates decided to form a national labor organization. The unit that will beformed will embrace employed physicians in negotiations with hospitals,health plans, and universities concerning employment contracts and patientcare. Where allowed, the negotiating unit also will represent residents. Esti-mates are that such a union could help up to 17% of the nation’s physicians.More than half the physicians practicing in this country would not be eligibleto join because they are self employed and thus barred from collective bar-gaining by federal antitrust laws. Strikes will not be part of the leverage usedby the union. Other actions, such as not filling out paperwork necessary foran employer to effectively collect, will be used.
The AMA will continue to lobby for federal antitrust relief in the form of theCampbell Bill, which would enable self-employed physicians to bargain collec-tively, or an amendment to the National Labor Relations Act.
A resolution that ACRO had submitted at the 1998 AMA annual meeting op-posing the forceful employment or contracting of physicians by hospitals was

2 ACRO • Winter 2000
finally passed at this meeting. TheAMA will assist physicians in thissituation through its legal de-partment.
��������������� ������������� ���A resolution asking theAMA to recommend annualmammograms for women>40 years old was passedwith the support of theAmerican College of Sur-geons, ACRO, and ASCO.The American College ofRadiology introduced it. Tomy astonishment, some sur-geons and primary-care phy-sicians opposed it.
����������������������������������The House of Delegatespassed a new policy on theconfidentiality of patient in-formation used for medicalresearch. The new policyadvocates that, where pos-sible, informed consent should beobtained before personally identifi-able health information is used forany purpose. However, in thosesituations in which informed con-sent is not possible, either identify-ing information should be strippedfrom the data or an objective, pub-licly accountable entity must deter-mine that patient consent is not re-quired after weighing the risks andbenefits of the proposed use. It alsosupports the voluntary adherence ofall IRBs to the Common Rule stan-dards, no matter the institution’ssource of funding.
������������������ ����AMA delegates narrowly approvednew ethical guidelines for the sale ofnonprescription health-related prod-ucts in physician’s offices. Delegatesalso passed a companion resolution
emphasizing that physicians shouldnot “coerce patients to purchase”
������������� ������������ � ��������� (continued from page 1)
ACRO
��������Comprehensive socioeconomic, political,
and professional news affecting thedaily practice of radiation oncology
The ACRO Bulletin welcomes letters, comments,suggestions, and submission of articles for con-sideration. The Bulletin reserves the right to edit
letters for clarity and length.
Published: Winter • Spring • Summer • Fall
Editor A. Robert Kagan, MD
Chairman Peter H. Blitzer, MD
President Arthur T. Porter, MD
Vice President A. Robert Kagan, MD
Secretary/Treasurer Michael L. Steinberg, MD
AccountExecutive Torry Mark Sansone
Assistant AccountExecutive Michael R. Eason
Managing Editor Stuart J. Birkby
Please send your correspondence to:
A. Robert Kagan, MDEditor, ACRO Bulletin
c/o American College ofRadiation Oncology820 Jorie Boulevard
Oak Brook, IL 60523-2251
(630) 368-3733 • ������������
The opinions and views expressed in the Bulletinare not necessarily those of the American
College of Radiation Oncology.
health-related products or to recruitthem to “participate in marketingprograms in which the physicianpersonally benefits, financially orotherwise, from the efforts of theirpatients.” To avoid conflicts of inter-est, physicians should offer productsfree or at cost. Dermatologists andplastic surgeons were generally op-posed since they often sell their owncustom preparations.
��� ����������������Luther Brady, MD, ACRO Past Presi-dent, was awarded the AMA’s tophonor, the Distinguished ServiceAward. He was nominated byACRO and is the only radiationoncologist so honored. John Knote,MD, a diagnostic radiologist, wasreelected speaker to the House.
Dennis Galinsky, MD, is directorof the Dupage Oncology Centerin Winfield, Ill. He is the ACROdelegate to the AMA House of Del-egates. ✮Luther W. Brady, MD

Volume 7, Number 1 3
������������� �������������������������������
For the 10th anniversary of ACRO,President Arthur T. Porter, MD, pro-posed that the College install thoseindividuals who have been ACROmembers continuously since the es-tablishment of the College as ACROFellows upon review and approvalof applications. Installation will oc-cur during a convocation ceremonyscheduled during the 10th annualmeeting of ACRO, to be held at thePark Hyatt in Washington, DC, onMay 6 and 7, 2000.
At the meeting of the Executive Com-mittee of ACRO, held in Santa Fe,New Mexico, on October 9, 1999,committee members decided that thestatus of Fellows must have valueand recognition, similar to theAmerican College of Radiology Fel-
low status. Also, criteria to decidewhether an individual is eligible tobecome an ACRO fellow should bebased on excellence in practice andrecognition by patients.
Dr Porter also proposed that indi-viduals who have been ACRO mem-bers for 5 continuous years or haveserved or continue to serve the Col-lege in an elected or appointed ca-pacity also be granted ACRO Fellowstatus. Finally, he proposed a cat-egory of Honorary ACRO Fellows.
All categories were approved andactivated during the Executive Com-mittee meeting. Procedures were es-tablished as follows:
1. If an ACRO member is board
certified in radiation oncology andhas 10 years of continued member-ship in the College, he or she canbe nominated for Fellow status withtwo sponsoring letters from currentACRO members regarding excel-lence in practice and two sponsor-ing letters from physicians in thecommunity where the individualpractices. Nominees will be re-viewed by the ACRO Fellows Com-mittee, with recommendations sub-mitted to the Board of Chancellorsfor review and approval. The nomi-nees must then be present at the an-nual meeting of ACRO for installa-tion. (NOTE: For 2000, nomineeswith 10 years of membership inACRO should already have beencontacted.)
