
Differential effects of Nintedanib and Pirfenidone on lung ...
The
PulmonaryPaperDedicated to Respiratory Health CareNovember/December 2014 Vol. 25, No. 6
All I want for Christmas is my liquid oxygen!
Featuring 03 | Editor‘s Note
04 | Calling Dr. Bauer
18 | Ask Mark
10 | Fibrosis File
18 | Sharing the Health
30 | Respiratory News
Your Health16 | In the Rear View &
On the Horizon
12 | COPD News
13 | Back to Basics: Clearing the Airways
17 | Christmas Quiz
21 | Flu Myths
22 | Stem Cell Replacement Therapy
27 | What to Say and What Not to Say
For Fun28 | SeaPuffer Cruises
Plan a vacation and leave your cares behind you!
We salute couples who have been together in good times and bad! Send us your photo!
www.pulmonarypaper.org Volume 25, Number 6
Table of Contents
Chris Scott
Talk to your doctor now about the benefits of Transtracheal Oxygen Therapy!• Improved mobility• Greater exercise capacity• Reduced shortness
of breath• Improved self-image• Longer lasting portable
oxygen sources• Eliminated discomfort
of the nasal cannula• Improved survival
compared to the nasal cannula
Live Longer! Breathe Easier! Improve Quality of Life! Even Look Better!
You’ve suffered long enough. Ask your doctor about TTO2!
For information call: 1-800-527-2667 or e-mail [email protected]
Chris and Scott Peterson of Missouri, who are also on the cover, are childhood sweet-hearts who are still going strong!
We are hiding The Pulmonary Paper logo on our front cover. Can you find it?

November/December 2014 www.pulmonarypaper.org 3
Editor’s Note
Dear Santa,
I have tried to be very good this year! I read a simple little book entitled Live and Learn and Pass It On and identified with many of the observations.
I have learned that every person I have met and talked to had some thing to say that I found interesting or helpful.
Every new place that I visit offers potential for adventure and excitement.I’ve learned that if you stay focused on yourself, you are guaran teed to be miserable.I’ve learned that I did a good job raising my children, seeing the way they live their lives.My whole attitude changes when I get a call or read a note that someone says they appre
ciate me or simply says thank you.I’ve learned that I cannot expect others to solve my problems. When bad times come, you
can let them make you bitter or use them to make you better.I’ve learned that I can keep going long after I thought I couldn’t.Thank you for my friend who is always there for me and
makes me go to the gym when I don’t want to.Santa, I hope to live a very long time without
growing old.Can you please help young people see that cigar
ettes do not make them grown up?Could the people in charge realize it is worth the
extra money to let us use a 3pound oxygen unit rather than a 17pound one?
Can we get more research dollars for COPD, the third leading cause of death?
Rather than have people resist change, can you help them see it is the only thing that brings progress.
Please keep surrounding me with people who are smarter than me.
And Santa, please help us see that regrets over yesterday and the fear of tomorrow will rob us
of happiness we can have today.
Happy Holidays to all! I appreciate your support more than you will ever know!
Happy Holidays from the Belyeas!
add santa hat to celetste pic

4 www.pulmonarypaper.org Volume 25, Number 6
Question for Dr. Bauer? You may write to him at The Pulmonary Paper, PO Box 877, Ormond Beach, FL 32175 or by email at [email protected].
Dr. Michael Bauer
Calling Dr. Bauer …
A s 2014 draws to a close, I thought this would be a good opportunity to give our readers a brief update on what’s new in the world of pulmonary medicine. Here we go:
• Lung Cancer: We are discovering new proteins called driver mutations on the surface of lung cancer cells that can predict a good response to a variety of new cancer drugs. These targeted agents may prolong life and improve symptoms in patients with advanced lung cancer.
• COPD: Every few months I’m seeing new inhalers on the market. Most of them are combination inhalers with a variety of long acting bronchodilators and steroids. Some are just once a day use. Bronchoscopic lung volume reduction is a technique being actively investigated. Introducing a variety of small plugs, mechanical valves and/or coils into the airways by bronchoscopy is a nonsurgical approach that may improve lung function in advanced COPD. The verdict is not in at this time.
• Interstitial lung disease: Two new drugs – Nintedanib and Pirfenidone – have just been approved by the Food and Drug Administration (FDA) and will soon be available. These have been shown to modestly slow the decline in lung function and slow disease progression in IPF but will be very expensive.
• Sleep apnea: A big trend led by insurance carriers is to perform more inhome sleep studies rather than in hospital or clinic for complete polysomnograms. Also a big push for AutoPAP self adjusting machines. Compliance and efficacy are being assessed by “smart card” computer chips or online modem reporting.
• Smoking cessation: Electronic cigarettes (ecigarettes) are a big unknown. They may be helpful as an aid for smoking cessation, but major concerns exist about use of flavored cigarettes in young adults and teens as a gateway drug towards regular cigarette use. Lots of ongoing research.
