
Allergic rhinitis and Acute Rhinosinusitis Evansville 09 ... · furpro\q ru qrq vhgdwlqj...
30
Wright, 2017 1 Wright, 2017 1 Treatment of Allergic Rhinitis/Acute Rhinosinusitis in Primary and Urgent Care Wendy L. Wright, MS, APRN, BC, FAANP, FAAN Adult / Family Nurse Practitioner Owner - Wright & Associates Family Healthcare Amherst, New Hampshire Owner – Wright & Associates Family Healthcare Concord, New Hampshire Owner – Partners in Healthcare Education, LLC Disclosures • Speaker Bureau: Sanofi-Pasteur, Merck, Takeda • Consultant: Pfizer, Sanofi-Pasteur, Merck, Arbor Wright, 2017 2 Wright, 2017 3 Objectives • Upon completion of this lecture, the participant will be able to: – Discuss the pathophysiology of allergic rhinitis and acute rhinosinusitis – Identify the non-pharmacologic and pharmacologic agents available for the treatment of allergic rhinitis and acute rhinosinusitis – Compare and contrast newer pharmacologic agents with older agents with regard to benefits, risks, side effects, and drug interactions.
Transcript of Allergic rhinitis and Acute Rhinosinusitis Evansville 09 ... · furpro\q ru qrq vhgdwlqj...

Wright, 2017 1
Wright, 2017 1
Treatment of Allergic Rhinitis/Acute Rhinosinusitis in Primary and Urgent Care
Wendy L. Wright, MS, APRN, BC, FAANP, FAANAdult / Family Nurse Practitioner
Owner - Wright & Associates Family HealthcareAmherst, New Hampshire
Owner – Wright & Associates Family HealthcareConcord, New Hampshire
Owner – Partners in Healthcare Education, LLC
Disclosures
• Speaker Bureau: Sanofi-Pasteur, Merck, Takeda
• Consultant: Pfizer, Sanofi-Pasteur, Merck, Arbor
Wright, 2017 2
Wright, 2017 3
Objectives
• Upon completion of this lecture, the participant will be able to:– Discuss the pathophysiology of allergic rhinitis and acute
rhinosinusitis– Identify the non-pharmacologic and pharmacologic agents
available for the treatment of allergic rhinitis and acute rhinosinusitis
– Compare and contrast newer pharmacologic agents with older agents with regard to benefits, risks, side effects, and drug interactions.

Wright, 2017 2
Wright, 2017
Impact of Allergic Rhinitis in the United States
• 17 million individuals in US have diagnosed allergic rhinitis– This accounts for 14% of the US population– Recent prevalence studies show that it may be present in
31.5% of all adults
• 10-20% of this number is children– Most common chronic medical condition of childhood
• 79.5 million Americans have undiagnosed allergic rhinitis
• Average age of onset: 10 years of age
Wright, 2017
Impact of Allergic Rhinitis in the United States
• 2 million school days lost yearly• Annual drug expenditure for allergic rhinitis is
3.4 billion dollars; + 2 billion for lost work time• Associated with an number of other conditions
including: – Otitis media, sinusitis, asthma, facial growth
abnormalities, behavioral issues, and GERD– Sleep apnea; adenoid hypertrophy, conjunctivitis
Wright, 2017
Pathophysiology of Allergic Rhinitis
• Results from repeated exposure to allergens in the individual already equipped with the genetic predisposition
• Upon exposure to an allergen, there is a release of IgE antibodies
• IgE antibody binds with the antigen • It then attaches itself to the mast cells on the nasal
and bronchial mucosa• Release of numerous chemical mediators; including
leukotrienes and histamine

Wright, 2017 3
Wright, 2017
Histamine
• Histamine is stored mainly in the mast cell• Circulated in the blood via the basophil• Causes an increase in blood flow to the affected area.
– This increase in blood flow causes the introduction of more fluids to the area
– Responsible for the increased nasal discharge, edematous mucous membranes, sneezing, itchy nose and eyes, and hives
– Also associated with airway inflammation and bronchoconstriction
Wright, 2017
Asthma and Allergic Rhinitis: Closely Related Diseases
• Similar risk factors, pathophysiology, patterns of inflammation and triggers
• Approximately 74%-80% of children and adults with asthma have associated rhinitis
• Approximately 5-15% of individuals with allergic rhinitis will develop asthma
• It is said that if you don’t treat the nose in the patient with asthma, you will never get their asthma under control
Wright, 2017
One Airway, One Disease

