Alternatives to Incarceration for Addicted and Mentally Ill ...
52
NEOMED TEMPLATE Alternatives to Incarceration for Addicted and Mentally Ill Populations County Commissioners Association of Ohio June 10, 2015
Transcript of Alternatives to Incarceration for Addicted and Mentally Ill ...
NEOMED TEMPLATE
Alternatives to Incarceration for Addicted and Mentally Ill Populations
County Commissioners Association of Ohio
June 10, 2015
PRESENTERS:
Ruth H. Simera, M.Ed., LSW Program Administrator
Criminal Justice Coordinating Center of Excellence
Northeast Ohio Medical University
Scott A. Sylak, MPA, LICDC-CS Executive Director
Mental Health & Recovery Services Board of Lucas County
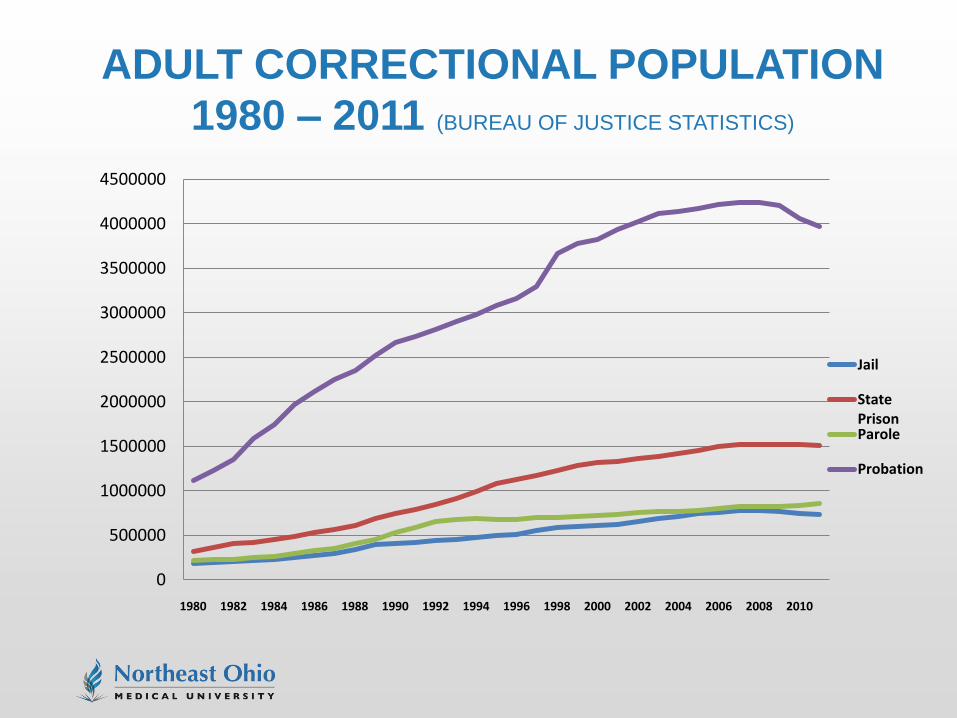
ADULT CORRECTIONAL POPULATION
1980 – 2011 (BUREAU OF JUSTICE STATISTICS)
0
500000
1000000
1500000
2000000
2500000
3000000
3500000
4000000
4500000
1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Jail
StatePrisonParole
Probation
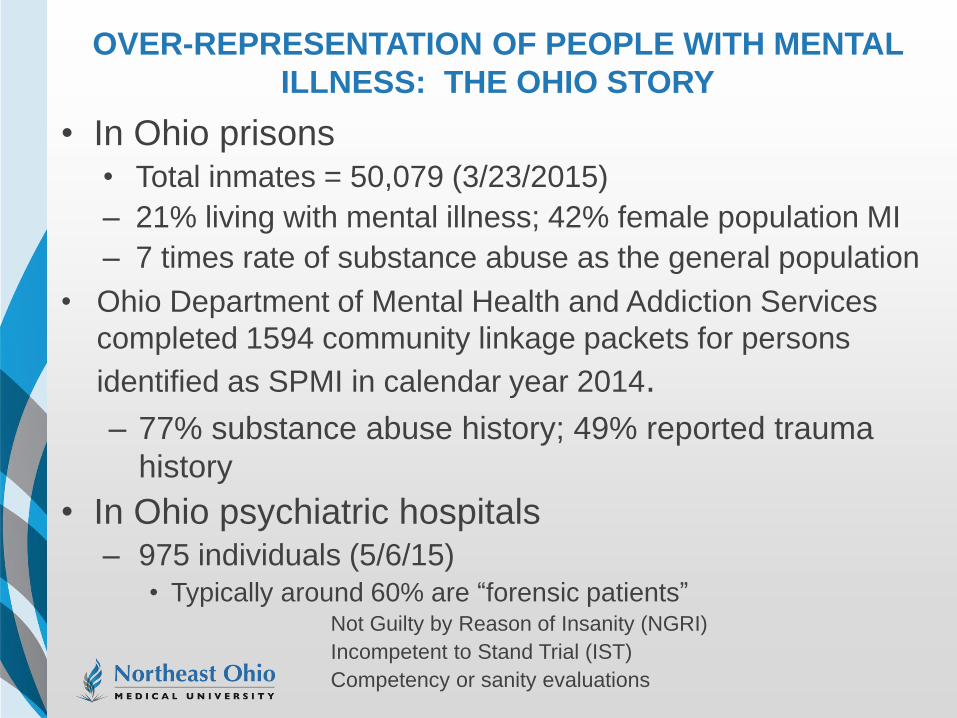
OVER-REPRESENTATION OF PEOPLE WITH MENTAL
ILLNESS: THE OHIO STORY
• In Ohio prisons • Total inmates = 50,079 (3/23/2015)
– 21% living with mental illness; 42% female population MI
– 7 times rate of substance abuse as the general population
• Ohio Department of Mental Health and Addiction Services
completed 1594 community linkage packets for persons
identified as SPMI in calendar year 2014.
