
Allergen Immunotherapy for Atopic Dermatitis: Is …...2016/05/15 · other allergic conditions,...
10
Pro/Con Review Allergen Immunotherapy for Atopic Dermatitis: Is There Room for Debate? Linda Cox, MD a , and Moises A. Calderon, MD, PhD b Ft. Lauderdale, Fla; and London, United Kingdom Allergen immunotherapy (AIT) is a disease-modifying inter- vention indicated for the treatment of allergic rhinitis (AR) and/ or rhinoconjunctivitis, asthma, and Hymenoptera-induced anaphylaxis. Multiple placebo-controlled trials, systematic reviews, and meta-analyses have confirmed the efficacy of AIT in these conditions. Studies suggest that AIT may be beneficial in other allergic conditions, for example, atopic dermatitis (AD), food allergy, and large local reactions to Hymenoptera sting. With the exception of AD, the use of AIT in these other conditions is considered investigational. AD has been included as a possible indication for AIT in individuals with aeroallergen sensitivity in US practice guidelines on AIT and AD. 1,2 Although the practice guideline recom- mendations are assigned an evidence rating B, 3 there continues to be debate about the effectiveness of AIT for AD. 4 One of the primary questions arising from this debate is which type of pa- tient and which allergens are most effective in AIT for AD. Is AIT effective for: all patients with AD or certain subpopulations? all aeroallergens or only specific allergens such as dust mite? At the AAAAI 2015 Annual Meeting in Houston, Texas, we debated the current evidence in favor (pro speaker: Moises A. Calderon) and against AIT for AD (con speaker: Linda Cox). The objective of this paper is to present this debate, which focused on the clinical trials and systematic reviews of AIT for AD. We aim to provide some perspective for readers to better “weigh in” on this debate. The paper also includes the discussion of AD heterogeneity (eg, different phenotypes) and the efficacy of non-AIT interventions for AD, for example, medications and avoidance measures. AD BACKGROUND AD is a complex disease with a genetic predisposition influenced by innate and adaptive immune responses to a number of envi- ronmental factors including allergens, irritants, and microbes. Although referred to as a single disease, there is considerable heterogeneity in the natural history, clinical, and biophysical fea- tures of the disease, such that it has been suggested that different phenotypes and endotypes exist, in a manner similar to asthma and rhinosinusitis subgroups. 5 AD is characterized by genetic or acquired epithelial skin barrier dysfunction, which allows for the penetration of allergens and microbes into the skin. Immune dysfunction also plays a key role in AD pathogenesis. The majority of patients with AD have elevated serum specific IgE (sIgE) and/or positive skin test reactivity (SPT) to food or inhalant allergens. In some patients, aeroallergen exposure through inhalation or direct skin contact can lead to severe AD exacerbations. 6 It is believed that an inflammatory response is initiated when allergens on the skin are internalized by IgE receptor-bearing epidermal dendritic cells. 7 This relationship between aeroallergen exposure, inflammation, and AD disease activity suggests that there may be a role for AIT in the treatment of AD. Considering the heterogeneity of AD, it is unlikely that AIT would benefit all AD phenotypes and/or endo- types. Although most patients with AD have evidence of allergen sensitivity on blood or skin test, approximately 20% do not have sIgE or SPT to any inhalant or food allergens. 5 In addition, not all positive allergy (sIgE or SPT) tests are clinically relevant. Attempts to determine an allergen’s clinical relevance can be challenging in individuals with persistent skin inflammation, particularly if the allergen is perennial. Unlike AR, where allergen sensitivity can be confirmed in an allergen environmental chamber or nasal provo- cation challenge, there are no validated tests to confirm the role of an aeroallergen in triggering AD. HOW ARE AD OUTCOMES ASSESSED? One of the challenges in evaluating the efficacy of AD treat- ment is the lack of a common standardized, validated outcome assessment tool. Generally, AD clinical trials utilize a scoring method that includes symptoms and examination findings. At present, there are more than 20 named instruments designed to measure the severity of AD. 8,9 The instruments vary in how each component is scored and weighed. Thus, it is difficult to compare the results of clinical trials utilizing different outcome tools to assess AD severity. To address this lack of standardiza- tion, an international collaboration, the Harmonising Outcome Measures for Eczema initiative, through a structured process of systematic reviews and international consensus, identified a core outcome measurement instrument for AD clinical trials. 9 The systematic review indicated that the Scoring Atopic Dermatitis (SCORAD) index and the Eczema Area and Severity Index (EASI) were the extensively validated and widely used instruments in AD clinical trials (see Figures 1 and 2 for example of the EASI and SCORAD scoring method). 10,11 The interna- tional consensus group, which included patients, health care professionals, methodologists, and pharmaceutical industry a Department of Medicine, Nova Southeastern University, Ft. Lauderdale, Fla b Imperial College London, National Heart and Lung Institute, Royal Brompton Hospital, London, United Kingdom No funding was received for this work. Conflicts of interest: The authors declare that they have no relevant conflicts. Received for publication September 28, 2015; revised December 6, 2015; accepted for publication December 18, 2015. Available online March 3, 2016. Corresponding author: Linda Cox, MD, Department of Medicine, Nova Southeastern University College of Osteopathic Medicine, 5333 North Dixie Highway, Ft. Lauderdale, FL 33334. E-mail: [email protected]. 2213-2198 Ó 2016 American Academy of Allergy, Asthma & Immunology http://dx.doi.org/10.1016/j.jaip.2015.12.018 435 Downloaded from ClinicalKey.com.au at University of Melbourne May 15, 2016. For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.
Transcript of Allergen Immunotherapy for Atopic Dermatitis: Is …...2016/05/15 · other allergic conditions,...
Pro/Con Review
Allergen Immunotherapy for Atopic Dermatitis:Is There Room for Debate?
Linda Cox, MDa, and Moises A. Calderon, MD, PhD
b Ft. Lauderdale, Fla; and London, United Kingdom
Allergen immunotherapy (AIT) is a disease-modifying inter-vention indicated for the treatment of allergic rhinitis (AR) and/or rhinoconjunctivitis, asthma, and Hymenoptera-inducedanaphylaxis. Multiple placebo-controlled trials, systematicreviews, and meta-analyses have confirmed the efficacy of AIT inthese conditions. Studies suggest that AIT may be beneficial inother allergic conditions, for example, atopic dermatitis (AD),food allergy, and large local reactions to Hymenoptera sting.With the exception of AD, the use of AIT in these otherconditions is considered investigational.
AD has been included as a possible indication for AIT inindividuals with aeroallergen sensitivity in US practice guidelineson AIT and AD.1,2 Although the practice guideline recom-mendations are assigned an evidence rating B,3 there continuesto be debate about the effectiveness of AIT for AD.4 One of theprimary questions arising from this debate is which type of pa-tient and which allergens are most effective in AIT for AD.
Is AIT effective for:
� all patients with AD or certain subpopulations?� all aeroallergens or only specific allergens such as dust mite?
At the AAAAI 2015 Annual Meeting in Houston, Texas, wedebated the current evidence in favor (pro speaker: Moises A.Calderon) and against AIT for AD (con speaker: Linda Cox).The objective of this paper is to present this debate, whichfocused on the clinical trials and systematic reviews of AIT forAD. We aim to provide some perspective for readers to better“weigh in” on this debate. The paper also includes the discussionof AD heterogeneity (eg, different phenotypes) and the efficacyof non-AIT interventions for AD, for example, medications andavoidance measures.
AD BACKGROUND
AD is a complex disease with a genetic predisposition influencedby innate and adaptive immune responses to a number of envi-ronmental factors including allergens, irritants, and microbes.
aDepartment of Medicine, Nova Southeastern University, Ft. Lauderdale, FlabImperial College London, National Heart and Lung Institute, Royal BromptonHospital, London, United Kingdom
No funding was received for this work.Conflicts of interest: The authors declare that they have no relevant conflicts.Received for publication September 28, 2015; revised December 6, 2015; acceptedfor publication December 18, 2015.
