Altered Patterns Of Motion - Hunger Ford - Lee 2004
9
Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers Barbara Hungerford a, * , Wendy Gilleard b , Diane Lee c a School of Exercise and Sport Science, University of Sydney, Sydney, Australia b School of Exercise Science and Sport Management, Southern Cross University, Lismore, Australia c Diane G. Lee Physiotherapist Corp., BC, Canada Received 14 February 2003; accepted 19 February 2004 Abstract Objective. To determine whether the pattern of pelvic bone motion, determined by skin markers, differs between control subjects and subjects with posterior pelvic pain. Design. Cross-sectional study of three-dimensional angular and translational motion of the innominates relative to the sacrum in two subject groups. Background. Comparative in vivo analysis of the 3D patterning of pelvic motion in subjects with posterior pelvic pain and controls is limited. Methods. Fourteen males with posterior pelvic pain and healthy age and height matched controls were studied. A 6-camera motion analysis system was used to determine 3D angular and translational motion of pelvic skin markers during standing hip flexion. Results. Posterior rotation of the innominate occurred with hip flexion in control subjects and pelvic pain subjects as previously reported in the literature. On the supporting leg, the innominate rotated posteriorly in controls and anteriorly in symptomatic subjects. Conclusion. Posterior rotation of the innominate, as measured using skin markers during weight bearing in controls may reflect activation of optimal lumbo-pelvic stabilisation strategies for load transfer. Anterior rotation occurred in symptomatic subjects, suggesting failure to stabilise intra-pelvic motion for load transfer. Relevance This study found that posterior rotation of the innominate occurred during weight bearing in controls. This movement pattern is thought to optimise stability of the pelvic girdle during increased loading. Conversely, anterior rotation occurred in symptomatic subjects during weight bearing. This is a non-optimal pattern and may indicate abnormal articular or neuromyofascial function during increased vertical loading through the pelvis. Ó 2004 Elsevier Ltd. All rights reserved. Keywords: Sacroiliac joint; Pelvic motion; Pelvic stabilisation; Low back pain; Pelvic pain 1. Introduction A primary function of the lumbar spine and pelvis is to transfer the loads generated by body weight and gravity during standing, walking and sitting (Snijders et al., 1993). How well this load is managed dictates the efficacy of function. A small amount of motion occurs at the sacroiliac joints (SIJ) and the pubic symphysis dur- ing movements of the trunk and lower limbs (Jacob and Kissling, 1995; Walheim and Selvik, 1984). Conse- quently, during weight bearing activities, control (sta- bilisation) of intra-pelvic motion is required for transference of loads between the spine and the lower limbs (Snijders et al., 1993; Vleeming et al., 1990). According to Panjabi (1992) stability is achieved when the passive, active and control systems work together. Snijders et al. (1993) suggests that the passive, active and control systems produce approximation of the joint surfaces, essential if stability is to be insured. The * Corresponding author. Present address: Sydney Spine and Pelvis Centre, 101 Lyons Road, Drummoyne, NSW 2047, Australia. E-mail address: [email protected] (B. Hungerford). 0268-0033/$ - see front matter Ó 2004 Elsevier Ltd. All rights reserved. doi:10.1016/j.clinbiomech.2004.02.004 www.elsevier.com/locate/clinbiomech Clinical Biomechanics 19 (2004) 456–464
-
Upload
wilton-filho -
Category
Documents
-
view
40 -
download
0
Transcript of Altered Patterns Of Motion - Hunger Ford - Lee 2004

www.elsevier.com/locate/clinbiomech
Clinical Biomechanics 19 (2004) 456–464
Altered patterns of pelvic bone motion determined in subjectswith posterior pelvic pain using skin markers
Barbara Hungerford a,*, Wendy Gilleard b, Diane Lee c
a School of Exercise and Sport Science, University of Sydney, Sydney, Australiab School of Exercise Science and Sport Management, Southern Cross University, Lismore, Australia
c Diane G. Lee Physiotherapist Corp., BC, Canada
Received 14 February 2003; accepted 19 February 2004
Abstract
Objective. To determine whether the pattern of pelvic bone motion, determined by skin markers, differs between control subjects
and subjects with posterior pelvic pain.
Design. Cross-sectional study of three-dimensional angular and translational motion of the innominates relative to the sacrum in
two subject groups.
Background. Comparative in vivo analysis of the 3D patterning of pelvic motion in subjects with posterior pelvic pain and
controls is limited.
Methods. Fourteen males with posterior pelvic pain and healthy age and height matched controls were studied. A 6-camera
motion analysis system was used to determine 3D angular and translational motion of pelvic skin markers during standing hip
flexion.
Results. Posterior rotation of the innominate occurred with hip flexion in control subjects and pelvic pain subjects as previously
reported in the literature. On the supporting leg, the innominate rotated posteriorly in controls and anteriorly in symptomatic
subjects.
Conclusion. Posterior rotation of the innominate, as measured using skin markers during weight bearing in controls may reflect
activation of optimal lumbo-pelvic stabilisation strategies for load transfer. Anterior rotation occurred in symptomatic subjects,
suggesting failure to stabilise intra-pelvic motion for load transfer.
Relevance
This study found that posterior rotation of the innominate occurred during weight bearing in controls. This movement pattern is
thought to optimise stability of the pelvic girdle during increased loading. Conversely, anterior rotation occurred in symptomatic
subjects during weight bearing. This is a non-optimal pattern and may indicate abnormal articular or neuromyofascial function
during increased vertical loading through the pelvis.