– 77% substance abuse history; 49% reported trauma
history
• In Ohio psychiatric hospitals – 975 individuals (5/6/15)
• Typically around 60% are “forensic patients” Not Guilty by Reason of Insanity (NGRI)
Incompetent to Stand Trial (IST)
Competency or sanity evaluations
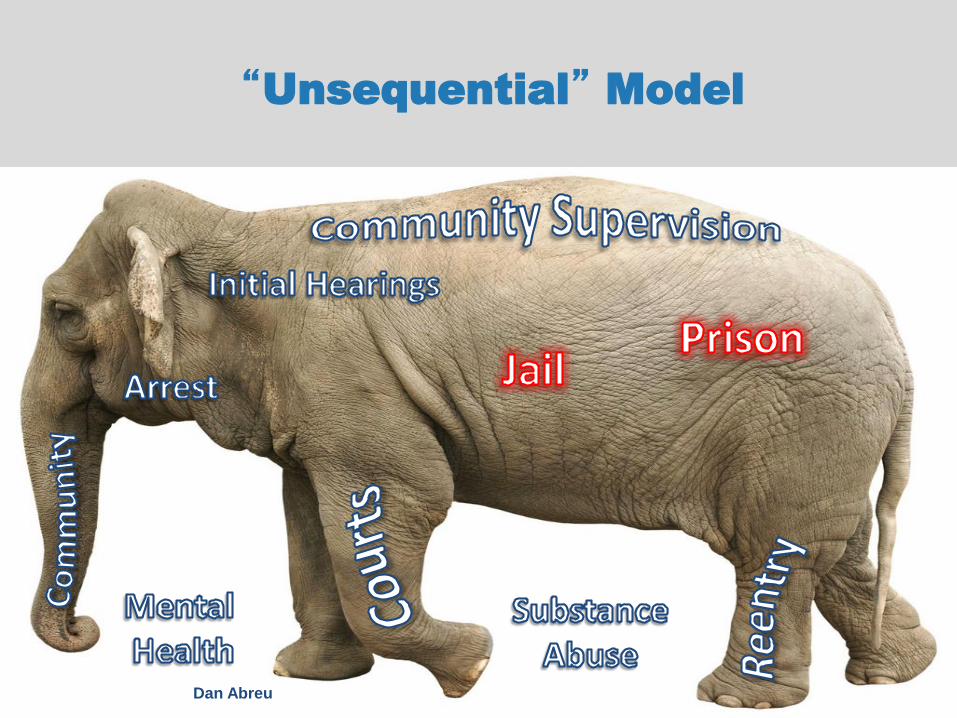
“Unsequential” Model
Dan Abreu
A SYSTEMATIC APPROACH TO THE
CRIMINALIZATION PROBLEM
• There is no single solution to the problem we are
calling “criminalization of people with mental illness”
– People move through the criminal justice
system in predictable ways
– The problem must be attacked from multiple levels
– The Sequential Intercept Model
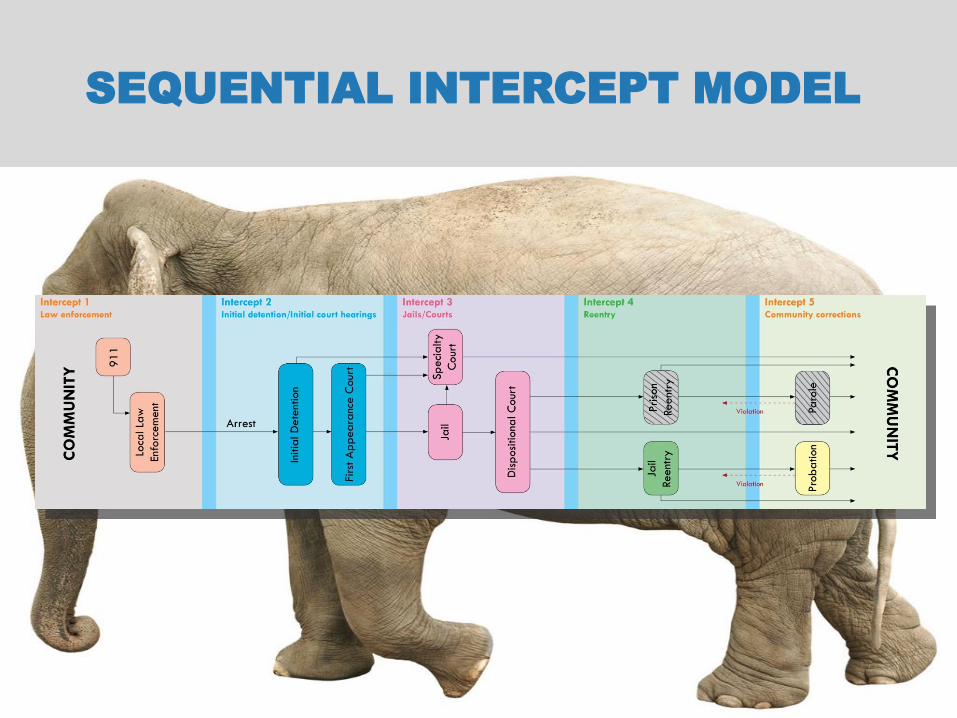
SEQUENTIAL INTERCEPT MODEL
Sequential Intercept Mapping
Problem: In multiple systems; expensive,
high service users
Focus
• Men and women with…
–Serious mental illness, and often
Co-occurring substance use disorders
– Involved in the criminal justice system
Solution: Cross-system Coordination & Collaboration

Goals
Promote & support recovery
Provide safety, quality of life for all
Keep out of jail, in treatment
Provide constitutionally adequate
treatment in jail
Link to comprehensive, appropriate, and
integrated community-based services
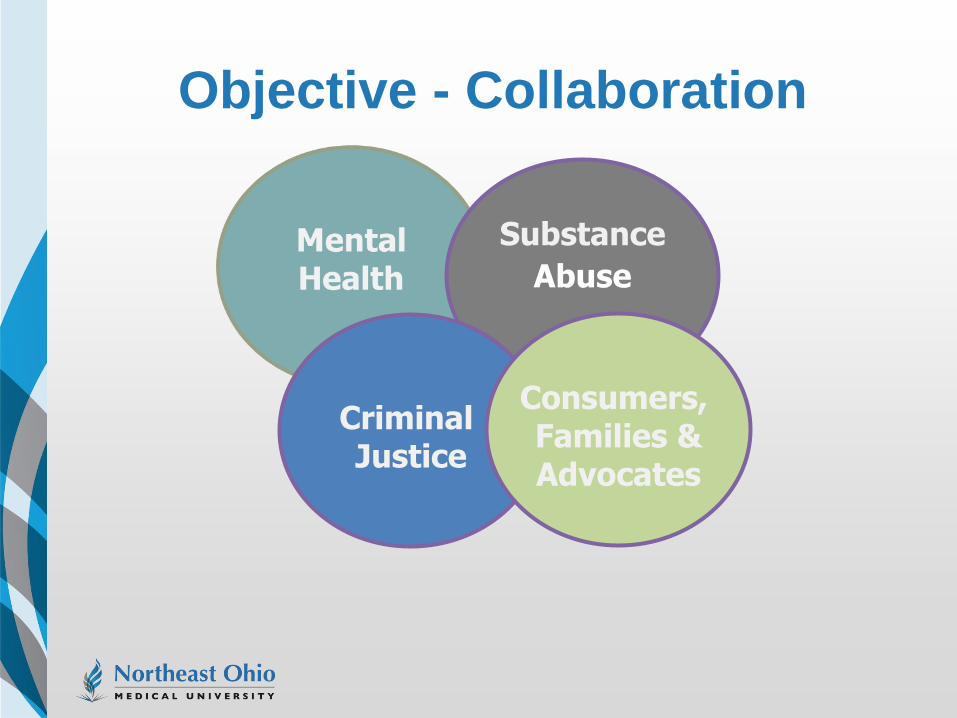
Objective - Collaboration
Substance
Abuse
Criminal Justice
Consumers, Families & Advocates
Challenges to Collaboration
Funding “silos”
Limited resources
System “cultures”
Benefits of Effective Collaboration
Community Collaboration + Services
Integration =
service retention
stability in the community
public safety
Effective Diversion
A different way of doing business for Criminal Justice, the Mental Health System,
consumers and their families
Additional Strategies
Shared vision & direction
Data
Evidence-based & promising
practices
Funds: creative use
NEOMED TEMPLATE
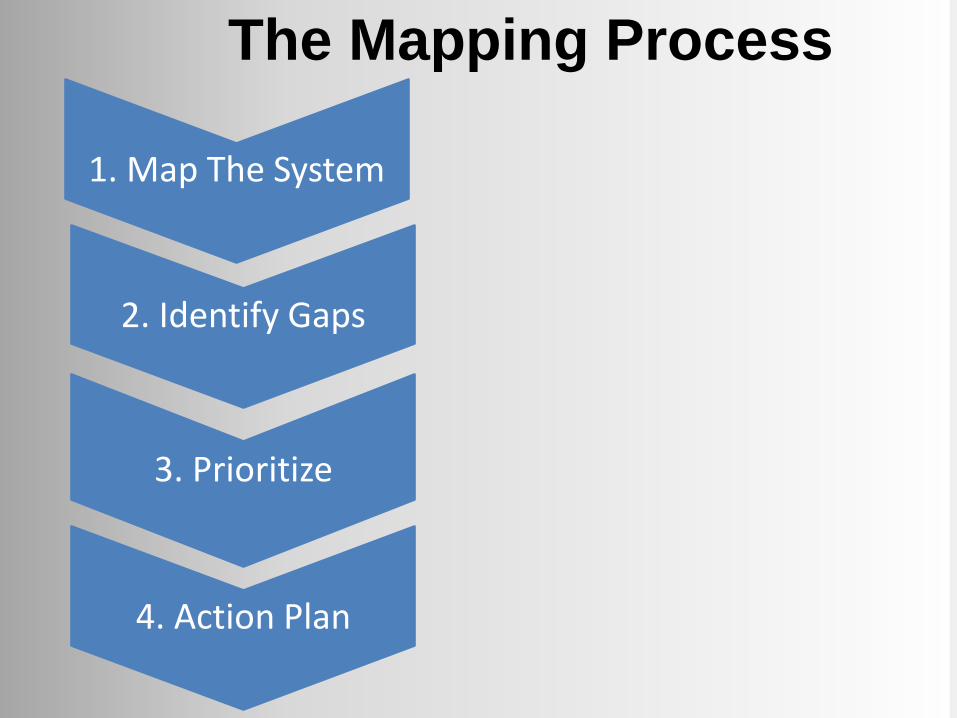
The Mapping Process
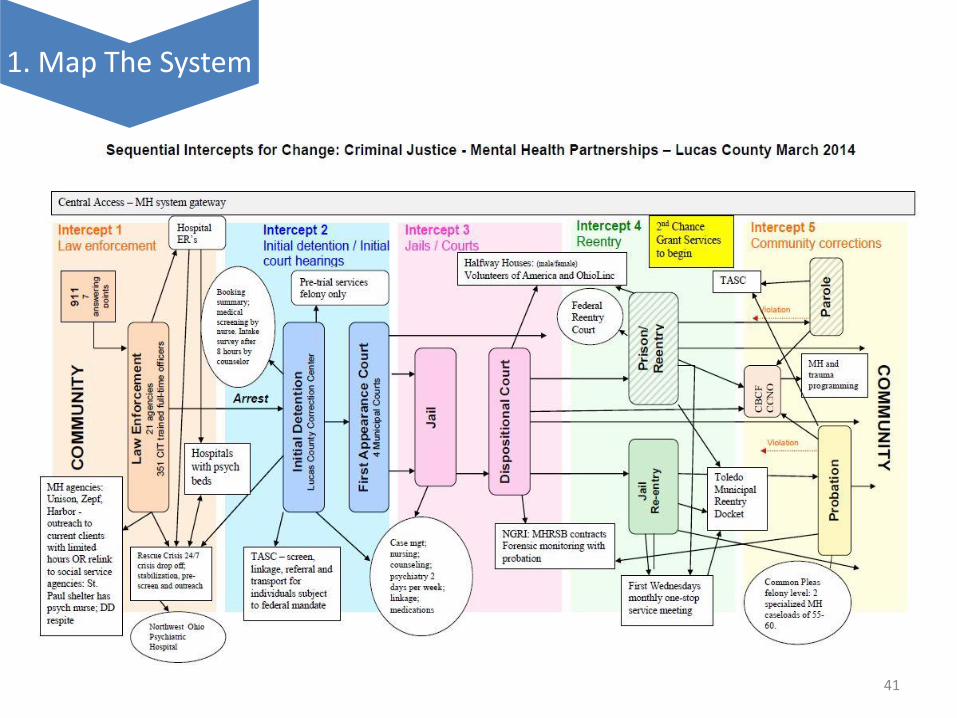
1. Map The System
2. Identify Gaps
3. Prioritize
4. Action Plan
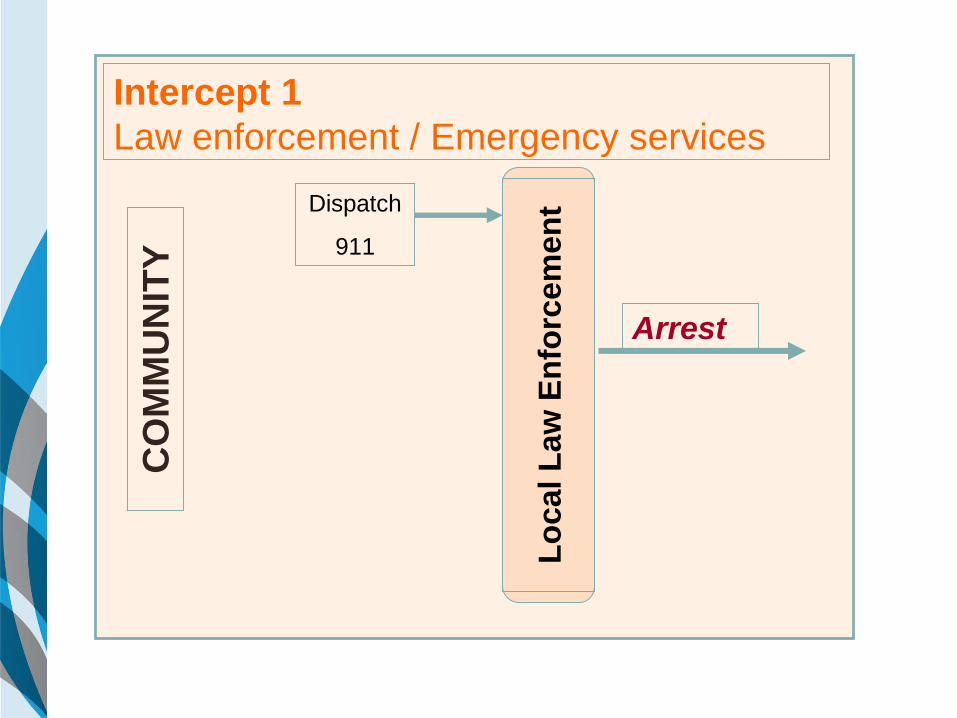
Intercept 1
Law enforcement / Emergency services C
OM
MU
NIT
Y