Best wishes to all our Pulmonary Paper readers for a great 2015. I enjoy my discussions with you. Keep in touch!
Ed’s Note: As a treat for the holidays, enjoy a special clip from Dr. Bauer’s
piano recital! Go to: http://www.youtube.com/watch?v=wkh3onuhkhk
November/December 2014 www.pulmonarypaper.org 5
Do You Use Oxygen or Know Someone Who Does?Oxy-View Oxygen Therapy Eyeglass Frames are a great Christmas gift for you or a loved one!
Call today! Speak to one of our customer service representatives to purchase a frame for only $210 (plus s/h).
Offer good through January 31, 2015
Toll Free 1-877-699-8439 or visit our website, www.oxyview.com

6 www.pulmonarypaper.org Volume 25, Number 6
In the Rear View and On the Horizon
As December 31 approaches, we often
reflect on the year that was and
look ahead to the year that will be.
2014 saw some popular home oxygen sys-
tems receive some notable upgrades as well
as the release of new home oxygen products.
Inogen upgraded their G2 portable oxygen
concentrator (POC) to include pulse settings
ranging from 1 to 6 and introduced a 5-liter
home stationary con-
centrator that weighs
under 20 pounds.
Perhaps one of the
more anticipated
new oxygen systems
was CAIRE SeQual’s
eQuinox POC. Tout-
ed as being the light-
est continuous flow (CF)-capable POC to hit
the market, the eQuinox was released over
the summer as an engineering overhaul of
the popular Eclipse systems. The eQuinox
retained all of the clinical features of the
Eclipse systems, but was about two-thirds
the size and weight of the Eclipse model.
So what might 2015 have in store for
home oxygen users?
Inova Labs will be introducing the
Activox DUO2, which will integrate their
existing LifeChoice Activox pulse flow POC
with a new 5-liter home stationary concen-
trator. Based on current specifications avail-
able on the Inova Labs website, the station-
ary concentrator will likely be very similar
to most existing stationary concentrators
but with one big difference – the Activox
POC will be able to be docked in the DUO2
stationary concentrator, allowing the POC
battery to be charged when the POC is not
in use. Oxygen users who have this system in
their home will be able to easily detach the
POC from the stationary unit for their away-
from-home ambulatory needs. The DUO2
can be likened to home-fill oxygen systems,
where the stationary concentrator gas is used
to fill up small cylinders for portable use, but
instead of cylinders the portable option is a
POC. As of now, it appears the LifeChoice
Activox POC capabilities will not be up-
dated, so be aware that the Activox only
offers pulse settings
of 1, 2 and 3 – there
is no CF option on
the POC – so users
should strongly con-
sider renting or try-
ing out an Activox
POC to ensure the
device is adequately
able to oxygenate
them during their
activities. More in-
formation on the
DUO2 can be found
at www.inovalabs.
com/duo2
MedTrade 2014, one of the larger home care
trade shows in the United States, gave home
care dealers the first glimpse of the updated
OxLife Independence CF POC. The cur-
rent OxLife Independence is similar to
the SeQual Eclipse in oxygen production
capacity, up to 3 LPM CF and common
pulse settings of 1 to 6. The updated OxLife
Independence will be able to produce up to
November/December 2014 www.pulmonarypaper.org 7
4 LPM CF, making it the first commercially
available POC to have continuous flow
settings ranging from 0.5 to 4.0 LPM. With
the additional oxygen production capability,
the updated OxLife Independence will also
feature significantly more pulse settings,
ranging from 1 to 15 with dose volumes
ranging from 16mL per breath at the 1 set-
ting to 240 mL per breath at the 15 setting.
Do note that at the higher pulse settings
there may be a breath rate limit; since the
unit will be able to produce 4,000 mL per
minute, the maximum breath rate for the
15 setting will be slightly under 17 breaths
per minute, which is not typical of an active
breath rate. Other promoted features of
the updated OxLife Independence include
improved battery life and quieter operation
at lower device settings.
More information on the upgrades to the
OxLife Independence can be found at www.
o2-concepts.com/dna-technology
On another note as we close 2014, I’d like
to extend my thanks to editor Celeste Belyea
for giving me the opportunity to regularly
write for the Pulmonary Paper, and to you
the readers for your positive feedback and
comments over the last several years. One
thing is missing, though – after writing nu-
merous articles, this column has never had
a title. I’d like to extend an offer to you, the
readers, to give this column a name. Please
feel free to submit to the Pulmonary Paper
or to myself your suggestions, as well as any
questions and/or ideas for future articles.
Happy holidays to you all, and my best
wishes to you for a wonderful 2015.
Ryan Diesem is Research Manager at Valley Inspired Products, Apple Valley, MN. Contact Ryan at [email protected] with questions or com-ments.
What’s in a
Name?
Give Ryan’s Oxygen Column a Titleand win a free membership to The Pulmonary Paper!
Join Ryan on the March 20, 2015 ten-
day cruise to the Southern Caribbean
on Holland America’s Westerdam,
roundtrip from Fort Lauderdale. Call
1-866-673-3019 to book today!