2. The ACRO Fellows Committeewill also review nominees with 5years of continued membership inthe College and who have served orcurrently serve in an elected or ap-pointed capacity for ACRO. Recom-mendations will be submitted to theBoard of Chancellors for review andapproval. All nominees must bepresent at the annual meeting ofACRO for installation.
3. In addition, nominees for Honor-ary ACRO Fellows will be reviewedand approved by the Board ofChancellors after review of the Fel-lows Committee.
The Fellows Committee was then es-tablished, with Dennis L. Galinsky,MD, director of the DuPage Oncol-ogy Center in suburban Chicago, aschairman. Appointed committeemembers are Dr Porter, SuchaAsbell, MD, and David Krause, MD.
For further information about theACRO Fellows Program, and for anapplication, please contact ACRO at820 Jorie Boulevard; Oak Brook, IL60523; telephone (630) 368-3733.
���������������� ���������������������� ��������������
The Membership Committee reported the following statistics regarding ACROmembership as of August 1999:
• Active Members ................ 1,196 • First-year Members ............ 104• Associate Members ................ 63 • Resident Members ............. 283• Corresponding Members .......... 7
The number of active members was an increase of 119 from the same time in 1998.
The Board of Chancellors directed the Membership Committee to collaborate withthe ACRO Website Editor, Peter H. Blitzer, MD, in developing a proposal to set upthe next ACRO membership directory on the ACRO website (www.acro.org).
Arve Gillette, MD, chairman of the Membership Committee, recommended thatthe function of marketing for ACRO be transferred to the Membership Committeesince marketing affects so many aspects of membership recruitment, promotion,and retention. The Board decided to change the name of the Membership Com-mittee to the Committee on Membership and Marketing.
��������������������After a long day of radiationoncology practice, have you satdown in the evenings with anespecially good book of fiction?
If so, share your readingwith other ACRO members!Send your book review to:
A. Robert Kagan, MDEditor, ACRO BulletinDepartment of Radiology/OncologyKaiser Permanente Medical Group4950 Sunset BlvdLos Angeles, CA 90027(323) 783-3865

4 ACRO • Winter 2000
��������������������� ������
�������������������������������������������������� !�"�������������#�������$%��
Radiation oncology received inter-national media coverage at the85th Scientific Assembly and An-nual Meeting of the RadiologicalSociety of North America. Twonoteworthy papers were previouslyselected by Nora A. Janjan, MD,head of the RSNA Radiation Oncol-ogy and Radiobiology Subcommit-tee, for wider circulation beyondthe attendees at the meeting. Thetwo papers dealt with breast cancerin women >75 years old and thequality of life of prostate-cancer pa-tients undergoing radiation therapy,respectively.
���������������� ����������������������������A group of physicians representingthe Naval Medical Center and theUniversity of California, both in SanDiego, and the Tripler Army Medi-cal Center in Honolulu, presented apaper noting there was no clearconsensus on the degree of diag-nostic and therapeutic aggressive-ness elderly women with breastcancer should receive. These pa-tients have traditionally beentreated conservatively because ofconcerns related to their conditionand advanced age. Consequently,researchers retrospectively re-viewed records of women with inva-sive breast cancer who were >75years old since January 1, 1988.Data examined included date of di-agnosis, stage at diagnosis, tumorpathology, comorbid medical condi-tions, Karnofsky performance sta-tus, treatment and diagnostic mo-dalities, tumor recurrence, and out-come. Forty-three percent of the pa-tients were treated with breast-
conserving surgery, 49% underwenta mastectomy, and 9% underwentfine needle aspiration only. Ofthose treated with breast-conservingsurgery, 63% underwent radiationtherapy. Although 80% were estro-gen receptor positive, only 51% ofthese patients were given hormonaltherapy. Of the patients in thisstudy who died, 58% were deadbecause of the breast cancer.
Based on this study, women >75years old with invasive breast can-cer frequently receive nonstandardtreatment or no treatment at all.Consequently, many of thesewomen die of the cancer and notcomorbid conditions. However, asthe general population ages, moreotherwise healthy women are enter-ing this age group. The research-ers suggested a reevaluation of thebelief that comorbid conditions inthe elderly will diminish benefitsfrom therapy.
���������������������������� ������������������������Another group of researchers fromthe Fox Chase Cancer Center andTemple University Hospital in Phila-delphia evaluated the long-termquality of life for prostate-cancerpatients who had undergone three-dimensional (3D) conformal radia-tion therapy. They quantified differ-ences for symptoms that affectedthe bowel and bladder for thosewho received treatment to the pros-tate and seminal vesicles alone ver-sus those who received treatment tothe whole pelvis. Quality of lifemeasures for these patients werecompared with that of the normal
population of men with a similarage distribution. Two health-statussurveys evaluating bowel and blad-der functioning were mailed to 195patients who had undergone 3Dconformal radiation therapy forprostate cancer at the Fox ChaseCancer Center. The response ratewas 62%.
