
ALOX5AP genetic variants and risk of atherothrombotic stroke in the Taiwanese population
5
Clinical Study ALOX5AP genetic variants and risk of atherothrombotic stroke in the Taiwanese population Jiann-Der Lee a,c , Tsong-Hai Lee b , Yen-Chu Huang b , Yeu-Jhy Chang b , Chien-Hung Chang b , Huan-Lin Hsu a , Ya-Hui Lin a , Chih-Ying Wu a , Meng Lee a , Ying-Chih Huang a , Shan-Jin Ryu b , Kuang-Ming Hsiao c,⇑ a Department of Neurology, Chang Gung Memorial Hospital at Chiayi, and Chang Gung University, Taiwan b Department of Neurology, Chang Gung Memorial Hospital at Taoyuan, and Chang Gung University, Taiwan c Department of Life Science, National Chung Cheng University, University Road, Min-Hsiung, Chiayi 168, Taiwan article info Article history: Received 7 February 2011 Accepted 28 March 2011 Keywords: Arachidonate 5-lipoxygenase-activating protein Atherosclerosis Cerebrovascular disease Single nucleotide polymorphism abstract We explored the role of variants of the arachidonate 5-lipoxygenase-activating protein (ALOX5AP) gene as factors for atherothrombotic stroke (ATS). A HapMap-based haplotype-tagging single nucleotide polymor- phism (htSNP) association study was conducted in an isolated Taiwanese population. Multivariate logistic regression analyses revealed that patients with the GG/CG genotype of rs4293222 and the AA/AG genotype of rs4360791 had a 1.61-fold (odds ratio [OR] = 1.61; 95% confidence interval [CI] = 1.02–2.56, p = 0.042) and a 1.69-fold (OR = 1.69; 95% CI = 1.00–2.86, p = 0.047) increased risk of ATS, compared with patients with the CC/GG genotype, respectively. The most common haplotype allele, GTA, was used as a reference when analyzing the association between the haplotypes related to rs4293222, rs10507391, rs12429692 and ATS. The combined frequencies of all minor variant alleles of the three selected htSNP were associated with a 44% decreased risk of ATS (OR = 0.56; 95% CI = 0.37–0.84, p = 0.005). This study provides preliminary evidence suggesting that genetic polymorphisms of ALOX5AP are associated with ATS. Ó 2011 Elsevier Ltd. All rights reserved. 1. Introduction Ischemic stroke is a complex multifactorial disorder, and the incidence increases as a function of the number of risk factors including hypertension, smoking and diabetes mellitus (DM). Evi- dence from twin, family-based studies suggests that genetic influ- ences may account for additional risk. 1 Reports indicate that inflammatory mechanisms are important in atherosclerosis and stroke. 2 A genetic variation in the components of the inflammatory response has also been implicated as a risk factor, particularly via interaction with proinflammatory conventional risk factors. 3,4 The arachidonate 5-lipoxygenase-activating protein (ALOX5AP) gene is required for the synthesis of leukotrienes, a protein family involved in inflammatory responses. 5 Leukotrienes are secreted by various types of inflammatory cells that cluster at injured sites in blood vessels, and have been implicated in the progression of ath- erosclerosis. 6 In a study led by Stefánsson et al. at deCODE genetics, Inc., a single ALOX5AP haplotype (HapA, rs17222814– rs10507391–rs4769874–rs9551963) doubled the risk of myocar- dial infarction (MI) and stroke in patients from Iceland. 7 A study in a central European population also suggested that sequence variants in the ALOX5AP gene (rs10507391) are significantly asso- ciated with stroke, particularly in males. 8 Conversely, other genetic studies that examined the association between ALOX5AP gene variants (HapA and HapB: rs17216473– rs10507391–rs9315050–rs17222842) and stroke have produced conflicting results. 9–11 Thus, the relationship between polymor- phisms in the ALOX5AP gene in different populations and ischemic stroke subtypes remains unclear. Most of the common haplotypes in the human genome occur in all ethnic populations; however, their frequencies vary significantly. In this study, we did not adopt the haplotype used in previous studies. The genotype information for ALOX5AP was downloaded from Han Chinese Bejing HapMap samples and the data were visualized using the Haploview applica- tion (Broad Institute of Harvard and MIT). 12,13 Tag-SNP to define all haplotypes with a frequency of >5% were selected from the block- by-block tags displayed in the ‘‘Haplotypes’’ window in Haploview. Due to the association between ALOX5AP and atherosclerosis, and the similar pathogenesis of atherothrombotic stroke (ATS) and MI, patients with ATS were enrolled in this study. 2. Materials and methods 2.1. Patients This study was designed and performed in accordance with the ethical principles established by the local Institutional Guidelines on Clinical Investigation. Written informed consent was provided by all study participants. 0967-5868/$ - see front matter Ó 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.jocn.2011.03.035 ⇑ Corresponding author. Tel.: +886 5 272 0411; fax: +886 5 272 2871. E-mail address: [email protected] (K.-M. Hsiao). Journal of Clinical Neuroscience 18 (2011) 1634–1638 Contents lists available at ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn
-
Upload
jiann-der-lee -
Category
Documents
-
view
217 -
download
2
Transcript of ALOX5AP genetic variants and risk of atherothrombotic stroke in the Taiwanese population

Journal of Clinical Neuroscience 18 (2011) 1634–1638
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
ALOX5AP genetic variants and risk of atherothrombotic strokein the Taiwanese population
Jiann-Der Lee a,c, Tsong-Hai Lee b, Yen-Chu Huang b, Yeu-Jhy Chang b, Chien-Hung Chang b, Huan-Lin Hsu a,Ya-Hui Lin a, Chih-Ying Wu a, Meng Lee a, Ying-Chih Huang a, Shan-Jin Ryu b, Kuang-Ming Hsiao c,⇑a Department of Neurology, Chang Gung Memorial Hospital at Chiayi, and Chang Gung University, Taiwanb Department of Neurology, Chang Gung Memorial Hospital at Taoyuan, and Chang Gung University, Taiwanc Department of Life Science, National Chung Cheng University, University Road, Min-Hsiung, Chiayi 168, Taiwan
a r t i c l e i n f o a b s t r a c t
Article history:Received 7 February 2011Accepted 28 March 2011
Keywords:Arachidonate 5-lipoxygenase-activatingproteinAtherosclerosisCerebrovascular diseaseSingle nucleotide polymorphism
0967-5868/$ - see front matter � 2011 Elsevier Ltd. Adoi:10.1016/j.jocn.2011.03.035
⇑ Corresponding author. Tel.: +886 5 272 0411; faxE-mail address: [email protected] (K.-M. Hsiao)
We explored the role of variants of the arachidonate 5-lipoxygenase-activating protein (ALOX5AP) gene asfactors for atherothrombotic stroke (ATS). A HapMap-based haplotype-tagging single nucleotide polymor-phism (htSNP) association study was conducted in an isolated Taiwanese population. Multivariate logisticregression analyses revealed that patients with the GG/CG genotype of rs4293222 and the AA/AG genotypeof rs4360791 had a 1.61-fold (odds ratio [OR] = 1.61; 95% confidence interval [CI] = 1.02–2.56, p = 0.042)and a 1.69-fold (OR = 1.69; 95% CI = 1.00–2.86, p = 0.047) increased risk of ATS, compared with patientswith the CC/GG genotype, respectively. The most common haplotype allele, GTA, was used as a referencewhen analyzing the association between the haplotypes related to rs4293222, rs10507391, rs12429692and ATS. The combined frequencies of all minor variant alleles of the three selected htSNP were associatedwith a 44% decreased risk of ATS (OR = 0.56; 95% CI = 0.37–0.84, p = 0.005). This study provides preliminaryevidence suggesting that genetic polymorphisms of ALOX5AP are associated with ATS.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction Conversely, other genetic studies that examined the association
Ischemic stroke is a complex multifactorial disorder, and theincidence increases as a function of the number of risk factorsincluding hypertension, smoking and diabetes mellitus (DM). Evi-dence from twin, family-based studies suggests that genetic influ-ences may account for additional risk.1 Reports indicate thatinflammatory mechanisms are important in atherosclerosis andstroke.2 A genetic variation in the components of the inflammatoryresponse has also been implicated as a risk factor, particularly viainteraction with proinflammatory conventional risk factors.3,4
The arachidonate 5-lipoxygenase-activating protein (ALOX5AP)gene is required for the synthesis of leukotrienes, a protein familyinvolved in inflammatory responses.5 Leukotrienes are secreted byvarious types of inflammatory cells that cluster at injured sites inblood vessels, and have been implicated in the progression of ath-erosclerosis.6 In a study led by Stefánsson et al. at deCODE genetics,Inc., a single ALOX5AP haplotype (HapA, rs17222814–rs10507391–rs4769874–rs9551963) doubled the risk of myocar-dial infarction (MI) and stroke in patients from Iceland.7 A studyin a central European population also suggested that sequencevariants in the ALOX5AP gene (rs10507391) are significantly asso-ciated with stroke, particularly in males.8
ll rights reserved.
: +886 5 272 2871..
between ALOX5AP gene variants (HapA and HapB: rs17216473–rs10507391–rs9315050–rs17222842) and stroke have producedconflicting results.9–11 Thus, the relationship between polymor-phisms in the ALOX5AP gene in different populations and ischemicstroke subtypes remains unclear. Most of the common haplotypesin the human genome occur in all ethnic populations; however,their frequencies vary significantly. In this study, we did not adoptthe haplotype used in previous studies. The genotype informationfor ALOX5AP was downloaded from Han Chinese Bejing HapMapsamples and the data were visualized using the Haploview applica-tion (Broad Institute of Harvard and MIT).12,13 Tag-SNP to define allhaplotypes with a frequency of >5% were selected from the block-by-block tags displayed in the ‘‘Haplotypes’’ window in Haploview.Due to the association between ALOX5AP and atherosclerosis, andthe similar pathogenesis of atherothrombotic stroke (ATS) and MI,patients with ATS were enrolled in this study.