8 www.pulmonarypaper.org Volume 25, Number 6
Mark Mangus, RRTEFFORTS Board
Mark Mangus RRT, BSRC, is a member of the Medical Board of EFFORTS (the online support group, Emphysema Foundation For Our Right To Survive, www.emphysema. net). He generously donates his time to answer members’ questions.
Ask Mark …
Robert from New Mexico was told to gargle with water, every time he uses an inhaler or nebulizer and asks if this is necessary. Mark says, While it won’t hurt to rinse your mouth after using your Spiriva, Albuterol, Formoterol or Salmeterol, it is not necessary to do so. It is the inhaled steroid medications where it is so important to rinse and spit after dosing yourself. The inhaled steroids thwart the natural immunity in your mouth and throat to candida albicans (the yeast organism that causes Thrush). See definition to left.
Virginia W. was wondering if portable liquid oxygen (LOX) devices deliver pulse or continuous flow. She now uses an Eclipse portable oxygen concentrator and would like to try an alternative.
Mark says, The Helios liquid portable is pulse only up to a setting of 4. The larger Marathon does have a continuous flow option up to 6LPM.
There are two Companion series LOX portables that are continuous only. The Companion goes to 6L/min continuous and the Companion T goes to 6, 8, 10, 12 and 15 L/min. Keep in mind that any LOX portable running at 6L/min continuous will not last very long!
The bottom line is that Medicare pays for a stationary (home) source of oxygen and a portable amount for those who qualify. They don’t care if the home care company provides you with LOX and a
concentrator and LOX portable and a POC and tanks or gives you three or ten of each. They pay one amount, no matter what equipment is used or how many.
Beyond that, Medicare says that whatever equipment the company places with you must meet the conditions of the doctor’s
Thrush is an infection characterized by the presence of white, slightly raised lesions in your mouth – on your tongue, inner cheeks, roof of your mouth, gums, tonsils or back of your throat. The lesions may be painful.

November/December 2014 www.pulmonarypaper.org 9
Loren doesn’t have a diagnosis yet but recent Pulmonary Function Testing (PFTs) show everything was within normal limits except the Diffusion Capacity which was 69% down from high 80s a year ago. What does this mean?Mark says, Lung Diffusion Capacity testing, or DLCO, measures how well oxygen can move through the lung and into the bloodstream. If your PFTs are otherwise normal, then I would expect that the variation in DLCO is due to what we often see which is momentary variation in that measurement. It is not unreasonable to expect that your next measurement of DLCO could well be back above 80% again.
prescription. If your doctor orders 5 liters, they can’t give you a system that delivers any less than 5 liters. If your doctor orders that you should adjust your oxygen between 3 and 10 L/min during activity to maintain a minimum saturation of 90%, then your company must give you an oxygen system that will deliver 10 L/min. It can be LOX. It can be tanks. Medicare doesn’t care.
Your company’s payment for home oxygen service has dropped to cost, and sometimes below cost, for just the basics. Since liquid oxygen involves visits to your home for refills, this system will be more expensive for the home care dealer. Unless our voice is heard to rethink the cuts Congress and Medicare made as too severe and limiting, it won’t get any better. It’s going to take changes in the law to make things better.
Bonnie from Illinois writes, my young friend is pregnant and has serious asthma. She is no longer able to use her normal meds –Albuterol, both rescue and nebulizer, and Advair. Her obstetrician has suggested she stop her meds, which she has, but this poor girl is really suffering!Mark advises, Your friend should consult with her asthma specialist – who I would think would insist she return to her Advair use. Pregnant mothers should not stop taking Advair during pregnancy as long as the risks outweigh the benefits. If her gynecologist doesn’t know that her symptoms have amplified since she followed his recommendation to stop the Advair, then he/she should also be made aware. If your friend has an asthma attack, the consequences could be fatal. There is not enough evidence to suggest that continuing
to use Advair is harmful to the fetus, especially if the mother’s asthma symptoms worsen while not using the maintenance drug.
She should be using a peak flow meter to check her airflow every day. It is the only definitive way she can safely manage her breathing and know the urgency of taking her inhaled medications.
A peak flow meter measures your peak expiratory flow rate. It may detect worsening lung function even before your symptoms (like coughing or wheezing) appear. When you take your readings daily and see your normal readings decrease, you will then know to take action. A person with wellcontrolled asthma will consistently have peak flows that vary less than 15%.

Fibrosis File
Merry Christmas! Thanks to input from people dealing with the disease, the Food and Drug Administration (FDA) has approved two new
drugs, Nintedanib (tradename Ofev® from Boehringer Ingelheim-BI) and Pirfenidone (tradename Esbriet® from InterMune), to help Idiopathic Pulmonary Fibrosis (IPF). It is the first time the FDA has approved any treatment for IPF.
ple who took Nintedanib had diarrhea.