Dispatch
911
Lo
cal L
aw
En
forc
em
en
t
Arrest
CHALLENGES – INTERCEPT 1
• 7-14% Law Enforcement encounters involve
individuals with mental illness
• No where to take people other than jail
• Lack of training – mental illness information, de-
escalation
• Poor outcomes
• Arrest
• Use of force and unsafe responses
• Further disruption of treatment
• Injury, death
SPECIALIZED CRISIS RESPONSE SITES:
BASIC PRINCIPLES
• Identifiable and centralized for law enforcement
• “Police-friendly” policies and procedures
• Streamlined intake
• “No refusal” policy
• Legal foundations (Ohio Revised Code, HIPAA)
• Innovative and extensive cross-training
• Linkages to community services – Even for those who do not meet criteria for inpatient
commitment
(Steadman, et al, 2001)
INTERCEPT 1: INTERCEPTING AT FIRST CONTACT
POLICE & EMERGENCY SERVICES (DEANE, ET AL, 1999)
• Police-based specialized police response – Front line police response
– Specialized training/support system
– Example: Memphis Crisis Intervention Team (CIT)
• Police-based specialized mental health response – MH professionals employed by police dept.
– Example: Community Service Officers in Birmingham AL
• Mental Health-based specialized response – Mobile crisis teams
– Ohio County Examples: Clermont, Portage, Lucas,
Butler (hybrid)
Intercept I
19
CO
MM
UN
ITY
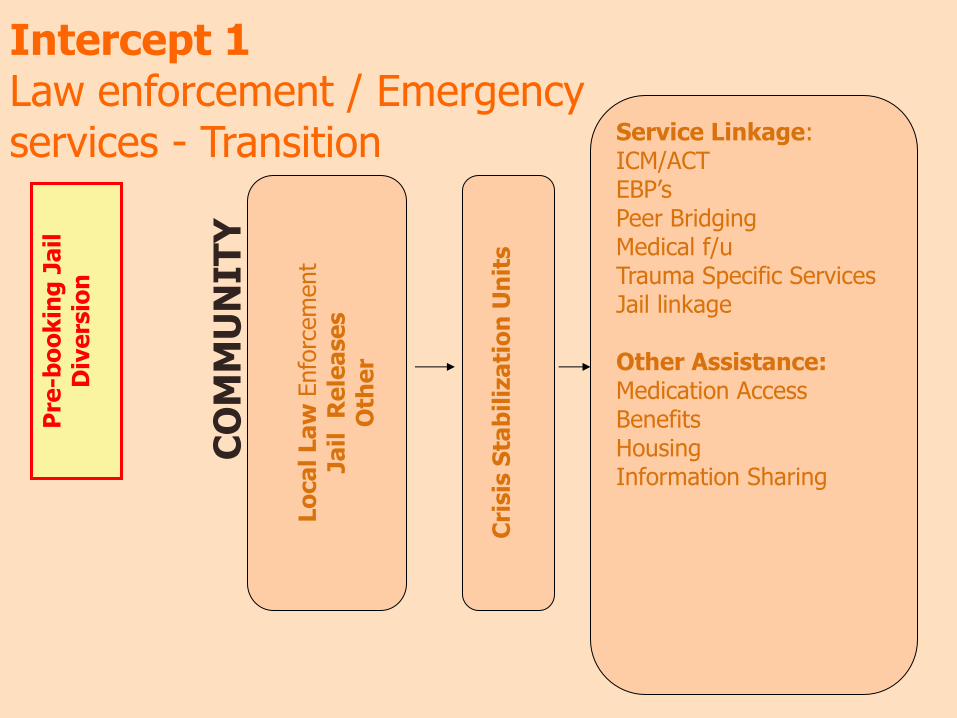
Intercept 1 Law enforcement / Emergency services - Transition
Lo
ca
l La
w E
nfo
rcem
ent
Ja
il R
ele
ase
s
Oth
er
Cri
sis
Sta
bil
iza
tio
n U
nit
s
Service Linkage: ICM/ACT EBP’s Peer Bridging Medical f/u Trauma Specific Services Jail linkage Other Assistance: Medication Access Benefits Housing Information Sharing
Pre
-bo
ok
ing
Ja
il
Div
ers
ion
Intercept 2
Initial detention/Initial court hearings
Arrest
Initia
l D
ete
ntion
First A
pp
ea
rance C
ourt
CHALLENGES - INTERCEPT 2
• Multiple agencies have stake in outcome
• Less flexible – limited options
• System moves fast – consumers swept up in the
rush
• Appointed counsel or public defense
• Lack of resources
• Competency
• Bail decisions
• Length of Stay - Defendants detained for the
