Allergy and Allergic Diseases
21
Allergy and Allergic Diseases • Incidence steadily rising • Trebling in the last 20 years • 1/ /3 of the population will develop clinical allergic condition • Amongst the highest rates in the World • Costs – Quality of Life issues 3 million consultations costing £300 million; 70,000 Admissions costing £80 million; £1 billion drugs expenditure
description
Allergy and Allergic Diseases. Incidence steadily rising Trebling in the last 20 years 1/ /3 of the population will develop clinical allergic condition Amongst the highest rates in the World Costs – Quality of Life issues - PowerPoint PPT Presentation
Transcript of Allergy and Allergic Diseases

Allergy and Allergic Diseases
• Incidence steadily rising• Trebling in the last 20 years• 1/ /3 of the population will develop clinical
allergic condition• Amongst the highest rates in the World
• Costs – Quality of Life issues 3 million consultations costing £300
million; 70,000 Admissions costing £80 million; £1 billion drugs expenditure

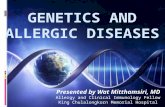
Food Allergy
Atopic Eczema Dermatitis
Allergic Rhinitis
AsthmaAge
“The Atopic March”
Infancy
Toddlers
School Age
Allergic Diseases – adverse, heightened immunological responses (hypersensitivity) to external agents
Anaphylaxis Acute Urticaria


Allergic disease prevalence
• AsthmaX 6 in ChildrenX 3-4 in Adults
Population Prevalence 12 – 15%
Atopic Dermatitis Allergic Rhinitis Food Allergy …also increasingAnaphylaxis… 7-fold

Asthma / Allergic Disease Genetics
• Strong Genetic AssociationCytokine genes – IL-4, IL-5, IL-10, TGF-
IgE receptor genesLPS responsiveness genes
Skin barrier function genes - fillagrin
Twin Concordance 75%1 affected parent - 40%
2 Affected Parents - 60%Same Disease - Even Higher
… but genes do not explain the growing prevalence

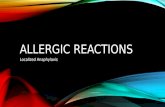
Asthma Prevalence Vs GNP per capita; adapted from ISAAC study
Asthma Epidemiology
•West Germany Vs East Germany Prevalence Studies
Inverse relationship with:
• Family Size
•Family Order
•Day Care in Early Years Outside the Home
•Place of residence – Farm / Animal exposure Vs City
Socioeconomic factors

The Hygiene Hypothesis
Centers for Disease Control, Atlanta
•Less Infectious Diseases
•More Antibiotic Use
•Better Sanitation
Western Countries
… Promotion of Allergic Immune Responses

The Infant Immune System
TH2 Bias •All Infants TH1
Increasing Age
•TH1-mediated diseases are also increasing
X2 Multiple SclerosisX3 Crohn’s Disease
•TH1 and TH2 diseases co-exist in many patients

Regulatory T
TH2 Bias •All Infants TH1
Increasing Age
IL-4, IL-5, IL-13 TNF-; IFN-; IL-10; TGF
Controlled Inflammation
The Infant Immune System – Normal Maturation

Allergy Investigation• HISTORY
• Laboratory tests (RASTs) / in-vivo – skin testing – IgE-dependent
• Challenges – Useful; Experienced; Monitored setting
• Usefulness – Disease / Interpreter
• Alternative testing – no basis in logic

Allergy Management
Anti-Inflammatory Treatments
•Corticosteroids•Leukotriene Inhibitors•Anti-histamines
Effector Antagonists-2 agonists•Adrenaline
Allergen Avoidance•Variable effects disease

Allergy Management cont./
Immune Manipulation •Conventional ImmunosuppressionVariable
Not Widespread
•Allergen Desensitization Therapy / ImmunotherapyMolecular engineering
Allergen sequencingIgG4 / TGF-production
•TH RedirectionM. Vaccae
Probiotic therapiesAllergen / Cytokine / CpG motif Conjugate “Vaccines”

Allergy Management cont. 2/
Anti-IgE Therapy Stopping the Cascade
•Humanised Mouse MAb
Omalizumab
•AsthmaReduced steroid use;
hospitalization; rescue treatments
Reduced IgE; IgE Receptor
FDA Approval 2003Incorporation in
Asthma Guidelines

+/ - Stridor; Breathing / Speaking Difficulty; Hypotension; Collapse;
GI Symptoms
ANAPHYLAXIS

Epidemiology
•Sharp increase
•Under-reported
•30 – 950 / 100,000 / year – US meta-analysis•0.5 – 2.0% lifetime prevalence•1 / 12 / year recur
•UK – 75 / 100,000 / year
•Fatalities – 1 / 2.5 million / year; lower in children

Triggers
• Potentially anything – careful history
Commonest -
• Foods – peanuts; Other tree nuts; fish and shellfish; milk
• Venoms – wasp, bee
• Drugs – penicillins; anaesthetics; ASA and NSAIDs; ACEIs
• Other Medical – Contrast media; Latex

Why Does This Happen?
Foodspeanut; egg; milk;
seafoodsDrugs
penicillins; suxamethonium; MabsLatex
Venoms


Adrenaline Autoinjectors
• UK Resuscitation Council Guidelines• Irish Consensus Document from IGI – IMJ Jan
2008– Definite
– Anaphylaxis in Asthma– Limited access to care– Trace amount triggers– Severe hypotension ( venoms)
– Probably– High incidence of Severe reactions ( nuts / shellfish)– Comorbidities
– No– Asthma alone; positive skin tests alone; clear avoidable trigger;
positive family history

Food Sensitivity and Other Allergic Disorders
• Does Food Allergy Cause Other Conditions?
• Atopic Eczema• Co-existence of conditions• High Frequency of RAST /
PST Positivity• Severe > Mild; Younger >
Older• Exclusions• Challenges
• Asthma• Severe acute reactions
• Early food allergy positively predicts later asthma
• Younger > Older• Consider in difficult asthma
• Urticaria

Asthma / Allergy Prevention
Early Allergen Exposure
•Food allergen avoidance / Breastfeeding
- food allergy prevention-Other allergic disorders ?
•Exposure to allergens in infancy e.g. house dust mite; food antigens; pollens -- IgE
productionEarly food exposure as a
preventative in at risk infants?
•Conflicting evidence re: pet exposure
•RESEARCH