That might sway the physician to go with
Pirfenidone instead of Nintedanib.
You probably won’t notice a big differ-
ence in your condition when you start these
drugs. What they have been proven to do is
to reduce the rate of deterioration in your
lung which is difficult to predict and differs
in each person.
Hopefully one day we can look back and
see people survived longer and performed
better after taking these medicines.
This is a long overdue good start in treat-
ment options for IPF!
10 www.pulmonarypaper.org Volume 25, Number 6
The pharmaceutical companies have been
doing clinical trials in IPF for about 15
years. Most of these trials have been neg-
ative and no potential medication has ever
been approved by the FDA. Earlier this year,
successful studies on the two drugs were
published in the New England Journal
of Medicine which helped convince the
FDA to approve these medications. The
drugs hope to lower the rate of lung function
decline, as well as decrease acute exacerba-
tions (flare-ups).
The drugs are used separately. It is un-
known how the two drugs might interact
with one another. Both have possible GI
side effects as nausea and vomiting. Studies
combining the drugs are sure to be in the
future as a possible treatment for those
with IPF.
We don’t know whether one is better
than the other. The recommended dose for
Pirfenidone is three capsules three times a
day, whereas Nintedanib, it is one capsule
twice a day. Almost two thirds of peo-
The Pulmonary Fibrosis Foundation has
a Patients Support Community where mem-
bers have been discussing gifts for the person
who has IPF. You might want to leave this
list someplace where the right people can
see it!
• I would relish “homemade” coupons to
run an errand, pack and take a package
to the post office or even help decorate
or put away decorations, yard clean-
up or gardening. Maybe even doing
laundry, changing sheets on the bed, or
putting away clean clothes. I find the
gift of someone’s time is invaluable and
precious.
• A gift card to the grocery or pharmacy
would be most welcome. For my friends
with pets, I buy three or six months
worth of their pet’s routine meds (like
Trifexis), or put a credit on their account
with their vet.
• Most people with PF agree that we feel
colder than most. Soft, warm socks,
lounge pants or a cuddly warm throw is
a good non-food gift. Gloves or mittens
that can convert to fingerless would be
nice. A selection of teas and hot choco-
late packets are handy and useful.
• Something homemade is always good.
• Gift cards to restaurants, especially
restaurants that deliver.
• The best gift given to me in this past
year has been my iPad.
• A prepaid gift of housecleaning. My
helper uses only vinegar to clean as most
household chemicals really bother me.
• I watch a lot of movies, documentaries
and read iBooks. You can’t go wrong
with prepaid gift cards for iTunes.
• I would adore it if someone sent a mas-
sage therapist to my home. I don’t go out
for massages because I’m so exhausted
getting there and getting back that it
spoils the whole experience.
November/December 2014 www.pulmonarypaper.org 11
Unfortunately, the medication is very
expensive – without insurance it would cost
$92,000 per year! We have heard of people
getting Pirfenidone (Esbriet) for $25/month
after approval. If you and your doctor have
decided this is the drug that is right for you,
you may be eligible for the Esbriet Start
Now program to get your first 45 days of
therapy at no cost. Visit www.esbriet.com/
careconnect/patients on the Internet or
call 1-844-372-7438 for more information.
Our Canadian friends have been paying
approximately $150 for a month’s supply
of 90 pills. Esbriet has been available in
Canada since 2012.
Boehringer Ingelheim-BI has a support
program called OpenDoor that you can
find out more about financial help for
Ofev at 1-866-673-6366 or www.ofev.com/
patient-support.php
12 www.pulmonarypaper.org Volume 25, Number 6
John Walsh, President of the COPD Foun-
dation, is asking all people with COPD to
become involved with the Patient-Centered
Outcomes Research Institute – PCORI.
The nonprofit agency is funded by imposed
fees on health insurance policies. PCORI’s
purpose is to assist people involved in health
care – the patients, medical personnel, pur-
chasers and policy makers – to make better
decisions. The information learned from en-
rolled people will help to prevent, diagnose,
treat, monitor and manage disease. Anyone
over the age of 18 with a confirmed diagno-
sis of COPD is eligible to enroll.
The COPD Patient-Powered Research
Network will be part of other registry
networks and together will be called the
National Patient Centered Clinical Research
Network. To join, call the COPD Founda-
tion at 1-866-316-2673 or go to www.copd
foundation.org and click on the ‘Research’
tab. The registry form will ask about your
symptoms, breathlessness, smoking history
and other medical problems. They are hop-
ing to enroll 75,000 individuals.
The COPD Foundation has also launched
an interactive social network on their web
site so you could interact with others. Visit
the main web page at www.copdfoundation.
org and click on the ‘360social’ tab to learn
more!
Your Voices Count!The FDA published a Federal Register
notice announcing the establishment of a
public docket for comments on FDA activ-
ities performed under the Food and Drug
Administration Safety and Innovation Act
(FDASIA), Patient Participation in Medical
Product Discussions. They would like to
have a more systematic approach to includ-
ing a patient consultant voice earlier in the
product development process.