2. Materials and methods
2.1. Patients
This study was designed and performed in accordance with theethical principles established by the local Institutional Guidelineson Clinical Investigation. Written informed consent was providedby all study participants.
J.-D. Lee et al. / Journal of Clinical Neuroscience 18 (2011) 1634–1638 1635
The study population comprised 291 Taiwanese patients withATS who had been consecutively admitted to the Department ofNeurology, Chang Gung Memorial Hospital, from 2008 to 2010,and 278 control participants without a history of stroke. Controlparticipants were identified from health examinations in the samehospital and had normal brain imaging studies. A chest X-ray; elec-trocardiogram; and tests for a complete blood count (hemoglobin,hematocrit, platelets, and leukocytes), blood glucose, triglycerides,and cholesterol were obtained for all patients with stroke. Patientsalso underwent a brain CT scan and/or brain MRI to define theinfarction area and to exclude any cerebral hemorrhage. Carotidultrasonography, CT angiography, magnetic resonance angiogra-phy or cerebral angiography (digital subtraction angiography)was used to evaluate steno-occlusive disease of the carotid, verte-bral and major cerebral arteries. The presence of hypertension (HT)was defined as: (i) the patient was previously diagnosed with HTby a clinician; or (ii) systolic blood pressure P140 mmHg and/ordiastolic blood pressure P90 mmHg on two separate occasions,measured after the acute stage of stroke. DM was diagnosedaccording to the National Institute of Health revised criteria(1980).14 Cigarette smoking was defined as a risk factor if a patientsmoked P10 cigarettes per day for more than 6 months before
Table 1Characteristics of patients with ALOX5AP (arachidonate 5-lipoxygenase-activating protein
Control group (n = 278)
Age (years) (mean ± SD)� 64.1 ± 11.1Male sex (%) (n)� 59.0% (164)Hypertension (%) (n)� 64.4% (179)Diabetes mellitus (%) (n)� 20.1% (56)Smoking (%) (n)� 22.3% (62)Total cholesterol (mg/dL)� 194.4 ± 34.9Triglyceride (mg/dL)� 161.0 ± 92.9LDL-C (mg/dL)� 115.8 ± 29.4HDL-C (mg/dL)� 47.4 ± 12.2VLDL-C (mg/dL)� 31.2 ± 17.3Uric acid (mg %)� 6.4 ± 1.7
ATS = atherothrombotic stroke, HDL-C = high-density lipoprotein cholesterol, LDL-C = low* p < 0.05.� Proportions were compared by chi-squared analysis.� Means were compared by Student’s t-test.
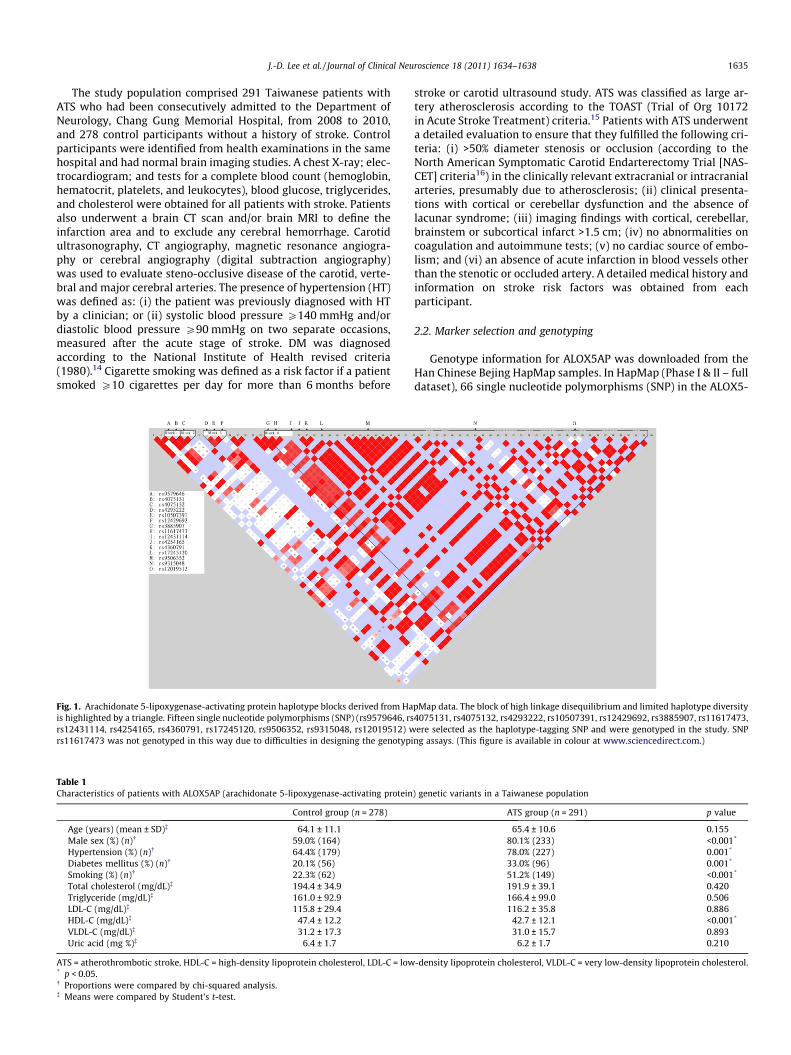
Fig. 1. Arachidonate 5-lipoxygenase-activating protein haplotype blocks derived from Hais highlighted by a triangle. Fifteen single nucleotide polymorphisms (SNP) (rs9579646, rsrs12431114, rs4254165, rs4360791, rs17245120, rs9506352, rs9315048, rs12019512) wrs11617473 was not genotyped in this way due to difficulties in designing the genotypi
stroke or carotid ultrasound study. ATS was classified as large ar-tery atherosclerosis according to the TOAST (Trial of Org 10172in Acute Stroke Treatment) criteria.15 Patients with ATS underwenta detailed evaluation to ensure that they fulfilled the following cri-teria: (i) >50% diameter stenosis or occlusion (according to theNorth American Symptomatic Carotid Endarterectomy Trial [NAS-CET] criteria16) in the clinically relevant extracranial or intracranialarteries, presumably due to atherosclerosis; (ii) clinical presenta-tions with cortical or cerebellar dysfunction and the absence oflacunar syndrome; (iii) imaging findings with cortical, cerebellar,brainstem or subcortical infarct >1.5 cm; (iv) no abnormalities oncoagulation and autoimmune tests; (v) no cardiac source of embo-lism; and (vi) an absence of acute infarction in blood vessels otherthan the stenotic or occluded artery. A detailed medical history andinformation on stroke risk factors was obtained from eachparticipant.