Available online March 3, 2016.Corresponding author: Linda Cox, MD, Department of Medicine, Nova SoutheasternUniversity College of Osteopathic Medicine, 5333 North Dixie Highway, Ft.Lauderdale, FL 33334. E-mail: [email protected].
2213-2198� 2016 American Academy of Allergy, Asthma & Immunologyhttp://dx.doi.org/10.1016/j.jaip.2015.12.018
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
Although referred to as a single disease, there is considerableheterogeneity in the natural history, clinical, and biophysical fea-tures of the disease, such that it has been suggested that differentphenotypes and endotypes exist, in amanner similar to asthma andrhinosinusitis subgroups.5 AD is characterized by genetic oracquired epithelial skin barrier dysfunction, which allows for thepenetration of allergens and microbes into the skin. Immunedysfunction also plays a key role in AD pathogenesis. The majorityof patients with AD have elevated serum specific IgE (sIgE) and/orpositive skin test reactivity (SPT) to food or inhalant allergens. Insome patients, aeroallergen exposure through inhalation or directskin contact can lead to severe AD exacerbations.6 It is believed thatan inflammatory response is initiatedwhen allergens on the skin areinternalized by IgE receptor-bearing epidermal dendritic cells.7
This relationship between aeroallergen exposure, inflammation,and AD disease activity suggests that there may be a role for AIT inthe treatment of AD. Considering the heterogeneity of AD, it isunlikely that AIT would benefit all AD phenotypes and/or endo-types. Although most patients with AD have evidence of allergensensitivity on blood or skin test, approximately 20% do not havesIgE or SPT to any inhalant or food allergens.5 In addition, not allpositive allergy (sIgE or SPT) tests are clinically relevant. Attemptsto determine an allergen’s clinical relevance can be challenging inindividuals with persistent skin inflammation, particularly if theallergen is perennial. Unlike AR, where allergen sensitivity can beconfirmed in an allergen environmental chamber or nasal provo-cation challenge, there are no validated tests to confirm the role ofan aeroallergen in triggering AD.
HOW ARE AD OUTCOMES ASSESSED?One of the challenges in evaluating the efficacy of AD treat-
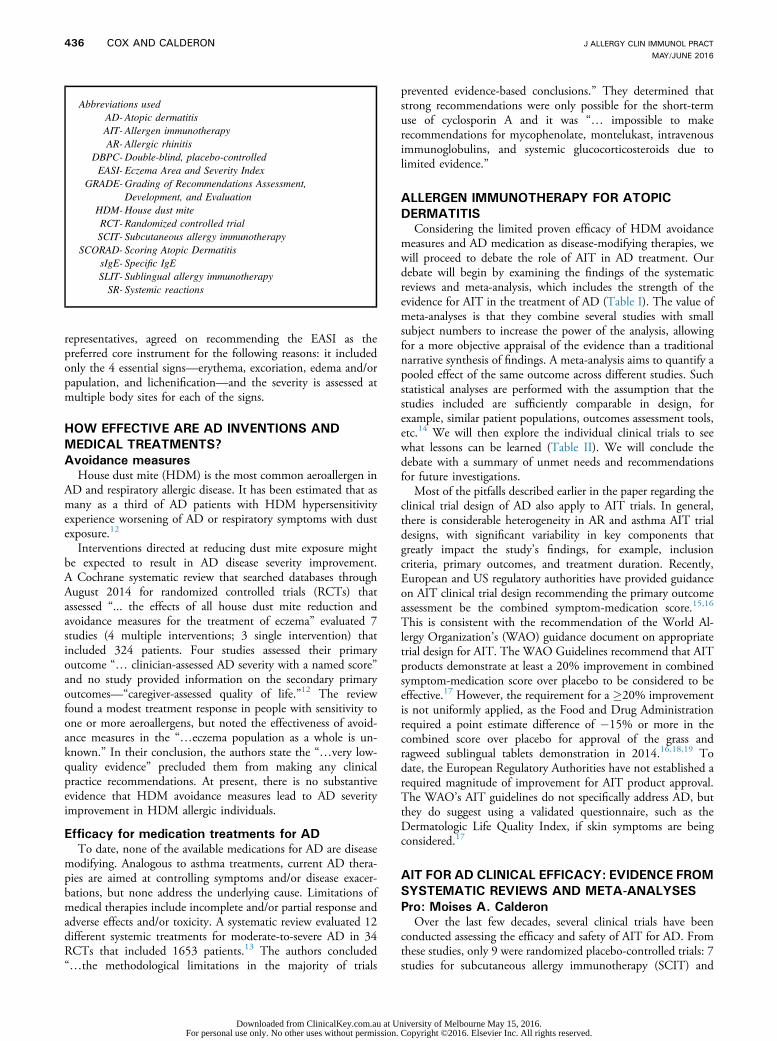
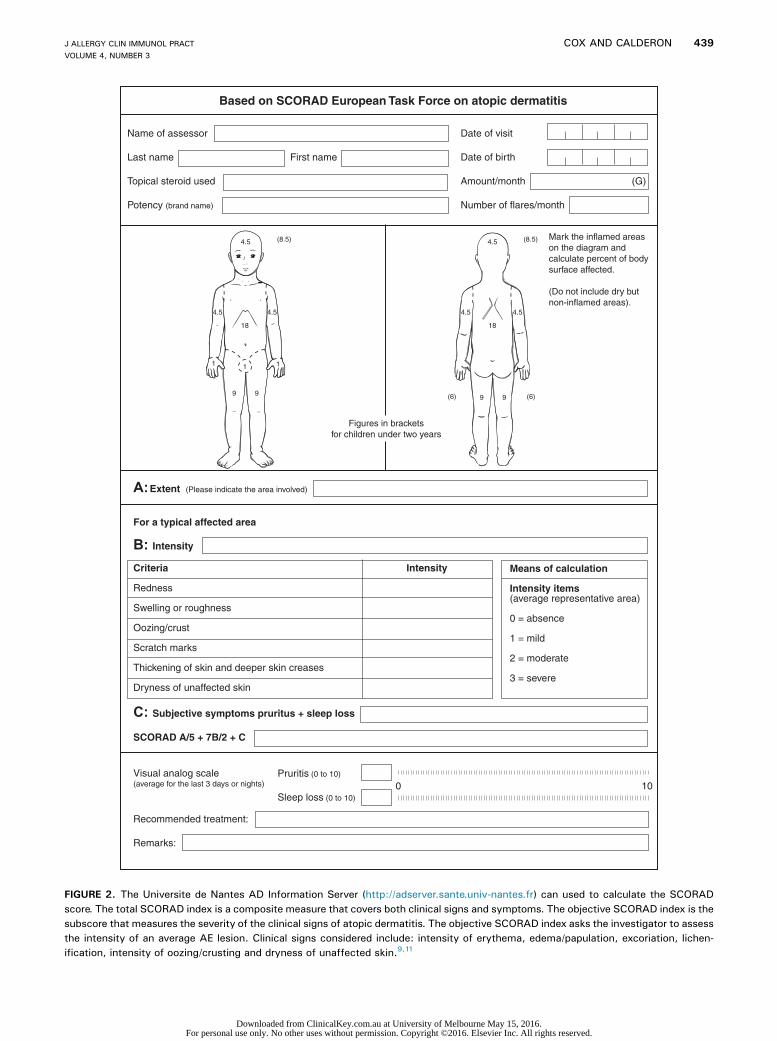
ment is the lack of a common standardized, validated outcomeassessment tool. Generally, AD clinical trials utilize a scoringmethod that includes symptoms and examination findings. Atpresent, there are more than 20 named instruments designed tomeasure the severity of AD.8,9 The instruments vary in how eachcomponent is scored and weighed. Thus, it is difficult tocompare the results of clinical trials utilizing different outcometools to assess AD severity. To address this lack of standardiza-tion, an international collaboration, the Harmonising OutcomeMeasures for Eczema initiative, through a structured process ofsystematic reviews and international consensus, identified a coreoutcome measurement instrument for AD clinical trials.9 Thesystematic review indicated that the Scoring Atopic Dermatitis(SCORAD) index and the Eczema Area and Severity Index(EASI) were the extensively validated and widely usedinstruments in AD clinical trials (see Figures 1 and 2 for exampleof the EASI and SCORAD scoring method).10,11 The interna-tional consensus group, which included patients, health careprofessionals, methodologists, and pharmaceutical industry
435
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.
