Alveolar Capillary Unit
44
The Alveolar- Capillary Unit Dimitar Sajkov MD, DSc, PhD, FRACP
description
Transcript of Alveolar Capillary Unit

The Alveolar- Capillary Unit
Dimitar SajkovMD, DSc, PhD, FRACP

Alveolar - Capillary Unit

Alveolar - Capillary Unit
Complex cardiovascular system with multiple functions: Gas exchange Oxygen sensing and redistribution of
pulmonary blood flow Non-respiratory functions
physical and chemical filteractivating and endocrine functionsfluid-balance regulator

Alveoli
Small, thin-walled, inflatable sacs at end of bronchiolesSurrounded by a jacket of pulmonary capillariesProvide thin barrier and enormous surface area for gas exchange by diffusionType II cells secrete surfactant

Alveolar - Capillary Unit

Alveolar - Capillary Unit
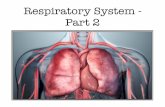
A scanning electron micrograph of the alveoli.
Humans have a thin layer of about 700 million alveoli within their lungs.
This layer is crucial in the process called respiration, exchanging O2 and CO2 with the surrounding blood capillaries.


Alveolar - Capillary Unit
Structure

Alveolar - Capillary Unit
1 - Capillary
2 - Alveolus
3 - RBC
4 - Endothelium
5 - Basal Membrane
3
4
5

Gas Exchange

Gas Exchange - Diffusion

Gas Exchange
Partial Pressures of O2 and CO2 in the
body (normal, resting conditions): Alveoli
PO2 = 100 mm Hg
PCO2 = 40 mm Hg
Alveolar capillaries Entering the alveolar capillaries
PO2 = 40 mm Hg (relatively low because this blood has just
returned from the systemic circulation & has lost much of its O2)
PCO2 = 45 mm Hg (relatively high because the blood returning
from the systemic circulation has picked up CO2)

Gas Exchange
While in the alveolar capillaries, the diffusion of gasses occurs: O2 diffuses from the alveoli into
the blood & CO2 from the blood into the alveoli. Leaving the alveolar capillaries
PO2 = 100 mm Hg
PCO2 = 40 mm Hg

Gas Exchange
Blood leaving the alveolar capillaries returns to the left atrium & is pumped by the left ventricle into the systemic circulation. This blood travels through arteries & arterioles and into the systemic, or body, capillaries. As blood travels through arteries & arterioles, no gas exchange occurs.
Entering the systemic capillaries
PO2 = 100 mm Hg
PCO2 = 40 mm Hg
Body cells (resting conditions)
PO2 = 40 mm Hg
PCO2 = 45 mm Hg

Because of the differences in partial pressures of O2 & CO2 in the systemic capillaries & the body cells, O2 diffuses from the blood & into the cells, while CO2 diffuses from the cells into the
blood. Leaving the systemic capillaries
PO2 = 40 mm Hg
PCO2 = 45 mm Hg
Blood leaving the systemic capillaries returns to the heart (right atrium) via venules & veins (and no gas exchange occurs while blood is in venules & veins). This blood is then pumped to the lungs (and the alveolar capillaries) by the right ventricle.
Gas Exchange

Gas Exchange

Non-Respiratory Functions of the Lung
Physical Filter
Chemical Filter
Activating Organ
Endocrine Organ
Fluid Balance regulator

Physical Filter
All particles larger than red blood cells (e.g. bubbles, clots, fat cells, fibrin)
Role in removing damaged white cells
Rapidly cleared by phagocytosis and proteolytic enzymes

Chemical Filter (John Vane’s theory)
Locally Acting (removed)
serotonin (90%) noradrenaline (35%) acetylcholine (95%) bradykinin (90%) angiotensin I (30%) PGE2 (95%)
PGF2a (95%) leukotrienes (95%) ATP, AMP (90+%)
Circulating (not affected)
dopamine adrenaline histamine vasopressin angiotensin II PGA2
substance P oxytocin eledoisin

Compliance
Measures the elastic characteristics, or “stretchiness” of the lungVaries with the degree of lung inflation and is different on inspiration or expiration
C = V/PDescribes how much lung inflation can be achieved by a unit pressure increase

Compliance

Surface Tension and Compliance
Kurt von Neergard (1929) suggested that ST was less than that of water and that surface active substances were present

Surface Tension
75% of tendency of the lung to collapse is due to surface tension (ST) at the gas-liquid interface

Surface Tension in Lung Mechanics
A B
r = 1 cmr = 10 m = = 10 x 10-4 cm
Assume ST is constant at 72 dyne/cm
Law of Laplace: P = 2T/r
A) P = 2T/r = 2 x 72/1 = = 144 dyne/cm2
B) P = 2T/r = 2 x 72/10-3 = = 144,000 dyne/cm2 = = 80 cmH2O
1000 X the pressure is required to maintain B than A