There are various ways that a patient or
caregiver may participate. One program
that FDA has managed for many years is the
patient representative program, where
patients or their caregivers participate as
members of FDA’s therapeutic advisory
committees to review important questions
about safety and efficacy of products un-
der consideration for marketing approval
with other members of various FDA expert
advisory committees.
For more information email Andrea
Furia-Helms at [email protected]
or write to her at:
Andrea Furia-Helms
Food and Drug Administration
10903 New Hampshire Ave.
Building 32, Room 5319
Silver Spring, MD 20993-0002
COPD News
November/December 2014 www.pulmonarypaper.org 13
The body’s respiratory system has sev-
eral ways to keep itself clean. When
you think about it, the lungs are the only
internal organ to have contact with the
outside world!
Your nose is the first defense. As you
breathe in, large particles are stopped in the
hairs while mucus traps smaller particles.
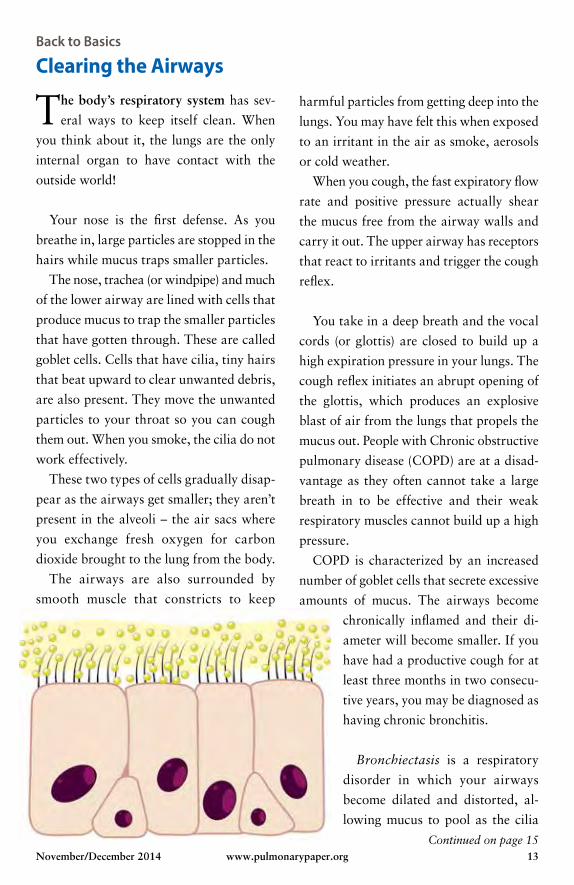
The nose, trachea (or windpipe) and much
of the lower airway are lined with cells that
produce mucus to trap the smaller particles
that have gotten through. These are called
goblet cells. Cells that have cilia, tiny hairs
that beat upward to clear unwanted debris,
are also present. They move the unwanted
particles to your throat so you can cough
them out. When you smoke, the cilia do not
work effectively.
These two types of cells gradually disap-
pear as the airways get smaller; they aren’t
present in the alveoli – the air sacs where
you exchange fresh oxygen for carbon
dioxide brought to the lung from the body.
The airways are also surrounded by
smooth muscle that constricts to keep
harmful particles from getting deep into the
lungs. You may have felt this when exposed
to an irritant in the air as smoke, aerosols
or cold weather.
When you cough, the fast expiratory flow
rate and positive pressure actually shear
the mucus free from the airway walls and
carry it out. The upper airway has receptors
that react to irritants and trigger the cough
reflex.
You take in a deep breath and the vocal
cords (or glottis) are closed to build up a
high expiration pressure in your lungs. The
cough reflex initiates an abrupt opening of
the glottis, which produces an explosive
blast of air from the lungs that propels the
mucus out. People with Chronic obstructive
pulmonary disease (COPD) are at a disad-
vantage as they often cannot take a large
breath in to be effective and their weak
respiratory muscles cannot build up a high
pressure.
COPD is characterized by an increased
number of goblet cells that secrete excessive
amounts of mucus. The airways become
chronically inflamed and their di-
ameter will become smaller. If you
have had a productive cough for at
least three months in two consecu-
tive years, you may be diagnosed as
having chronic bronchitis.
Bronchiectasis is a respiratory
disorder in which your airways
become dilated and distorted, al-
lowing mucus to pool as the cilia
Back to Basics
Clearing the Airways
Continued on page 15
14 www.pulmonarypaper.org Volume 25, Number 6
The Aerobika® OPEP* is designed to aid in the loosening and removal of secretions in your lungs
The device is lightweight, simple to use and can be carried anywhere
It may also be used in combination with your nebulizer treatments
The Aerobika® OPEP* is easy to clean and dishwasher safe
Now available through The Pulmonary PaperCall Today, 1-800-950-3698 or visit www.pulmonarypaper.org
monaghan means it matters™
www.monaghanmed.com
• It was easier to raise my secretions• I don’t cough as often• I don’t feel so short of breath• It has improved my ability to do different activities• It has made my life better
After using the
® device people say 1
™ and ® are trademarks and registered trademarks of Monaghan Medical CORPORATION or an affiliate of Monaghan Medical Corporation © 2014 Monaghan Medical Corporation. 1 Data on file. * OPEP=Oscillating Positive Expiratory Pressure.