J ALLERGY CLIN IMMUNOL PRACTMAY/JUNE 2016
436 COX AND CALDERON
Abbreviations used
AD- A topic dermatitis AIT- A llergen immunotherapy AR- A llergic rhinitisDBPC-D
ouble-blind, placebo-controlled EASI- E czema Area and Severity IndexGRADE-G
rading of Recommendations Assessment,Development, and EvaluationHDM-H
ouse dust mite RCT- R andomized controlled trial SCIT- S ubcutaneous allergy immunotherapySCORAD- S
coring Atopic Dermatitis sIgE- S pecific IgE SLIT- S ublingual allergy immunotherapy SR- S ystemic reactionsrepresentatives, agreed on recommending the EASI as thepreferred core instrument for the following reasons: it includedonly the 4 essential signs—erythema, excoriation, edema and/orpapulation, and lichenification—and the severity is assessed atmultiple body sites for each of the signs.
HOW EFFECTIVE ARE AD INVENTIONS AND
MEDICAL TREATMENTS?
Avoidance measuresHouse dust mite (HDM) is the most common aeroallergen in
AD and respiratory allergic disease. It has been estimated that asmany as a third of AD patients with HDM hypersensitivityexperience worsening of AD or respiratory symptoms with dustexposure.12
Interventions directed at reducing dust mite exposure mightbe expected to result in AD disease severity improvement.A Cochrane systematic review that searched databases throughAugust 2014 for randomized controlled trials (RCTs) thatassessed “... the effects of all house dust mite reduction andavoidance measures for the treatment of eczema” evaluated 7studies (4 multiple interventions; 3 single intervention) thatincluded 324 patients. Four studies assessed their primaryoutcome “. clinician-assessed AD severity with a named score”and no study provided information on the secondary primaryoutcomes—“caregiver-assessed quality of life.”12 The reviewfound a modest treatment response in people with sensitivity toone or more aeroallergens, but noted the effectiveness of avoid-ance measures in the “.eczema population as a whole is un-known.” In their conclusion, the authors state the “.very low-quality evidence” precluded them from making any clinicalpractice recommendations. At present, there is no substantiveevidence that HDM avoidance measures lead to AD severityimprovement in HDM allergic individuals.
Efficacy for medication treatments for AD
To date, none of the available medications for AD are diseasemodifying. Analogous to asthma treatments, current AD thera-pies are aimed at controlling symptoms and/or disease exacer-bations, but none address the underlying cause. Limitations ofmedical therapies include incomplete and/or partial response andadverse effects and/or toxicity. A systematic review evaluated 12different systemic treatments for moderate-to-severe AD in 34RCTs that included 1653 patients.13 The authors concluded“.the methodological limitations in the majority of trials
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
prevented evidence-based conclusions.” They determined thatstrong recommendations were only possible for the short-termuse of cyclosporin A and it was “. impossible to makerecommendations for mycophenolate, montelukast, intravenousimmunoglobulins, and systemic glucocorticosteroids due tolimited evidence.”
ALLERGEN IMMUNOTHERAPY FOR ATOPIC
DERMATITISConsidering the limited proven efficacy of HDM avoidance
measures and AD medication as disease-modifying therapies, wewill proceed to debate the role of AIT in AD treatment. Ourdebate will begin by examining the findings of the systematicreviews and meta-analysis, which includes the strength of theevidence for AIT in the treatment of AD (Table I). The value ofmeta-analyses is that they combine several studies with smallsubject numbers to increase the power of the analysis, allowingfor a more objective appraisal of the evidence than a traditionalnarrative synthesis of findings. A meta-analysis aims to quantify apooled effect of the same outcome across different studies. Suchstatistical analyses are performed with the assumption that thestudies included are sufficiently comparable in design, forexample, similar patient populations, outcomes assessment tools,etc.14 We will then explore the individual clinical trials to seewhat lessons can be learned (Table II). We will conclude thedebate with a summary of unmet needs and recommendationsfor future investigations.
Most of the pitfalls described earlier in the paper regarding theclinical trial design of AD also apply to AIT trials. In general,there is considerable heterogeneity in AR and asthma AIT trialdesigns, with significant variability in key components thatgreatly impact the study’s findings, for example, inclusioncriteria, primary outcomes, and treatment duration. Recently,European and US regulatory authorities have provided guidanceon AIT clinical trial design recommending the primary outcomeassessment be the combined symptom-medication score.15,16
This is consistent with the recommendation of the World Al-lergy Organization’s (WAO) guidance document on appropriatetrial design for AIT. The WAO Guidelines recommend that AITproducts demonstrate at least a 20% improvement in combinedsymptom-medication score over placebo to be considered to beeffective.17 However, the requirement for a �20% improvementis not uniformly applied, as the Food and Drug Administrationrequired a point estimate difference of �15% or more in thecombined score over placebo for approval of the grass andragweed sublingual tablets demonstration in 2014.16,18,19 Todate, the European Regulatory Authorities have not established arequired magnitude of improvement for AIT product approval.The WAO’s AIT guidelines do not specifically address AD, butthey do suggest using a validated questionnaire, such as theDermatologic Life Quality Index, if skin symptoms are beingconsidered.17
AIT FOR AD CLINICAL EFFICACY: EVIDENCE FROM
SYSTEMATIC REVIEWS AND META-ANALYSES
Pro: Moises A. CalderonOver the last few decades, several clinical trials have been
conducted assessing the efficacy and safety of AIT for AD. Fromthese studies, only 9 were randomized placebo-controlled trials: 7studies for subcutaneous allergy immunotherapy (SCIT) and
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.
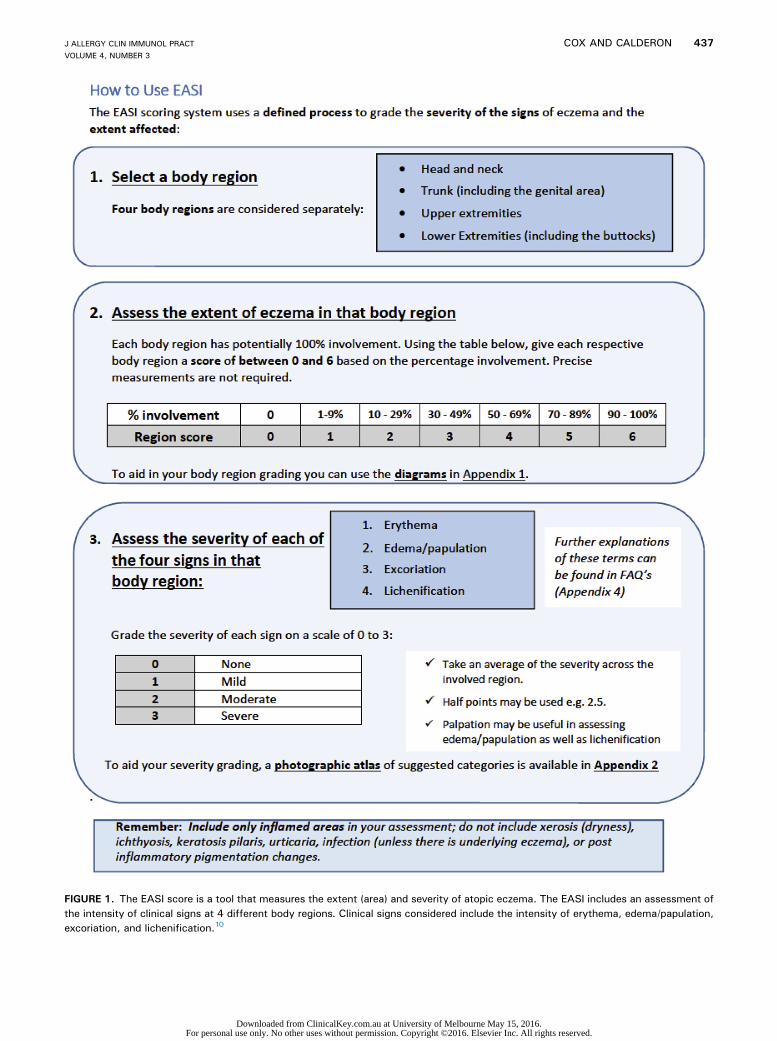
FIGURE 1. The EASI score is a tool that measures the extent (area) and severity of atopic eczema. The EASI includes an assessment ofthe intensity of clinical signs at 4 different body regions. Clinical signs considered include the intensity of erythema, edema/papulation,excoriation, and lichenification.10
J ALLERGY CLIN IMMUNOL PRACTVOLUME 4, NUMBER 3
COX AND CALDERON 437
Downloaded from ClinicalKey.com.au at University of Melbourne May 15, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.