entire pretrial period are more likely to be
sentenced to jail or prison – and for longer
periods of time (Lowenkamp, VanNostrand, Holsinger/ Arnold Foundation)
VALIDATED SCREENING TOOLS
• Brief Jail Mental Health Screen (Sandusky, Shelby)
• 3 minutes at booking by corrections officer
• 8 yes/no questions
• General, not specific mental illness
• TCU Drug Screen V • screens for mild to severe substance use
disorder
• GAIN SS (Global Appraisal
of Individual Needs Short
Screen) (Wood County)
• can be used to screen for both MH and AoD
• Veteran/Military Screening Steadman et al. (2005)
PROMISING AND BEST PRACTICES
Role of Pretrial Services, bail investigators
Use of management information systems to identify and re-link to services
Immediate referrals to community services Screening Liaisons, Service providers attending arraignment hearings
Court supervised release as condition of bail
Follow-up into the community
Specialty Courts
Other Court
Programs
Jail-Based:
Mental Health &
Substance Abuse
Services
Intercept 3
Jails/Courts
CHALLENGES - INTERCEPT 3
Longer Stays
Case Outcomes
Reason for Detention
Impact of Detention
Medication
Housing - classification
USING CRIMINAL CHARGES TO LEAD TO
TREATMENT
Diversionary or Intervention in Lieu --- Generally pre-adjudication
contracts with judges to participate in treatment; Conviction is not
recorded Example:
Prosecutor holds charges in abeyance based on agreement to enter treatment under
supervision of mental health court; Plea is entered but adjudication is withheld
Post-Plea Based --- Adjudication occurs but disposition or sentence is
deferred Example:
Guilty plea is accepted; Sentence is deferred
Probation Based Example:
Conviction with treatment as a term of probation plus suspended jail sentence
Griffin, Steadman, & Petrila 2002

INTERCEPT 3: JAILS AND COURTS Ohio Specialized Dockets:
Mental Health Courts Drug Courts
OVI/DUI Courts Domestic Violence Courts
Child Support Enforcement Courts
Re-entry Courts Sex Offender Courts
Veterans Courts
In-jail services:
Identification / screening
Access to mental health / substance abuse services
(medications, etc.)