� 2004 Elsevier Ltd. All rights reserved.
Keywords: Sacroiliac joint; Pelvic motion; Pelvic stabilisation; Low back pain; Pelvic pain
1. Introduction
A primary function of the lumbar spine and pelvis is
to transfer the loads generated by body weight and
gravity during standing, walking and sitting (Snijders
et al., 1993). How well this load is managed dictates the
efficacy of function. A small amount of motion occurs at
* Corresponding author. Present address: Sydney Spine and Pelvis
Centre, 101 Lyons Road, Drummoyne, NSW 2047, Australia.
E-mail address: [email protected] (B. Hungerford).
0268-0033/$ - see front matter � 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.clinbiomech.2004.02.004
the sacroiliac joints (SIJ) and the pubic symphysis dur-
ing movements of the trunk and lower limbs (Jacob and
Kissling, 1995; Walheim and Selvik, 1984). Conse-
quently, during weight bearing activities, control (sta-
bilisation) of intra-pelvic motion is required for
transference of loads between the spine and the lower
limbs (Snijders et al., 1993; Vleeming et al., 1990).According to Panjabi (1992) stability is achieved when
the passive, active and control systems work together.
Snijders et al. (1993) suggests that the passive, active and
control systems produce approximation of the joint
surfaces, essential if stability is to be insured. The

B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464 457
amount of approximation required is variable and dif-ficult to quantify as it is dependent on an individual’s
structure (form closure) and the forces they need to
control (force closure). The ability to effectively transfer
load through the pelvis is dynamic and therefore de-
pends on: (1) optimal function of the bones, joints and
ligaments (Vleeming et al., 1989, 1990); (2) optimal
function of the muscles and fascia (Hungerford et al.,
2003; Richardson et al., 2002; Snijders et al., 1998;Vleeming et al., 1995a,b); (3) appropriate neural func-
tion (Hodges and Richardson, 1997; Hungerford et al.,
2003).
1.1. Stabilisation and motion control of the pelvic girdle
For every joint, there is a position called the self-
braced (close-packed) position in which there is maxi-mum congruence of the articular surfaces and maximum
tension on major ligaments. In this position, the joint is
under significant compression and the ability to resist
shear forces is enhanced by tensioning of the passive
structures and increased friction between the articular
surfaces (Snijders et al., 1993; Vleeming et al., 1990).
The self-braced position of the SIJ is nutation of the
sacrum or posterior rotation of the innominate (Vlee-ming et al., 1989). Studies have shown (Sturesson et al.,
2000) that nutation of the sacrum relative to posterior
rotation of the innominate occurs bilaterally whenever
the lumbo-pelvic spine is loaded vertically (sitting,
standing). Counternutation of the sacrum, or anterior
rotation of the innominate, is thought to be a relatively
less stable position for the SIJ (Vleeming et al., 1995b).
The long dorsal ligament becomes taut during thismotion, however tension in other ligaments such as
sacrotuberous and interosseous ligaments decreases
(Vleeming et al., 1996).
At present there is only limited research comparing
the in vivo pattern of pelvic motion during weight
bearing and non-weight bearing activities. This is due to
the invasiveness of the most reliable and valid methods
of analysis, consequential ethical considerations forusing invasive procedures to evaluate large number of
subjects and difficulty in evaluating the small amplitude
of in vivo SIJ motion. When an individual stands on
one leg and flexes the contralateral hip, the non-weight
bearing innominate posteriorly rotates relative to the
sacrum (range of motion 0.1–5.0�) (Jacob and Kissling,1995; Sturesson et al., 2000). Side flexion and axial
rotation of the innominate occur concurrently aboutsagittal and vertical axes respectively. Translation
(motion along the sagittal, vertical and/or coronal axes)
also occurs (Jacob and Kissling, 1995; Sturesson et al.,
2000), although the specific direction of translation that
occurs with angular motion is not fully understood. It
has been hypothesised (Lee, 1999) that anterior and
superior translation of the innominate, relative to the
sacrum, will occur with posterior rotation of theinnominate.
1.2. Range of motion versus patterning of pelvic motion
Buyruk et al. (1995) and Damen et al. (2002) estab-
lished that a Doppler imaging system was able to mea-
sure stiffness of the SIJ. This research showed that
stiffness of the SIJ is variable between subjects andtherefore the range of motion is potentially variable. It
also revealed that stiffness of right and left SIJs is sym-
metric in subjects without pelvic pain. The results sup-
port putting less emphasis on amplitude of motion and
more on the pattern or symmetry of SIJ, or pelvic
motion, as range of motion varies between subjects,
however within one subject joint stiffness remains sym-
metric between sides.
1.3. The impact of posterior pelvic pain
The SIJs and the posterior SIJ ligaments are a knownsource of posterior pelvic pain (Fortin et al., 1994;
Vleeming et al., 2002). Jacob and Kissling (1995) noted
that in the presence of SIJ symptoms, the amplitude of
SIJ motion about a coronal axis increased during hip
flexion in one subject. Mens et al. (1999) determined
increased amplitude of anterior rotation of the innom-
inate in posterior pelvic pain patients. Sturesson et al.
(2000) reported no difference in the amplitude or patternof either angular or translational motion of the in-
nominates when the left and right SIJs were compared
in subjects with posterior pelvic pain. No comparison
was made with an asymptomatic group. Hungerford
et al. (2003) showed that posterior pelvic pain alters the
pattern of lumbo-pelvic muscle recruitment, while
Buyruk et al. (1999) and Damen et al. (2002) showed
that stiffness of the SIJ is asymmetric in subjects withpelvic pain and that asymmetrical stiffness of the SIJs is
prognostic for pelvic impairment and pain. It is pres-
ently unknown if posterior pelvic pain alters the pat-
terning of bone motion within the pelvis for single leg
stance.