Alveolar Surface Tension Forces
Attraction of liquid molecules produces surface tension (ST), which draws liquids closer together resists force that would increase the area of the
surface
ST is reduced by surfactant

Surfactant
Phospholipid produced by type II alveolar cells surface tension in alveoli total lung compliance lung “stability”

Reduces “stiffness” of the lungsProtects patency of small airwaysPrevents total collapse of the alveoli (i.e. stabilises alveoli)Reduces work of breathingPrevents small alveoli emptying into larger ones
Roles of Surfactant

Roles of Surfactant
Prevents movement of fluid into the alveolus and keeps lungs dry (osmotic > hydrostatic pressure)
Acts as an anti-glueStimulates Lung host defence system: Immunosuppresses Acts as a chemotactic agent Opsonises bacteria Enhances mucous clearance

Surfactant Composition
Phospholipids 80% dipalmitoyphosphatidylcholine (DPCC) 60% Phosphatidylglycerol/ethanolamine/inositol 20%
Neutral Lipids 10% Mostly Cholesterol
Surfactant Proteins 10% SP-A; SP-D: hydrophilic SP-B; SP-C: hydrophobic
L/S ratio: predictor of foetal lung maturity
L – lecithinS – Sphyngomyelin

Surfactant Proteins
SP-A: Hydrophilic formation of tubular lattice regulatory function defence function
SP-B: Hydrophobic re-formation of layer after compression
SP-C: Hydrophobic spreading function
SP-D: Hydrophilic regulatory function defence function

Surfactant Metabolism
Produced, stored and secreted by type II alveolar cells and Clara cells
Half-time for turnover 5 - 10 hours
90% recycled by type II pneumocytes
10% cleared by alveolar macrophages
SP-A is primary regulator of metabolism and lung defence mechanisms

Type II Alveolar Cell

Surfactant

Loss of Surfactant Function
Inhibition by serum proteins (albumin), fibrinogen, meconium, bilirubin and degradation products
Inactivation by O2 radicals and enzymes (phospholipases)
Decreased pool size due to lung injury
Mechanical factors (eg. Alveolar collapse)
Enhanced conversion to small aggregate forms of lipids

Interdependence

Interdependence

The Foetal Lung
Airways formed by week 16
Alveoli start to form ~ at week 20; ~20 million alveoli present at birth
Alveolar type II cells appear ~ at week 24
Foetal lung fluid (5 ml/kg/hr) maintains lung at FRC [high Cl-, low HCO3 and protein c.f. plasma]
Foetal breathing: development of neural control

Amniocentesis: phosphatidylcholine increases rapidly after ~ 33 wk
Lecithin/Sphingomyelin ratio + 2.0 at ~ 35 wk
80% of infants < 30 wk have RDS
45% of infants < 32 wk have RDS
At birth: adrenaline activates Na channels in type II cell
(vasopressin, cortisol and T3 are also involved); aquaporins: water channel-forming proteins
The Foetal Lung

Not conducive to gas exchange Thick blood gas barrier Low compliance Immature epithelial cells Low surfactant levels Small area for gas exchange Poorly vascularized High resistance to blood flow
Conducive to gas exchange Thin blood gas barrier Highly compliant Mature epithelial cells Adequate surfactant Large area for gas exchange Highly vascular Low resistance to blood flow
Immature lung
Mature lung

Surfactant - Acute Effects
Oxygenation improvement
Improved lung compliance
More uniform lung inflation
inflammation and implementation of lung defence mechanisms

Acute Lung Injury: A Condition Involving Impaired Oxygenation
Defined as: A ratio of the partial pressure of arterial
oxygenation (PaO2) to the fraction of inspired oxygen (FiO2) that is < 300 regardless of whether or how much positive end-expiratory pressure is used to provide respiratory support
Bilateral pulmonary infiltrates on chest radiograph Pulmonary Artery Occlusion Pressure of < 18
mmHg or no clinical evidence of elevated left atrial pressure
When the injury is “severe”, we have recognizable clinical features of ARDS.

ARDS – Predisposing Factors
Direct InjuryInhalation Injury (i.e. Burns) Aspiration (i.e. chemical pneumonitis)
Indirect InjuryBacterial Sepsis (i.e. endotoxemia) Pancreatitis
With some of these “predisposing conditions”, the risk of A.R.D.S. is substantial
Gastric Aspiration & Sepsis: Overall Mortality of 30 - 40 %

ARDS - Management
Measures to correct the abnormality in vascular permeability or to limit the degree of inflammatory reaction present in ARDS, do not exist.Clinical management involves primarily supportive measures aimed at maintaining cellular and physiologic function, while the acute lung injury resolves.What cellular functions are you trying to maintain ? Alveolar Gas Exchange Organ Perfusion Aerobic Metabolism

Alveolar – Capillary Unit