Ambulatory Clinical Informatics and The Health Record … · Ambulatory Clinical Informatics and...
43
Ambulatory Clinical Informatics Ambulatory Clinical Informatics and and The Electronic Health Record Incentive Payment The Electronic Health Record Incentive Payment Program Program Neil R. Kudler, MD Neil R. Kudler, MD Medical Director of Clinical Informatics Medical Director of Clinical Informatics Baystate Health Baystate Health Springfield, MA Springfield, MA AAPC Springfield Regional Conference AAPC Springfield Regional Conference October 7, 2010 October 7, 2010
Transcript of Ambulatory Clinical Informatics and The Health Record … · Ambulatory Clinical Informatics and...
Ambulatory Clinical Informatics Ambulatory Clinical Informatics and and The Electronic Health Record Incentive Payment The Electronic Health Record Incentive Payment ProgramProgram
Neil R. Kudler, MDNeil R. Kudler, MDMedical Director of Clinical InformaticsMedical Director of Clinical InformaticsBaystate HealthBaystate HealthSpringfield, MASpringfield, MA
AAPC Springfield Regional Conference AAPC Springfield Regional Conference October 7, 2010October 7, 2010
The Electronic Health Record Incentive The Electronic Health Record Incentive Payment Program Payment Program isis
Meaningful UseMeaningful Use
Interim Final Rule released 12Interim Final Rule released 12‐‐3131‐‐0909
Public comment to 3Public comment to 3‐‐1010
Reformulation and response released as Reformulation and response released as
Final Rule on July 13, 2010Final Rule on July 13, 2010
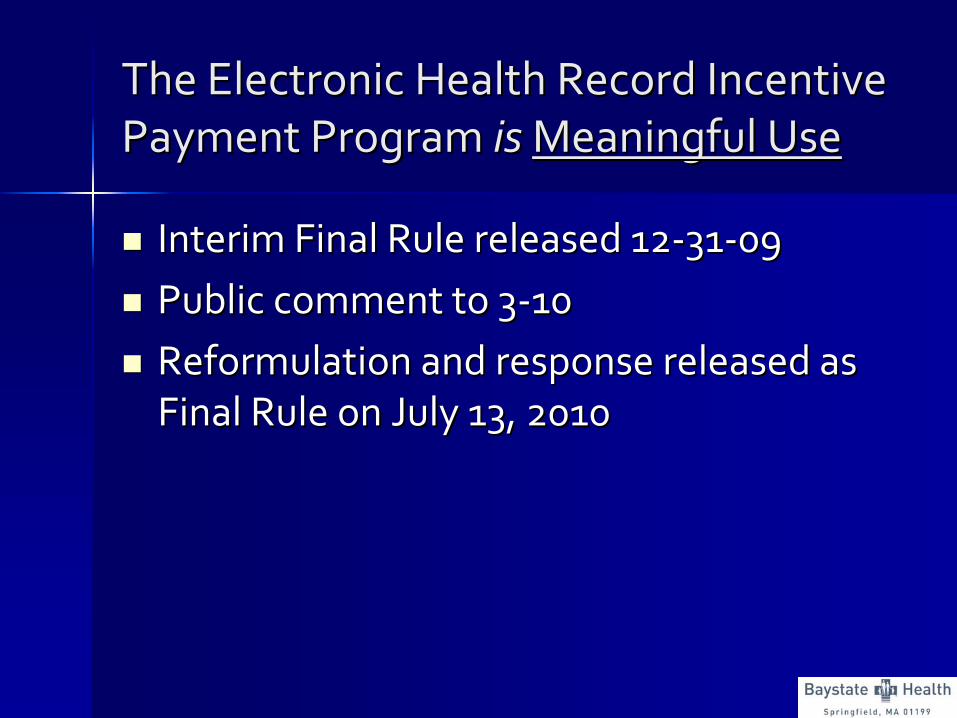
Medicare and Medicaid EHR Incentive Medicare and Medicaid EHR Incentive Payment BasicsPayment Basics
Defining Meaningful UseDefining Meaningful Use