Communication with previous services as appropriate
Peer Supports
Priso
n
Jail Reentry
Intercept 4
Reentry
CHALLENGES - INTERCEPT 4
Delay or break in continuity of services
Employment
Supports
Transportation
Medication discontinuation
Housing
Organized discharge planning
Post Release Risk of Death
THE BACK DOOR: LINKAGES BETWEEN INSTITUTIONS AND THE
COMMUNITY
• Refer Out
– Institution staff refer to community agencies
• Community Linkage
• In-Reach
– Providers come in for intake (Butler County)
• Transition Reentry (Centers)
– Shared responsibility (NY, TX)
• Let the Other Guy Do It
– Parole assumes responsibility at or following release
• $40 and Bus Ticket
STRATEGIES & PROMISING
PRACTICES
• GAINS Reentry Checklist - Based on APIC Model:
Assess, Plan, Identify, Coordinate
• Permanent supportive housing can reduce
recidivism and homelessness in this population
(Returning Home Ohio)
• Ex-Offender Reentry Coalitions & Services
– Employment, Peer Support, Resource Assistance
• Maximizing use of public benefits: SOAR, Ohio
Benefit Bank, ROMPIR, Medicaid Expansion,
expediting applications, Fidelity Bonding
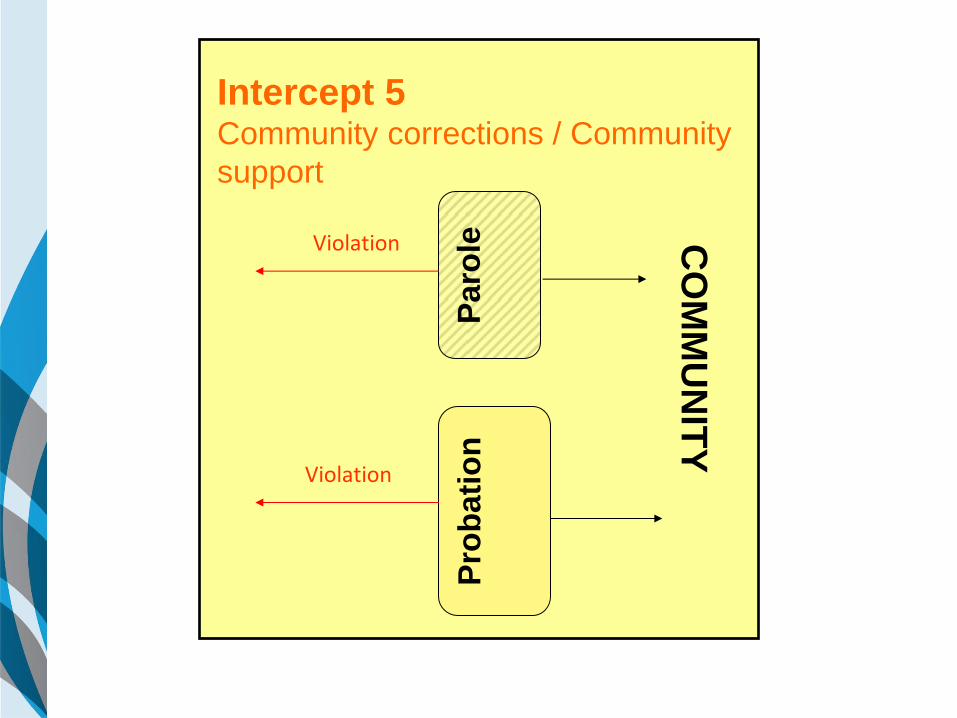
Paro
le
CO
MM
UN
ITY
Pro
bati
on
Violation
Violation
Intercept 5 Community corrections / Community
support
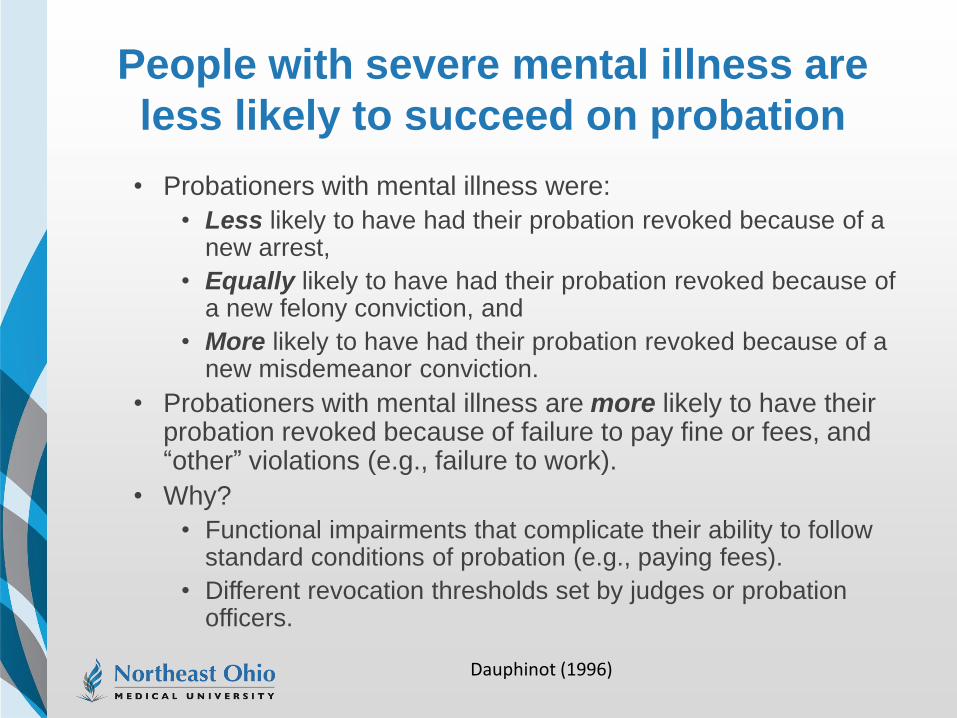
People with severe mental illness are
less likely to succeed on probation
• Probationers with mental illness were:
• Less likely to have had their probation revoked because of a new arrest,
• Equally likely to have had their probation revoked because of a new felony conviction, and
• More likely to have had their probation revoked because of a new misdemeanor conviction.