2.2. Marker selection and genotyping
Genotype information for ALOX5AP was downloaded from theHan Chinese Bejing HapMap samples. In HapMap (Phase I & II – fulldataset), 66 single nucleotide polymorphisms (SNP) in the ALOX5-
) genetic variants in a Taiwanese population
ATS group (n = 291) p value
65.4 ± 10.6 0.15580.1% (233) <0.001*
78.0% (227) 0.001*
33.0% (96) 0.001*
51.2% (149) <0.001*
191.9 ± 39.1 0.420166.4 ± 99.0 0.506116.2 ± 35.8 0.886
42.7 ± 12.1 <0.001*
31.0 ± 15.7 0.8936.2 ± 1.7 0.210
-density lipoprotein cholesterol, VLDL-C = very low-density lipoprotein cholesterol.
pMap data. The block of high linkage disequilibrium and limited haplotype diversity4075131, rs4075132, rs4293222, rs10507391, rs12429692, rs3885907, rs11617473,ere selected as the haplotype-tagging SNP and were genotyped in the study. SNP
ng assays. (This figure is available in colour at www.sciencedirect.com.)

Table 2ALOX5AP htSNP genotypic association results in patients with atherothromboticstroke (ATS) and control participants (adjusted by sex + HTN + DM + smoking + HDL-C)
ATS group Control group Multivariate OR(95% CI)
p value
Rs9579646 AA/GG vs AGAA 70 (24%) 69 (25%)AG 149 (52%) 139 (51%) 0.77 (0.53–1.11) 0.16GG 67 (23%) 67 (24%)Rs4075131 AA/GG vs AGAA 111 (39%) 115 (41%)AG 142 (49%) 129 (46%) 0.78 (0.54–1.12) 0.17GG 34 (12%) 34 (12%)Rs4075132 TT/CC vs CTCC 6 (2%) 7 (3%)TC 83 (29%) 72 (26%) 0.88 (0.59–1.33) 0.56TT 198 (69%) 196 (71%)Rs4293222 GG/CG vs CCCC 43 (15%) 64 (23%)CG 143 (50%) 128 (46%) 1.61 (1.02–2.56) 0.042*
GG 101 (35%) 86 (31%)Rs10507391 AA/TT vs ATAA 47 (16%) 46 (17%)TA 146 (51%) 136 (49%) 0.83 (0.57–1.19) 0.31TT 94 (33%) 96 (35%)Rs12429692 AT/TT vs AAAA 109 (38%) 117 (42%)AT 140 (49%) 123 (45%) 1.36 (0.93–1.97) 0.11TT 37 (13%) 36 (13%)Rs3885907 AA/AC vs CCAA 146 (52%) 150 (54%)AC 119 (42%) 100 (36%) 1.79 (0.90–3.57) 0.092CC 18 (6%) 28 (1%)Rs12431114 AG/GG vs AAAA 233 (81%) 235 (85%)AG 52 (18%) 42 (15%) 1.31 (0.81–2.11) 0.27GG 2 (1%) 1 (0%)Rs4254165 AG/GG vs AAAA 111 (39%) 95 (34%)AG 126 (44%) 135 (49%) 0.80 (0.55-1.16) 0.24GG 47 (17%) 47 (17%)
1636 J.-D. Lee et al. / Journal of Clinical Neuroscience 18 (2011) 1634–1638
AP gene were successfully genotyped. A Haploview analysis of the66 SNP identified four distinct haplotype blocks: hapblock 1(rs9579646–rs4075131), hapblock 2 (rs4075132), hapblock 3(rs4293222–rs10507391–rs12429692) and hapblock 4 (rs3885907–rs11617473–rs12431114–rs4254165–rs4360791–rs17245120–rs9506352–rs9315048–rs12019512) (Fig. 1). We selected a panelof 15 haplotype-tagging SNP (htSNP) for subsequent genetic asso-ciation analyses, representing all ALOX5AP haplotypes with a fre-quency >5%. This htSNP panel included the following SNP:rs9579646, rs4075131, rs4075132, rs4293222, rs10507391,rs12429692, rs3885907, rs11617473, rs12431114, rs4254165,rs4360791, rs17245120, rs9506352, rs9315048, and rs12019512.