1.4. Posterior pelvic pain and the active straight leg raise
test
The supine active straight leg raise test (ASLR)
(Mens et al., 2001) has been validated as a clinical test
for measuring effective load transfer between the trunk
and lower limbs. When the lumbo-pelvic region is
functioning optimally, the leg should rise effortlessly
from the table (effort graded from 0 to 5) (Mens et al.,
1999). A correlation has been shown between positiveASLR findings and posterior pelvic pain (Mens et al.,
1999; O’Sullivan et al., 2002). Similarly, Damen et al.

458 B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464
(2001) and Buyruk et al. (1999) showed that the ASLRis positive in the presence of asymmetric stiffness of the
SIJ. This suggests that altered pelvic stabilisation strat-
egies may affect pelvic mobility (Buyruk et al., 1999;
Damen et al., 2001).
1.5. Limitations of methodology in this study
A non-invasive motion analysis system using skinmounted markers was chosen to acquire the kinematic
data of pelvic bone motion during a standing hip flexion
movement for ethical reasons. Errors in determining the
range of motion are likely to occur with an opto-
electronic system due to skin marker motion relative to
underlying bony landmarks (Maslen and Ackland,
1994). A high resolution motion analysis system has
however been reported to provide reliable and consistentin vivo data of lumbar segmental motion patterns
(Gracovetsky et al., 1995). In this study, the authors
recognise that the movements noted reflect motion of
the innominates, sacrum, and femurs in conjunction
with overlying skin, and therefore the main emphasis of
this study was to investigate the patterns of bone motion
rather than the range of motion.
The aim of this study was to determine the three-dimensional pattern of innominate bone motion occur-
ring in subjects determined to have posterior pelvic pain
and impaired pelvic stabilisation strategies during
weight bearing and non-weight bearing components of a
standing hip flexion movement. These results were
compared to age and height matched controls with
clinically assessed normal pelvic stabilisation and pelvic
motion patterns. It was hypothesised that the pattern ofinnominate bone motion would alter in subjects with
posterior pelvic pain during both components of the
movement trial.
2. Methods
2.1. Subjects
2.1.1. Impaired pelvic stabilisation and posterior pelvic
pain group
Fourteen male subjects with SIJ pain and a mean
(range) age, height and weight of 32.7 (24–47) years,
176.8 (168–184) cm, and 77.0 (71–90) kg respectively,
volunteered for the study. The criteria for inclusion in
this study were:
1. Each subject in the posterior pelvic pain group
reported unilateral pain over the posterior pelvic/SI
region (Fortin et al., 1994) for greater than two
months, and no pain above the lumbo-sacral junc-
tion. The pain was consistently and predictably
aggravated by activities that vertically loaded the pel-vis (walking, standing or sitting).
2. Positive results on the side of posterior pelvic pain in
clinical tests for impaired lumbo-pelvic stabilisation.
These tests included:
(a) Active straight leg raise test (Mens et al., 1999,
2001): A positive test was indicated when the pelvis
failed to remain in neutral alignment, and the sub-
ject reported difficulty or inability to elevate astraight leg in supine. The perceived difference of
effort, or pain aggravation was scaled from 0
(not difficult to raise the leg) to 5 (unable to per-
form ASLR).
(b) Standing hip flexion test (Mitchell, 1995): Dur-
ing a left standing hip flexion test, the subject
stands on their right leg and flexes the left hip to-
wards 90�. The left innominate should posteriorlyrotate relative to the sacrum (Jacob and Kissling,
1995). A positive test was indicated when superior
motion of the posterior superior iliac spine (PSIS)
was palpated relative to the sacrum.
(c) Neutral zone analysis test (joint play) (Lee,
1999)––this test was used clinically to apply the re-
search of Buyruk et al. (1999) and Damen et al.
(2002) and to evaluate motion in the neutral zoneof the SIJ. Panjabi (1992) noted that joints have
non-linear load–displacement curves and that the
size of the neutral zone may increase with injury,
articular degeneration and/or weakness of the sta-
bilising musculature and that this is a more sensi-
tive indicator than angular range of motion for
detecting instability. All symptomatic subjects
demonstrated asymmetric stiffness of the SIJ whenthe innominate was glided relative to the sacrum
(analysis of the neutral zone).
As the reliability and predictive ability of the standing
hip flexion and neutral zone analysis tests remains
uncertain (Carmichael, 1987; Vincent-Smith and Gib-
bons, 1999) all clinical tests were required to be positive
on the side of pain, in conjunction with the ASLR test,for inclusion in the posterior pelvic pain subject group.
Subjects were excluded from the study if they could not
flex each hip to 90� without pain, if they had undergonespinal surgery, or displayed overt neurological signs
such as sensory paraesthesia or motor paresis.
2.1.2. Control group
The SIJ pain group were age and height matched to acontrol group of 14 males with a mean (range) age,
height, and weight of 33.5 (22–50) years, 176.0 (168–183)
cm, and 72.5 (61–85) kg respectively. The control sub-
jects had no history of low back pain in the last 12
months, no history of congenital lumbar or pelvic
anomalies, and tested negative to the ASLR and
standing hip flexion and neutral zone analysis tests.

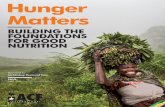
Fig. 1. The three axes for angular and translational motion of the
innominate relative to the sacral segment. Note the axis of innominate
segment motion is centred at the PSIS.