Wright, 2017 4
Wright, 2017
Allergic Rhinitis: A Risk Factor for Asthma
• Brown University Study– 690 students– 162 diagnosed with allergic rhinitis– 528 without allergic rhinitis– 23 years later
• Of the 162 with allergic rhinitis, 10.5% had developed asthma compared with 3.6% of those without allergic rhinitis
Settipane, RJ et al. allergy Proc. 1994; 15:21-25.
Wright, 2017
Symptoms of Allergic Rhinitis
• Nasal congestion• Sneezing• Profuse watery
discharge from nose and/or eyes
• Itching of nose, eyes, and palate
• Frequent clearing of the throat
• Nose picking• Grimacing or twitching
• Cough• Mouth breathing• Fatigue• Irritability• Decreased appetite• Decreased hearing• Hoarse voice• Decreased smell• Sniffling• Epistaxis
Wright, 2017
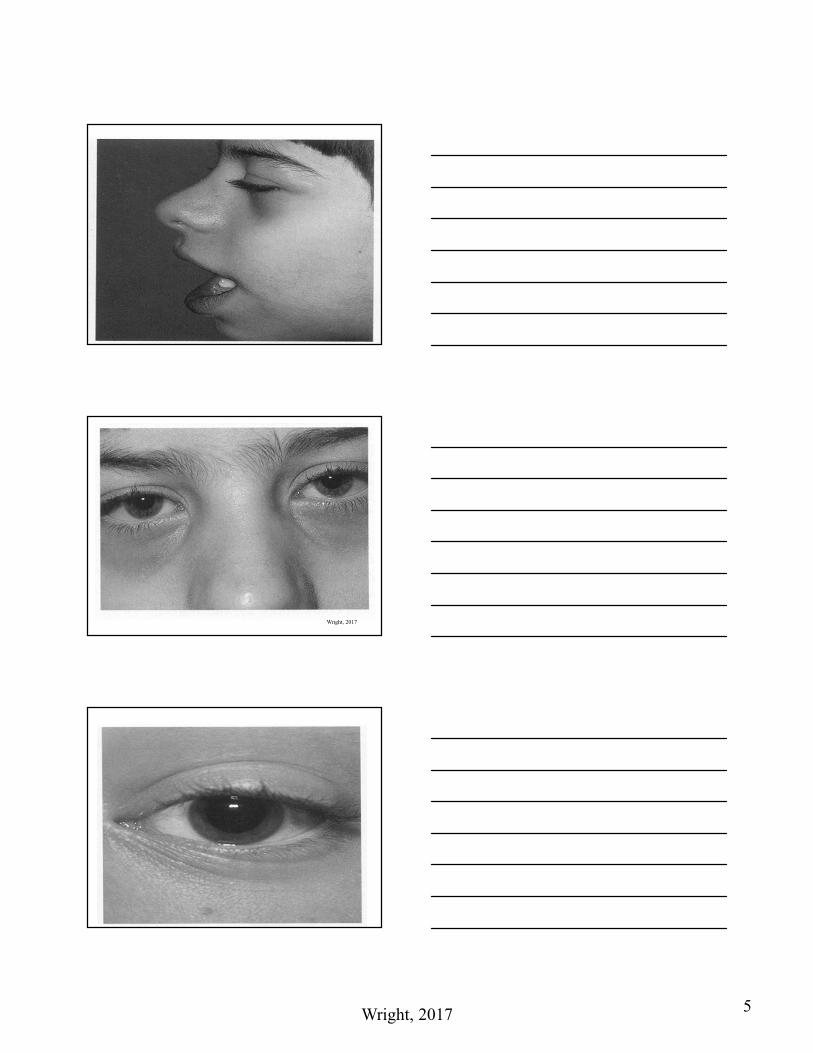
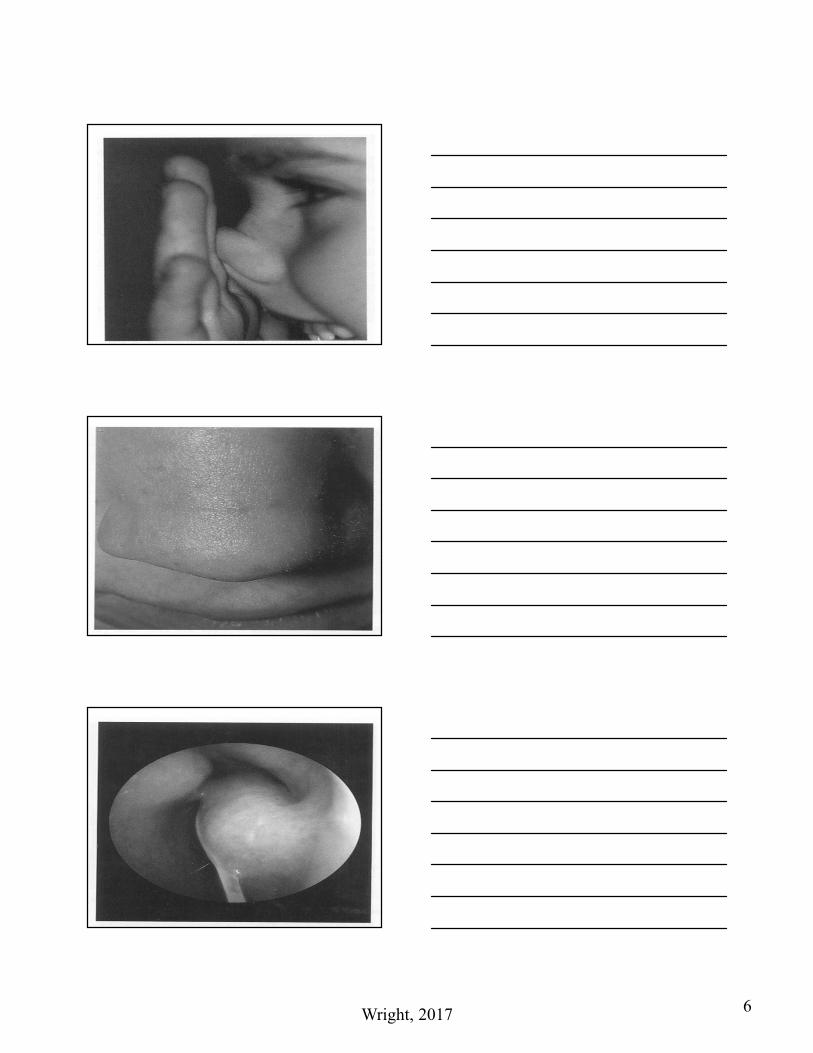
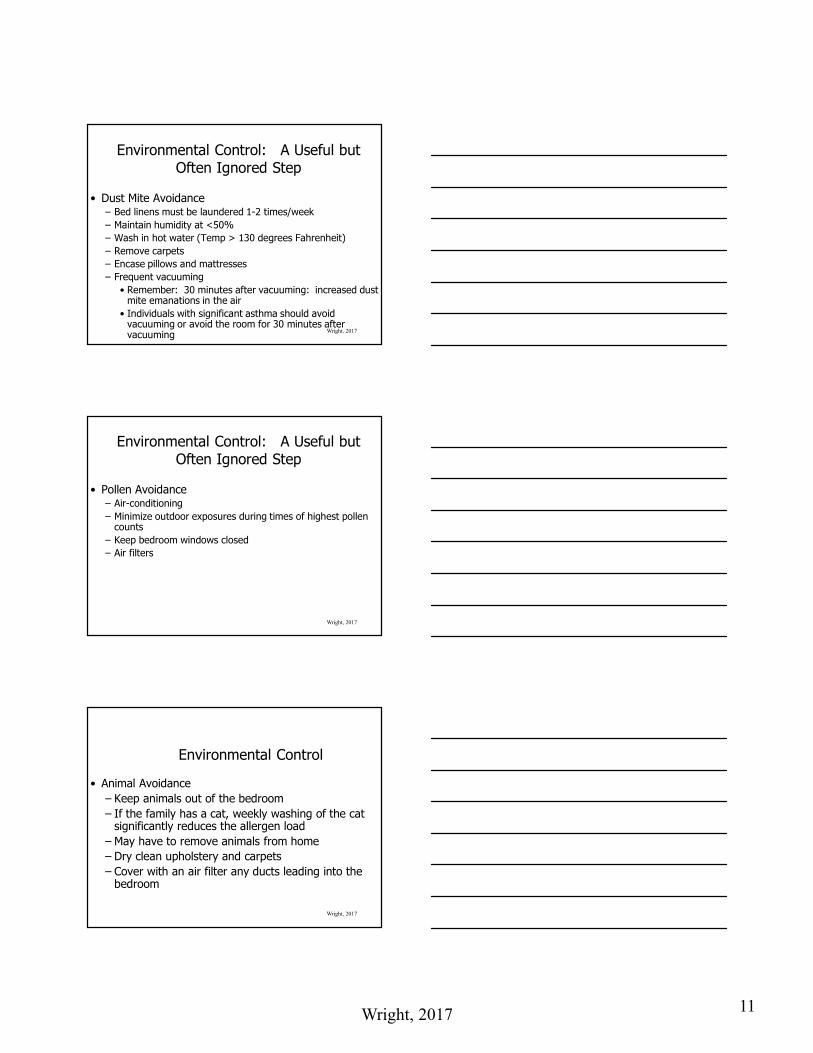
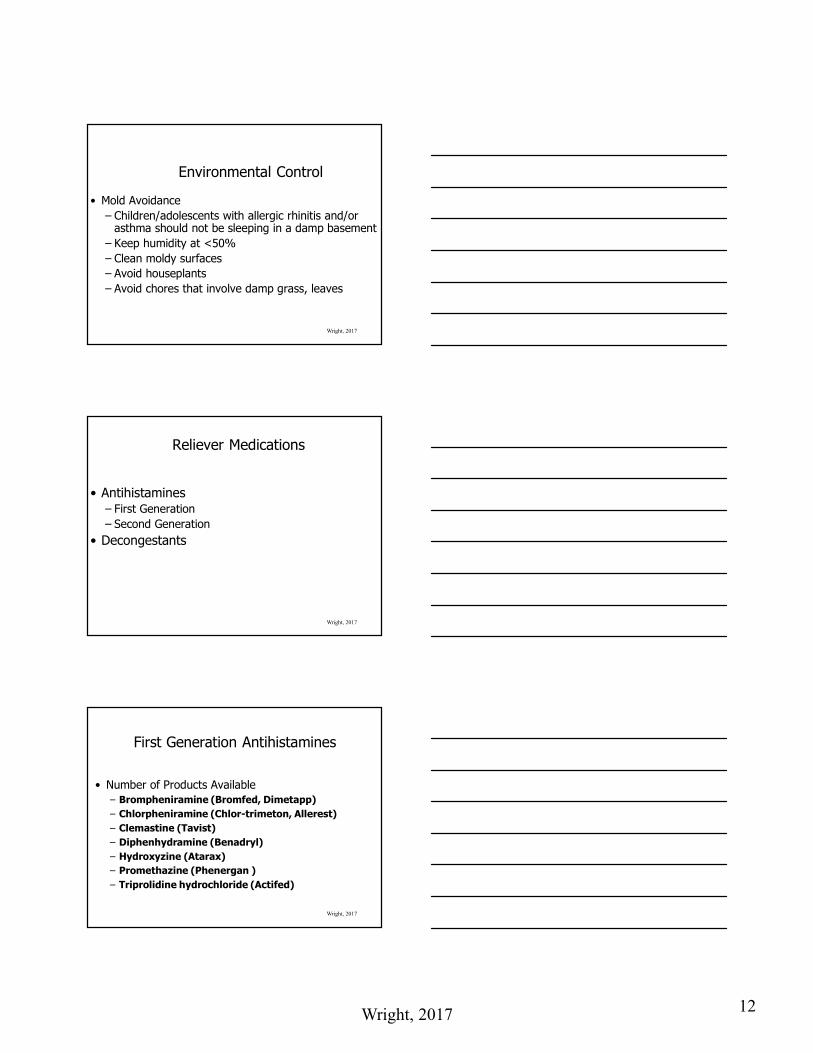
Physical Examination Findings in the Individual With Allergic Rhinitis
• Pale, boggy mucosa and turbinates
• Allergic shiners• Allergic salute• Conjunctival injection• Cobblestoning• Allergic facies• Dennie’s lines
• Watery discharge in nose and eyes
• Ulcerations on nasal mucosa
• Pharyngeal edema• Lymphoid tissue• Nasal polyps• High arched palate
Wright, 2017 5
Wright, 2017
Wright, 2017
Wright, 2017
Wright, 2017 6
Wright, 2017
Wright, 2017
Wright, 2017