The SNP were genotyped by primer extension of the allele-spe-cific extension products and matrix-assisted laser desorption/ioni-zation time-of-flight (MALDI-TOF; Sequenom�, San Diego, CA, USA)mass spectroscopy. SNP rs11617473 was not genotyped in thisway due to difficulties in designing the genotyping assays.
2.3. Statistical methods
The genotype frequencies of each htSNP were calculated foreach locus and tested for Hardy–Weinberg equilibrium.
Biological and clinical variables were compared between theatherothrombotic and control group using the Student’s t-testand chi-square test for continuous and categorical variables,respectively. Clinical characteristics and genotype distribution inboth groups were analyzed univariately. We performed multivari-ate logistic regression analyses adjusted for sex, hypertension, DM,smoking, and high-density lipoprotein cholesterol (HDL-C) toassess the independent contribution of genotypes and haplotypesto ATS (versus control group). The odds ratios (ORs) and 95%confidence intervals (CIs) were calculated from the b coefficientsand standard errors. A p value < 0.05 was considered statistically sig-nificant. Statistical assessments were performed using SNPstats soft-ware (http://bioinfo.iconcologia.net/index.php?module=snpstats).17
Rs4360791 AA/AG vs GGAA 111 (39%) 105 (38%)AG 137 (48%) 126 (45%) 1.69 (1.00–2.86) 0.047*
GG 35 (12%) 47 (17%)Rs17245120 CA/AA vs CCAA 2 (1%) 1 (0%)CA 51 (18%) 43 (15%) 1.18 (0.73–1.91) 0.49CC 234 (82%) 234 (84%)Rs9506352 GG/AG vs AAAA 17 (6%) 22 (8%)GA 110 (39%) 99 (36%) 1.69 (0.81–3.57) 0.16GG 158 (55%) 155 (56%)Rs9315048 GG/GT vs TTGG 163 (57%) 159 (57%)GT 111 (39%) 108 (39%) 0.66 (0.26–1.64) 0.37TT 13 (5%) 11 (4%)Rs12019512 AA/AG vs GGAA 165 (57%) 168 (61%)AG 109 (38%) 100 (36%) 0.45 (0.17–1.22) 0.11GG 14 (5%) 9 (3%)
ALOX5AP = arachidonate 5-lipoxygenase-activating protein, CI = confidence inter-val, DM = diabetes mellitus, HDL-C = high-density lipoprotein cholesterol,HTN = hypertension, htSNP = haplotype-tagging single nucleotide polymorphism,OR = odds ratio.* p < 0.05.
3. Results
This analysis included 291 patients with ATS and 278 controlparticipants. The clinical profiles of each group are shown in Ta-ble 1. Significant differences between the ATS and control groupwere observed for sex, hypertension, DM, smoking, and HDL-C.