B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464 459
Subjects were excluded if no palpable motion betweenthe PSIS and S2 spinous process was observed during
unilateral hip flexion in standing, or if they experienced
any pain during the clinical assessment.
All subjects were assessed by the same experienced
physiotherapist to maintain continuity. Informed con-
sent was given by each subject prior to participation in
the study, and all rights of the subjects were protected.
The study was approved by the institutional HumanEthics Committee.
2.2. Procedure
Fifteen lightweight highly reflective 15 mm diameter
balls were used to define the bony landmarks of each
innominate, both femoral segments, and the sacrum.
The pelvic bony landmarks were chosen for theircloseness to the skin surface with minimal overlying
fascia, and because they reflected palpation points
commonly used by therapists. Each innominate was
therefore defined by three markers placed on the ante-
rior superior iliac spine (ASIS), the PSIS, and the lateral
iliac tubercle. A three armed triangular wand with a
single marker attached to each arm was applied to the
sacral spinous process of S2. Each arm was 10 mm long,and solidly welded to the triangular base. The apical
marker of the wand approximated the S1 spinous pro-
cess, while a left and right marker formed the base of the
triangle at the horizontal level of S2. The left and right
femoral segments were defined by markers on the
greater trochanter, the lateral femoral condyle, and a
mid thigh marker placed 20 cm inferior and 5 cm
anterior to the greater trochanter. All markers wereapplied to the skin while the subjects were standing.
A six camera Expert Vision Motion Analysis (Eva)e
Hi Res.6.0 System (Motion Analysis Corporation, Cal-
ifornia, USA) was used to video (60 Hz) the subject
motion. Measurements of a known angle showed the six
camera Evae system was accurate to 0.25�. Forceplatform data (960 Hz) were used to identify initiation
of single leg support during each standing hip flexiontrial. Following practice trials, data from one quiet
standing trial were collected. The subject then per-
formed six left and six right standing hip flexion trials.
For example, during a left standing hip flexion trial the
subject was asked to stand on his right leg, and flex his
left hip and knee toward 90� hip flexion, then lower thefoot back down.
2.3. Data analysis
The Evae motion analysis system was used to track
the 3D trajectories of each marker over time. These
trajectories were then imported into Kintrake (Motion
Analysis Corporation) which provided the 3D angular
rotation, and translation, of each innominate relative to
the sacral segment throughout each trial, in respect to
neutral position from the quiet standing trial. Calcula-tion of the angular kinematics required definition of
individual segment coordinate systems, and a joint
coordinate system. The segment coordinate systems
were assumed to be embedded within each adjacent
segment. The axes of the innominate segment originated
at each respective PSIS, and the axes of the sacral seg-
ment intercepted at the S2 spinous process (Fig. 1).
Pelvic motion was determined by aligning the coronalaxis of each innominate and sacral segment to intersect
both the PSIS and S2 spinous process. Kintrake sub-
sequently determined relative angular and translational
motion of each bone segment about their aligned seg-
ment coordinate systems. Hip joint motion was deter-
mined by computing the motion of the femur, as defined
by linking the three femoral markers, in relation to
ipsilateral innominate motion. The hip joint centre wasdetermined using the equation provided by Tylkowski
et al. (1982).
All angular and translational motion was determined
at maximum coronal axis motion of the innominate,
relative to the sacrum, during hip flexion. Two tailed
paired Student t-tests assuming unequal variance
(Domholdt, 1993) were performed for all variables be-
tween the left and right side in the control group, andbetween the symptomatic side and the asymptomatic
side in the SIJ pain group. In order to determine if there
was a significant alteration to the mean angular and
translational intra-pelvic motion measured between the
control subjects and the SIJ pain group, independent
groups two tailed Student t-tests assuming unequal
variance (Domholdt, 1993) were performed for all
variables. Further graphical comparisons of coronalaxis motion on the side of single leg support were

-6
-4
-2
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 10 11 12 13 14
subjects
coronalaxisrotation(°)
posterior
anterior
pelvic pain asymptomaticpelvic pain symptomaticcontrols mean
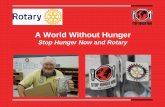
Fig. 2. A comparison of coronal axis angular motion at single leg support in each subject with posterior pelvic pain. Mean coronal axis motion for
control subjects is depicted as a solid line. Error bars denote 2 · standard error for each subject. �Significant at P < 0:05.
460 B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464
performed for each subject in the SIJ pain group. Two
times the standard error of mean motion for eachsubject was determined and plotted. As the mean± 2 SE
is approximately equal to the 95% confidence interval
(Sim and Reid, 1999), determination of no overlay of
each subject’s data was defined as a significant difference
(Fig. 2).
3. Results
The pattern of angular and translational motion of
each innominate segment, relative to the sacral segment,
Table 1
Comparison of angular and translational motion of the left and right innom
posterior pelvic pain
Motion
segment
Axis of motion A: Control subjects
Left hip flexion Right hip flexion
Mean SD Mean SD
Femur Coronal 70.00 5.25 73.00 5.50
Innominate
angular (�)Coronal )8.50 3.50 )10.00 3.50
Sagittal )6.00 3.50 )7.75 5.00
Vertical 4.50 4.50 3.50 3.00
Innominate
translation
(mm)
Antero-posterior 3.50 2.50 4.00 3.00
Medio-lateral )5.50 3.00 )5.50 2.50
Vertical )6.50 3.00 )7.50 3.50
Negative coronal value¼ posterior; negative sagittal¼ toward flexed hip; neganegative medio-lateral translation¼ toward flexed hip; negative vertical tran* Significant at P < 0:05.
was measured during a standing hip flexion movement
using a non-invasive method. Possible errors in deter-mining the magnitude of pelvic bone motion may have
occurred due to the movement of skin markers over
bony landmarks, therefore the emphasis of this study
was on changes to the patterns of pelvic bone motion as
reflected by the measured skin marker movement.