American Recovery and Reinvestment Act American Recovery and Reinvestment Act (ARRA) authorizes CMS to provide incentive (ARRA) authorizes CMS to provide incentive
reimbursement to physician and hospital reimbursement to physician and hospital providers for becoming providers for becoming ““meaningful usersmeaningful users””
of a of a
certified electronic health record certified electronic health record
Stage 1 of 3 begins in 2011 with project Stage 1 of 3 begins in 2011 with project culmination in 2015culmination in 2015
Penalties are incurred for nonPenalties are incurred for non‐‐compliance in compliance in 20162016
Defining Meaningful UseDefining Meaningful Use
In 2008, the National Quality Forum identified a In 2008, the National Quality Forum identified a set of national priorities for healthcare set of national priorities for healthcare
improvementimprovement––
Patient engagementPatient engagement
––
Reducing racial disparitiesReducing racial disparities
––
Improved safetyImproved safety
––
Increased efficiencyIncreased efficiency
––
Coordination of careCoordination of care
––
Improved population healthImproved population health
Privacy and security have since been built into the Privacy and security have since been built into the
frameworkframework

HITECH HITECH ((Health Information Technology for Health Information Technology for Economic and Clinical HealthEconomic and Clinical Health))
Act created Act created 3 3
incentives programsincentives programs
for Meaningful Use: for Meaningful Use: ––
Medicare FeeMedicare Fee‐‐forfor‐‐ServiceService
––
Medicare AdvantageMedicare Advantage––
Medicaid programsMedicaid programs
Three categories of eligibilityThree categories of eligibility––