• Probationers with mental illness are more likely to have their probation revoked because of failure to pay fine or fees, and “other” violations (e.g., failure to work).
• Why?
• Functional impairments that complicate their ability to follow standard conditions of probation (e.g., paying fees).
• Different revocation thresholds set by judges or probation officers.
Dauphinot (1996)
STRATEGIES TO IMPROVE SUCCESS FOR
PROBATIONERS/ PAROLEES WITH SEVERE
MENTAL ILLNESS
Reduce caseloads for specialty probation:
– Knowledge about mental health & community resources
– Relationships with clinicians
– Advocate for services
– Actively supervise these individuals
– Dual role - legal, surveillance and therapeutic, problem-solving
– Quality relationships with probationers that can strongly influence
outcomes.
– Problem-solving strategies to resolve noncompliance issues and
address individual inabilities or barriers
– Maximize limited resources in creative ways to address specialized
needs
Skeem & Louden (2006)
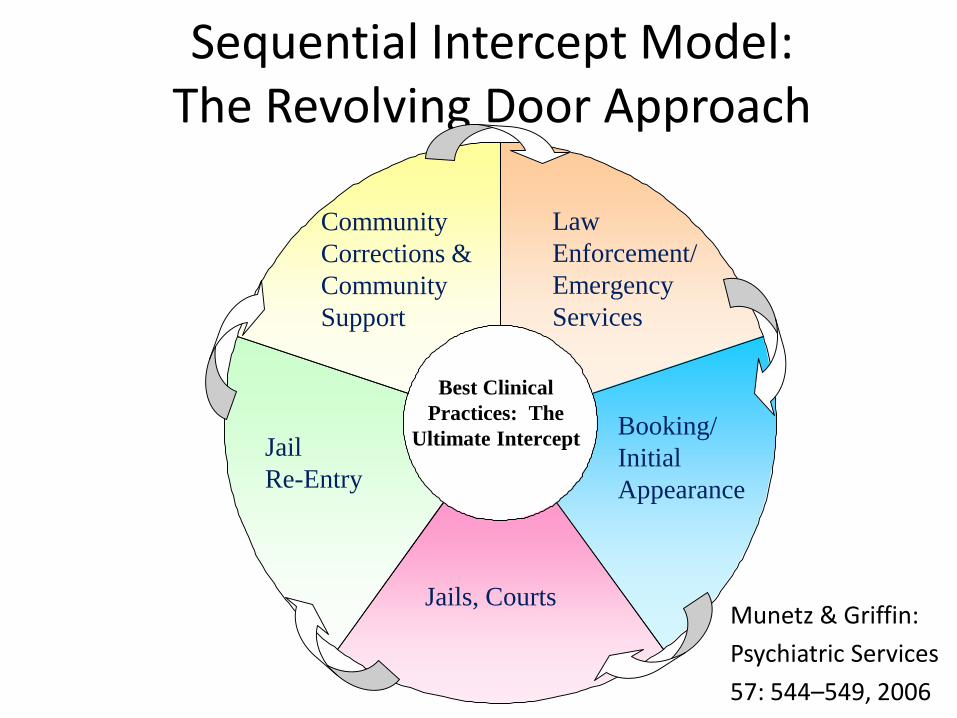
Sequential Intercept Model: The Revolving Door Approach
Community
Corrections &
Community
Support
Law
Enforcement/
Emergency
Services
Jail
Re-Entry
Booking/
Initial
Appearance
Jails, Courts
Best Clinical
Practices: The
Ultimate Intercept
Munetz & Griffin:
Psychiatric Services
57: 544–549, 2006
CROSS INTERCEPTS
• The GAINS Center has identified system-level
approaches relevant across all the intercepts.
– Collaboration among the stakeholders
– The “ultimate intercept” = community based
services
• For example, supported housing, education and
employment, peer support and other EBPs
• Culturally competent, gender specific and trauma informed
services
• Services which address the specific needs of veterans
• Attention to criminogenic risks and needs

Keys to Success
Task Force
Work Groups
Consumer Involvement
Communication & Information Sharing
Boundary Spanner(s)/Champion(s)
Momentum