For drug-free, natural airway clearance.
Oscillating Positive Expiratory Pressure Therapy System
®

November/December 2014 www.pulmonarypaper.org 15
cannot clear it. This can make you vulner-
able to infections.
Cystic fibrosis (CF) is a genetic disorder
characterized by overproduction of thick
mucus affecting the respiratory, digestive
and reproductive systems. People who have
CF must undergo a daily regimen to remove
secretions and maintain lung function;
otherwise, they’re prone to developing po-
tentially fatal respiratory infections.
Pneumonia causes pooling of secretions
in the air sacs and lower airways, leading to
decreased oxygen levels and lung collapse.
Bacterial or viral pneumonia develops when
a person breathes in foreign matter that
breeds infection.
Neuromuscular diseases may also place
people at higher risk for developing in-
creased pulmonary secretions. Examples in-
clude myasthenia gravis, which results from
a breakdown in communication between
the nerves and muscles, and Guillain-Barré
syndrome, an acute disease that produces
fever and an immune attack on the nerves.
The muscle and nerve problems can reduce
effectiveness of your cough, causing you to
retain more secretions.
Contributing factors to excessive secre-
tions include smoking, air pollution and
occupational exposure to irritants. Having
anesthesia or sedation may depress the
body’s cough reflex.
We are excited to be able to work
with Monaghan Medical Corporation
to provide the Aerobika® to people who
struggle with secretions.
When you breathe into the device,
you will encounter some resistance.
This resistance will create positive pres-
sure inside your lungs which will hold
your airways open. Think of when you
blow up a balloon, it is the positive
pressure that holds the balloon open.
Inside your lungs this positive pressure
opens up the small airways that may be
blocked by mucus.
The Aerobika® has a valve that
switches quickly between higher and
lower resistance. This vibration – or
oscillation – inside the lungs loosens
and seems to decrease the thickness
of the mucus. So between the positive
pressure opening the small airways and
the oscillations loosening the mucus,
it will be easier for you to raise the
secretions. Getting out excess mucus
improves breathing and reduces the
chance of infection.
The Aerobika® is offered to our mem-
bers at the reduced cost of $79.95
plus $5.95 for shipping. If you would
like to order, please call 1-800-950-
3698. Website ordering will be available
soon.
Continued from page 13

The Ultimate Package:Inogen One G3 & Phillips Respironics SimplyFlo
Portable and Continuous Flow: The Best of Both!
Phillips Respironics SimplyGo Package Continuous Flow On Demand 1 to 6
SALE PRICE INCLUDES:• Portable Oxygen Concentrator
• SimplyGo carrying case
• Matching SimplyGo accessory case
• SimplyGo mobile wheeled cart
• A/C wall outlet power
• D/C car power supply
16 www.pulmonarypaper.org Volume 25, Number 6
Order Online: Store.MainClinicSupply.com
Order by Phone: 1-800-775-0942
Inogen One G3 Package Flow 1 to 4
SALE PRICE INCLUDES:• G3 Portable oxygen device
• 8-Cell battery & 16-Cell battery
• Carrying bag w/shoulder strap
• Accessory case
$2495
CUSTOMER SERVICE 24 HOURS A DAY, 7 DAYS A WEEK
$3989
Travel with portability and con-stant flow!
Own the best!
• A/C wall outlet power supply
• D/C car power supply
• Airline power supply
• Power surge & interference protection: $5,000 ultimate lifetime insurance
• 5-Year warranty
• Lifetime technical support: 24 hours a day, 7 days a week customer service
• Free overnight FedEx
CALL• Power surge &
interference protection: $5,000 ultimate lifetime insurance
• 5-Year warranty
• Lifetime technical support: 24 hours a day, 7 days a week customer service
• Free overnight FedEx
SALE PRICE INCLUDES:• Inogen One G3
• Phillips Respironics SimplyFlo
• SimplyFlo travel case
• Factory warranty
• Lifetime technical support: 24 hours a day, 7 days a week customer service
• Free overnight FedEx
CALL TODAY! 1-800-775-0942
November/December 2014 www.pulmonarypaper.org 17
1) What were the names of the Three
Wise Men?
2) What is the best-selling Christmas
recording of all-time?
3) How many sides does a snowflake
have?
4) ‘Good King Wenceslas looked out on
the Feast of Stephen’. When is the
‘Feast of Stephen’?
5) If you received all of the gifts listed
in “The Twelve Days of Christmas”
song, how many presents would you
have?
6) What is a Christmas Cracker?
7) From what material were the first
artificial trees made?
8) What county lays claim to Christmas
Island?