Eligible hospitals (EH)Eligible hospitals (EH)
––
Critical access hospitals (CAH)Critical access hospitals (CAH)––
Eligible providers (EP)Eligible providers (EP)
Defining Meaningful UseDefining Meaningful Use

Defining Meaningful UseDefining Meaningful Use
Eligible Hospitals and Critical Access Hospitals Eligible Hospitals and Critical Access Hospitals are eligible for both Medicare and Medicaid are eligible for both Medicare and Medicaid
incentive paymentsincentive payments––
Medicare and Medicaid programs have minor Medicare and Medicaid programs have minor
variations in eligibility and reimbursement planningvariations in eligibility and reimbursement planning––
Incentive payments for eligible hospitals would be Incentive payments for eligible hospitals would be
calculated based on the provider number used for calculated based on the provider number used for
cost reporting purposes cost reporting purposes
CMS Certification Number (CCN) CMS Certification Number (CCN)

Eligible Hospital: incentive payments for Eligible Hospital: incentive payments for
eligible hospitals would be calculated eligible hospitals would be calculated based on the provider number used for based on the provider number used for
cost reporting purposes, which is the CMS cost reporting purposes, which is the CMS Certification Number (CCN) of the main Certification Number (CCN) of the main
providerprovider––
Eligible Hospitals and CAHs may participate Eligible Hospitals and CAHs may participate
in both the Medicare programs and the in both the Medicare programs and the Medicaid programMedicaid program
Defining Meaningful UseDefining Meaningful Use
Defining Meaningful UseDefining Meaningful Use