Lawrence
Scioto Gallia
Adams
Pike Meigs
Jackson
Brown
Clermont
Hamilton Highland
Vinton
Ross Athens
Clinton
Warren
Butler Washington Hocking
Fayette Morgan Pickaway
Greene Monroe Preble
Montgomery
Perry Fairfield Noble
Clark
Madison
Franklin
Muskingum Belmont Miami Guernsey
Champaign Licking Darke
Harrison Delaware
Coshocton Shelby
Union
Logan
Knox
Jefferson
Tuscarawas
Holmes Auglaize Marion Morrow
Mercer Carroll
Hardin
Allen Columbiana
Stark Van Wert
Wayne Wyandot
Richland
Crawford Ashland
Mahoning Putnam Hancock
Paulding
Seneca Medina
Huron Portage
Summit
Defiance Henry Erie Sandusky
Trumbull Lorain
Wood
Ottawa
Cuyahoga
Williams
Geauga
Fulton Lucas
Lake
Ashtabula
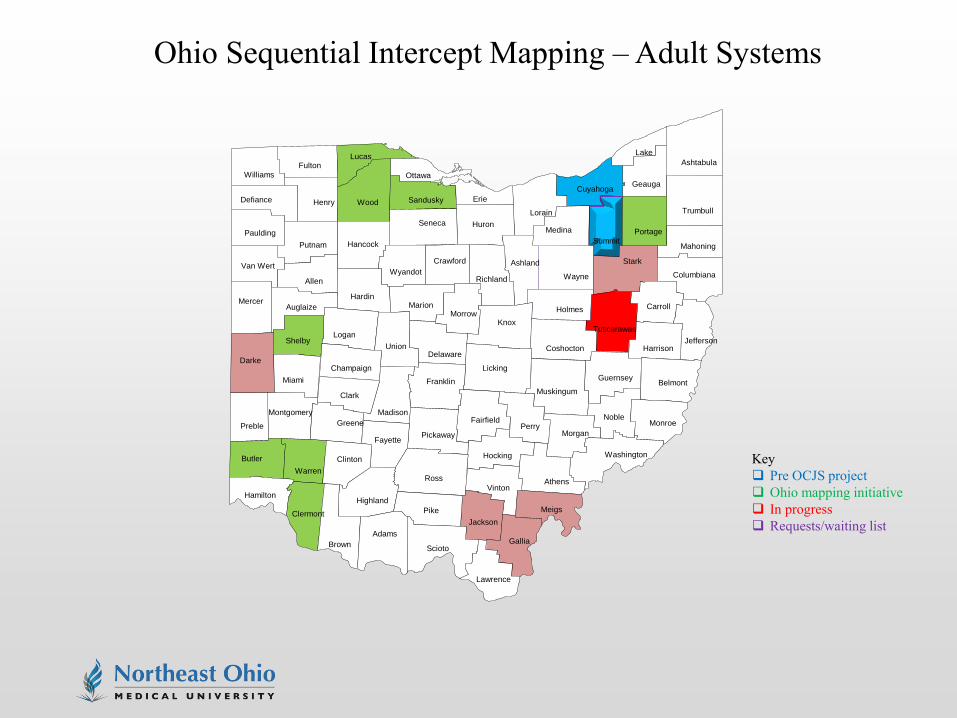
Ohio Sequential Intercept Mapping – Adult Systems
Key
Pre OCJS project
Ohio mapping initiative
In progress
Requests/waiting list
TECHNICAL ASSISTANCE – CJ CCOE
• Trainers and Consultants
• Website
• Lending Library
• Local, State and National Resources
• Guidance on Best Practices and Evidence-
based Practices
• Peer networking
Ruth H. Simera, M.Ed., LSW Program Administrator
330-325-6670
www.neomed.edu/academics/criminal-justice-coordinating-center-of-excellence
41
1. Map The System
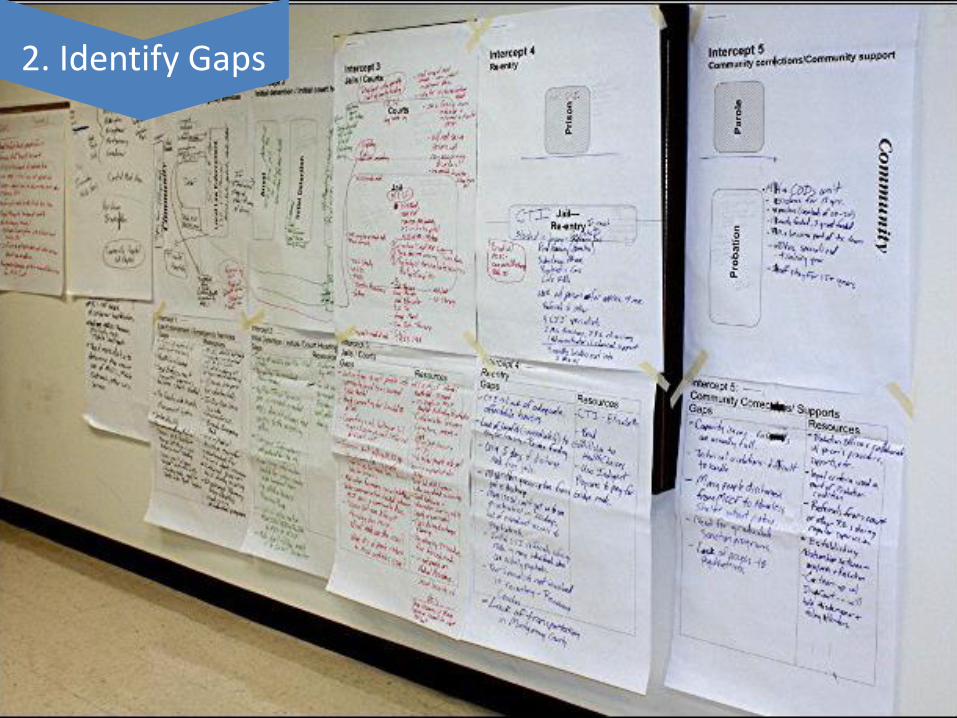
2. Identify Gaps
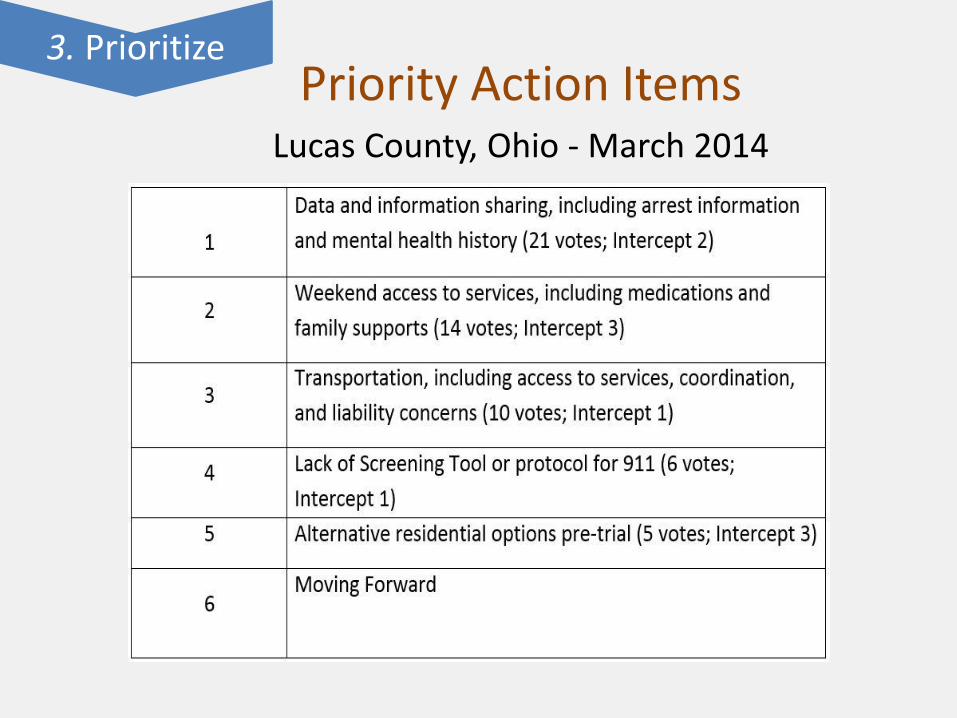
Priority Action Items Lucas County, Ohio - March 2014
3. Prioritize
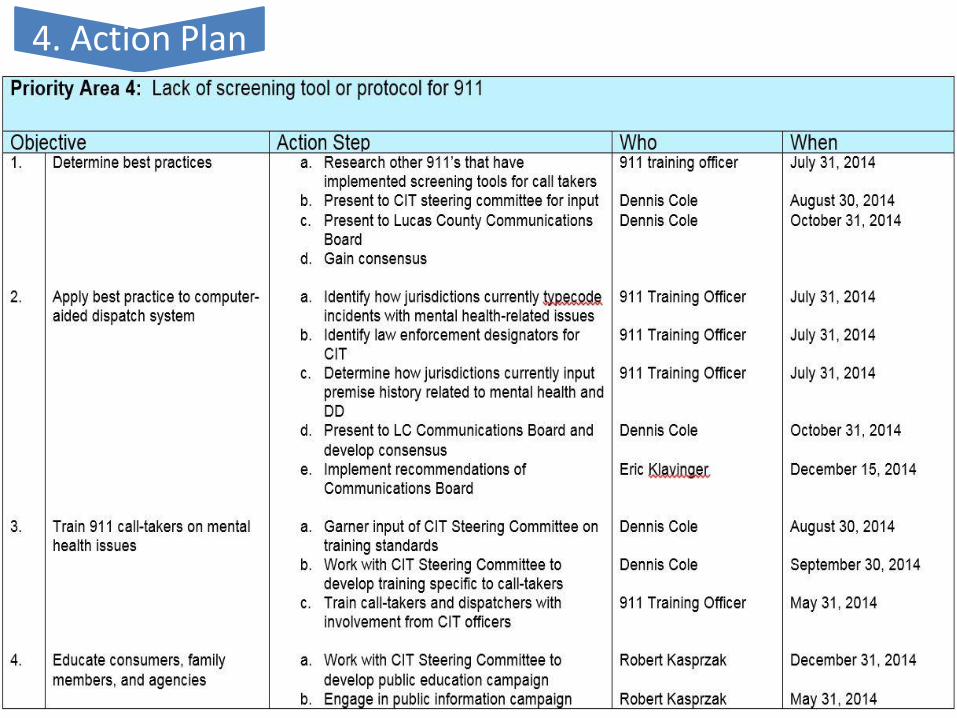
4. Action Plan
Final Report • First cross-systems picture
• Wide distribution among local partners
• Planning reference
• Support for future funding applications
• Reference/resource materials included
• Priorities addressed over time – Especially with the CJAB and OBH
• Developmental tool
• Outcome measurement tool
Keeping the Momentum Going!
• Behavioral Health / Criminal Justice Alternatives Committee
– Be inclusive but stay focused
– Monthly meeting schedule (2nd Wednesday @ 10 AM)
– Workgroups broken down by priority