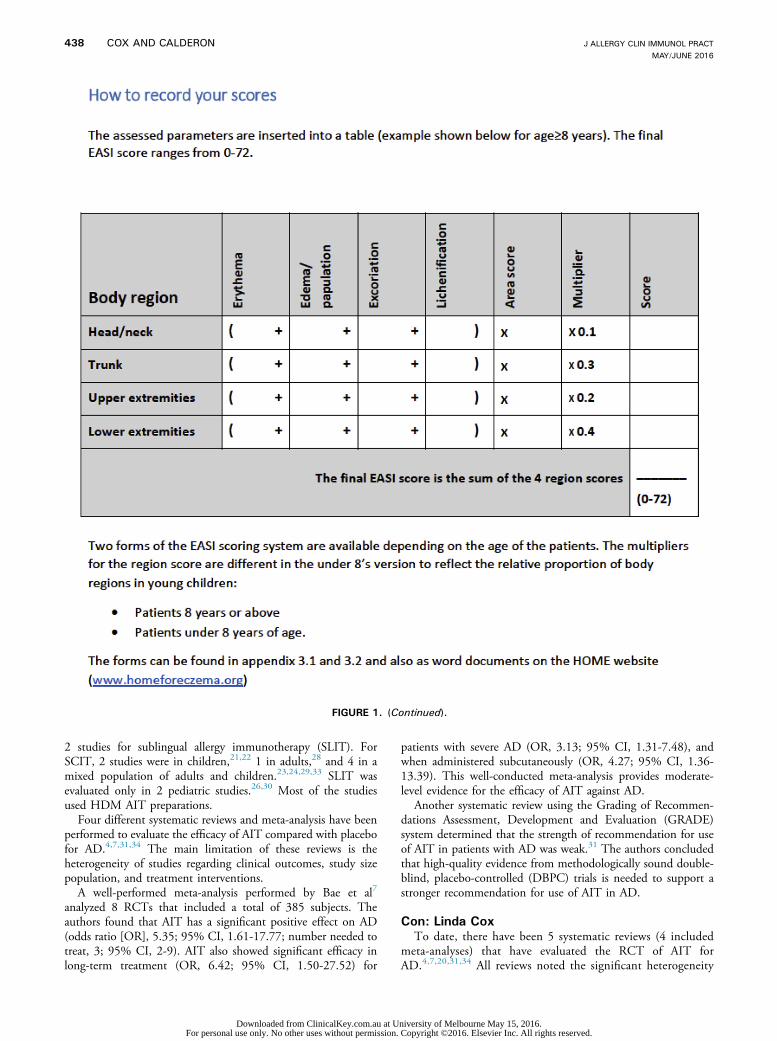
FIGURE 1. (Continued).
J ALLERGY CLIN IMMUNOL PRACTMAY/JUNE 2016
438 COX AND CALDERON
2 studies for sublingual allergy immunotherapy (SLIT). ForSCIT, 2 studies were in children,21,22 1 in adults,28 and 4 in amixed population of adults and children.23,24,29,33 SLIT wasevaluated only in 2 pediatric studies.26,30 Most of the studiesused HDM AIT preparations.
Four different systematic reviews and meta-analysis have beenperformed to evaluate the efficacy of AIT compared with placebofor AD.4,7,31,34 The main limitation of these reviews is theheterogeneity of studies regarding clinical outcomes, study sizepopulation, and treatment interventions.
A well-performed meta-analysis performed by Bae et al7
analyzed 8 RCTs that included a total of 385 subjects. Theauthors found that AIT has a significant positive effect on AD(odds ratio [OR], 5.35; 95% CI, 1.61-17.77; number needed totreat, 3; 95% CI, 2-9). AIT also showed significant efficacy inlong-term treatment (OR, 6.42; 95% CI, 1.50-27.52) for
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
patients with severe AD (OR, 3.13; 95% CI, 1.31-7.48), andwhen administered subcutaneously (OR, 4.27; 95% CI, 1.36-13.39). This well-conducted meta-analysis provides moderate-level evidence for the efficacy of AIT against AD.
Another systematic review using the Grading of Recommen-dations Assessment, Development and Evaluation (GRADE)system determined that the strength of recommendation for useof AIT in patients with AD was weak.31 The authors concludedthat high-quality evidence from methodologically sound double-blind, placebo-controlled (DBPC) trials is needed to support astronger recommendation for use of AIT in AD.
Con: Linda Cox
To date, there have been 5 systematic reviews (4 includedmeta-analyses) that have evaluated the RCT of AIT forAD.4,7,20,31,34 All reviews noted the significant heterogeneity
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.
Based on SCORAD European Task Force on atopic dermatitis
Name of assessor
First name
Topical steroid used
Potency (brand name)
A: Extent (Please indicate the area involved)
For a typical affected area
B: Intensity
Intensity
Swelling or roughness
Oozing/crust
Scratch marks
Thickening of skin and deeper skin creases
Dryness of unaffected skin
C: Subjective symptoms pruritus + sleep loss
SCORAD A/5 + 7B/2 + C
Visual analog scale (average for the last 3 days or nights)
Recommended treatment:
Remarks:
Means of calculation
Intensity items(average representative area)
0 = absence
1 = mild
2 = moderate
3 = severe
Date of visit
Date of birth
(G)
Number of flares/month
Pruritis (0 to 10)
Sleep loss (0 to 10)0 10
(8.5)
(6) (6)
(8.5)
Figures in bracketsfor children under two years
Mark the inflamed areason the diagram and calculate percent of bodysurface affected.
(Do not include dry butnon-inflamed areas).