3.1. Hip flexion side
The angular and translational motions of the left and
right innominates, during left and right standing hip
flexion movements are summarised in Tables 1–3. In the
inates on the side of hip flexion in control subjects and subjects with
B: Posterior pelvic pain subjects
P -value Asymptomatic
hip flexion
Symptomatic hip
flexion
P -value
Mean SD Mean SD
0.08 73.25 7.00 74.50 4.50 0.28
0.05 )7.50 3.00 )10.00 3.25 0.04�
0.18 )5.00 5.50 )6.25 4.00 0.44
0.39 3.75 2.50 4.75 1.75 0.27
0.49 2.00 4.00 2.00 3.75 0.70
0.74 )5.50 2.00 )6.50 3.00 0.36
0.46 )4.00 3.50 )5.00 2.00 0.76
tive vertical¼ toward flexed hip; negative antero-posterior¼ posterior;slation¼ superior.

Table 2
Comparison of angular and translational motion of the innominates on the side of single leg support in control subjects and subjects with posterior
pelvic pain
Motion
segmentAxis of motion A: Control subjects B: Posterior pelvic pain subjects
Left single leg
support
Right single leg
support
P -value Asymptomatic
single leg support
Symptomatic
single leg support
P -value
Axis Mean SD Mean SD Mean SD Mean SD
Femur Coronal 1.50 3.00 1.50 2.50 0.79 1.75 3.50 1.75 3.25 0.86
Innominate
angular (�)Coronal 0.00 2.00 )0.50 3.00 0.88 0.50 1.50 2.00 2.00 0.02�
Sagittal )6.00 2.50 )5.75 2.50 0.46 )4.75 3.25 )3.75 3.00 0.42
Vertical 3.50 2.75 4.50 4.50 0.17 5.00 2.50 3.75 2.75 0.09
Innominate
translation
(mm)
Antero-posterior )4.50 6.00 )2.50 4.00 0.13 )4.00 2.50 )6.00 2.75 0.02�
Medio-lateral )6.50 3.25 )6.50 3.00 0.96 )7.00 3.25 )5.00 2.50 0.03�
Vertical )4.50 2.50 )3.50 2.50 0.19 3.50 2.25 2.00 3.00 0.04�
Negative coronal value¼posterior; negative sagittal¼ toward flexed hip; negative vertical¼ toward flexed hip; negative A-P translation¼ posterior;negative medio-lateral¼ toward flexed hip; negative vertical¼ superior.
Table 3
Comparison of angular and translational motion of the innominates between control subjects and subjects with posterior pelvic pain
Motion
segmentAxis of motion A: Hip flexion B: Single leg support
Controls right Pelvic pain group
symptomatic
P -value Controls right Pelvic pain group
symptomatic
P -value
Axis Mean SD Mean SD Mean SD Mean SD
Femur Coronal 73.00 5.50 74.50 4.50 0.45 1.50 2.50 1.75 3.25 0.67
Innominate
angular (�)Coronal )10.00 3.50 )10.00 3.25 0.16 )0.50 3.00 2.00 2.00 <0.01�
Sagittal )7.75 5.00 )6.25 4.00 0.94 )5.75 2.50 )3.75 3.00 0.12
Vertical 3.50 3.00 4.75 1.75 0.46 4.50 4.50 3.75 2.75 0.90
Innominate
translation
(mm)
Antero-posterior 4.00 3.00 2.00 3.75 0.05 )2.50 4.00 )6.00 2.75 0.02�
Medio-lateral )5.50 2.50 )6.50 3.00 0.94 )6.50 3.00 )5.00 2.50 0.13
Vertical )7.50 3.50 )5.00 2.00 0.04� )3.50 2.50 2.00 3.00 <0.001�
Negative coronal value¼posterior; negative sagittal¼ toward flexed hip; negative vertical¼ toward flexed hip; negative A-P translation¼ posterior;negative medio-lateral¼ toward flexed hip; negative vertical¼ superior.* Significant at P < 0:05.
B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464 461
control subjects, standing hip flexion (Table 1A) pro-
duced posterior rotation of the non-weight bearinginnominate relative to the sacral segment. On the side of
hip flexion, femoral flexion showed a mean (range) 73.0�(10.0) at maximum coronal axis angular motion of the
innominate. The innominate concurrently side flexed
toward the side of hip flexion, and rotated about the
vertical axis away from the side of hip flexion. Trans-
lation of the innominate relative to the sacral segment
was associated with this angular motion. The innomi-nate translated anteriorly, superiorly, and laterally (to-
ward the side of hip flexion) as the innominate
posteriorly rotated (Table 1A). No significant difference
was found in the controls between the pattern of left and
right innominate motion on the side of hip flexion.
On the side of hip flexion for the posterior pelvic pain
group, maximum posterior rotation of the innominate
occurred at a mean of 73.25� (7.0) femoral flexion on theasymptomatic side, and at a mean of 74.5� (4.5) femoralflexion on the symptomatic side (Table 1B). A pattern of
side flexion of the innominate, and rotation about the
vertical axis away from the side of hip flexion, occurredon both the asymptomatic and symptomatic sides dur-
ing hip flexion.