Alexander Hanlon, MD, who pre-sented the study, concluded thatprostate-cancer patients who hadundergone high-dose 3D conformalradiation therapy enjoyed thesame quality of life related to blad-der and bowel function as the nor-mal population. Those patientswho had undergone whole-pelvistreatment were more likely to havea slightly decreased quality of lifeas defined by increased feelingsof urgency and satisfaction withbowel function. However, qualityof life did not seem adversely af-fected regardless of therapeuticfield size. ✮
Nora A. Janjan, MD
Volume 7, Number 1 5
����������� ������������� ����������������������������
Nearly all physicians in the UnitedStates can recall hearing complaintsfrom colleagues and patients aboutthe managed-care system. Manycan relate anecdotal reports of indi-viduals denied life-saving treatmentdue to the for-profit motivations ofmanaged-care companies. SeymourH. Levitt, MD, 1999 president of theRadiological Society of NorthAmerica (RSNA), from the Depart-ment of Therapeutic Radiology at theFairview University Medical Centerin Minneapolis, described the resultsof a study examining the effects ofmanaged care on research andother scholarly activity in radiologyand radiation oncology during hisPresident’s Address at the 85th Sci-entific Assembly and Annual Meet-ing of the RSNA, held in Chicagofrom November 28 to December 3,1999.
“Managed care and current legisla-tion based on the 1997 BalancedBudget Act are placing huge finan-
cial constraints onscholarly activityand patient care,”Dr Levitt warned.
He asked the au-dience to remem-ber the reasonsthey had for ini-tially pursuing acareer in medi-cine. He remindedattendees thattheir reasons werelikely based on adesire to servepeople afflicted bydisease or injury.“Our responsibility
is to our patients,” Dr Levitt empha-sized. However, healthcare undermanaged care is being driven byconsiderations related primarily toprofitability.
Research and scholarly activity havebeen relegated to a “secondary sta-tus,” said Dr Levitt. “Centers of edu-cation and research are under at-tack due to the dominance of man-aged care,” he added.
Specifically, managed care has re-sulted in constraints on the growth ofpatient care revenues. Dr Levitt re-ported that the nation’s teachinghospitals will lose a cumulative $15billion by 2002. He added that re-searchers no longer have the time topursue their work. This hurts facultymorale and retention at many re-search institutions.
Most of the studies illustrating theeffects of managed care have beenanecdotal. Consequently, Dr Levitt
gave some preliminary conclusionsbased on the first phase of anRSNA-sponsored study to more ac-curately quantify the problem. In-formation was collected from sixacademic departments of diagnos-tic radiology and radiation oncol-ogy. The study samples were se-lected based on “managed-carepenetration” as defined byInterstudy’s HMO Penetration andIndustry Data: Metropolitan Statisti-cal Areas. A study questionnairewas developed to compare fiscalyear 1993 to fiscal year 1998 andasked questions relating to topicssuch as revenue, expenditures, RVUproduction, number of full-time fac-ulty, source of research funding,and number of fellowships. Overall,the study revealed that radiologyand radiation oncology depart-ments that deal within a communitythat has a “medium” or “high” pen-etration by managed-care compa-nies are more dissatisfied with theresults of managed care. Facultyretention, no time for research, anda deterioration in the residency-training program were frequentcomplaints. The RSNA is about tobegin the second phase of thisstudy.
Dr Levitt concluded his presentationby stating that radiologists mustdefine the importance of educationand research to their field and makeit known that the practice of radiol-ogy is “not about profit.” He admit-ted that, as the 21st century ap-proaches, physicians will have toadapt to evolutionary changes inmedicine, but this does not necessar-ily mean sacrificing the main objec-tives of healthcare. ✮
Seymour H. Levitt, MD

6 ACRO • Winter 2000
��������������������� ������
������������������������������������������������������������������� ����!���"�����������#������$�����������
Over the past few decades, ad-vances have been made in the fieldof systemic therapy for early-stagebreast cancer. For example, high-risk patients may receive cytotoxicpolychemotherapy and estrogen-receptor-positive patients may betreated over the long term withtamoxifen. Lars E. Rutqvist, MD,PhD, from Stockholm, pointed outthat the efficacy of such systemictreatment is still inadequate. Hegave his comments as part of the1999 Annual Oration in RadiationOncology at the 85th Scientific Ses-sion and Annual Meeting of the Ra-diological Society of North America(RSNA), held from November 28–December 2, 1999, in Chicago.The oration was given in memory ofJerome H. Vaeth, MD, an expert inradiation oncology who had writtenextensively on this subject.
Dr Rutqvist noted that in the first 10years after primary diagnosis, 30%–40% of women with early-stagebreast cancer who received systemictherapy still experience a distant dis-ease recurrence. He added that lo-cal control is also a significant clini-cal problem since the risk of local
failure varies depending on clinicalstage, biologic markers of tumor ag-gressiveness, and type of local treat-ment. Radiation therapy as an ad-junct to primary surgery decreasesthe risk of local failure, but salvagetherapy for clinically diagnosed lo-cal recurrences often fails, leadingto an increased rate of uncontrolledlocal disease on the chest wall and,subsequently, a deteriorating, poorquality of life.
In addition, relevant radiationtherapy trials date back to the late1940s. Dr Rutqvist told RSNA meet-ing attendees that over the years thedesign of these trials has been influ-enced by developments in the fieldsof biostatistics, radiobiology, and ra-diation physics, as well as radiationoncology and, at the eve of the 21stcentury, most are now obsolete andno longer of value to current prac-tice. Consequently, overviews ofradiation therapy trials, which DrRutqvist called “meta-analyses,”have been performed to generatestatistically more reliable results. Yeteven meta-analyses are flawed be-cause of their dependence on resultsderived from decades-old trials.
Still, certain trends are becomingclear. Dr Rutqvist said that radiationtherapy has resulted in a significantdecrease in mortality due to breastcancer, but that many radiationtherapy techniques have been asso-ciated with an increase in mortalitydue to cardiovascular disease. In-depth evaluations with three-dimen-sional dose reconstruction tech-niques have suggested that adversecardiac effects of radiation can beobviated by paying careful attentionto appropriate treatment methodolo-gies and avoiding excessive treat-ment.