4.5 4.5
4.54.5 4.54.5
18 18
11 1
9999
FIGURE 2. The Universite de Nantes AD Information Server (http://adserver.sante.univ-nantes.fr) can used to calculate the SCORADscore. The total SCORAD index is a composite measure that covers both clinical signs and symptoms. The objective SCORAD index is thesubscore that measures the severity of the clinical signs of atopic dermatitis. The objective SCORAD index asks the investigator to assessthe intensity of an average AE lesion. Clinical signs considered include: intensity of erythema, edema/papulation, excoriation, lichen-ification, intensity of oozing/crusting and dryness of unaffected skin.9,11
J ALLERGY CLIN IMMUNOL PRACTVOLUME 4, NUMBER 3
COX AND CALDERON 439
Downloaded from ClinicalKey.com.au at University of Melbourne May 15, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

J ALLERGY CLIN IMMUNOL PRACTMAY/JUNE 2016
440 COX AND CALDERON
and considerable variations in the included studies’ treatmentprotocols. The first systematic review of AIT for AD foundsome improvement in objective and subjective findings in the5 DBPC studies analyzed.25 In one study, a significantimprovement was only seen in the mild-to-moderate groupafter 9 months of treatment, whereas there was no improve-ment in the severe group at any time point.26 The first sys-tematic review concluded that even though the positive effectof AIT on AD seemed to predominate, “no general conclusionon the value of AIT in AD can be drawn at present.”20
Compalati et al4 performed a subsequent systematic reviewthat included 4 additional RCT studies (2 SCIT and 2 SLIT).They found variable improvement in AD severity, but notedthe methodological interstudy heterogeneity and shortcomingsin the available trials, which included small dimensions andincomplete reporting. They concluded that “. the evidenceof efficacy has not critically changed from previous systematicobservations.”
The most favorable systematic review conducted by Baeet al7 included a total of 8 RCTs of 385 patients, who receivedeither SCIT (6 studies; 177 patients), SLIT (2 studies; 42 pa-tients), or placebo (166 patients). The primary outcomeconsidered was “. the proportion of patients whose conditionimproved, as assessed by the investigators or patients, regardlessof different evaluation methods” and the evidence rating wasbased on the GRADE system. The authors concluded that therewas moderate-level evidence for the efficacy of AIT in ADtreatment, but noted that this determination was based on asmall number of RCTs with considerable heterogeneity. Sub-group analysis found a significant effect with SCIT, in severeAD, and longer treatment duration, whereas no effect wasfound in children or with SLIT. The GRADE method was alsoused in a systematic review conducted by Gendelman andLang.31 Despite using the same grading methodology andnearly the same database—5 of the 7 studies included in theBae et al review—they reach a different conclusion. Theydetermined that the strength of recommendation for use of AITin AD is weak. They also noted that there were “seriousmethodological shortcomings. including, but not limited to,many enrolled patients not completing participation; smallstudy [size]; and incomplete descriptions of randomization,blinding, allocation concealment, and/or data analysis not byintention to treat.”31
LESSONS LEARNED FROM INDIVIDUAL STUDIES
Pro: Moises CalderonThe efficacy of 18-month treatment with HDM SLIT for AD
was evaluated in an RCT of 56 children aged 5 to 16 years.26
A significant improvement versus baseline SCORAD was seenonly in the SLIT group starting from month 9. There was also asignificant reduction in the use of medications only in the SLITgroup. A separate subgroup analysis of patients with mild-moderate (SCORAD < 40) and severe (SCORAD > 40) ADwas performed. A significant improvement in consideredparameters was only found in patients with a mild-moderatedisease, whereas patients with a severe disease had only a mar-ginal benefit.
The efficacy of HDM SCIT with the use of depigmentedpolymerized extract as an add-on therapy to usual (eg, topicaland, as necessary, systemic) medication was assessed in a phase
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
III RCT of 168 adults with AD aggravated by HDM.28 Theprimary study end points were the assessments of the totalSCORAD score’s area under the curves and medication useduring the 18-month treatment period. Interestingly, theoverall efficacy analysis of the intention-to-treat and per-protocol study populations showed no statistically significantdifferences between the active treatment and placebo groups.However, the subgroup of patients with severe AD (SCORAD> 50) showed a statistically significant reduction of the mediantotal SCORAD by 18% (P ¼ .02) compared with placebo.Results were significant when data were evaluated during thewinter season.
In general, these studies suggest that AIT (both SCIT andSLIT) is an effective treatment for some patients with AD.However, it is unclear from the current literature to whichAD subpopulation AIT is most indicated. We have learnedthat the selection of patients according to severity isfundamental.
Con: Linda Cox
It is generally accepted that the evidence for a medical treat-ment efficacy must be established in appropriately designedplacebo-controlled clinical trials. It is clear from the above dis-cussion of the systematic reviews conducted to date that there is apaucity of such evidence supporting the role of AIT in ADtreatment. Only 7 DBPC trials were identified in the mostlyfavorable systematic reviews, all of which noted the considerablelimitations of their analyses due to the heterogeneity andmethodological shortcomings in the trials that met criteria forconsideration. However, the findings from individual studiesmay help determine which AD patients will benefit from whichAIT protocols.
For example, although Novak et al28 found no statisticallysignificant overall effect of SCIT in a DBPC study of 168 adultswith HDM-aggravated AD, post hoc analysis showed a signifi-cant reduction in median total SCORAD scores (18%) in thesevere AD (SCORAD > 50) subgroup.
This might suggest that only patients with severe AD wouldbenefit from AIT. However, the opposite effect was found inPajno et al26 evaluating the efficacy of HDM SLIT in childrenwith AD. In this DBPC study of 56 children (28 SLIT), thesignificant improvement in SCORAD scores was found only inthe subgroup with mild-moderate AD, whereas only a marginalbenefit was seen in patients with severe AD.
In addition to demonstrating efficacy compared with placebo,medications generally need to demonstrate a dose response. Thisdose-response requirement is applicable to SLIT and SCIT forAR and/or asthma. To date, there has been only 1 dose-responsestudy of AIT for AD.25 This RCT evaluated the effect onSCORAD scores and topical corticosteroid use of 3 doses ofSCIT administered weekly for 1 year. Although both outcomeparameters improved in a dose-dependent manner, the lack of aplacebo group would preclude this study from being consideredin many systematic reviews, which are the basis for most practiceguideline recommendations.
In closing, these individual studies provide conflicting data onwhich the subgroup of AD patients would benefit from AIT.Although a dose response is suggested, clearly more research isneeded to identify the optimal AIT dose and/or dosing regimenand AD subgroup most likely to benefit.
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.
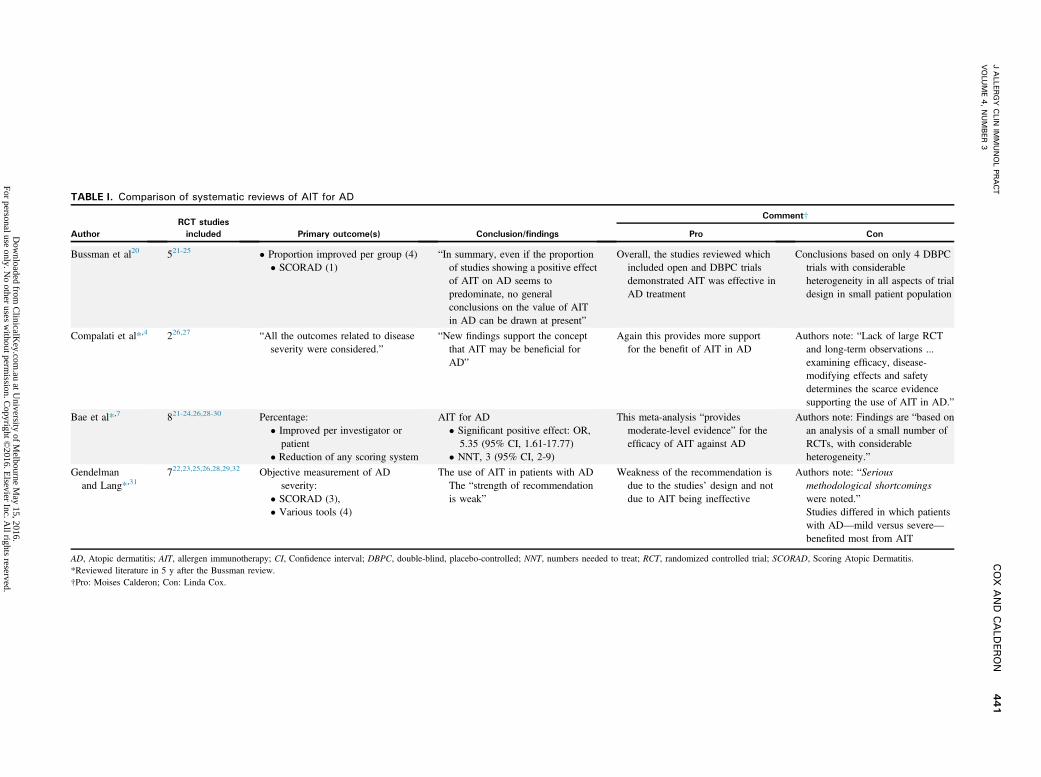
TABLE I. Comparison of systematic reviews of AIT for AD
Author
RCT studies
included Primary outcome(s) Conclusion/findings
Comment†
Pro Con
Bussman et al20 521-25 � Proportion improved per group (4)� SCORAD (1)
“In summary, even if the proportionof studies showing a positive effectof AIT on AD seems topredominate, no generalconclusions on the value of AITin AD can be drawn at present”
Overall, the studies reviewed whichincluded open and DBPC trialsdemonstrated AIT was effective inAD treatment
Conclusions based on only 4 DBPCtrials with considerableheterogeneity in all aspects of trialdesign in small patient population
Compalati et al*,4 226,27 “All the outcomes related to diseaseseverity were considered.”