Wright, 2017 7
Wright, 2017
Triggers
• Inhalant allergens are the most common triggers for both asthma and allergic rhinitis– House dust– Pollens– Mold spores– Animal and insect emanations
• Cockroach feces
Wright, 2017
Triggers
• Chemicals– Occupational setting (Carpenters, Hair Stylists)
• Perfumes• Foods
– Sulfites (wine), shrimp, dried fruit, processed potatoes, beer
Wright, 2017
Triggers
• Latex• House Plants
– Large amount of mold
• Tobacco smoke• Pollution
– Work exposures

Wright, 2017 8
Wright, 2017
Diagnosis of Allergic Rhinitis
Wright, 2017
Diagnosis of Allergic Rhinitis
• History and physical examination• Skin tests
– Exposure to a number of allergen via prick test or intradermal
– Positive response: hive or wheal within 15-20 minutes
– Up to 17% false negatives– More sensitive and specific– Yields information quickly
Wright, 2017
Diagnosis of Allergic Rhinitis
• Skin tests– Less expensive– Contraindications:
• Beta blockers– Reason: if an anaphylaxis occurs, diminished
response from epinephrine• Pregnancy• Generalized skin disorders• Currently taking antihistamines

Wright, 2017 9
Wright, 2017
Diagnosis of Allergic Rhinitis
• CAP testing
–Much more advanced than previous RAST testing
–Numerous panels available–Blood test– In vitro quantitative assay measures allergen
specific IgE in human serum
Wright, 2017
Why Treat Allergic Rhinitis:Treating Allergic Rhinitis Will Improve
Asthma
• Treatment of children with nasal steroids, nonsteroidal antiinflammatory drugs (such as cromolyn), or non-sedating antihistamines has been shown to improve lung function short and long term
Wright, 2017
Treating Allergic Rhinitis Will Improve Memory and Mood
• Study in Minnesota examined individuals with allergic rhinitis– Memory and mood were assessed during allergy
season and during non-allergy season– Untreated group showed significant reduction in
memory and mood when compared with the treatment group

Wright, 2017 10
Wright, 2017
Treatment Options
Wright, 2017
Remember…
• May need to treat the eyes in individuals with allergic rhinitis
• AND must treat the eyes and nose in children and adults with asthma...
Wright, 2017
Environmental Modification
• Environmental modification is recommended as first line therapy for the individual with allergic rhinitis
Wright, 2017 11
Wright, 2017
Environmental Control: A Useful but Often Ignored Step
• Dust Mite Avoidance – Bed linens must be laundered 1-2 times/week– Maintain humidity at <50% – Wash in hot water (Temp > 130 degrees Fahrenheit)– Remove carpets– Encase pillows and mattresses– Frequent vacuuming
• Remember: 30 minutes after vacuuming: increased dust mite emanations in the air
• Individuals with significant asthma should avoid vacuuming or avoid the room for 30 minutes after vacuuming
Wright, 2017
Environmental Control: A Useful but Often Ignored Step
• Pollen Avoidance– Air-conditioning– Minimize outdoor exposures during times of highest pollen
counts– Keep bedroom windows closed– Air filters
Wright, 2017
Environmental Control
• Animal Avoidance– Keep animals out of the bedroom– If the family has a cat, weekly washing of the cat
significantly reduces the allergen load– May have to remove animals from home– Dry clean upholstery and carpets– Cover with an air filter any ducts leading into the
bedroom
Wright, 2017 12
Wright, 2017
Environmental Control
• Mold Avoidance– Children/adolescents with allergic rhinitis and/or
asthma should not be sleeping in a damp basement– Keep humidity at <50%– Clean moldy surfaces– Avoid houseplants– Avoid chores that involve damp grass, leaves
Wright, 2017
Reliever Medications
• Antihistamines– First Generation– Second Generation
• Decongestants
Wright, 2017
First Generation Antihistamines
• Number of Products Available– Brompheniramine (Bromfed, Dimetapp)– Chlorpheniramine (Chlor-trimeton, Allerest)– Clemastine (Tavist)– Diphenhydramine (Benadryl)– Hydroxyzine (Atarax)– Promethazine (Phenergan )– Triprolidine hydrochloride (Actifed)