Dr Rutqvist also made attendeesaware that many questions concern-ing the role of radiation therapy inearly-stage breast cancer still needto be answered. Specifically, thereshould be a clearer definition ofthose patients most likely to benefitfrom radiation treatment as differen-tiated from patients who can betreated with a local excision withoutradiation therapy. Further advancesin molecular biology over the nextdecade may help to clarify some ofthese issues. ✮
������������ ����������
��������� �����������������������
��� ���������������� ���������
!��"#��$�%���&
Lars E. Rutqvist, MD, PhD
����������� ������� ��� ������� �����������
����������� ������� ��� ������� �����������

Volume 7, Number 1 7
��������������� ������������������������������ ����� ��������
At the 85th Scientific Assembly andAnnual Meeting of the RadiologicalSociety of North America, held inChicago from November 28 to De-cember 3, 1999, a multidisciplinarygroup of experts forming the Onco-diagnosis Panel described the diag-nostic imaging, pathologic diagnosis,and treatment of lung cancer. Lungcancer is the second most commoncancer among men and women andremains a leading cause of cancerdeath for both sexes. Groups such asthe American Cancer Society haveestimated that approximately 68,000women and 91,000 men died of thedisease in 1999. That exceeds thetotal number of deaths from breast,prostate, and colorectal cancer. Thecombined 5-year survival rate forlung cancers at all stages averages adismal 14%. The OncodiagnosisPanel illustrated that a multidisciplin-ary approach was most beneficial forthe patient. The panelists reviewedcases and described improved diag-nostic procedures and combinedtreatment regimens. Ritsuko U.Komaki, MD, from the M. D. Ander-son Cancer Center in Houston, Tex,was panel moderator. The panelists
were Roger W. Byhardt, MD, fromMilwaukee, Wisc; Marvin H.Chasen, MD, Frank V. Fossella, MD,and Joe B. Putnam, Jr, MD, all fromHouston; and William Travis, MD,from Washington, DC.
During the first case review involvingsmall-cell carcinoma, Dr Chasen em-phasized that the radiologist shouldstrive to identify signs of disease sta-bility. Dr Travis subsequently detailedrevised histologic classifications ofsmall-cell and large-cell cancers andtypical and atypical carcinomas.“There is no such thing as a benigncarcinoid,” Dr Travis added. DrFossella outlined the treatment forsmall-cell cancer, which is dependenton a determination of the extent ofthe disease. He discussed the role ofchemotherapy and radiation therapyfor locally advanced non–small-celland small-cell lung cancer. Small-cellcancer is difficult to treat because,
although it responds to therapy, itspreads quickly. “These patients needan aggressive approach becausethey can be cured,” said Dr Fossella.
The second case review dealt with a20 pack-year cigarette smoker whohad also smoked 2–4 cigars per dayfor 10 years. Radiographs showed alarge lung mass but did not clearly vi-sualize the exact anatomic location.CT scans further defined the diseasestate. Histologic analysis led to a di-agnosis of squamous-cell carcinoma.When subsequently discussingtherapy for non–small-cell lung can-cer, Dr Fossella stressed, “We canimprove treatment by using a multi-modality approach.” He and DrByhardt then proceeded to discussthe advantages and disadvantages ofcombination radiation therapy andchemotherapy, with and without sur-
gery, for this disease. Inthis particular case, thepatient is still alive 2 yearslater after undergoingradiation therapy andchemotherapy only.
In the third case, Dr Chasen pointedout that the radiologist’s primary rolewas to evaluate for cancer recur-rence, and he showed an MR imag-ing assessment of a superior sulcustumor’s effect on non-pulmonary sys-tems and organs, particularly thebrain. Dr Byhardt then discussed thedisadvantages of treating such a dis-ease with preoperative radiationtherapy.
The Oncodiagnosis Panel stressedthe growing importance of functionalimaging and demonstrated how ithas the potential to change diagnos-tic and therapeutic procedures forlung cancer. ✮
The OncodiagnosisPanel was composed of(from left to right)Marvin H. Chasen, MD,Ritsuko U. Komaki, MD,William Travis, MD,Frank V. Fossella, MD,Joe B. Putnam, Jr, MD,and Roger W. Byhardt,MD.
“We can improve treatment byusing a multimodality approach.”
8 ACRO • Winter 2000
��������������������� ������
�����������������������������������������������
The Radiological Society of NorthAmerica (RSNA) dedicated its Scien-tific Program for its 85th ScientificAssembly and Annual Session, heldin Chicago from November 28 toDecember 3, 1999, to Juan Angeldel Regato, MD, a pioneer in thera-peutic radiology. Dr del Regato diedon June 12, 1999, following sur-gery for injuries sustained in a fall.Born in Camagüey, Cuba, on March1, 1909, he was naturalized as anAmerican citizen in 1941. He at-tended medical school at the Univer-sity of Havana and earned his medi-cal degree from the University ofParis in 1937. He served as an in-tern at the Radium Institute of Parisfrom 1935 to 1936 and as a re-search fellow at the Curie Founda-tion in France from 1936 to 1938.After serving as assistant radiothera-pist at the Institute of Radium at theUniversity of Paris, he became anassociate radiotherapist and lecturerat the Chicago Tumor Institute in1939. In 1941, he joined theWarwick Cancer Clinic in Washing-ton, DC, and later the Ellis FischelCancer Hospital in Columbia, Mis-souri. In 1949, with the assistanceof wealthy philanthropist SpencerPenrose, he established the PenroseCancer Hospital in ColoradoSprings, the first training center inthe United States dedicated to thera-peutic radiology. Dr del Regato di-
rected the hospital from 1949 to1973. He was named DistinguishedPhysician (Consultant at Large) forthe James A. Haley Veterans Admin-istration Medical Center in Tampa in1974 and served that institution asemeritus professor from 1982 untilhis death.