3.1. Single-marker association
The genotype distributions of the rs9579646, rs4075131,rs4075132, rs4293222, rs10507391, rs12429692, rs3885907,rs12431114, rs4254165, rs4360791, rs17245120, rs9506352,rs9315048, and rs12019512 polymorphisms of the ATS and controlgroup are summarized in Table 2. Akaike’s information criterion(AIC) was calculated for each SNP to determine the inheritancemodel that best fitted the data (that is, a model with a low AIC va-lue would minimize the expected entropy).17
According to the AIC value, the dominant model was selected forrs12429692, rs12431114, rs4254165, and rs17245120; the reces-sive model for rs4293222, rs4360791, rs3885907, rs9506352,rs9315048, and rs12019512; and the over-dominant model forrs9579646, rs4075131, rs4075132, and rs10507391 (data notshown). The distribution of genotypes for rs4293222 andrs4360791 was significantly different between the ATS and controlgroup. However, there was no significant difference between thegroups for the other 12 SNP. The genotype frequencies forrs4293222 were 35% (GG), 50% (CG), and 15% (CC) in the ATS group;and 31% (GG), 46% (CG), and 23% (CC) in the control group. In therecessive model, the ORs associated with the GG/CG genotype were
calculated using the results of the CC carriers, who were consideredto be the reference group. The logistic regression analysis showedthat the GG/CG carriers had a 1.61-fold increased risk of ATS(OR = 1.61; 95% CI = 1.02–2.56, p = 0.042) compared to the CC carri-ers. The genotype frequencies for rs4360791 were 12% (GG), 48%(AG), and 39% (AA) in the ATS group; and 17% (GG), 45% (AG), and38% (AA) in the control group. In the recessive model, the ORs

J.-D. Lee et al. / Journal of Clinical Neuroscience 18 (2011) 1634–1638 1637
associated with the AA/AG genotype were calculated using the re-sults of the GG carriers, who were considered to be the referencegroup. The logistic regression analysis showed that the AA/AG carri-ers had a 1.69-fold increased risk of ATS (OR = 1.69; 95% CI = 1.00–2.86, p = 0.047) compared to the GG carriers (Table 2).
These data suggest that the genetic polymorphisms ofrs4293222 and rs4360791 are associated with ATS; however, thesepolymorphisms do not cause an amino acid change. They may berisk alleles or in linkage with other unknown risk alleles.
3.2. Haplotype association
To further investigate the combined effect of the 14 htSNP, weperformed haplotype analysis based on the HapMap-defined hap-lotype blocks (Fig. 1). The frequency distribution of the haplotypealleles between the ATS and control group was not significantlydifferent. However, in hapblock 3, for which the most commonhaplotype allele, GTA, was used as a reference, the combined fre-quencies of all minor variant alleles of the three selected htSNPwere associated with a 44% decreased risk of ATS (OR = 0.56; 95%CI = 0.37–0.84, p = 0.005) (Table 3).
4. Discussion
Genetic factors appear to be important in the pathogenesis ofmultifactorial stroke, but the underlying molecular mechanismsremain unclear. Clearly, a genetic component, such as Notch3, 18
cystatin C, 19 amyloid precursor protein, 20 and KRIT1, 21 is involvedin certain types of hereditary stroke. However, none of these pro-teins is involved in atherosclerosis; therefore, the correspondinggenes are probably not involved in the common forms of stroke.We report that variants in the ALOX5AP gene are associated withATS in the Taiwanese population.
ALOX5AP is an important regulator in the biosynthesis of proin-flammatory leukotrienes. A genetic variation in the ALOX5AP andLTA4H (leukotriene A4 hydrolase) genes has been shown to con-tribute to the risk of MI and stroke in the Icelandic and Scottishpopulations.7,11 Kaushal et al. reported a significant association ofvariants of ALOX5AP with ischemic stroke among a Caucasian pop-ulation, but no significant association was identified amongblacks.22 A common genetic variant (SG13S114T/A, rs10507391)in the ALOX5AP gene is reportedly associated with an increasedrisk of ATS in males in the Chinese population.23 However, a
Table 3ALOX5AP htSNP haplotype association results in patients with atherothrombotic stroke (A
LD block Haplotype� Control group (%)
Hapblock 1 GA 49AG 35AA 16Others 0
Hapblock 2 T 84C 16
Hapblock 3 GTA 52CAT 34Others 14
Hapblock 4 AAGACGGA 30CAAGCAGA 22AAAACGTG 18AGAGAGGA 4Others 16
ALOX5AP = arachidonate 5-lipoxygenase-activating protein, ATS = atherothrombotic strotein cholesterol, HTN = hypertension, htSNP = haplotype-tagging single nucleotide pRef. = reference.* p < 0.05.� Haplotypes with an estimated overall frequency of <5% were combined in other group
meta-analysis of all ALOX5AP genotyping studies showed hetero-geneity. The SG13S114 (rs10507391), SG13S89 (rs4769874),SG13S25 (rs17222814), SG13S32 (rs9551963), SG13S35(rs17222842), and SG13S42 (rs4769060) polymorphisms werenot associated with stroke. Additionally, the HapA and HapB hap-lotypes were not associated with a risk of stroke. Only theSG13S106 (rs9579646) and SG13S377 (rs17216473) polymor-phisms were marginally associated.24 We speculate that racial dif-ferences in: (i) the frequencies of the allele, genotype, and at-riskhaplotypes of the examined SNP; (ii) population linkage disequilib-rium (LD) structures; and (iii) the different pathogenesis of thestroke subtypes may partially account for the variability in thefindings of association studies.
New haplotypes may be found in a single population; therefore,choosing a suitable tag-SNP to identify haplotypes requires consid-eration of the haplotype frequencies in different populations. Wedid not use previously reported SNP and haplotypes because theseinitial studies were conducted in a Caucasian population. In ourstudy, the SNP in the ALOX5AP gene were downloaded from theHan Chinese Bejing HapMap samples and analyzed by Haploview.Thereafter, 14 htSNP were used for further association studies. Webelieve that these htSNP more precisely represent the LD structureof ALOX5AP compared to previously reported htSNP in a Taiwanesepopulation.