Wright, 2017 13
Wright, 2017
Side Effects of First Generation Antihistamines
• First generation antihistamines have been utilized since the 1950’s
• Pass readily through the blood-brain barrier• Rapidly absorbed and reach peak plasma
concentrations in 2-3 hours• Side effects; Somnolence, drowsiness, impaired
functioning, anticholinergic effects
Wright, 2017
Driving Performance Study (US)Study Design
• Single-center, randomized, double-blind, crossover study
• 40 Fall SAR patients (during season)
• 4 Treatments: – Placebo
– Fexofenadine HCl 60 mg
– Diphenhydramine 50 mg
– Alcohol (to 0.1% blood alcohol concentration)
• Simulated drivingWeiler et al. Ann Allergy Asthma Immunol1999;82:112.
Wright, 2017
Second Generation Antihistamines
• These have emerged as first line rescue medications– Loratadine (Claritin)
• 2 years and up: 5 - 10mg daily
– Desloratadine (Clarinex)• 6 months of age and up• 1 mg – 5 mg daily depending upon age

Wright, 2017 14
Wright, 2017
Second Generation Antihistamines• Fexofenadine (Allegra)
– 60mg bid; 180 mg once daily: 12 years and up– 30 mg bid: age 2 years of age – 11 years of age– 15 mg bid: 6 months – 1 year (urticaria)
• Cetirizine (Zyrtec)– 2-5 years: 2.5-5 mg daily– 6 or greater: 5-10 mg daily6
• Levocetirizine (Xyzal)– 1.25 mg once daily: 2 – 5 years of age– 2.5 mg once daily: 6 – 11 years of age– 2.5 mg – 5 mg once daily: 12 years of age and older
Wright, 2017
Decongestants may offer some benefit
• According to a survey of allergy patients who take medications more than 180 days per year– 9 out of 10 seasonal allergy patients experience
nasal congestion– Nasal congestion is the single most frustrating
symptom for seasonal allergy patients– Over 90% of seasonal allergy patients with nasal
congestion want faster relief
Source: IAS 2004
Controller Medications
• Mast Cell Stabilizers• Nasal Corticosteroids
– Preferred controller therapy• Nasal Antihistamines
– (seasonal, perennial, and allergic rhinitis)• Nasal Anticholinergics• Leukotriene Antagonists
– Recommends against using monotherapy• Accupuncture
Wright, 2017 42

Wright, 2017 15
Wright, 2017
Inhaled Nasal Corticosteroids
• Numerous Products– Beclomethasone dipropionate (Qnasal, Beconase A!) * 4
years of age and older– Budesonide (Rhinocort Aqua) **6 and older– Flunisolide (Nasarel) **6 and older– Fluticasone (Flonase, Veramyst) **4 and older– Mometasone (Nasonex) **Age 2 and older– Triamcinolone acetonide (Nasacort AQ) **2 and older– Ciclesonide (Omnaris, Zetonna) **6 years of age and older
Wright, 2017
According to the Guidelines
• Corticosteroids are first line for the person with moderate to severe allergic rhinitis
• Very potent and effective– Most corticosteroids are equally efficacious
• Many are now available OTC
Wright, 2017
Inhaled Corticosteroids
• Most potent antiinflammatory on the market• Side effects
– Nasal irritation, epistaxis
• Precautions– High dosages: Increased systemic absorption
leading to HPA axis suppression

Wright, 2017 16
Wright, 2017
Controversy Regarding Inhaled Corticosteroids
• Concern that inhaled corticosteroids are associated with hypothalamic-pituitary-adrenal suppression
• Concerns also expressed that the long-term use of these medications may be associated with an increase in cataract formation and an increase in intraocular pressure
Wright, 2017
Schenkel, E. et. al
• 98 patients randomized to either placebo or mometasone furoate aqueous nasal spray
• Ages: 3 - 9 years• After 1 year, there was no suppression of height in the
children using the nasal corticosteroid when compared with the child using placebo
Pediatrics Vol 105 No. 2 February 2000, p. 22
Wright, 2017
Mast Cell Stabilizers• Cromolyn Sodium (Nasalcrom)
– Best for children or adults with mild to moderate symptoms
– Indication: 2 years and up– 1 spray each nostril tid-qid; maximum; 6 times/day– Side effects: stinging
• Olopatadine nasal (Patanase)– 6 years of age and older– 1 spray – 2 sprays each nostril once daily

Wright, 2017 17
Wright, 2017
Leukotriene Receptor Antagonists
• Cysteinyl leukotriene production in the body has been associated with airway edema, smooth muscle constriction and the inflammatory process
• These medications block the leukotriene receptors which in turn is able to prevent inflammation and bronchoconstriction
Wright, 2017
Montelukast (Singulair)
• (Montelukast) Singulair– 4 mg tablet for children 12 months – 5 years of age– 5mg qhs for ages 6-14– 10mg qhs for ages 15 and older– Caution: mood destabilization
Other Nasal Spray Options
• Azelastine (Astelin, Astepro)• Azelastine/fluticasone (Dymista)• Ipratropium bromide (Atrovent)
Wright, 2017 51