Eligible Professionals (EPs) can receive Eligible Professionals (EPs) can receive eithereither Medicare Medicare oror
Medicaid incentive paymentsMedicaid incentive payments
––
EP must provide >10% of services in ambulatory EP must provide >10% of services in ambulatory
setting (including observation status patients; setting (including observation status patients;
excludes all POS 21 & 23)excludes all POS 21 & 23)
HospitalHospital‐‐based clinic providers are eligible as EPsbased clinic providers are eligible as EPs
––
Medicare: MD, DO, DDS, DMD, DPM, DC, ODMedicare: MD, DO, DDS, DMD, DPM, DC, OD
––
Medicaid: 30% Medicaid volume (20% for pediatrics)Medicaid: 30% Medicaid volume (20% for pediatrics)
Physicians, NPs, Physicians, NPs, CNMsCNMs, , PAsPAs
in health centersin health centers

The HITECH Act does not award partial The HITECH Act does not award partial
paymentspayments
The EHR reporting period is any The EHR reporting period is any
continuous 90 day period of continuous 90 day period of demonstration in 2011demonstration in 2011
––
Full incentive payment will be awarded for Full incentive payment will be awarded for this 90 day periodthis 90 day period
––
Subsequent payment will require the entire Subsequent payment will require the entire year of meaningful useyear of meaningful use
Defining Meaningful UseDefining Meaningful Use
Criteria is divided into Criteria is divided into Core Core and and Menu Menu setssets––
Must satisfy Must satisfy allall
1515
Core Core measures and measures and 5 of 10 5 of 10
MenuMenu
measuresmeasures
Emergency Department explicit Emergency Department explicit
participant in the EH projectparticipant in the EH project
Aggressive quality reporting programs for Aggressive quality reporting programs for