Dr del Regato was vice-president ofthe RSNA in 1959 and 1960. Hewas the founding father of theAmerican Society for TherapeuticRadiology and Oncology. Also, heenjoyed a long and distinguishedcareer as an educator, researcher,inventor, historian, and author. “FewAmerican physicians have had asgreat an impact on the developmentof a medical specialty as did Dr delRegato,” said his former student, J.Frank Wilson, MD, of Milwaukee.
Serving the medical community formore than 5 decades, Dr del Regatowas instrumental in the advancementof therapeutic radiology. Among hismany accomplishments, while still inFrance he invented the “del Regatolocalizer,” a device that facilitatedthe delivery of effective radiationtreatments in the early days of radia-tion oncology. He also helped to co-ordinate one of the first cooperativeclinical trials in cancer investigation,evaluating the effectiveness of radia-tion therapy in treating inoperableprostate cancer.
He was a respected lecturer and aprolific author of hundreds of articlesand books in several languagesread worldwide. He co-authoredone of the first multidisciplinary text-books, Cancer: Diagnosis, Treatmentand Prognosis, and profiled the livesof physicians, medical physicists,
and other scientists important in thedevelopment of radiology and radia-tion oncology, many of whom heknew personally.
Dr del Regato was an eminent pro-fessional highly regarded world-wide. Organizations around theglobe bestowed more than 40 hon-ors on him. He was named SilverMedal Laureate by the Faculty ofMedicine, University of Paris in1937; Prix Chevillon Laureate, Na-tional Academy of Medicine ofFrance, 1948; and Prix BruninghausLaureate, French Academy of Medi-cine in Paris in 1979. He is amongfive American radiation oncologiststo receive the Beclere Medal fromthe Centre Antoine Beclere in Paris.The RSNA gave him its Gold Medalin 1966. He received a Distin-guished Service Award from theAmerican Cancer Society and a Sci-entific Achievement Award from theAmerican Medical Association. ✮
Juan Angel del Regato, MD
Volume 7, Number 1 9
������������ �������������������������������� �����������
Five $2,000 grants are awarded toradiation oncology residents to sup-port subspecialty electives at anyqualified United States institutiondemonstrating expertise in the de-sired subspecialty area. (There areno European elective grants.) Eli-gible applicants are ACRO andARRO radiation oncology residentmembers in their second, third, orfourth years of an accredited U.S.residency through June 2000 whohave not previously been awardedan ACRO fellowship grant.
Applicants are responsible for ar-ranging their electives with the hostinstitution before the submission oftheir application. Electives must bearranged for a minimum of fourweeks and for a maximum of eightweeks. Electives must be completedbetween July 1, 1999, and June 30,2000. Subspecialty electives includebrachytherapy, conformal, andthree-dimensional treatment planningtherapy, gynecologic radiation on-cology, head and neck radiation on-cology, pediatric radiation oncology,and radiosurgery.
�������������� ��The application must include the fol-lowing information: the elective;dates of the elective; the residency
program director; the host institutionadvisor; an essay, describing howthe elective will supplement resi-dency training and benefit a careeras a radiation oncologist; and a cur-riculum vita. Eligible radiation oncol-ogy residents must submit five copiesof both the official application and acurriculum vita to ACRO by June 1,2000.
� �� ����� ��Applications are reviewed by theACRO Fellowship Program Commit-tee, made up of five members (thechairman, appointed by the ACROpresident; the ACRO vice-president,the ARRO representative to ACRO,an appointee of the ACRO vice-president, and an appointee of thechairman). Committee membersrank the candidates. The committeechairman tabulates rankings and in-forms committee members of the fi-nal selection of fellowship awards.Committee members have an oppor-tunity to appeal the final selectionsbefore the announcement of theaward on July 1.
The committee chairman contactseach fellowship award recipient bytelephone to extend congratulations.Subsequently, the ACRO presidentforwards formal notification letters to
each recipient. Also, the committeechairman forwards formal regret let-ters to applicants who were not se-lected for fellowship awards.
�� ���� ����� ���Upon the completion of the elective,the resident obtains a letter from theprogram director or hosting physi-cian indicating successful completionof the elective and the beginningand ending dates of the elective. Inaddition, the resident will submit asummary report of the experiencespecifying how the elective supple-mented his or her residency trainingand how it will benefit his or her fu-ture career as a radiation oncolo-gist. Once the program-completionletter and report are forwarded tothe ACRO president, ACRO head-quarters forwards the $2,000 grantto the resident.