It has been hypothesised that increased ALOX5AP activity couldlead to an accumulation of leukotrienes in the fatty deposits on thearterial wall. The subsequent breakdown of these deposits by theimmune system may lead to the development of atherosclerosisand an increased risk of stroke.7 Relative elevations in the leuko-cyte count are associated with carotid atherosclerosis and are inde-pendently associated with an increased risk of future ischemicstroke. Importantly, the effect of inflammation on atheroscleroticand cardioembolic stroke is reportedly greater than in other strokesubtypes.25,26 In addition, Nencini et al. showed that acute inflam-matory events increase the risk of acute atherothrombotic and car-dioembolic ischemic stroke.27 These results indicate that theinflammatory process increases the risk of ATS to a greater degreecompared to that of lacunar stroke. Therefore, in order to evaluatethe genetic effect of ALOX5AP on ischemic stroke, we enrolled onlypatients with ATS and compared them with the control partici-pants in this study.
Many candidate-gene association studies have attempted toidentify genes related to stroke; however, only a few replicable
TS) and control participants (adjusted by sex + HTN + DM + smoking + HDL-C)
ATS group (%) Adjusted OR (95% CI) p value
48 1.00 (Ref.) NA35 1.08 (0.81–1.45) 0.616 0.92 (0.63–1.34) 0.661 2.55 (0.44–14.99) 0.3
83 1.00 (Ref.) NA17 0.96 (0.68–1.36) 0.807
56 1.00 (Ref.) NA35 1.01 (0.76–1.34) 0.959 0.56 (0.37–0.84) 0.005*
33 1.00 (Ref.) NA21 0.90 (0.63–1.29) 0.5721 1.30 (0.88–1.92) 0.197 1.69 (0.90–3.16) 0.118 0.72 (0.50–1.03) 0.07
ke, CI = confidence interval, DM = diabetes mellitus, HDL-C = high-density lipopro-olymorphism, LD = linkage disequilibrium, NA = not applicable, OR = odds ratio,
s.

1638 J.-D. Lee et al. / Journal of Clinical Neuroscience 18 (2011) 1634–1638
and robust associations have been reported. Stroke is a syndromecaused by a number of different pathologies, which may resultfrom different genetic predispositions. Therefore, accurate strokesubtyping is likely to be important to identify genetic associations.Patients with ATS underwent a detailed evaluation to ensure thatthey fulfilled the TOAST criteria for ATS; therefore, the patients en-rolled in this study may represent a relatively homogenous popu-lation. Precise phenotype classification may improve the successrate of future association studies.
Because the phenotype is determined by the genotype – that is,by the combination of two alleles – analysis of the single allelic fre-quency between the ATS and control group may not reflect the ex-act effect of the gene on the phenotype. Furthermore, a genotypecan affect a phenotype via different hereditary patterns includingdominant, recessive, or co-dominant. We used the AIC value tochoose the best inheritance model for each SNP.17 The effect ofthe gene on the phenotype can be better explained by analyzingthe genotype rather than the allele. Although there was no signif-icant difference in the allelic frequency between the ATS and con-trol group, the distribution of the genotypes for rs4293222 andrs4360791 was significantly different between both groups in arecessive model. Patients with the genotypes GG/CG forrs4293222 and the genotypes AA/AG for rs4360791 are at a higherrisk of ATS than are patients with the genotype CC for rs4293222and GG for rs4360791. Furthermore, rs4293222 is in strong LDwith rs10507391 (r2 = 0.909), which has been reported to be asso-ciated with ATS in a Chinese population and with ischemic strokein a central European population.8,23 In addition, when comparedto the most common haplotype, GTA, the combined frequenciesof all minor variant alleles in the three selected htSNP showed anegative association with ATS in hapblock 3 (p = 0.005).
5. Conclusion
Our HapMap-based genetic association study of ALOX5AP dem-onstrates involvement of the ALOX5AP gene in ATS. However, thisis an indirect association study, and the polymorphism in thisstudy is a surrogate for the causal locus. Further studies are re-quired to identify the true causal variants involving the abovepolymorphisms that either lie in the coding region or cause varia-tions in the regulation, expression, or differential splicing of theALOX5AP gene.
Acknowledgments
The authors acknowledge the Genomic Medicine Research CoreLaboratory of Chang Gung Memorial Hospital for technical support.This work was supported by Grants from the Chang Gung MedicineResearch Project (CMRPG – 650763, 650762, 350761).
Reference
1. Flossmann E, Schulz UG, Rothwell PM. Systematic review of methods andresults of studies of the genetic epidemiology of ischemic stroke. Stroke2004;35:212–27.
2. Libby P. Inflammation in atherosclerosis. Nature 2002;420:868–74.3. Jerrard-Dunne P, Sitzer M, Risley P, et al. Inflammatory gene load is associated
with enhanced inflammation and early carotid atherosclerosis in smokers.Stroke 2004;35:2438–43.