both ambulatory and hospital projectsboth ambulatory and hospital projects
Defining Meaningful UseDefining Meaningful Use

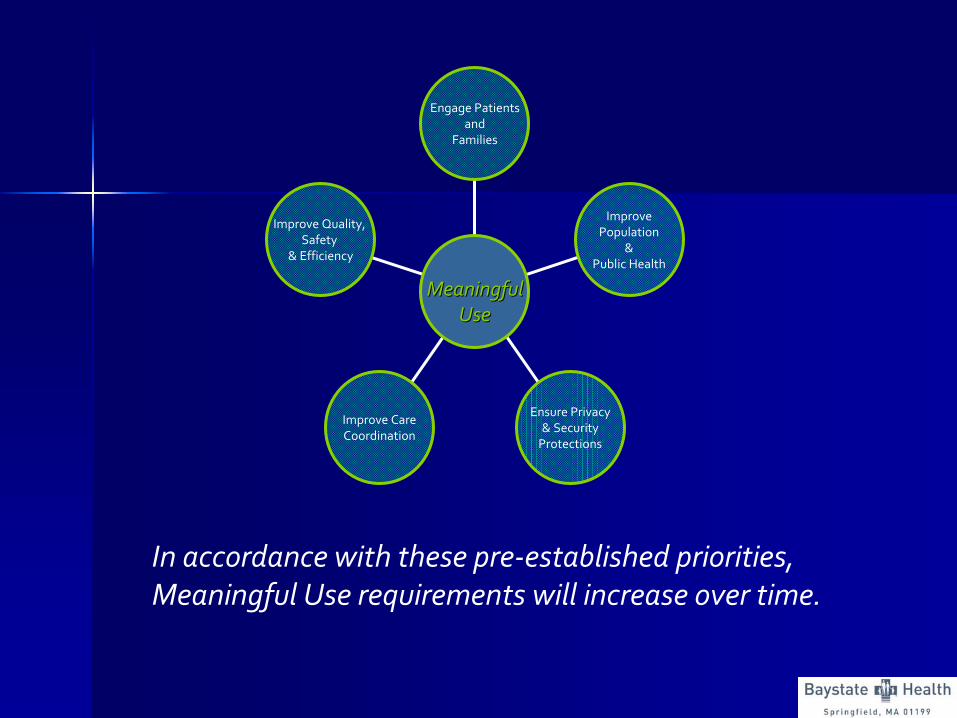
Improve Quality, Safety
& Efficiency
Improve CareCoordination
Ensure Privacy& SecurityProtections
ImprovePopulation
&Public Health
Engage Patientsand
Families
MeaningfulMeaningfulUseUse

Improve Quality, Safety
& Efficiency
MeaningfulMeaningfulUseUse
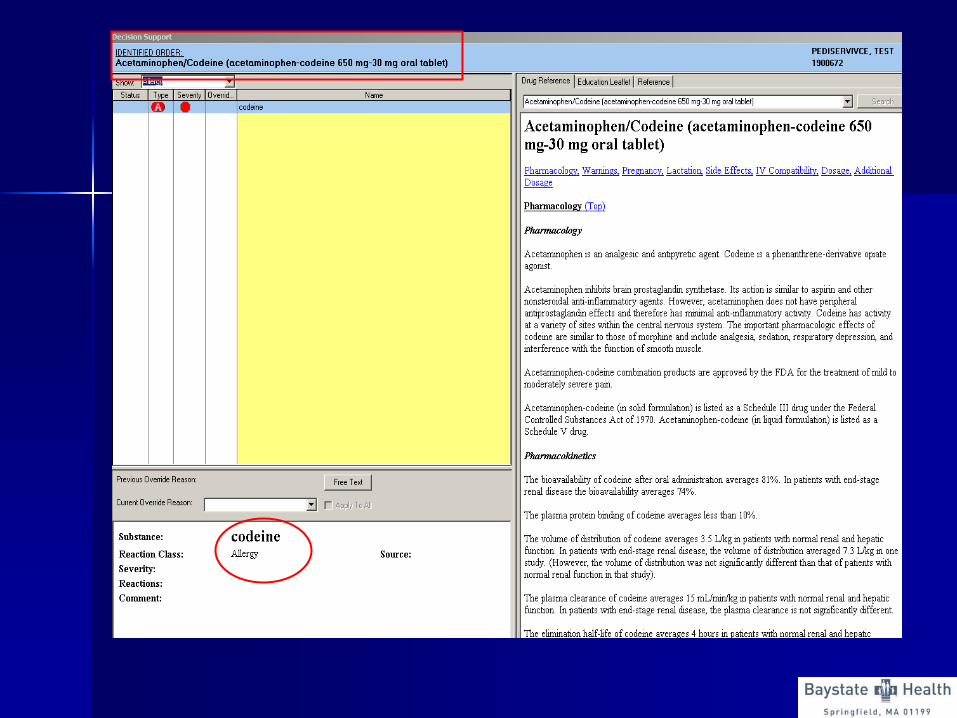
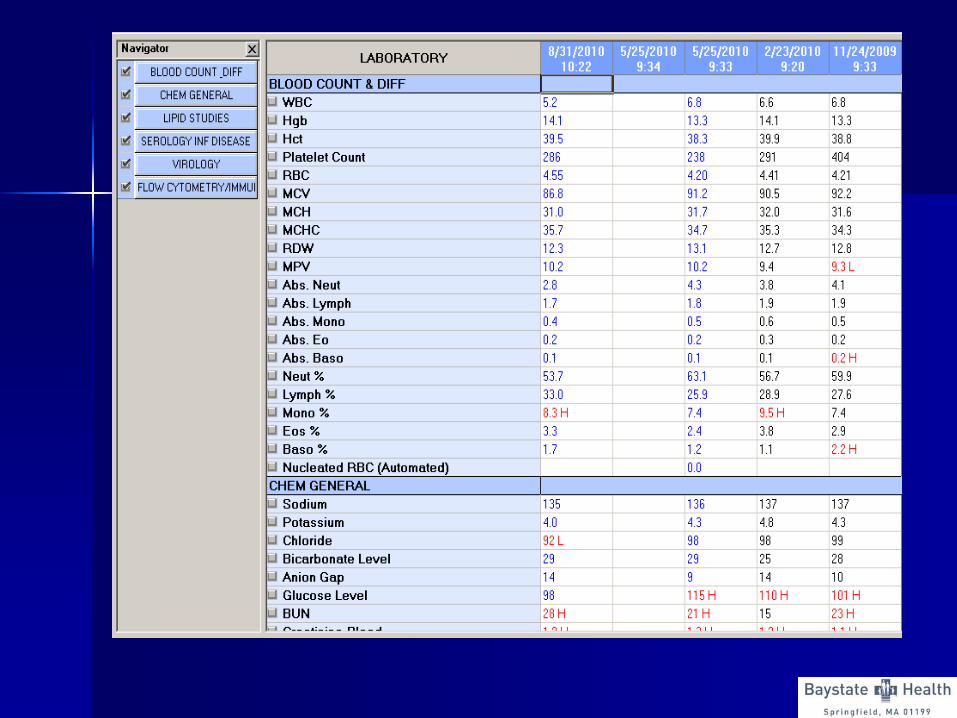
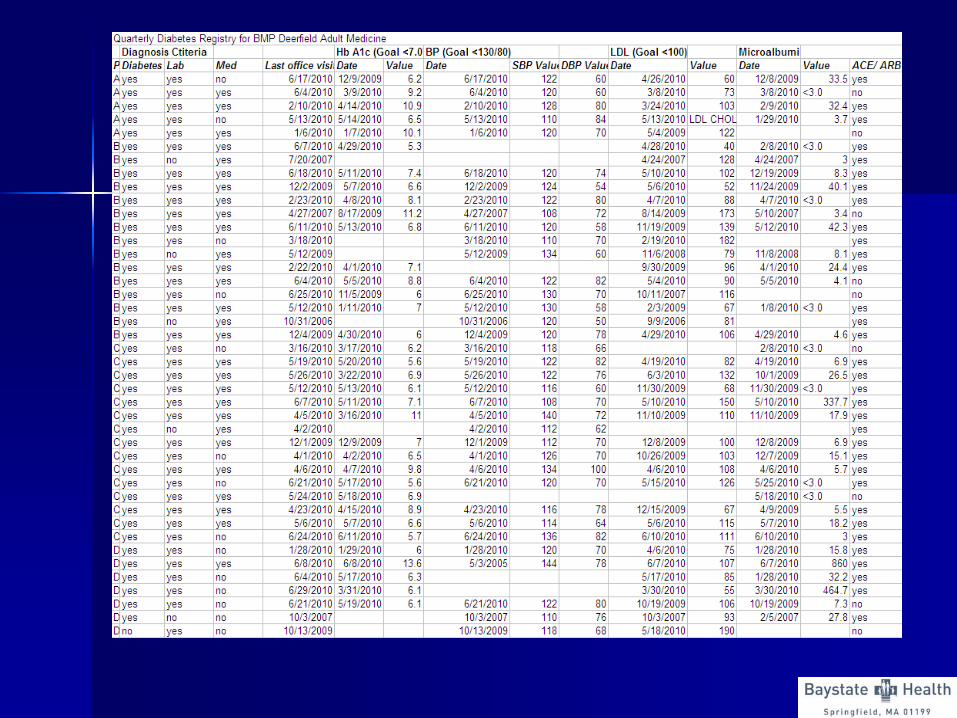
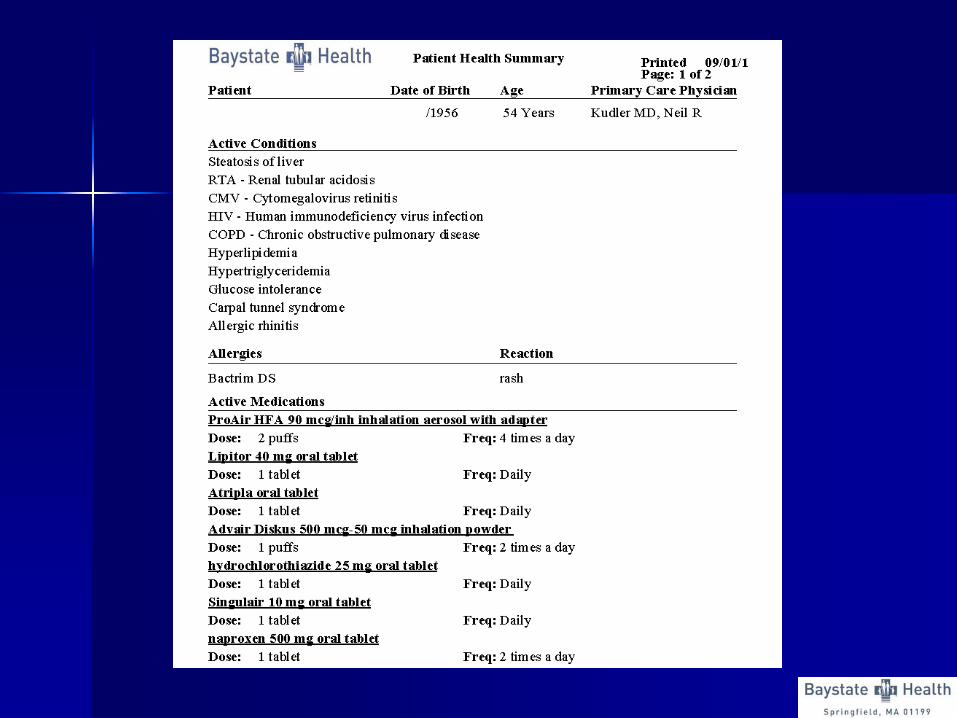
DemographicsProblem ListVital SignsMedication ListAllergy ListePrescribingCPOEDrug CheckingCDS RuleSmoking StatusQuality Reporting
Patient RemindersLab ResultsRegistriesCore: block
Menu: Italics


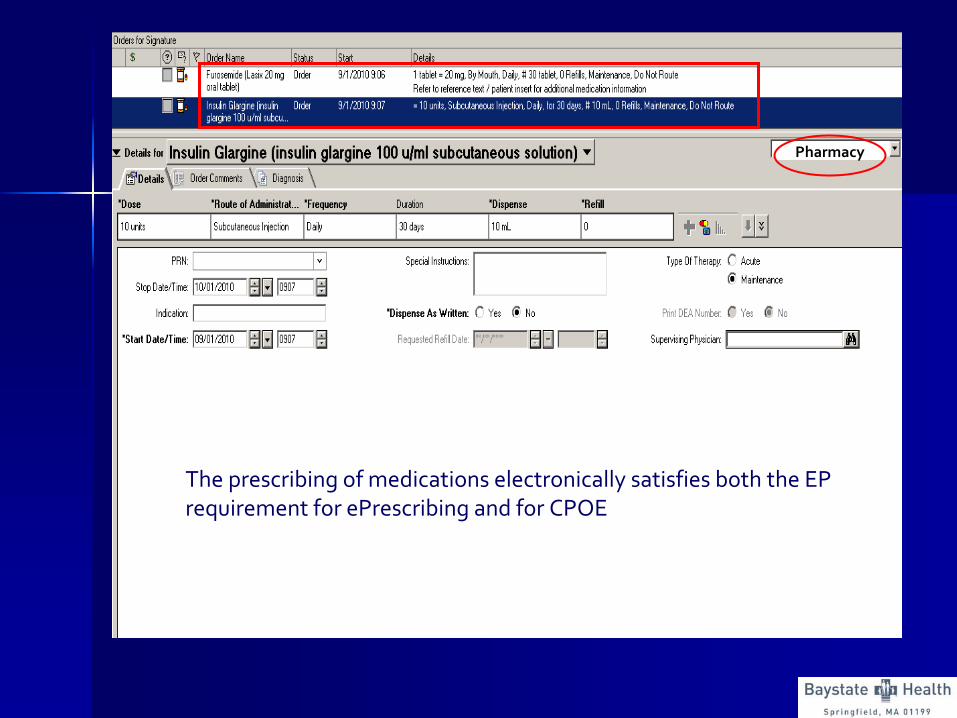
The prescribing of medications electronically satisfies both the
EP requirement for ePrescribing
and for CPOE
Pharmacy
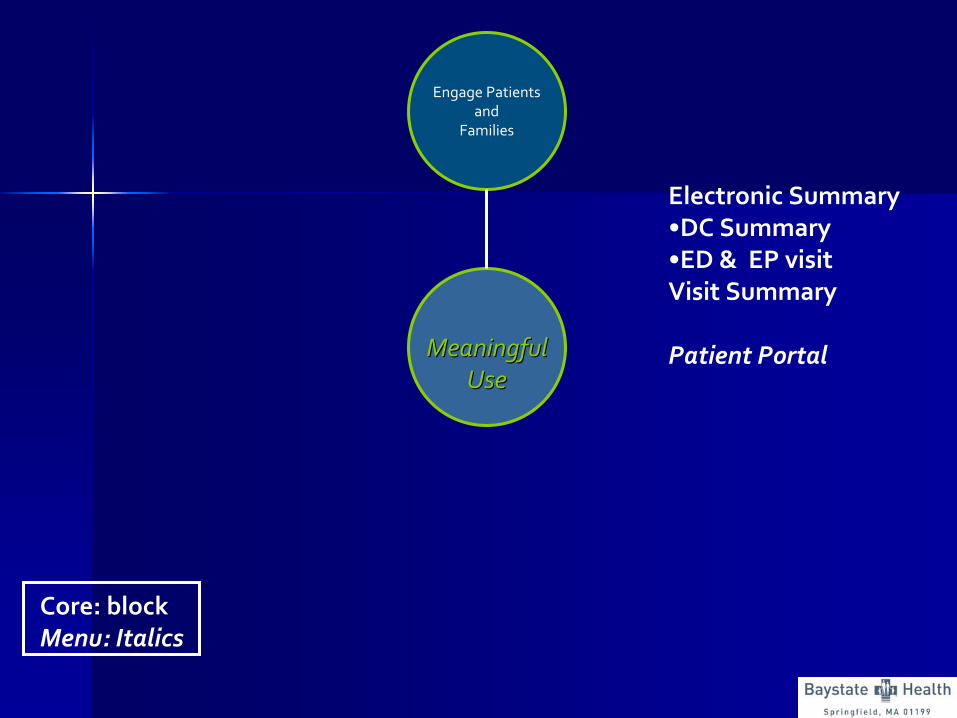
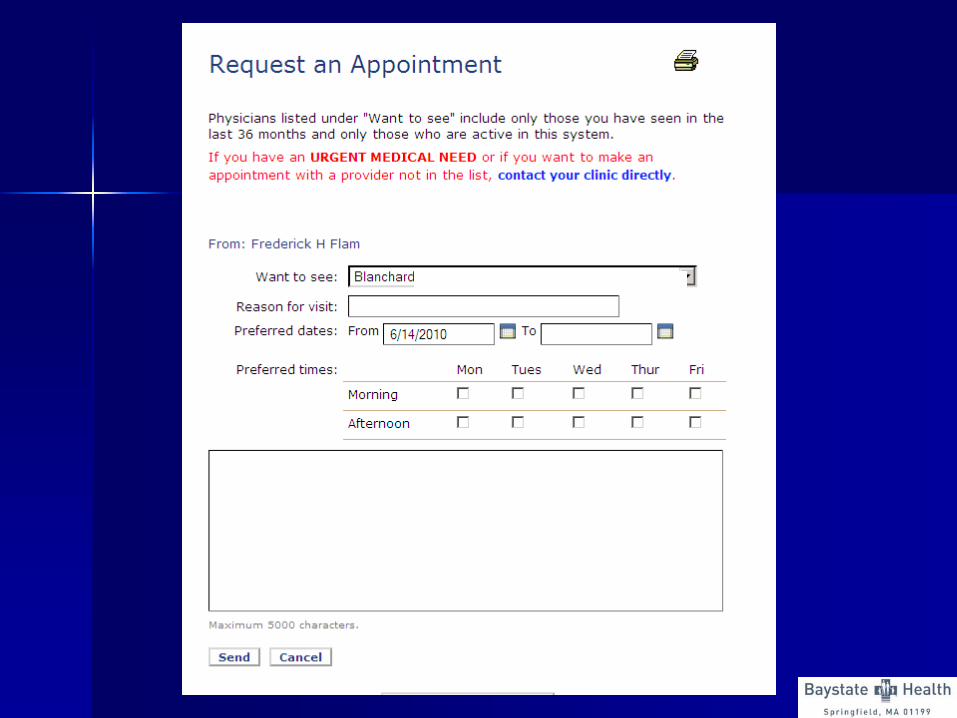
Engage Patientsand
Families
MeaningfulMeaningfulUseUse
Electronic Summary•DC Summary•ED & EP visitVisit Summary
Patient Portal
Core: blockMenu: Italics


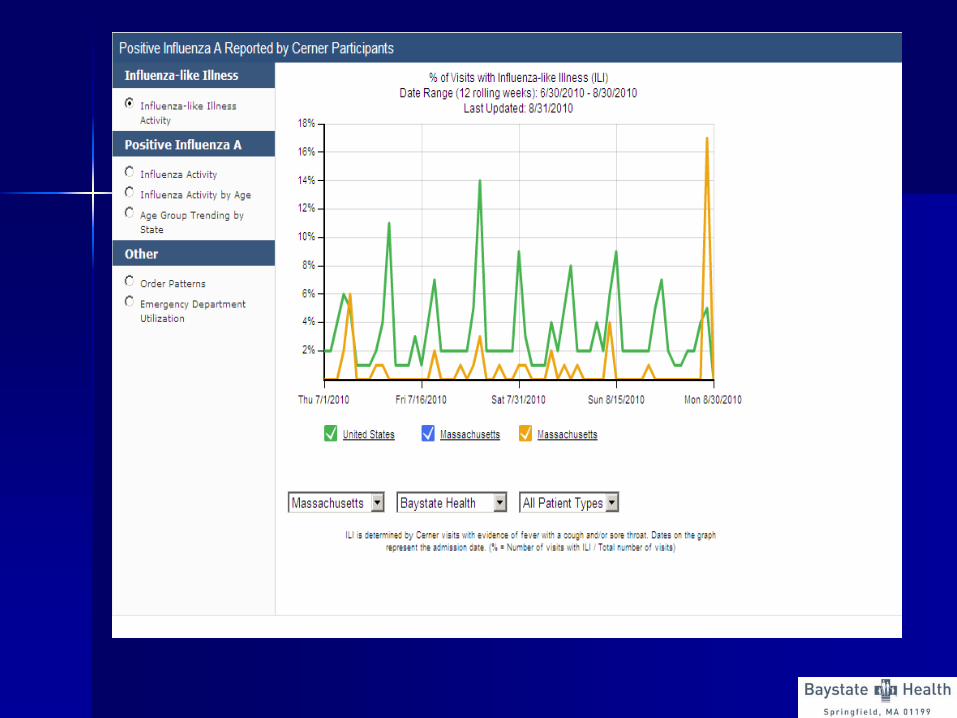
ImprovePopulation
&Public Health
MeaningfulMeaningfulUseUse
Public Health ObjectivesPublic Health ObjectivesImmunizations reportsLabs submission to DPHOutbreak surveillance
Core: blockMenu: Italics
Improve CareCoordination
MeaningfulMeaningfulUseUse
Exchange key clinical information
Summary of care Medication Reconciliation
Core: blockMenu: Italics

Ensure Privacy& SecurityProtections
MeaningfulMeaningfulUseUse
Protecting PatientProtecting PatientHealth Information!Health Information!