Anterior, superior, and lateral translation of the
innominate toward the side of hip flexion, were associ-
ated with posterior rotation of the innominate on the
side of hip flexion. In the posterior pelvic pain group
there was no significant difference between the asymp-
tomatic and symptomatic sides in translational motion,or angular motion of the innominate about the sagittal
or vertical axes during hip flexion (Table 1B).
3.2. Single leg support
The contralateral limb maintained single leg support
during the standing hip flexion movement. Posterior
rotation of the weight bearing innominate occurredabout the coronal axis in control subjects (Table 2A). A
concurrent pattern of side flexion of the innominate

462 B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464
toward, and rotation about the vertical axis away fromthe side of hip flexion also occurred. The weight bearing
innominate translated posteriorly, superiorly and
medially (toward the side of hip flexion) (Table 2A). No
significant difference was found in the pattern of either
angular or translational motion of the weight bearing
innominate during single leg support in control subjects.
The angular and translational motion of the weight
bearing innominate on the side of single leg support, insubjects with posterior pelvic pain, is depicted in Table
2B. The weight bearing innominate anteriorly rotated
significantly more (P ¼ 0:02) about the coronal axis onthe symptomatic in comparison to the asymptomatic
side. Concurrently, the innominate side flexed toward,
and rotated away from the side of hip flexion on both
the symptomatic and asymptomatic sides. The innomi-
nate translated inferiorly, posteriorly, and medially(toward the side of hip flexion) relative to the sacral
segment (Table 2B). Posterior translation of the
innominate relative to the sacral segment was signifi-
cantly greater (P ¼ 0:02) on the symptomatic side thanthe asymptomatic side, while inferior translation of the
innominate was significantly less (P ¼ 0:04) on the
symptomatic side in comparison to the asymptomatic
side. Medial translation, or compression, of theinnominate was also significantly less (P ¼ 0:03) on thesymptomatic side in comparison to the asymptomatic
side (Table 2B).
Further comparison of coronal axis motion on the
symptomatic side and asymptomatic side of single leg
support was performed for each subject with posterior
pelvic pain (Fig. 2). The mean range of posterior rota-
tion on the side of single leg support in control subjectswas depicted as a solid line for comparison to the
symptomatic group. A significant change toward ante-
rior rotation of the innominate occurred in 12 of the 14
posterior pelvic pain subjects on the symptomatic side;
that is in subjects 1, 2, 4 to 7, 9 to 14 (Fig. 2).
3.3. Comparison of control subjects and subjects with
posterior pelvic pain
During the hip flexion component of the standing hip
flexion movement there was no significant difference in
patterning of angular or translational motion between
groups on the side of hip flexion (Table 3A).
On the side of single leg support, a significant differ-
ence in the pattern of angular and translational motion
of the innominate between controls and symptomaticsubjects was determined (Table 3B). In the control
group, posterior rotation of the weight bearing innom-
inate occurred on the side of single leg support; however,
in the posterior pelvic pain group, anterior rotation
occurred on the symptomatic side (P < 0:01). A pattern
of posterior, superior and medial translation occurred
concurrently with posterior rotation of the innominate
in control subjects; however, inferior, posterior, andmedial translation occurred with anterior rotation of the
innominate in the symptomatic subjects.
4. Discussion
Significant differences were found in the pattern of
pelvic bone motion that occurred during standing hipflexion when intra-subject (between weight bearing and
non-weight bearing sides) and inter-subject (between the
control group and posterior pelvic pain group) com-
parisons were made. The range of motion reported be-
tween the innominate and sacral segments, as
determined using motion analysis, was generally larger
than the range of motion determined during analysis of
SIJ motion using stereophotogrammetry (Sturessonet al., 2000). This may be due to errors created by skin
deformation over bone landmarks, or the movement of
muscles close to the placement of the skin markers, such
as gluteus maximus or obliquus abdominis internus, as
they activated to create the test movement (Hungerford
et al., 2003).
4.1. Intra-subject comparisons––control group
In the control subjects hip motion toward 90� offemoral flexion produced posterior rotation of the non-
weight bearing innominate (side of hip flexion), consis-
tent with previous research (Jacob and Kissling, 1995;
Sturesson et al., 2000). A concurrent pattern of side
flexion toward the side of hip flexion, and rotation about
the vertical axis away from the side of hip flexion wasfound. In addition, a concurrent translational motion
occurred (anterior, superior and lateral) during hip
flexion. This pattern of translation is consistent with the
model of arthrokinematic motion of the SIJ proposed
by Lee (1999).
During this same movement, the weight bearing
innominate (side of single leg support) posteriorly ro-
tated; a finding consistent with previous research(Sturesson et al., 2000). In addition, this study found a
concurrent side flexion of the innominate toward, and
axial rotation away from the side of hip flexion. Pos-
terior rotation of the innominate (or sacral nutation) is
thought to occur as a consequence of the self-bracing
mechanism of the pelvis; essential for optimal load
transfer during single leg support (Snijders et al., 1993;
Vleeming et al., 1989, 1995b). A concurrent translationalmotion occurred (posterior, superior and medial) during
single leg support. Although both the non-weight bear-
ing and weight bearing innominates posteriorly rotated
during standing hip flexion, the pattern of the concur-
rent translation between the innominate and sacral
segments on the non-weight bearing and weight bearing
sides differed. This variation of translational motion

B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464 463
may reflect different patterns of muscle activation anddifferent compressive forces acting on the innominate
during single leg support. Using the Doppler imaging
system, Richardson et al. (2002) noted that a co-
contraction of multifidus and transversus abdominis
increased the stiffness of the SIJ. An optimal lumbo-
pelvic stabilisation strategy requires recruitment of these
muscles and could explain the compression (medial
translation of the innominate) noted in the controlsubjects during single leg support.