– Monitor performance
– Adjust “on the fly”
– Celebrate the big (and small) accomplishments
The Ultimate Intercept – Best Clinical Practices
• Crisis Intervention Team Training – Intersect 1
– Goals include improving de-escalation skills of law enforcement when dealing with people in psychiatric distress, reduce physical altercations, increase diversion, increase knowledge of community resources
– 508 law enforcement officers & 64 justice professionals trained
– http://www.citinternational.org/
The Ultimate Intercept – Best Clinical Practices
• Program of Assertive Community Treatment (includes ACT & FACT)
– Intercept 1-5
– Team Approach
– Community based & personalized
– Flexible & Time Unlimited
– NGRI/ICST-CJ (recidivism < 5% over last 5 years)
– http://store.samhsa.gov/product/Assertive-Community-Treatment-ACT-Evidence-Based-Practices-EBP-KIT/SMA08-4345
The Ultimate Intercept – Best Clinical Practices
• Treatment Accountability for Safer Communities – Intercept 1-5
– Independent entity (Boundary Spanner)
– Assessment, Referral, Linkage, Case Management, Reporting
– Improves treatment, employment and recidivism outcomes http://www.lucastasc.org/research.html
– http://nationaltasc.org/
The Ultimate Intercept – Best Clinical Practices
• Specialty Dockets
– Team intensive treatment
– regular court attendance and drug testing
– Judicial oversight
– System of rewards and immediate sanctions
– Family, Reentry, Veterans (2 drug courts planning stage)
– http://www.nadcp.org/
The Ultimate Intercept – Best Clinical Practices
• Medication Assisted Treatment – Intercept 1 – 5
– Methadone (tab or liquid)
– Buprenorphene (Subutex – tab)
– Buprenorphene & Naloxone (Suboxone –tab & film)
– Naltrexone (Vivitrol – injectable)
– Always in conjunction with counseling
– Associated with improved treatment outcomes
– http://www.samhsa.gov/medication-assisted-treatment
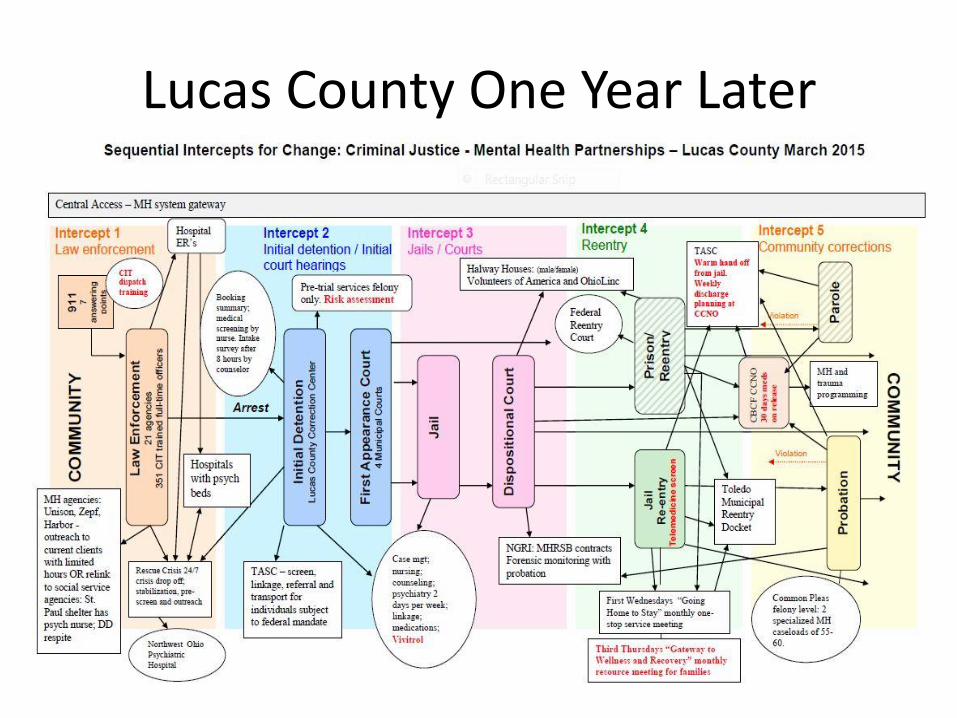
Lucas County One Year Later