4. Jerrard-Dunne P, Sitzer M, Risley P, et al. Interleukin-6 promoter polymorphismmodulates the effects of heavy alcohol consumption on early carotid arteryatherosclerosis: the Carotid Atherosclerosis Progression Study (CAPS). Stroke2003;34:402–7.
5. Dixon WT, Demetrick DJ, Ohyama K, et al. Biosynthesis, glycosylation andintracellular processing of the neuroglandular antigen, a human melanoma-associated antigen. Cancer Res 1990;50:4557–65.
6. Spanbroek R, Grabner R, Lotzer K, et al. Expanding expression of the 5-lipoxygenase pathway within the arterial wall during human atherogenesis.Proc Natl Acad Sci USA 2003;100:1238–43.
7. Helgadottir A, Manolescu A, Thorleifsson G, et al. The gene encoding 5-lipoxygenase activating protein confers risk of myocardial infarction andstroke. Nat Genet 2004;36:233–9.
8. Lohmussaar E, Gschwendtner A, Mueller JC, et al. ALOX5AP gene and the PDE4Dgene in a central European population of stroke patients. Stroke 2005;36:731–6.
9. Zee RY, Cheng S, Hegener HH, et al. Genetic variants of arachidonate 5-lipoxygenase-activating protein, and risk of incident myocardial infarction andischemic stroke: a nested case-control approach. Stroke 2006;37:2007–11.
10. Meschia JF, Brott TG, Brown Jr RD, et al. Phosphodiesterase 4D and 5-lipoxygenase activating protein in ischemic stroke. Ann Neurol2005;58:351–61.
11. Helgadottir A, Gretarsdottir S, St Clair D, et al. Association between the geneencoding 5-lipoxygenase-activating protein and stroke replicated in a Scottishpopulation. Am J Hum Genet 2005;76:505–9.
12. Thorisson GA, Smith AV, Krishnan L, et al. The international HapMap projectweb site. Genome Res 2005;15:1592–3.
13. Barrett JC, Fry B, Maller J, et al. Haploview: analysis and visualization of LD andhaplotype maps. Bioinformatics 2005;21:263–5.
14. From the NIH: new standards for classification and diagnosis of diabetes. JAMA1980; 243:2296-7.
15. Adams Jr HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acuteischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trialof org 10172 in acute stroke treatment. Stroke 1993;24:35–41.
16. Fisher M, Martin A, Cosgrove M, et al. The NASCET-ACAS plaque project. NorthAmerican Symptomatic Carotid Endarterectomy Trial. Asymptomatic carotidatherosclerosis study. Stroke 1993;24:I24–5 [discussion I31–I22].
17. Sole X, Guino E, Valls J, et al. SNPStats: a web tool for the analysis of associationstudies. Bioinformatics 2006;22:1928–9.
18. Tournier-Lasserve E, Joutel A, Melki J, et al. Cerebral autosomal dominantarteriopathy with subcortical infarcts and leukoencephalopathy maps tochromosome 19q12. Nat Genet 1993;3:256–9.
19. Palsdottir A, Abrahamson M, Thorsteinsson L, et al. Mutation in cystatin c genecauses hereditary brain haemorrhage. Lancet 1988;2:603–4.
20. Levy E, Carman MD, Fernandez-Madrid IJ, et al. Mutation of the Alzheimer’sdisease amyloid gene in hereditary cerebral hemorrhage, Dutch type. Science1990;248:1124–6.
21. Gunel M, Awad IA, Anson J, et al. Mapping a gene causing cerebral cavernousmalformation to 7q11.2–q21. Proc Natl Acad Sci USA 1995;92:6620–4.
22. Kaushal R, Pal P, Alwell K, et al. Association of ALOX5AP with ischemic stroke: apopulation-based case-control study. Hum Genet 2007;121:601–7.
23. Zhang WL, Yang XM, Shi J, et al. Polymorphism of SG13S114T/A in the ALOX5APgene and the risk for stroke in a large Chinese cohort. Yi Chuan Xue Bao2006;33:678–84.
24. Zintzaras E, Rodopoulou P, Sakellaridis N. Variants of the arachidonate 5-lipoxygenase-activating protein (ALOX5AP) gene and risk of stroke: a HuGEgene-disease association review and meta-analysis. Am J Epidemiol2009;169:523–32.
25. Elkind MS, Sciacca RR, Boden-Albala B, et al. Relative elevation in baselineleukocyte count predicts first cerebral infarction. Neurology 2005;64:2121–5.
26. Elkind MS, Cheng J, Boden-Albala B, et al. Elevated white blood cell count andcarotid plaque thickness: the northern manhattan stroke study. Stroke2001;32:842–9.
27. Nencini P, Sarti C, Innocenti R, et al. Acute inflammatory events and ischemicstroke subtypes. Cerebrovasc Dis 2003;15:215–21.


