ACRO provides information on theACRO fellowship program in theARRO spring mailing to all U.S. radia-tion oncology residents, in additionto program promotion in the ACROBulletin. For further information aboutthe Howard H. Wong Fellowships inRadiation Oncology, contact ACROheadquarters at 820 Jorie Boulevard;Oak Brook, IL 60523-2251; tele-phone (630) 368-3733. ✮
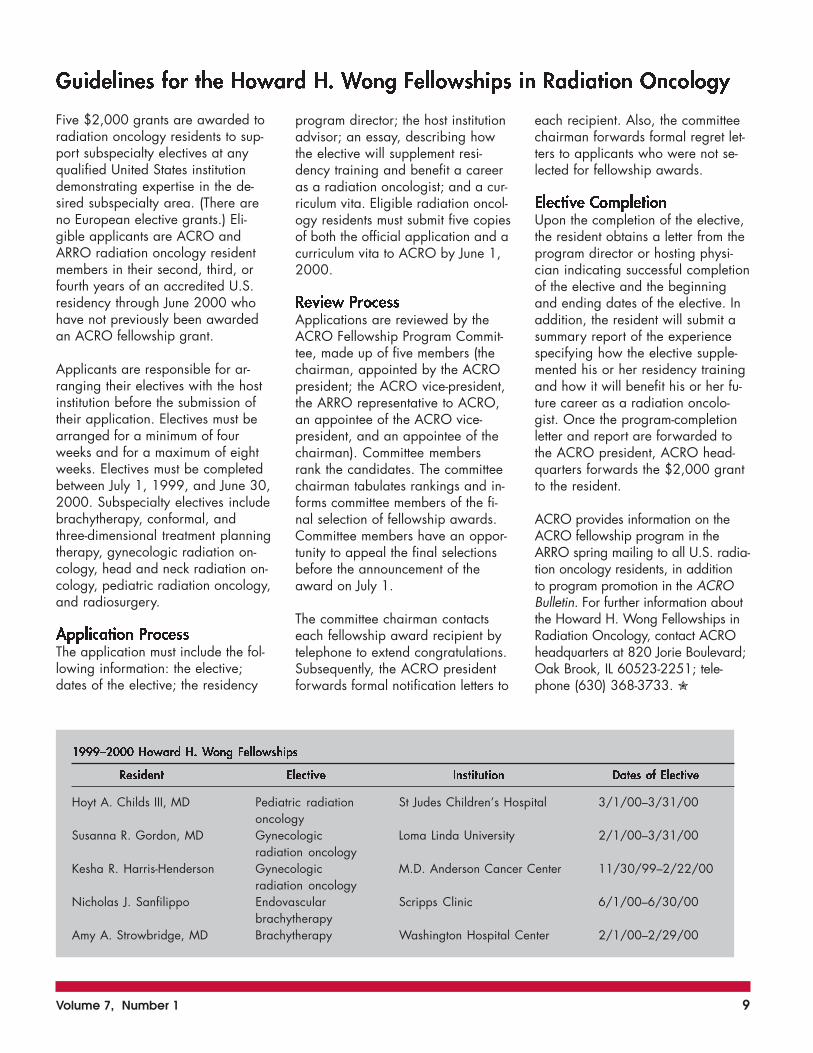
���������������� ����������������
�������� �������� ����������� ������ ���������
Hoyt A. Childs III, MD Pediatric radiation St Judes Children’s Hospital 3/1/00–3/31/00oncology
Susanna R. Gordon, MD Gynecologic Loma Linda University 2/1/00–3/31/00radiation oncology
Kesha R. Harris-Henderson Gynecologic M.D. Anderson Cancer Center 11/30/99–2/22/00radiation oncology
Nicholas J. Sanfilippo Endovascular Scripps Clinic 6/1/00–6/30/00brachytherapy
Amy A. Strowbridge, MD Brachytherapy Washington Hospital Center 2/1/00–2/29/00

10 ACRO • Winter 2000
Please share your experienceswith your peers. Write an articlefor the ACRO Bulletin. Your in-formation is valuable, whetheryou are new to radiation oncol-ogy or have worked in the fieldfor many years.
Attention Writers!
Please send your material to:A. Robert Kagan, MDDepartment of Radiology/OncologyKaiser Permanente Medical Group4950 Sunset BlvdLos Angeles, CA 90027(323) 783-3865
���������������� �� �
check a password-protected site tosee when copies of their manu-script were sent to reviewers andwhen the reviews are due. Review-ers’ comments are posted anony-mously. Once all reviews are in,Neoplasia editors post their deci-sion to accept, accept with revi-sions, or reject the manuscript forpublication.
The Editor of Neoplasia, Brian D.Ross, MD, a professor of radiologyat the University of Michigan, notesboth the journal and contributorssave money because manuscriptsare not mailed worldwide. Dr Rossalso believes the online system ispopular because less time is spent
A one-year-old journal of oncol-ogy, entitled Neoplasia (http://www.neoplasia.org), uses anonline review process. Authors cantrack the status of their submissionselectronically.
Potential contributors to Neoplasiamust submit their manuscripts digi-tally and recommend potential re-viewers. The copyright releaseform must be printed out from thejournal’s Internet site, signed, andfaxed to the journal’s editorial of-fices. Reviewers receive the manu-scripts as E mail or through a pass-word-protected Web site. They usea Web form to rate the paper andcomment. Meanwhile, authors can
in the American College of Radiation Oncology Newsletter
To place your listing, look on page 11 for details and rate information!
Be part of the latest information and ideas in the industry
It Pays to AdvertiseIt Pays to Advertise
waiting for reviewers’ responses. Ithas taken an average of 19.2 daysfor a manuscript to go from submis-sion to decision.
In addition, Dr Ross states that re-views are posted as they come in,not held back until all reviews havebeen received by the editors. Someauthors have written a defense oftheir work after a negative review,which is helpful when the final de-cision to publish is made. ✮

Volume 7, Number 1 11
ACRO ��������
Comprehensive socioeconomic, political andprofessional news affecting the daily practice ofradiation oncology
Official Newsletter of the AmericanCollege of Radiation Oncology
������������ ����Editor
820 Jorie BoulevardOak Brook, IL 60523-2251
Phone: (630) 368-3733Fax: (630) 571-7837
Published: Winter • Spring • Summer • Fall
Payment must accompany order. Make checkspayable to American College of RadiationOncology (ACRO), or payment may be madeby credit card (MasterCard, Visa, or AmericanExpress); call for details. Advertisers who can-cel ads will not receive refunds.