Wright, 2017 18
Sublingual Allergen Extract
• Oralair (other products: ragwitek, grastek)– Treatment of allergic rhinitis with or without allergic
conjunctivitis– For those allergic to certain grass pollens age 10 –
65 years– First dose administered in healthcare providers
office with observation for minimum of 30 minutes• If tolerated, patient may then use at home• Once daily, initiated 4 months before allergy season
– Box warning: anaphylaxis
Wright, 2017 52
Wright, 2017
Immunotherapy
• Reserved for the most severe cases; those unresponsive to treatment, unwilling or unable to tolerate pharmacologic treatments
• Successful therapy causes an initial rise in IgE levels and then a subsequent decline in levels and symptomatology
• Treatment for 6 months or longer is required before benefits will be seen
• Entire course of treatment: 3-5 years
Acute Rhinosinusitis
Wright, 2017 54
Wright, 2017 19
Wright, 2017 55
Pathogens and Resistance
Wright, 2017 56
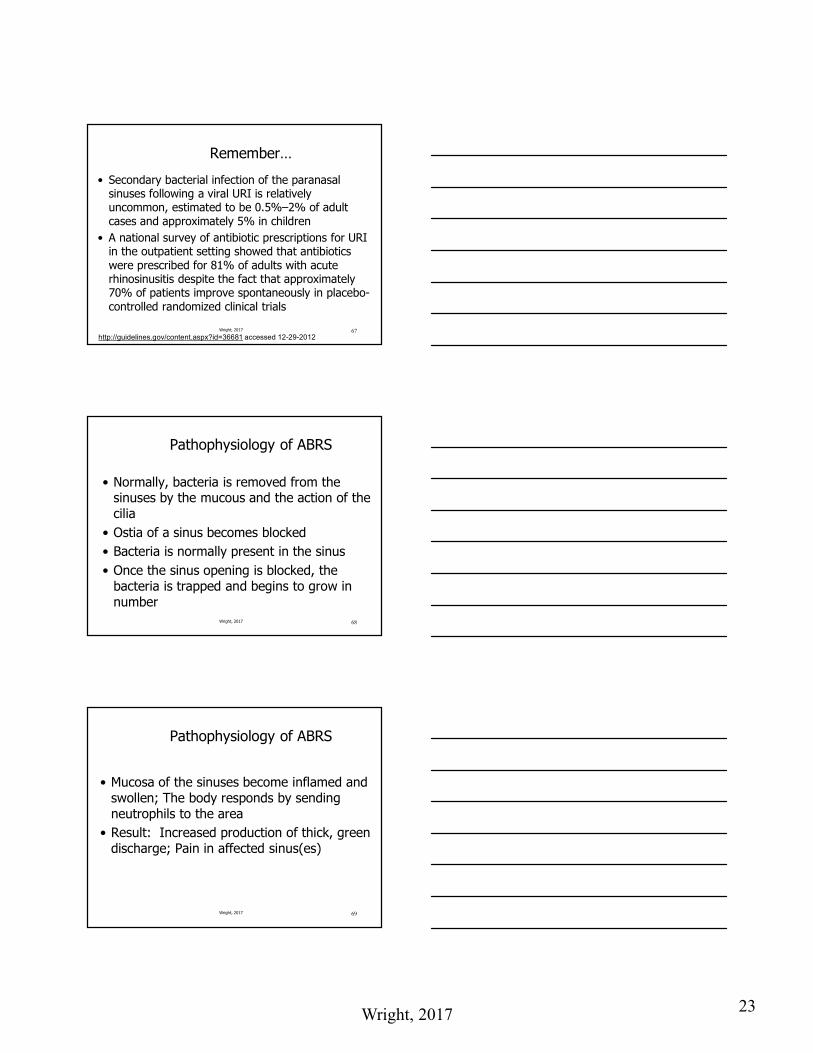
Causative Pathogens in ABRS
Streptococcus pneumoniae
Haemophilus influenzae
Moraxella catarrhalis
Major pathogens in sinusitis
Wright, 2017 57
Streptococcus pneumoniae
• Gram positive diplococci • Most common cause of Community Acquired
Pneumonia– Also the most common bacterial cause of OM
and sinusitis
• 70% of children and 30% of adults have nasopharyngeal colonization
• Disease results from a microaspiration

Wright, 2017 20
Wright, 2017 58
Mechanism for the Development of Antimicrobial Resistance
• Streptococcus pneumoniae–Many mechanisms for resistance–Most common mechanism: Resistance
from an alteration in the penicillin binding proteins which reduce/eliminate binding of penicillin to the proteins
Wright, 2017 59
Mechanism for the Development of Antimicrobial Resistance
• Streptococcus pneumoniae–Erythromycin resistance: ribosome
modification and alteration in antibiotic transport• Of increasing concern is the ermAM gene. This
gene confers cross-resistance to other 14, 15, and 16 membered rings (clarith, azith)
Wright, 2017 60
Where are we now?
• S. pneumoniae– 25% - 50% is not fully responsive to penicillin– 33% is resistant to macrolides