4.2. Intra-subject comparisons––posterior pelvic pain
group
During hip flexion in the subjects with posterior pelvic
pain, hip motion toward 90� of femoral flexion also
produced posterior rotation of the non-weight bearinginnominate. This pattern of motion was found on both
the symptomatic and asymptomatic side. The pattern of
side flexion, rotation, and translation of the non-weight
bearing innominate did not differ between the asymp-
tomatic and symptomatic sides.
On the side of single leg support, anterior rotation of
the weight bearing innominate occurred in subjects with
posterior pelvic pain. This pattern of motion has beennoted previously by Mens et al. (1999) during single leg
loading in patients with posterior pelvic pain. In addi-
tion, this study found that the concurrent translational
motion of the weight bearing innominate differed in
pelvic pain patients. As the innominate rotated anteri-
orly it translated inferiorly and posteriorly; a pattern
hypothesised to be consistent with less intra-pelvic
compression (Lee, 1999). It is interesting to note that inthis study, all of the subjects in the posterior pelvic pain
group reported increased symptoms with vertical load-
ing through the pelvis (standing, walking). This may
suggest they were unable to adequately compress the
weight bearing SIJ and maintain self-bracing of the
pelvis (Snijders et al., 1998) in order to control vertical
shear loads.
4.3. The two groups––inter-subject comparisons
A comparison of both the angular and translational
motion of the non-weight bearing innominate on the
side of hip flexion between control subjects and matched
subjects with posterior pelvic pain showed no significant
difference. This has important clinical relevance. Clinical
assessment of posterior rotation of the innominate onthe side of hip flexion (the stork test) as a method of
distinguishing normal joint motion from SIJ dysfunc-
tion (Mitchell, 1995) has been found to be unreliable
and unspecific (Vincent-Smith and Gibbons, 1999). This
study further validates such conclusions.
A significant difference was noted in the pattern of
angular motion of the weight bearing innominate during
single leg support when the control group (posteriorrotation) was compared to the posterior pelvic pain
group (anterior rotation). Vleeming et al. (1995b) sug-
gest that anterior rotation of the innominate (sacral
counternutation) disengages the self-bracing mechanism
of the pelvis and consequently diminishes the ability to
transfer loads between the spine and legs. The positive
clinical tests noted in the posterior pelvic pain group
may reflect their inability to posteriorly rotate theweight bearing innominate on the symptomatic side.
Alternately, subjects may have lacked the ability to
create sufficient compression due to altered motor con-
trol of the musculature known to stabilise the pelvis,
such as transversus abdominis, lumbo-sacral multifidus,
and gluteus maximus (Hungerford et al., 2003; Rich-
ardson et al., 2002).
5. Conclusions
The most significant alteration to the pattern of bone
motion between controls and subjects with posterior
pelvic pain occurred on the side of single leg support. In
the control subjects, the weight bearing innominate
posteriorly rotated and translated superiorly, posteriorlyand medial relative to the sacral segment. In the subjects
with posterior pelvic pain, the weight bearing innomi-
nate anteriorly rotated and translated inferiorly. The
results of this study suggest that posterior rotation of the
innominate is a normal component for optimal stabili-
sation of the pelvis. Anterior rotation of the innominate
is indicative of failure of the self-bracing mechanism and
load transfer through the pelvis, with a resultant de-crease in the ability to oppose vertical shear loads during
weight bearing.
Acknowledgements
The technical assistance of Ray Patton and Dr.
Richard Smith from the School of Exercise and Sports
Science, University of Sydney is acknowledged.
References
Buyruk, H.M., Snijders, C.J., Vleeming, A., Lam�eris, J.S., Holland,
W.P.J., Stam, H.J., 1995. The measurements of sacroiliac joint
stiffness with colour Doppler imaging: a study on healthy subjects.
European Journal of Radiology 21, 117–121.
Buyruk, H.M., Snijders, C.J., Vleeming, A., Lameris, J.S., Holland,
W.P.J., Stam, H.J., 1999. Measurements of sacroiliac joint stiffness
in peripartum pelvic patients with Doppler imaging of vibrations.
European Journal of Radiology 83, 159–163.
Carmichael, J., 1987. Inter and intra-examiner reliability of palpation
of the sacroiliac joint dysfunction. Journal of Manipulative and
Physiological Therapeutics 10, 164–171.

464 B. Hungerford et al. / Clinical Biomechanics 19 (2004) 456–464
Damen, L., Buyruk, H.M., Guler-Ulysal, F., Lotgering, F.K., Snijders,
C.J., Stam, H.J., 2001. Pelvic pain during pregnancy is associated
with asymmetric laxity of the sacroiliac joints. Acta Obstetricia et
Gynecologica Scandinavica 80, 1019–1024.
Damen, L., Buyruk, H.M., Guler-Uysal, F., Lotgering, F.K., Snijders,
C.J., Stam, H.J., 2002. Prognostic value of asymmetric laxity of the
sacroiliac joints in pregnancy-related pelvic pain. Spine 27, 2820.
Domholdt, E., 1993. Physical Therapy Research: Principles and
Applications. W.B Saunders Co, Philadelphia.