The ACRO Bulletin accepts classifiedadvertising for:
������ ����������������� ���������������������� �������� ��������������������
Ads must be submitted, typed, double-spaced.Initials or abbreviations equal one word. Tele-phone numbers with area code equal one word.
Any advertisements submitted that are notcamera ready or electronically supplied willincur additional charges.
������������� �������� ��������� ������ ������ �����
� � �� ��� ���� ����
�� � �� ���� ��� ����
��� ���������� ����� ������������������������������������������������ ���������!�������"�#���� $���$���������$%$�&���!���$&���%$�&'��(��%$!���$&���%$�&�������&�)��$����&%�
�������� �����������
��������������� ���������������� �����������������������������������������Study Supports Clinical Utility of Vaccine Therapy in the Treatment of Cancer
according to the results of a phase2 clinical trial. The findings of thestudy, which was sponsored byAVAX Technologies, Inc (AVAX),were presented earlier this yearat the 90th Annual Meeting of theAmerican Association for CancerResearch and suggest that vaccinesmay play an important role in thetreatment of one of the most fatalforms of cancer.
M-Vax is one of AVAX’s AC Vac-cines made from the patient’s owncancer cells. The vaccine is madeby modifying the tumor cells witha molecule called a “hapten.” Thisprocess, known as “hapteniza-tion,” alters the tumor cells andmakes them appear foreign to thepatient’s immune system. When thehapten-modified cells are injectedinto patients, they stimulate the im-mune system to recognize the can-cer cells and destroy them.
“These data support and expandon the results of previous phase 2trials, which suggested that M-Vaxincreased the overall survival ratein patients with large, surgicallyresectable metastases to a singlelymph node site,” said David Berd,MD, principal trial investigator, in-ventor of the AC Vaccine, and pro-fessor of medicine at the KimmelCancer Center of Thomas JeffersonUniversity, Philadelphia. “Now, wehave extended those findings to pa-tients with a much lower chance ofcure with surgery alone. All of the
patients in the current study hadrecurrence of their melanoma in asecond lymph node before receiv-ing M-Vax.”
Out of the 40 patients who partici-pated in the trial, 43% (n=17)were still alive and 30% (n=12)remained relapse free. The ex-pected 5-year survival rate aftersurgery alone was <10%. A sub-
group of 15 patientswith a particularlybad prognosis (ie,those with an exten-sive spread of mela-noma to the pelviclymph nodes) didsurprisingly well after
treatment with M-Vax. A 5-yearsurvival rate of 47% was pro-jected for this subgroup, com-pared to a 5%–10% historicalsurvival rate with surgery alone.
In this study, patients were treatedwith multiple injections of M-Vaxaccording to one of four dosageschedules over 2–6 months. No se-rious adverse events occurred. Allpatients had inflammatory or pustu-lar reactions at the vaccine injec-tion sites, which caused itching ormild discomfort.
Melanoma is the most serious formof skin cancer and affects approxi-mately 390,000 people world-wide. The American Cancer Soci-ety estimates that, in the UnitedStates alone, >40,000 new casesare diagnosed, and >7,000people die of the disease everyyear. The current treatment forstage III melanoma is surgical re-moval of the tumor mass, followedby high doses of alpha-interferon,a form of chemotherapy. ✮
Postsurgical treatment with the au-tologous cell vaccine (AC Vaccine),M-Vax, appears to extend survivaland reduce relapse rates in mela-noma patients whose disease hadmetastasized to two nodal sites,
Melanoma is the most serious formof skin cancer and affects approxi-mately 390,000 people worldwide.

12 ACRO • Winter 2000
������������ �������
The Official Internet Resource of the
American College of Radiation Oncology
Advancing Communication ... Realizing Opportunities ...
Founded in 1989 with a current membership of approximately1,700, the American College of Radiation Oncology is theonly organization that exclusively, and uniquely, representsradiation oncologists in the socioeconomic and political spherewithout influence from any other specialty.
�����
���
��
��
� ��
�����
���
��
��
� �� www.acro.orgPeter H. Blitzer, MD • Website Editor
������������ �������
May 6–7, 2000Park HyattWashington, DC
������������ �������
The meeting is a seminarfocusing on currenteducational and socio-economic issues in thespecialty of radiationoncology. ACRO offersfree admission to itsannual meeting for allresidents and discountedfees to all members.ACRO will award CMEcredits to all meetingattendees.