Core: blockMenu: Italics
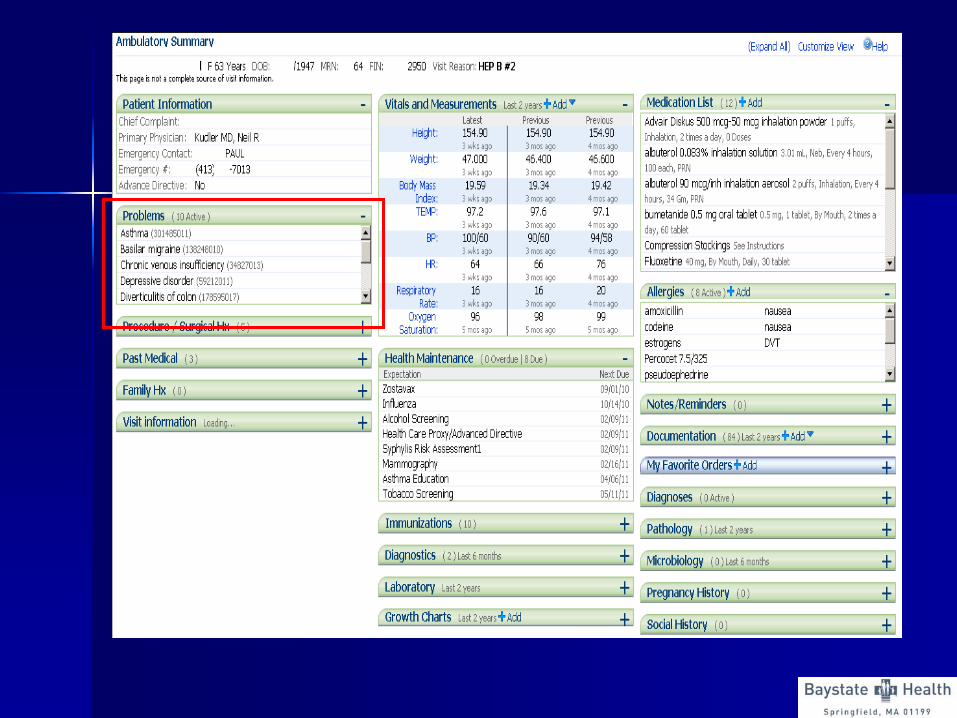
Areas of Focus for PhysiciansAreas of Focus for Physicians
––
Problem List (80% of Problem List (80% of ““unique patientunique patient”” charts) charts)
––
Medication List (80%)Medication List (80%)––
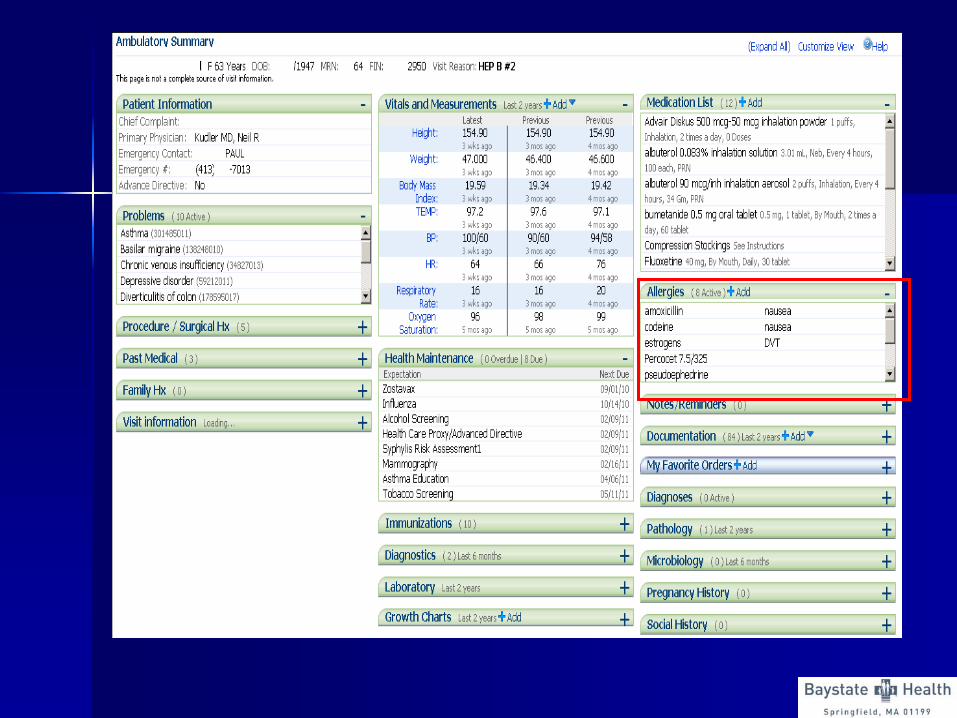
Allergy List (80%)Allergy List (80%)
––
Medication Reconciliation (50%)Medication Reconciliation (50%)––
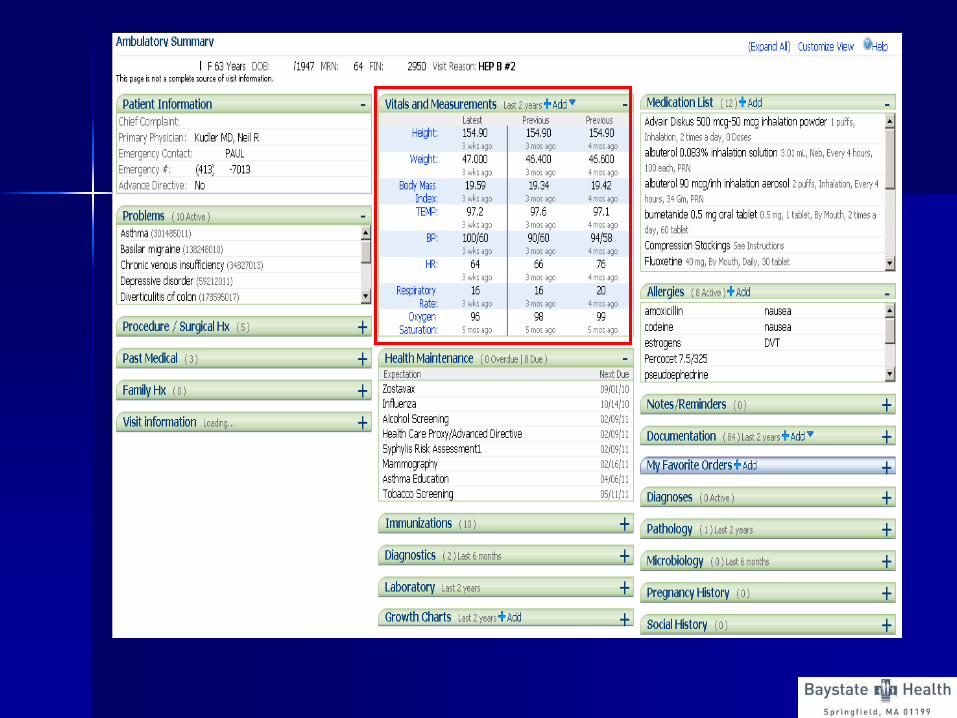
Vital signs (50%)Vital signs (50%)
––
Smoking status (50%)Smoking status (50%)––
Clinical information distributionClinical information distribution
Improve Quality, Safety
& Efficiency
Improve CareCoordination
Ensure Privacy& SecurityProtections
ImprovePopulation
&Public Health
Engage Patientsand
Families
MeaningfulMeaningfulUseUse
In accordance with these pre‐established priorities, Meaningful Use requirements will increase over time.