“New findings support the conceptthat AIT may be beneficial forAD”
Again this provides more supportfor the benefit of AIT in AD
Authors note: “Lack of large RCTand long-term observations ...examining efficacy, disease-modifying effects and safetydetermines the scarce evidencesupporting the use of AIT in AD.”
Bae et al*,7 821-24,26,28-30 Percentage:� Improved per investigator orpatient
� Reduction of any scoring system
AIT for AD� Significant positive effect: OR,
5.35 (95% CI, 1.61-17.77)� NNT, 3 (95% CI, 2-9)
This meta-analysis “providesmoderate-level evidence” for theefficacy of AIT against AD
Authors note: Findings are “based onan analysis of a small number ofRCTs, with considerableheterogeneity.”
Gendelmanand Lang*,31
722,23,25,26,28,29,32 Objective measurement of ADseverity:
� SCORAD (3),� Various tools (4)
The use of AIT in patients with ADThe “strength of recommendationis weak”
Weakness of the recommendation isdue to the studies’ design and notdue to AIT being ineffective
Authors note: “Seriousmethodological shortcomingswere noted.”Studies differed in which patientswith AD—mild versus severe—benefited most from AIT
AD, Atopic dermatitis; AIT, allergen immunotherapy; CI, Confidence interval; DBPC, double-blind, placebo-controlled; NNT, numbers needed to treat; RCT, randomized controlled trial; SCORAD, Scoring Atopic Dermatitis.*Reviewed literature in 5 y after the Bussman review.†Pro: Moises Calderon; Con: Linda Cox.
JALLER
GY
CLIN
IMMUNOLPR
ACT
VOLU
ME4,NUMBER
3COX
AND
CALD
ERON
441
Dow
nloaded from C
linicalKey.com
.au at University of M
elbourne May 15, 2016.
For personal use only. No other uses w
ithout permission. C
opyright ©2016. E
lsevier Inc. All rights reserved.
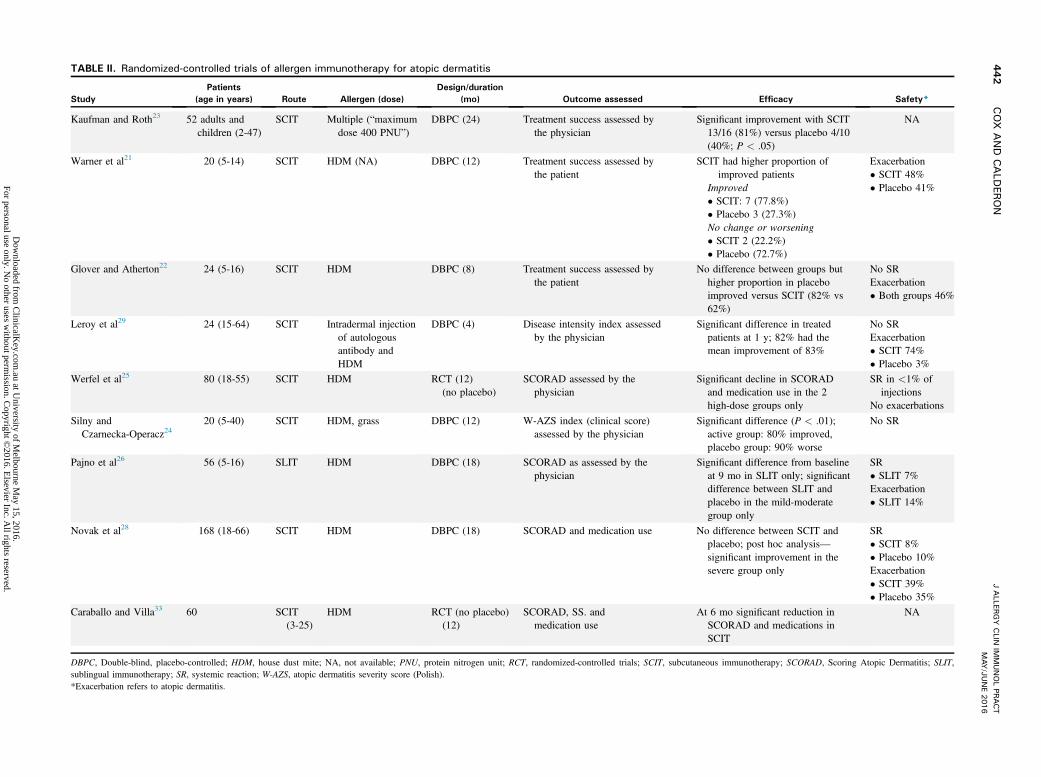
TABLE II. Randomized-controlled trials of allergen immunotherapy for atopic dermatitis
Study
Patients
(age in years) Route Allergen (dose)
Design/duration
(mo) Outcome assessed Efficacy Safety*
Kaufman and Roth23 52 adults andchildren (2-47)
SCIT Multiple (“maximumdose 400 PNU”)
DBPC (24) Treatment success assessed bythe physician
Significant improvement with SCIT13/16 (81%) versus placebo 4/10(40%; P < .05)
NA
Warner et al21 20 (5-14) SCIT HDM (NA) DBPC (12) Treatment success assessed bythe patient
SCIT had higher proportion ofimproved patients
Improved� SCIT: 7 (77.8%)� Placebo 3 (27.3%)No change or worsening� SCIT 2 (22.2%)� Placebo (72.7%)
Exacerbation� SCIT 48%� Placebo 41%
Glover and Atherton22 24 (5-16) SCIT HDM DBPC (8) Treatment success assessed bythe patient
No difference between groups buthigher proportion in placeboimproved versus SCIT (82% vs62%)
No SRExacerbation� Both groups 46%
Leroy et al29 24 (15-64) SCIT Intradermal injectionof autologousantibody andHDM
DBPC (4) Disease intensity index assessedby the physician
Significant difference in treatedpatients at 1 y; 82% had themean improvement of 83%
No SRExacerbation� SCIT 74%� Placebo 3%
Werfel et al25 80 (18-55) SCIT HDM RCT (12)(no placebo)
SCORAD assessed by thephysician
Significant decline in SCORADand medication use in the 2high-dose groups only
SR in <1% ofinjections
No exacerbations
Silny andCzarnecka-Operacz24
20 (5-40) SCIT HDM, grass DBPC (12) W-AZS index (clinical score)assessed by the physician
Significant difference (P < .01);active group: 80% improved,placebo group: 90% worse
No SR
Pajno et al26 56 (5-16) SLIT HDM DBPC (18) SCORAD as assessed by thephysician
Significant difference from baselineat 9 mo in SLIT only; significantdifference between SLIT andplacebo in the mild-moderategroup only
SR� SLIT 7%Exacerbation� SLIT 14%
Novak et al28 168 (18-66) SCIT HDM DBPC (18) SCORAD and medication use No difference between SCIT andplacebo; post hoc analysis—significant improvement in thesevere group only
SR� SCIT 8%� Placebo 10%Exacerbation� SCIT 39%� Placebo 35%
Caraballo and Villa33 60 SCIT(3-25)
HDM RCT (no placebo)(12)
SCORAD, SS. andmedication use
At 6 mo significant reduction inSCORAD and medications inSCIT
NA
DBPC, Double-blind, placebo-controlled; HDM, house dust mite; NA, not available; PNU, protein nitrogen unit; RCT, randomized-controlled trials; SCIT, subcutaneous immunotherapy; SCORAD, Scoring Atopic Dermatitis; SLIT,sublingual immunotherapy; SR, systemic reaction; W-AZS, atopic dermatitis severity score (Polish).*Exacerbation refers to atopic dermatitis.