Volume 7, Number 1 13
������������ ������������������ ������������� ������������������ ������������� ������������������ ������������� ������������������ ������������� ������������������ �
���������������� ���������������� ���������������� ���������������� ����������������
������������ ������������������ ������������� ������������������ ������������� ������������������ ������������� ������������������ ������������� ������������������ �
���������������� ���������������� ���������������� ���������������� ����������������
���������� ���
�����
7:30 AM Continental breakfast/registration
8:00 AM Session 1: Government RelationsKeynote Address: U.S. SurgeonGeneralPresentations by Tom Harkins, ConnieMack, and Andrew L. Woods
10:30 AM Break
11:00 AM Panel Discussion (Andrew L. Woods,moderator)
12:00 noon Lunch
1:00 PM Session 2: Practice AccreditationKeynote Address: John Ginapp, PhDPresentations by Ralph R. Dobelbower,Jr., MD, PhD, Donald P. Ragan, PhD,Peter Garrett, MD, and Gregory W.Cotter, MED
3:30 PM BreakPanel Discussion (Ralph R.Dobelbower, Jr, MD, PhD, moderator)
4:00 PM 2000 ACRO Gold Medal Presentationto James Robert Cassady, MDPresentation by Peter H. Blitzer, MD,ChairmanAddress by James Robert Cassady,MD
5:00 PM Adjournment
6:30 PM President’s Reception
�����
7:30 AM Continental breakfast/registration
8:00 AM Session 3: Business EducationKeynote Speaker: Joseph Bales, MDPresentations by Gadi Weinrich (Fraudand Abuse) and David Main (PracticeManagement)
10:00 AM BreakPanel discussion
11:00 AM Installation of 2000 ACRO FellowsIntroduction by Luther W. Brady, Jr,MDInduction of ACRO OfficersPresentation of 2000 Honorary ACROFellows
12:00 noon Meeting adjournment
���� ����� � �� �� �� ������ �������������� ��

14 ACRO • Winter 2000
������������ ����������
Since 1996, ACRO has been composed of more than 1,000 active members.ACRO welcomes the following individuals who have become new members since
September 1999:
WelcomeWelcome
Eric G. Aguero, MDMajid O. Al-Othman, MDLaura H. Allen, MDMorgan Barrett, MDGregory H. Carlsen, MDMary Anne C. DePaz, MDAnnie Ebacher , MDLoren Godfrey, MDMelanie D. Graham, MDLesley A. Hughes, MD, RPhMatthew C. Hull, MDJ. B. Hunter, MD, MScChristopher M. Iannuzzi, MDTeri S. Katz, MDLarry L. Kestin MDRex A. Kiteley MDDavid A. Koeplin, MDAnuradha Koka, MDAlbert C. Koong, MD, PhDChi Lin, MD, PhDAdir Ludin, MDMargaret T. Macdowell, MD
Kevin P. McMullen, MDRandy L. Moore, DOAndrew C. Neuschatz, MDDavid S. Parda, MDAlexander C. Perez, MDGary M. Proulx, MDShari B. Rudoler, MDWalter M. Sahijdak, MDMaygol Sarvi, DO, MSVictor G. Schweitzer, MDMark S. Sinesi , MD, PhDArnold B. Smith, MDJames L. Studt , MDSarah A. Thurman, MDShannon K. Tomlinson, MDLoubna Toufik-Scally, MDThanh J. Van, MD, PhDNancy H. Wiggers, MDAnne W. Winterland, MDAlexander M. Yeh, MDTorunn I. Yock, MD, MChMei Zhang, MD

Volume 7, Number 1 15
YOUR PRESCRIPTION FOR DATA MANAGEMENT
AND FINANCIAL SUCCESS
Billing Services
On-Site Audits and Evaluations
Review of Fee Schedule
Retainer Client Services
On-Site Training
Corporate Clients
Equipment Vendors
Pharmaceutical Companies
Documentation Review
Managed Care Contract Review
Legislative Updates
Liaison to Third Party Payors
Our company was founded with the premisethat we understand your concerns, your
markets, your customersand your values.
Established in 1983
Telephone: (770) 693-6031 • Fax: (770) 693-6030www.amac-usa.com / www.amac-atl.com
Linda L. Lively, M.H.AFounder and CEO
James E. Hugh, M.H.AVice President
�������� The mission of the American College of Radiation Oncologyis to promote the education and science of radiation oncology,to improve oncologic service to the patient, to study the socio-economic aspects of the practice of radiation oncology, and toencourage improved and continuing education in radiationoncology and its allied professional fields.
Become a member of ACRO and take advantage of the benefits it has to offer. Mem-bership classifications range from Active to Corporate. You will receive newsletters,journals, and be able to attend the Annual Meeting. You may qualify for fellowshipawards and can be appointed to the College’s various committees. To find out moreinformation about becoming a member, please call (630) 368-3733.
������������ ������������������ ������������� ������������������ �
������������������

16 ACRO • Winter 2000
FIRST CLASSU.S. POSTAGE
PAIDWHEELING, IL
PERMIT NO. 281
American College of Radiation Oncology820 Jorie Boulevard • Oak Brook, IL 60523-2251
ICTR 2000Dr. Jacques BernierCantonal Departmentof Radio-OncologySan Giovanni HospitalCH-6504 Bellinzona, SwitzerlandTelephone 41 91 820915Fax 41 91 8209044
������ ����������� �������������������������������� ������� �������
March 5–8, 2000Lugano, Switzerland
European Congress ofRadiologyNeutorgasse 9/2A1010 ViennaAustriaTelephone 43 1 533-4064Fax 43 1 533-40649
� ������March 5–10, 2000Vienna, Austria
������������� �� ����� ����� ������ ���
International Society ofRadiography and RadiationTherapyGPO Box 2609Sydney, NSW 2001AustraliaTelephone 61 292411478Fax 61 292513552
�������������� �����������March 19–23, 2000Sydney, Australia
American Radium Society (ARS)
����������� ����April 1–5, 2000Hotel IntercontinentalLondon, England
American College ofRadiation Oncology (ACRO)
!���������� ����May 6–7, 2000Park HyattWashington, DC
British Institute of RadiologyCollege of RadiographersInstitue of Physics and Engineering inMedicinePO Box 2895London W1A 5RSUnited KingdomTelephone 44(0) 20 7307 1410Fax 44(0) 20 7307 1414
�"������#� �$����%�"�������%�����
May 22–24, 2000Birmingham, England
Radiological Society of NorthAmerica (RSNA)820 Jorie BoulevardOak Brook, IL 60523-2251Telephone (630) 571-7835Fax (630) 571-7837
�&����������������$'����������� ����November 26–December 1, 2000Chicago, IL