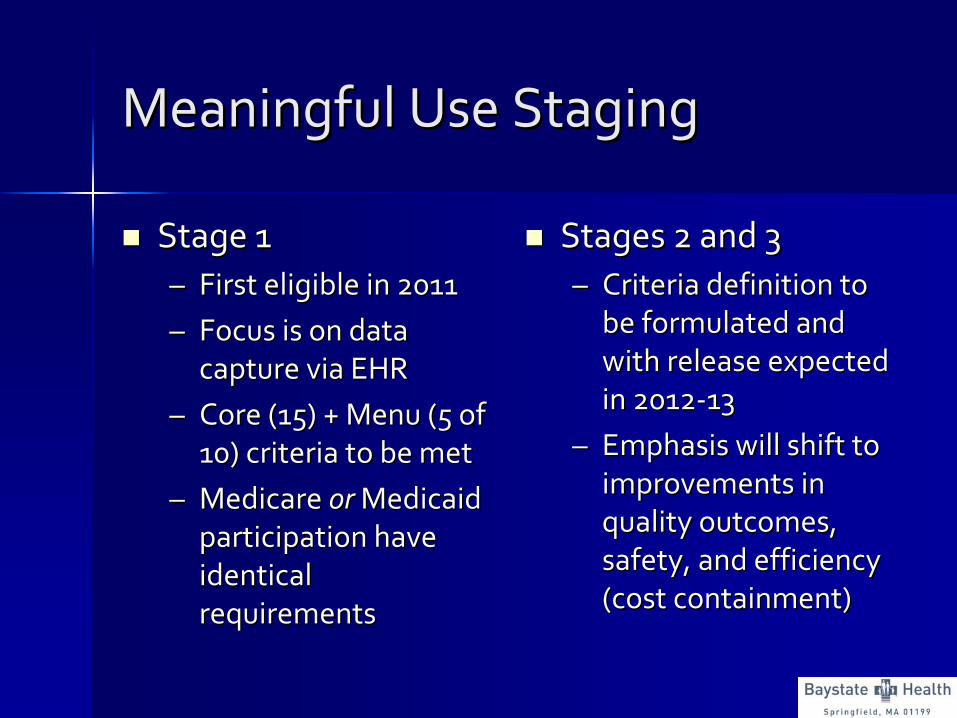
Meaningful Use Staging Meaningful Use Staging
Stage 1Stage 1––
First eligible in 2011First eligible in 2011
––
Focus is on data Focus is on data
capture via EHRcapture via EHR––
Core (15) + Menu (5 of Core (15) + Menu (5 of
10) criteria to be met10) criteria to be met––
Medicare Medicare or or Medicaid Medicaid
participation have participation have
identical identical
requirementsrequirements
Stages 2 and 3Stages 2 and 3––
Criteria definition to Criteria definition to
be formulated and be formulated and
with release expected with release expected
in 2012in 2012‐‐1313––
Emphasis will shift to Emphasis will shift to
improvements in improvements in
quality outcomes, quality outcomes,
safety, and efficiency safety, and efficiency
(cost containment)(cost containment)

Timeline for Stage criteriaTimeline for Stage criteria
First First
QualifyingQualifyingYearYear
FFY2011
FFY2012
FFY2013
FFY2014
FFY 2015
and
Beyond
FFY 2011 Stage 1 Stage 1 Stage 2 Stage 2 TBD
FFY 2012 Stage 1 Stage 1 Stage 2 TBD
FFY 2013 Stage 1 Stage 1 TBD
FFY 2014 Stage 1 TBD
FFY 2015 TBD
Attesting to Meaningful Use Attesting to Meaningful Use
Eligible Providers must attest to CMS that:Eligible Providers must attest to CMS that:––
A certified EHR system is usedA certified EHR system is used––
The EHR achieves functionality requirements and associated The EHR achieves functionality requirements and associated
measuresmeasures
EPs must also attest on quality reporting requirementsEPs must also attest on quality reporting requirements––
Data were generated from EHRData were generated from EHR––
Results are reported in the aggregate (numerators, denominators,Results are reported in the aggregate (numerators, denominators,
and and
exclusions) to CMS (or states for Medicaid project)exclusions) to CMS (or states for Medicaid project)
––
Results are accurateResults are accurate––
Data include all patients to whom the measure appliesData include all patients to whom the measure applies
Quality reporting is not focused on performance or other outcomeQuality reporting is not focused on performance or other outcomes, but s, but
rather on the ability to utilize the EHR to provide accurate andrather on the ability to utilize the EHR to provide accurate and
comprehensive datacomprehensive data

Attesting to Meaningful UseAttesting to Meaningful Use
CMS will establish a webCMS will establish a web‐‐based based
attestation tool by Spring 2011attestation tool by Spring 2011
Attestation will occur once per payment Attestation will occur once per payment
yearyear
Year One of Stage 1 will be any Year One of Stage 1 will be any
continuous 90continuous 90‐‐day demonstration periodday demonstration period
Subsequent reporting will be for the Subsequent reporting will be for the
entire payment (calendar) yearentire payment (calendar) year

Attesting to Meaningful UseAttesting to Meaningful Use
Attestation for EPs who work at multiple Attestation for EPs who work at multiple