Wright, 2017 21
Wright, 2017 61
Of Increasing Concern…
• The first clinical isolate of S. pneumoniaeto exhibit a high level of resistance to fluoroquinolones was found in 2001 in Taiwan
Wright, 2017 62
Streptococcus pneumoniae
• Most likely to be present with recurrent disease and least likely of all pathogens to resolve without treatment
• <30% chance of spontaneous resolution; Some sources say <10%
Wright, 2017 63
H. influenzae
• Gram negative coccobacillus– Bronchotrachial tree becomes colonized and
microaspiration occurs
• Most commonly seen among smokers, children of smokers and daycare children– 33% - 35% of H. influenzae is beta lactamase producing– TRUST results (Tracking Resistance in the United States)
• 31.3% produced B lactamase in 99-2000• TMP-SMX resistance increased to 14% from 11.9%• Ampicillin resistance decreased from 33.9% to 30.7%

Wright, 2017 22
Wright, 2017 64
M. catarrhalis
• Gram negative bacillus• Implicated in recurrent OM and Sinusitis• Will often spontaneously resolve if left
untreated• 90% - 98% beta lactamase producing
Wright, 2017 65
Acute Bacterial Rhinosinusitis
Wright, 2017 66
Tammy
• 27 year old woman with an 12 day history of nasal discharge
• Seemed to be improving until past 2 days; developed worsening of post-nasal drip and pain over both cheeks. Temp past 1-2 days: 99.8 – 100.5
• Last antimicrobial use: 1 year ago• PMH: Noncontributory; No tobacco, No allergies• LMP: 2 weeks ago; denies pregnancy• PE: Nasal mucosa erythematous. Maxillary sinuses
2+ tender
Wright, 2017 23
Wright, 2017 67
Remember…
• Secondary bacterial infection of the paranasal sinuses following a viral URI is relatively uncommon, estimated to be 0.5%–2% of adult cases and approximately 5% in children
• A national survey of antibiotic prescriptions for URI in the outpatient setting showed that antibiotics were prescribed for 81% of adults with acute rhinosinusitis despite the fact that approximately 70% of patients improve spontaneously in placebo-controlled randomized clinical trials
http://guidelines.gov/content.aspx?id=36681 accessed 12-29-2012
Wright, 2017 68
Pathophysiology of ABRS
• Normally, bacteria is removed from the sinuses by the mucous and the action of the cilia
• Ostia of a sinus becomes blocked • Bacteria is normally present in the sinus• Once the sinus opening is blocked, the
bacteria is trapped and begins to grow in number
Wright, 2017 69
Pathophysiology of ABRS
• Mucosa of the sinuses become inflamed and swollen; The body responds by sending neutrophils to the area
• Result: Increased production of thick, green discharge; Pain in affected sinus(es)

Wright, 2017 24
Predisposing Factors of ABRS
Upper respiratory infections
Colds
Allergy
Smoking
Immunodeficiency syndromes
Anatomical abnormalities
Dental infections
70Wright, 2017
Diagnosis of Bacterial Acute Sinusitis
• Who should be treated with antimicrobial:– Persistent symptoms or signs compatible with acute
rhinosinusitis, lasting for ≥10 days without any evidence of clinical improvement
– Onset with severe symptoms or signs of high fever (≥39°C [102°F]) and purulent nasal discharge or facial pain lasting for at least 3–4 consecutive days at the beginning of illness
– Onset with worsening symptoms or signs characterized by the new onset of fever, headache, or increase in nasal discharge following a typical viral upper respiratory infection (URI) that lasted 5–6 days and were initially improving ("double sickening")
Wright, 2017 71http://guidelines.gov/content.aspx?id=36681 accessed 12-29-2012
Wright, 2017 72
Diagnostic Testing
• Sinus X-rays– Allows visualization of the maxillary and frontal
sinuses– Lack of specificity is a limiting factor– US Agency on Healthcare Policy – not cost effective
• CT Scan– Best visualization of the paranasal sinuses– Not recommended unless patient suspected to
have suppurative complications2
http://www.medscape.com/viewarticle/557184_2 accessed 01-28-20102http://guidelines.gov/content.aspx?id=36681 accessed 12-29-2012

Wright, 2017 25
Cultures: What and When to Recommend
• Cultures should be obtained by direct sinus aspiration rather than by nasopharyngeal swab in patients with suspected sinus infection who have failed to respond to empiric antimicrobial therapy
• Endoscopically guided cultures of the middle meatus may be considered as an alternative in adults, but their reliability in children has not been established
• Nasopharyngeal cultures are unreliable and are not recommended for the microbiologic diagnosis of ABRS
Wright, 2017 73http://guidelines.gov/content.aspx?id=36681 accessed 12-29-2012
IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis
in Children and AdultsClinical Infectious Diseases Advance
Access published March 20, 2012
Wright, 2017 74
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Wright, 2017 75
Goals of Treatment
• Restore integrity and function of ostiomeatal complex–Reduce inflammation–Restore drainage–Eradicate bacterial infection
http://www.medscape.com/viewprogram/5621 accessed 01-22-07
Wright, 2017 26
Wright, 2017 76
Treatment of Acute Bacterial Rhinosinusitis
• Nonpharmacologic Therapies– Cold steam vaporizer– Increased water intake– Intranasal saline irrigations with either
physiologic or hypertonic saline are recommended as an adjunctive treatment in adults with ABRS1
1http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Wright, 2017 77
Management Strategies in ABRS
• Antihistamines or decongestants– No longer recommended
• Topical corticosteroids– Intranasal corticosteroids are recommended as an adjunct
to antibiotics in the empiric treatment of ABRS, primarily in patients with a history of allergic rhinitis1
• Corticosteroids
1http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Wright, 2017 78
IDSA
• Who should be treated with antimicrobials– 10 or more days of illness not improving– Double sickening– 3-4 days of severe illness
1http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012