JALLER
GY
CLIN
IMMUNOLPR
ACT
MAY
/JUNE201
6442
COX
AND
CALD
ERON
Dow
nloaded from C
linicalKey.com
.au at University of M
elbourne May 15, 2016.
For personal use only. No other uses w
ithout permission. C
opyright ©2016. E
lsevier Inc. All rights reserved.

J ALLERGY CLIN IMMUNOL PRACTVOLUME 4, NUMBER 3
COX AND CALDERON 443
SAFETY OF AIT IN AD
Pro: Moises A. CalderonLocal and systemic reactions (SR) were reported in most of the
studies of AIT for AD. The incidence of these reported adverseeffects varied among studies. In the systematic review conductedby Bae et al,7 the AIT and control groups had comparableproportions of systemic (0%-8.0% vs 0%-10.7%, respectively)and local reactions (6.3%-80.0% vs 0%-60.0%, respectively).
For SCIT, systemic adverse reactions are usually mild inseverity, reported as grade 1 or 2. The most common systemicsymptoms were eczema flare-ups, urticaria, rhinitis, pruritus,headache, and asthma.28
For SLIT, the local reactions reported were mild in severity,transient in duration, and did not require medication treatment.Mild lip swelling and mouth or lip itchiness were mostcommonly reported. Transient AD exacerbations were ascommon among patients in AIT groups (14.3%-74%) as thecontrol groups (0%-83.3%).7 At present, there have been nofatal or near-fatal adverse events reported with AIT for AD.
Con: Linda CoxThe adverse effects of AIT include common local application
site reactions and less frequently, SR, which could be lifethreatening. Local reactions are common to SCIT and SLIT, butthe incidence of SR significantly varies between the 2 routesfavoring SLIT as being safer. The risk of severe SCIT SR appearsto be greater in patients with asthma than those with AR. Thereare limited data on the safety of AIT in patients with AD interms of SR. It has been suggested that AIT poses a risk ofexacerbating AD. This is largely anecdotal without confirmationin the published clinical trials. There was a comparable incidenceof AD disease exacerbations and SR in the AIT and controlgroups in the 8 studies considered in the Bae et al7 systematicreview (385 patients; 177 SCIT, 42 SLIT, and 166 placebo).However, the authors noted that the adverse events were notclearly defined and that it would be a “. challenge to combinethe data from all studies.” Considering the relatively low inci-dence of SR, approximately 0.1% of injections per a largemultiyear AIT safety surveillance study,35 and even lower inci-dence of severe SR (1 in 1 million injections),36 data from aconsiderably larger population than the 385 patients in the Baeet al review are needed to make any conclusions regarding thesafety of AIT in patients with AD.
AIT FOR AD OTHER CONSIDERATIONS: COST-
EFFECTIVENESS AND LONG-TERM EFFICACYThere have been no prospective controlled trials evaluating the
long-term efficacy of AIT in AD in terms of persistent clinicalbenefits after discontinuation or prevention of disease progres-sion. One study of 15 patients with AD treated with SCIT forHDM or grass found a significant difference between theDermatology Life Quality Index before and 2 to 12 years afterdiscontinuation of AIT.37
There are no studies comparing the cost-effectiveness of AITfor AD with any other standard AD therapy. However, sys-tematic reviews have found AIT to be cost-effective comparedwith standard drug treatment for AR38,39 and asthma.39 Varyingcost-effective “break-even” points have been reported that rangefrom as early as 3 months after treatment initiation40 to severalyears after discontinuation. One systematic review of AIT for AR
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
concluded that the cost-effective time point was generally 6 yearsafter treatment initiation.38 Whether these systematic reviewsand individual study findings supporting the cost-effectiveness ofAIT for AR can be applied to AD is unknown.
We both agree that further research is needed to determine thecost-effectiveness of AIT as compared with other AD treatmentinterventions.
UNMET NEEDS
Despite our opposing views in Houston, we both agree thatthis treatment is worth further investigation and that thefollowing are unmet needs regarding AIT for AD:
� Need well-designed RCTs that compare efficacy of AIT withstandard treatment in well-defined AD “phenotypes”.
� Need a uniform method for assessing AD efficacy in clinicaltrials and practice.
� To optimize treatment; need to determine if AIT efficacy.B Depends on specific allergens (eg, dust mite) or applies toall.
B Depends on AD severity.B Depends on disease duration.
CONCLUSIONS
At present, few studies have evaluated the efficacy of AIT inAD. The heterogeneity and methodological limitations of thesestudies make comparisons difficult and thus, nearly impossible tobase conclusions about the treatment efficacy. Additionally, inthe studies demonstrating efficacy, there are conflicting data onwhich patient population benefits, for example, severe versusmoderate. Although AD is included as a potential indication forAIT in current practice guidelines, this may be reconsidered inthe future as guideline criteria have become more stringent. Tobe considered in the National Guideline Clearinghouse, arepository for national and international practice guideline, rec-ommendations should be based on systematic review and analysisof the evidence.41 As indicated by the discussion earlier, such areview and evidence analysis would not lend strong support to anAIT for AD treatment recommendation.
In conclusion, more research is needed with randomized trialsof well-defined patient populations with AD using uniform,standardized outcome assessment tools to establish comparativeeffectiveness of AIT in AD.
REFERENCES
1. Schneider L, Tilles S, Lio P, Boguniewicz M, Beck L, LeBovidge J, et al.Atopic dermatitis: a practice parameter update 2012. J Allergy Clin Immunol2013;131:295-299.e1-27.
2. Cox L, Nelson H, Lockey R, Calabria C, Chacko T, Finegold I, et al. Allergenimmunotherapy: a practice parameter third update. J Allergy Clin Immunol2011;127(Suppl):S1-55.
3. Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guidelines: developingguidelines. BMJ 1999;318:593-6.
4. Compalati E, Rogkakou A, Passalacqua G, Canonica GW. Evidences of efficacyof allergen immunotherapy in atopic dermatitis: an updated review. Curr OpinAllergy Clin Immunol 2012;12:427-33.
5. Leung DY, Guttman-Yassky E. Deciphering the complexities of atopicdermatitis: shifting paradigms in treatment approaches. J Allergy Clin Immunol2014;134:769-79.
6. Novak N. New insights into the mechanism and management of allergic dis-eases: atopic dermatitis. Allergy 2009;64:265-75.
7. Bae JM, Choi YY, Park CO, Chung KY, Lee KH. Efficacy of allergen-specificimmunotherapy for atopic dermatitis: a systematic review and meta-analysis ofrandomized controlled trials. J Allergy Clin Immunol 2013;132:110-7.
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.
J ALLERGY CLIN IMMUNOL PRACTMAY/JUNE 2016
444 COX AND CALDERON
8. Schmitt J, Langan S, Williams HC. European Dermato-Epidemiology Network.What are the best outcome measurements for atopic eczema? A systematic re-view. J Allergy Clin Immunol 2007;120:1389-98.