locationslocations––
Must have 50% of their total patient Must have 50% of their total patient
encounters at locations where certified EHR encounters at locations where certified EHR technology is availabletechnology is available
––
Base all MU measures only on encounters Base all MU measures only on encounters that occurred at location where certified EHR that occurred at location where certified EHR
technology is availabletechnology is available
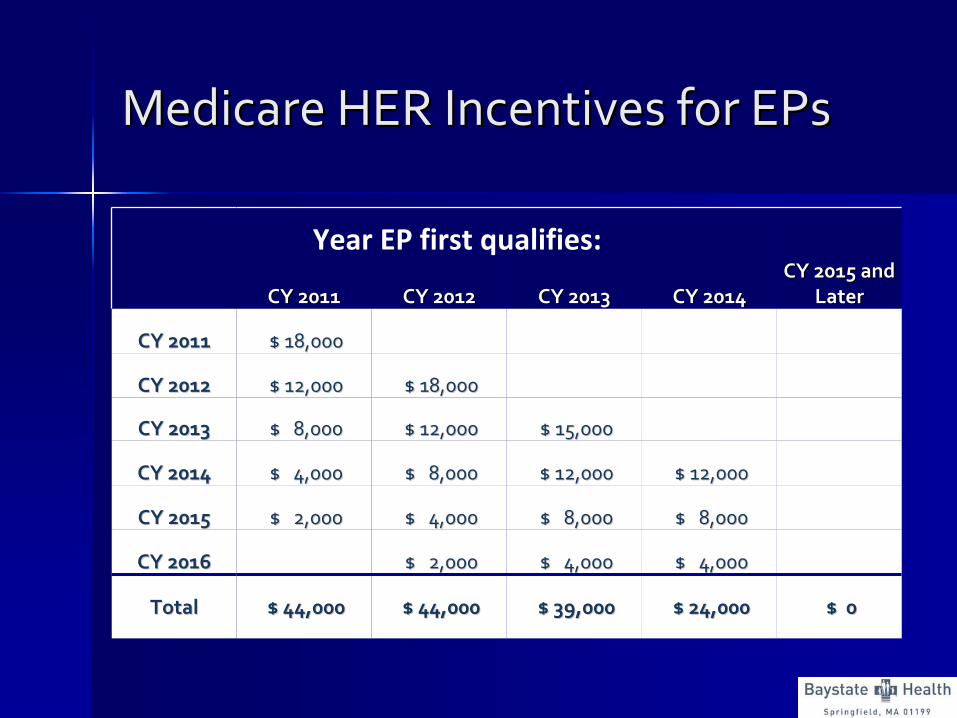
Medicare HER Incentives for EPsMedicare HER Incentives for EPs
CY 2011CY 2011 CY 2012CY 2012 CY 2013CY 2013 CY 2014CY 2014CY 2015 and CY 2015 and
LaterLater
CY 2011CY 2011 $ 18,000 $ 18,000
CY 2012CY 2012 $ 12,000 $ 12,000 $ 18,000 $ 18,000
CY 2013CY 2013 $ 8,000 $ 8,000 $ 12,000 $ 12,000 $ 15,000 $ 15,000
CY 2014CY 2014 $ 4,000 $ 4,000 $ 8,000 $ 8,000 $ 12,000 $ 12,000 $ 12,000 $ 12,000
CY 2015CY 2015 $ 2,000 $ 2,000 $ 4,000 $ 4,000 $ 8,000 $ 8,000 $ 8,000 $ 8,000
CY 2016CY 2016 $ 2,000 $ 2,000 $ 4,000 $ 4,000 $ 4,000 $ 4,000
TotalTotal $ 44,000 $ 44,000 $ 44,000 $ 44,000 $ 39,000 $ 39,000 $ 24,000 $ 24,000 $ 0 $ 0
Year EP first qualifies:
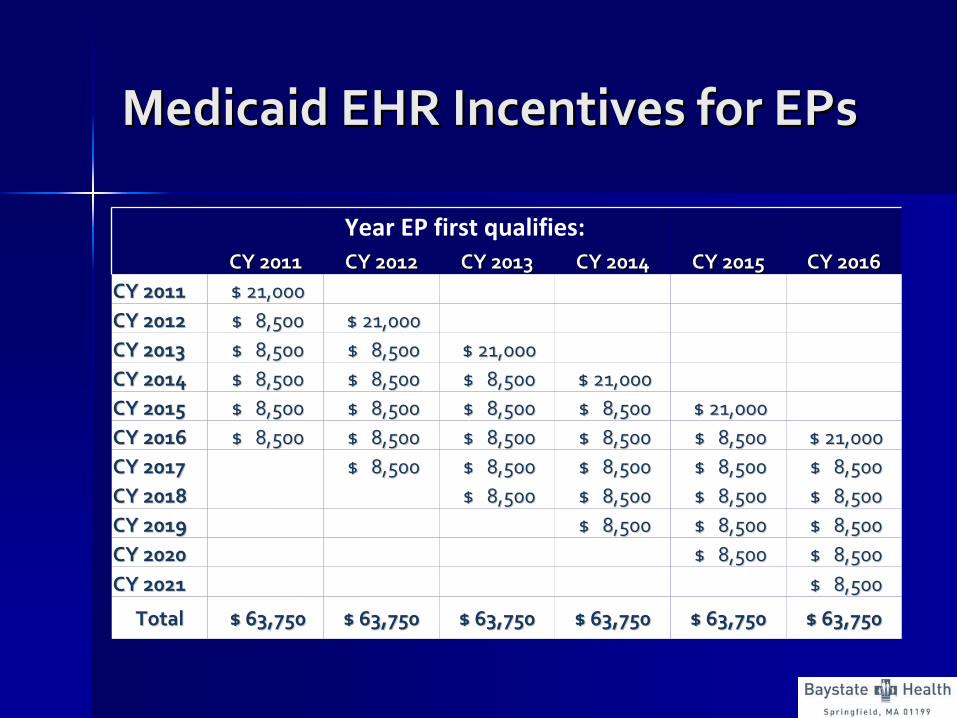
Medicaid EHR Incentives for EPsMedicaid EHR Incentives for EPs
CY 2011CY 2011 CY 2012CY 2012 CY 2013CY 2013 CY 2014CY 2014 CY 2015CY 2015 CY 2016CY 2016CY 2011CY 2011 $ 21,000 $ 21,000 CY 2012CY 2012 $ 8,500 $ 8,500 $ 21,000 $ 21,000 CY 2013CY 2013 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 21,000 $ 21,000 CY 2014CY 2014 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 21,000 $ 21,000 CY 2015CY 2015 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 21,000 $ 21,000 CY 2016CY 2016 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 21,000 $ 21,000 CY 2017CY 2017 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 CY 2018CY 2018 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 CY 2019CY 2019 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 $ 8,500 CY 2020CY 2020 $ 8,500 $ 8,500 $ 8,500 $ 8,500 CY 2021CY 2021 $ 8,500 $ 8,500
TotalTotal $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750 $ 63,750
Year EP first qualifies:

How can coders assist in the How can coders assist in the success of the EHR?success of the EHR?
Data integrity auditsData integrity audits––
DemographicsDemographics
––
Vital signs including height and BMIVital signs including height and BMI––
Use of data within documentationUse of data within documentation
Structured lab entryStructured lab entry
““CloningCloning””
of clinical notesof clinical notes

How can coders assist in the How can coders assist in the success of the EHR?success of the EHR?
Teach me!Teach me!
How can coders best How can coders best
collaborate with clinicians to create the collaborate with clinicians to create the best electronic health record in order to best electronic health record in order to meet the highest goals for quality patient meet the highest goals for quality patient
care?care?