Wright, 2017 27
• First line therapy– Amoxicillin-clavulanate rather than amoxicillin alone
is recommended as empiric antimicrobial therapy for ABRS in adults and children
– Standard dosage:• 500 mg/125 mg 1 pill po three times daily or….• 875mg/125mg 1 pill two times daily
Wright, 2017 79
Initial Antimicrobial Regimenfor Adults with ABRS
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
• Individuals with B-lactam allergy– Doxycycline
• 100 mg 1 pill two times daily or 200 mg once daily or…
– Levofloxacin• 500 mg 1 pill once daily or….
– Moxifloxacin• 400 mg 1 pill once daily
Wright, 2017 80
Initial Antimicrobial Regimenfor Adults with ABRS
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Initial Antimicrobial Regimenfor Adults with ABRS (Risk for resistance)
• Second line therapy– Amoxicillin-clavulanate
• 2000mg/125 mg 1 pill two times daily or….
– Doxycycline• 100 mg 1 pill two times daily or 200 mg once daily
Wright, 2017 81
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012

Wright, 2017 28
Antimicrobial Regimen for ABRS in Adults at Risk for Resistance or Failed Initial
Therapy
– Amoxicillin-clavulanate• 2000 mg/125mg 1 pill two times daily or…
– Levofloxacin• 500 mg 1 pill once daily or….
– Moxifloxacin• 400 mg 1 pill once daily
Wright, 2017 82
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlaccessed 12-29-2012
FDA recommending
• Restrictions on fluoroquinolones for uncomplicated UTIs, bronchitis and ABRS– Ciprofloxacin, moxifloxacin, gemifloxacin,
levofloxacin and ofloxacin
http://www.consultant360.com/topic/fda-alerts accessed 05-12-2016 Wright, 2017 83
What Constitutes at Risk for Resistance?
• Age < 2 years or > 65 years• Daycare• Antimicrobial within past 1 month• Hospitalization within past 5 days• Comorbidities• Immunocompromised
Wright, 2017 84
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Wright, 2017 29
Important Changes
• Macrolides (clarithromycin and azithromycin) are not recommended due to high rates of resistance among S. pneumoniae (30%)
• TMP/SMX is not recommended due to high rates of resistance among both S. pneumoniae and H. influenzae (30%–40%)
• Second and third-generation cephalosporins are no longer recommended due to variable rates of resistance among S. pneumoniae.
Wright, 2017 85
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlaccessed 12-29-2012
Length of treatment
• The recommended duration of therapy for uncomplicated ABRS in adults is 5–7 days
• In children with ABRS, the longer treatment duration of 10–14 days is still recommended
Wright, 2017 86
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
When to Change Treatments
• An alternative treatment should be considered if symptoms worsen after 48–72 hours of initial empiric antimicrobial therapy, or when the individual fails to improve despite 3–5 days of antimicrobial therapy
Wright, 2017 87
http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012

Wright, 2017 30
When to Refer
• Recalcitrant infection• 3-4 infections in 1 year• Evaluation for immunotherapy• Severe infection• Immunocompromised host• Fungal sinusitis
Wright, 2017 88http://cid.oxfordjournals.org/content/early/2012/03/20/cid.cir1043.full.pdf+htmlAccessed 12-29-2012
Wright, 2017 89
End of Presentation!
Thank you for your time and attention.
Wendy L. Wright, MS, APRN, BC, FAANP









![RF Stability Test of RFQ Cavity with Prototype Low-level ... · WHVW ZLOO EH FRQGXFWHG IRU EHDP DFFHOHUDWLRQ :H ZLOO LPSURYH WKH UHOLDELOLW\ RI //5) DQG RSWLPL]H WKH 3,' FRHIILFLHQWV](https://static.fdocuments.in/doc/165x107/6042a59a870ea863a24b328a/rf-stability-test-of-rfq-cavity-with-prototype-low-level-whvw-zloo-eh-frqgxfwhg.jpg)
![Pediatric Refresher 2016 08-15-2016 - Moegalweb.com4healtheducation.com/pdf/EvidenceBasedPediatricGuidelines2016.pdf · 0dvw fhoo vwdelol]huv lqfoxgh furpro\q vrglxp dqg orgr[dplgh](https://static.fdocuments.in/doc/165x107/5bd9fb1609d3f2db058bbb3e/pediatric-refresher-2016-08-15-2016-0dvw-fhoo-vwdelolhuv-lqfoxgh-furproq.jpg)

![ASDRVE OSI 008 - Heathrow Airport · &odvvlilfdwlrq 3xeolf +hdwkurz v srolf\ lv wr lpsohphqw dq xowud orz hplvvlrq ]rqh iru dluvlgh yhklfohv e\ 7kh dlp lv wr lpsuryh dlu txdolw\ wkurxjk](https://static.fdocuments.in/doc/165x107/5f37729e0df4d33b31143d82/asdrve-osi-008-heathrow-airport-odvvlilfdwlrq-3xeolf-hdwkurz-v-srolf-lv.jpg)