9. Schmitt J, Spuls PI, Thomas KS, Simpson E, Furue M, Deckert S, et al. TheHarmonising Outcome Measures for Eczema (HOME) statement to assessclinical signs of atopic eczema in trials. J Allergy Clin Immunol 2014;134:800-7.
10. EASI Scoring System. Available from: http://www.nottingham.ac.uk/homeforeczema/documents/easi-user-guide-dec-2014-final.pdf. Accessed August23, 2015.
11. Severity scoring of atopic dermatitis: the SCORAD index. Consensus Report ofthe European Task Force on Atopic Dermatitis. Dermatology 1993;186:23-31.
12. Nankervis H, Pynn EV, Boyle RJ, Rushton L, Williams HC, Hewson DM, et al.House dust mite reduction and avoidance measures for treating eczema.Cochrane Database Syst Rev 2015;1:CD008426.
13. Roekevisch E, Spuls PI, Kuester D, Limpens J, Schmitt J. Efficacy and safety ofsystemic treatments for moderate-to-severe atopic dermatitis: a systematicreview. J Allergy Clin Immunol 2014;133:429-38.
14. Portnoy JM. Immunotherapy for asthma: unfavorable studies. Ann AllergyAsthma Immunol 2001;87(Suppl 1):28-32.
15. European Medicines Agency. Guideline on the Clinical Development ofProducts for Specific Immunotherapy for the Treatment of Allergic Diseases.Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003605.pdf. Published November 20,2008. Accessed June 3, 2009
16. Summary Basis for Regulatory Action Template. Available from: http://www.fda.gov/downloads/BiologicsBloodVaccines/Allergenics/UCM393021.pdf.Accessed September 6, 2015.
17. Canonica GW, Baena-Cagnani CE, Bousquet J, Bousquet PJ, Lockey RF,Malling HJ, et al. Recommendations for standardization of clinical trials withAllergen Specific Immunotherapy for respiratory allergy. A statement of aWorld Allergy Organization (WAO) taskforce. Allergy 2007;62:317-24.
18. GRASTEK� (Timothy Grass Pollen Allergen Extract). Available from: http://www.fda.gov/downloads/BiologicsBloodVaccines/Allergenics/UCM393184.pdf.Accessed December 14, 2014.
19. RAGWITEKTM (Short Ragweed Pollen Allergen Extract) Tablet for SublingualUse Prescribing Information. Available from: http://www.merck.com/product/usa/pi_circulars/r/ragwitek/ragwitek_pi.pdf. Accessed December 26, 2014.
20. Bussmann C, Bockenhoff A, Henke H, Werfel T, Novak N. Does allergen-specific immunotherapy represent a therapeutic option for patients with atopicdermatitis? J Allergy Clin Immunol 2006;118:1292-8.
21. Warner JO, Price JF, Soothill JF, Hey EN. Controlled trial of hyposensitisationto Dermatophagoides pteronyssinus in children with asthma. Lancet 1978;2:912-5.
22. Glover MT, Atherton DJ. A double-blind controlled trial of hyposensitization toDermatophagoides pteronyssinus in children with atopic eczema. Clin ExpAllergy 1992;22:440-6.
23. Kaufman HS, Roth HL. Hyposensitization with alum precipitated extracts inatopic dermatitis: a placebo-controlled study. Ann Allergy 1974;32:321-30.
24. Silny W, Czarnecka-Operacz M. Specific immunotherapy in the treatment ofpatients with atopic dermatitis—results of double blind placebo controlledstudy. Pol Merkur Lekarski 2006;21:558-65.
Downloaded from ClinicalKey.com.au at UFor personal use only. No other uses without permission.
25. Werfel T, Breuer K, Rueff F, Przybilla B, Worm M, Grewe M, et al. Usefulnessof specific immunotherapy in patients with atopic dermatitis and allergicsensitization to house dust mites: a multi-centre, randomized, dose-responsestudy. Allergy 2006;61:202-5.
26. Pajno GB, Caminiti L, Vita D, Barberio G, Salzano G, Lombardo F, et al.Sublingual immunotherapy in mite-sensitized children with atopic dermatitis: arandomized, double-blind, placebo-controlled study. J Allergy Clin Immunol2007;120:164-70.
27. Shi HWX, Ren H, Zhuang Y. Effect analysis of the dust mite allergen specificimmunotherapy of chronic eczema. Chin J Derm Venereol 2010;24:424-6.
28. Novak N, Bieber T, Hoffmann M, Folster-Holst R, Homey B, Werfel T, et al.Efficacy and safety of subcutaneous allergen-specific immunotherapy withdepigmented polymerized mite extract in atopic dermatitis. J Allergy ClinImmunol 2012;130:925-931.e924.
29. Leroy BP, Boden G, Lachapelle JM, Jacquemin MG, Saint-Remy JM. A noveltherapy for atopic dermatitis with allergen-antibody complexes: a double-blind,placebo-controlled study. J Am Acad Dermatol 1993;28(Pt 1):232-9.
30. Galli E, Chini L, Nardi S, Benincori N, Panei P, Fraioli G, et al. Use of a specificoral hyposensitization therapy to Dermatophagoides pteronyssinus in childrenwith atopic dermatitis. Allergol Immunopathol 1994;22:18-22.
31. Gendelman SR, Lang DM. Specific immunotherapy in the treatment of atopicdermatitis: a systematic review using the GRADE system. Ann Allergy AsthmaImmunol 2013;111:555-61.
32. Ring J. Successful hyposensitization treatment in atopic eczema: results of a trialin monozygotic twins. Br J Dermatol 1982;107:597-602.
33. Caraballo JMS, Villa RC. Clinical and immunological changes of immuno-therapy in patients with atopic dermatitis: randomized controlled trial. ISRNAllergy 2012;2012:183983.
34. Gendelman SR, Lang DM. Sublingual immunotherapy in the treatment of atopicdermatitis: a systematic review using the GRADE system. Curr Allergy AsthmaRep 2015;15:498.
35. Epstein TG, Liss GM, Murphy-Berendts K, Bernstein DI. AAAAI/ACAAIsurveillance study of subcutaneous immunotherapy, years 2008-2012: an updateon fatal and nonfatal systemic allergic reactions. J Allergy Clin Immunol Pract2014;2:161-167.e163.
36. Amin HS, Liss GM, Bernstein DI. Evaluation of near-fatal reactions to allergenimmunotherapy injections. J Allergy Clin Immunol 2006;117:169-75.
37. Wyrzykowska N, Czarnecka-Operacz M, Adamski Z. Long-term efficacy ofallergen specific immunotherapy in atopic dermatitis patients in relation toquality of life. Eur Ann Allergy Clin Immunol 2015;47:5-9.
38. Meadows A, Kaambwa B, Novielli N, Huissoon A, Fry-Smith A, Meads C,et al. A systematic review and economic evaluation of subcutaneous and sub-lingual allergen immunotherapy in adults and children with seasonal allergicrhinitis. Health Technol Assess 2013;17:1-322. vi, xi-xiv.
39. Hankin CS, Cox L. Allergy immunotherapy: what is the evidence for costsaving? Curr Opin Allergy Clin Immunol 2014;14:363-70.
40. Hankin CS, Cox L, Bronstone A, Wang Z. Allergy immunotherapy: reducedhealth care costs in adults and children with allergic rhinitis. J Allergy ClinImmunol 2013;131:1084-91.
41. National Guideline Clearinghouse Inclusion Criteria. Available from: http://www.guideline.gov/about/inclusion-criteria.aspx. Accessed September 6,2015.
niversity of Melbourne May 15, 2016. Copyright ©2016. Elsevier Inc. All rights reserved.


