9) What state was last to declare Christ-
mas a holiday in 1907?
10) Traditionally, where does the ‘Xmas’
come from?
Answers will appear in our next issue!
Do you know where the origins of these Christmas references began in our Christmas pop culture? Test yourself with these questions!
For our customers:When you purchase a Portable Oxygen Concentrator, from Main Clinic Supply, you will be entered in a drawing to win a cabin for two on the Sea Puffer’s Southern Caribbean Cruise roundtrip from Fort Lauderdale on Holland America’s Noordam.
Cruise dates are March 20–30, 2015. Cruise Drawing is February 14, 2015.
Special Discount Pricing for Pulmonary Paper Readers!
1-800-775-0942www.mainclinicsupply.com

18 www.pulmonarypaper.org Volume 25, Number 6
This holiday season, remember to plan
and pace! Plan your activities in advance
so you have the time to pack your clothes,
or get all the gift wrapping supplies or rec-
ipe ingredients without being rushed. Pace
yourself to go as fast as you feel comfortable
going!
Be careful of strong smells during the
holidays. Air fresheners with balsam scents
can be so strong it can send sensitive airways
into spasm. The same holds true for candles.
When getting your decorations out from
their storage space, be careful of the dust
that may have gathered on them.
Be careful not to eat too much, even
though this is much easier said than done!
Sharing the Health!
When your stomach is distended and
pushes up on your diaphragm, it will
make it harder to breathe.
If you are lucky enough to celebrate
with family and friends, try to simply
enjoy it. If there have been strained rela-
tions in the past, try and forget it while
together.
Get in the spirit! Dress your inhaler,
nebulizer or oxygen units up for Christ-
mas!
Volunteer in any capacity to help
someone as a gift to yourself.
Enjoy reminiscing about the good
memories you have and think about the
ones to come!
I keep one and two pound weights next
to the chair where I watch TV and try and
do arm exercises while sitting.
It motivates me to also be involved with
others in a yoga class – they have low cost
sessions at my local senior center.
Susan A.
Palm Coast, FL

November/December 2014 www.pulmonarypaper.org 19
Want a simple often forgotten exercise?
Take a walk! With a friend, neighbor, family
member, your dog – around the block or
any part of it, around the mall or around
your house – with or without headphones
for music!
Just make sure you have comfortable
shoes on. Vary your pace – step it up a bit
and slow back down. I like to use a pedom-
eter so I can track how many steps I have
gone. I am lucky enough to live in Florida
so we can walk outside most of the year.
I have written my steps in a journal every
day for over a year.
Mary, Largo, FL
Ann O. of Maryland saw an advertise-
ment for a Salt Room that said it would
be beneficial for people with lung disease.
An article in the Wall Street Journal several
years ago reports owners of indoor salt
rooms say small salt particles can soothe
respiratory and skin conditions. Scientific
evidence is scant and some doctors urge
caution for asthmatics. Salt is an irritant that
could cause airways to constrict.
The experience of breathing in salt air is
designed to mimic salt caves, which have
been considered therapeutic in Eastern Eu-
rope. Sometimes called halotherapy cham-
bers, the walls and ceilings are salt-coated,
and grains are often scattered a few inches
deep on the floor. Some facilities just pile
up salt in the room, while others use special
“salt generators,” machines that grind the
salt into very tiny breathable particles and
blow it into the air. Salt is thought to help
respiratory conditions by drawing water into
airways, thinning mucus and improving the
function of cilia, the small hairs that help
move mucus out of the lungs.
The cost averages about $50 for a one
hour session. The spa experience can be re-
laxing in itself. If there is a salt room in your
area, get your physician’s opinion about it!
20 www.pulmonarypaper.org Volume 25, Number 6
Sharing the Health! continued
Rhyming answers to the Halloween
quiz from our last issue:
• What do you call an Abominable
Snowman named Elizabeth? Betty
Yeti
• What do you call a cart used by a
monster who breathes fire? Dragon
Wagon
• What do you call a fake monster
wrapped in linen? Mummy Dummy
• What do you call a sugary candy?
Sweet Treat
• What do you call a serious monster
made of clay? Solemn Golem
• What did the grave keeper use to
sweep the graveyard? Tomb Broom
• What is a fast prank? Quick Trick
• What is a scare in the evening?
Night Fright
• What is a great incantation? Swell
Spell
• What is a thin furry animal that flies?
Flat Bat
The United States Department of Ag-
riculture has launched What’s Cooking?
USDA Mixing Bowl. It is a resource for
healthy recipes for one person or a large
crowd. You will find many cookbooks
including one with lunch-time ideas and one
from the White House. You will be able to
create healthy recipes on a budget and save
them in your own personal cookbook. Get
started with Holiday Recipes at http://www.
whatscooking.fns.usda.gov/
Smoking PreventionIn the tobacco settlement of 1998, $206
billion was pledged to each state to fund
anti-smoking campaigns. This year only
1.9% of the money was spent on preven-
tion. The rest was spent on everything from
fixing potholes to building jails. Nine states
have even issued bonds backed by future
payments. Where did we read these sad
facts? From Mr. Butts, a character in Garry
Trudeau’s comic strip Doonesbury! Pay-
ment will continue through the year 2025.