Fortin, J.D., Dwyer, A., West, S., Pier, J., 1994. Sacroiliac joint
referral patterns upon application of a new injection/arthrogra-
phy technique. I: Asymptomatic volunteers. Spine 19, 1475–
1482.
Gracovetsky, S., Newman, N., Pawlowsky, M., Lanzo, V., Davey, B.,
Robinson, L., 1995. A database for estimating normal spinal
motion derived from noninvasive measurements. Spine 20, 1036–
1046.
Hodges, P.W., Richardson, C.A.., 1997. Contraction of the abdominal
muscles associated with movement of the lower limb. Physical
Therapy 77, 132–144.
Hungerford, B., Gilleard, W., Hodges, P.W., 2003. Evidence of altered
lumbo-pelvic muscle recruitment in the presence of sacroiliac joint
pain. Spine 28, 1593–1600.
Jacob, H., Kissling, R., 1995. The mobility of the sacroiliac joints in
healthy volunteers between 20 and 50 years of age. Clinical
Biomechanics 10, 352–361.
Lee, D., 1999. The Pelvic Girdle: An Approach to Examination and
Treatment of the Lumbo-Pelvic-Hip Region. Churchill Living-
stone, Edinburgh.
Maslen, B., Ackland, T., 1994. Radiographic study of skin displace-
ment errors in the foot and ankle during standing. Clinical
Biomechanics 9, 291–296.
Mens, J.M.A., Vleeming, A., Snijders, C.J., Stam, H.J., Ginai, A.Z.,
1999. The active straight leg raising test and mobility of the pelvic
joints. European Spine Journal 8, 468–473.
Mens, J.M., Vleeming, A., Snijders, C.J., Koes, B., Stam, H.J., 2001.
Reliability and validity of the active straight leg raise test in
posterior pelvic pain since pregnancy. Spine 26, 1167–1171.
Mitchell, F.J., 1995. The Muscle Energy Manual, vol. 1. MET Press,
East Lansing.
O’Sullivan, P.B., Beales, D.J., Beetham, J.A., et al., 2002. Altered
motor control strategies in subjects with sacroiliac joint pain during
the active straight leg raise test. Spine 27, E1–E8.
Panjabi, M.M., 1992. The stabilising system of the spine. Part 2:
Neutral zone and stability hypothesis. Journal of Spinal Disorders
5, 390–397.
Richardson, C.A., Snijders, C.J., Hides, J.A., Damen, L., Martijn,
S.P., Storm, J., 2002. The relationship between transversus
abdominis muscles, sacroiliac joint mechanics, and low back pain.
Spine 27, 399–405.
Sim, J., Reid, N., 1999. Statistical inference by confidence intervals:
issues of interpretation and utilization. Physical Therapy 79, 186–
195.
Snijders, C.J., Ribbers, M.T., de Bakker, H.V., Stoeckart, R., Stam,
H.J., 1998. EMG recordings of abdominal and back muscles in
various standing postures: validation of a biomechanical model on
sacroiliac joint stability. Journal of Electromyography and Kine-
siology 8, 205–214.
Snijders, C.J., Vleeming, A., Stoeckart, R., 1993. Transfer of lumbo-
sacral load to iliac bones and legs. 1: Biomechanics of self-bracing
of the sacroiliac joints and its significance for treatment and
exercise. Clinical biomechanics 8, 285–294.
Sturesson, B., Uden, A., Vleeming, A., 2000. A radiological analysis of
movements of the sacroiliac joint during the standing hip flexion
test. Spine 25, 364–368.
Tylkowski, C.M., Simon, S.R., Mansour, J.M., 1982. Internal rotation
gait in spastic cerebral palsy in the hip. Paper presented at the
Proceedings of the 10th Open Scientific Meeting of the Hip Society,
St Louis. pp. 89–125.
Vincent-Smith, B., Gibbons, P., 1999. Inter-examiner and intra-
examiner reliability of the standing hip flexion test. Manual
Therapy 4, 87–93.
Vleeming, A., de Vries, H.J., Mens, J.M., van Wingerden, J.P., 2002.
Possible role of the long dorsal sacroiliac ligament in women with
peripartum pelvic pain. Acta Obstetrics Gynecology Scandinavia
81, 430.
Vleeming, A., Pool-Goudzwaard, A.L., Hammudoghlu, D., Stoeckart,
R., Snijders, C.J., Mens, J.M., 1996. The function of the long
dorsal sacroiliac ligament: its implication for understanding low
back pain. Spine 21, 556–562.
Vleeming, A., Pool-Goudzwaard, A.L., Stoeckart, R., van Wingerden,
J.P., Snijders, C.J., 1995a. The posterior layer of the thoracolum-
bar fascia: its function in load transfer from spine to legs. Spine 20,
753–758.
Vleeming, A., Snijders, C.J., Stoeckart, R., Mens, J.M., 1995b. A new
light on low back pain. Paper presented at the 2nd Interdisciplinary
World Congress on Low Back Pain, San Diego, pp. 149–168.
Vleeming, A., van Wingerden, J.P., Snijders, C.J., Stoeckart, R.,
Stijnen, T., 1989. Load application to the sacrotuberous ligament:
influences on sacroiliac joint mechanics. Clinical Biomechanics 4,
204–209.
Vleeming, A., Volkers, A.C.W., Snijders, C.J., Stoeckart, R., 1990.
Relation between form and function in the sacroiliac joint. 2:
Biomechanical aspects. Spine 15, 133–136.
Walheim, G.G., Selvik, G., 1984. Mobility of the pubic symphysis.
Clinical Orthopaedics and related Research 191, 129–135.