The state of New Jersey has been awarded
$7,576,167,918.47 so far – not one penny
has been spent on smoking education.
Cindy G. from NY has a tip for those who
have tried DaliResp – a medication used to
prevent flare-ups of COPD. “I was getting
nauseated when using it when my doctor
suggested I take half the pill on Monday,
Wednesday and Friday for a week. The next
week I was to take a full pill on those days.
When I tolerated this much better, we went
to the normal dose of one pill every day.
Here’s hoping I have a hospital-free winter!”
November/December 2014 www.pulmonarypaper.org 21
COPD Advocate!Since January
2006, Grace Anne
Dorney Koppel
has served as a
national spokes-
woman and patient
advo cate for the
National Heart,
Lung, and Blood
Institute (NHLBI)
to increase awareness of COPD. Dorney
Koppel is a practicing attorney and business
manager for her husband, former Nightline
anchor, Ted Koppel.
She is president of the Dorney-Koppel
Family Charitable Foundation, one of whose
missions is to provide start-up funding for
pulmonary rehabilitation centers.
She advises others that doctors can give us
the tools to treat our disease, but if we don’t
use them properly, the best tools can’t help.
Doctors can prescribe inhalers to open our
airways, but if we don’t use those inhalers
on time and follow the directions on exact-
ly how to use them, they’re going to be of
limited help. Doctors can recommend an nu al
flu shots and getting the pneumonia vaccine,
but we’re the ones who have to do it.
Perhaps the best advice I received from a
doctor was to exercise. Understand, though,
we’re not training for the Olympics. We’re
trying to get as much as we possibly can out
of a damaged set of lungs
When I was diagnosed with COPD, I was
in a wheelchair. My lung capacity was at 26
percent of predicted capacity. I was told I’d
probably be dead by 2006. I’m still here. My
predicted lung capacity is at 50 percent. I
walk a couple miles at least five days a week.
Grace Anne Dorney Koppel
Myths Surrounding the FluTara Haelle is the author of an Internet
blog at www.RedWineandAppleSauce.com
for parents. She recently wrote about the
myths and misinformation about the flu vac-
cine that people still continue to believe. She
backs each one up with medical evidence.
We hope you will encourage others to get
their flu vaccination to help stop its spread!
1: The flu vaccine gives you the flu or
makes you sick. (No, it doesn’t.)
2: Pregnant women should not get the
flu shot. (They should.) The flu shot
can cause miscarriages. (It doesn’t.)
Pregnant should only get the preserva-
tive-free flu shot. (Nope.)
3: Flu vaccines don’t work. (Um, they do
work.)
4: Flu vaccines make it easier for people
to catch pneumonia or other infectious
diseases. (No, they make it harder.)
5: Flu vaccines cause vascular or cardio-
vascular disorders. (No, they don’t.)
6: The flu vaccine weakens your body’s
immune response. (It actually strength-
ens it.)
7: The flu vaccine causes nerve disorders
such as Guillain-Barré syndrome. (Ex-
tremely rarely – and more commonly
with flu infections.)
8: People don’t die from the flu unless
they have another underlying condition
already. (Actually, healthy people do die
from the flu.)
9: The flu shot doesn’t work for me,
personally, because last time I got it,
I got the flu anyway. (It still reduces
your risk.)
10: I never get the flu, so I don’t need the
shot. (You can see the future?)

22 www.pulmonarypaper.org Volume 25, Number 6
Stem cell replacement (SCR) therapy
for a wide variety of medical diseases
has been a topic of discussion for
many years now. The term “stem cell” first
appeared in the scientific literature as far
back as 1868. A German biologist named
Ernst Haeckel used the term to describe the
single-celled organism that acted as an ances-
tor cell to all living things in history. Jump
forward to August 9, 2001 when President
George W. Bush signed an order authorizing
the use of federal funds for research on a
limited number of existing human embryon-
ic stem cell lines.
In January of 2009 the Geron Corpora-
tion announced the FDA’s announcement
of approval for a limited phase 1 trial for a
new treatment of spinal cord injuries based
entirely on human embryonic stem cells.
Later that year, President Barack Obama
signed Executive Order 13505 which loos-
ened restrictions on human embryonic stem
cell research. In July of 2009 the NIH issued
revised guidelines for federal funding for
stem cell research. Currently the National
Institutes of Health approves of at least 13
new human embryonic stem cell lines for
federal funding.
Replacement TherapyWill the Real Stem Cell Please Stand Up?
After a hundred and fifty years and many
millions of research dollars spent … what
do we know about stem cell replacement
therapy, specifically its possible role in lung
disease? Just exactly what is a stem cell?
Stem cells are found throughout the body
and have several main characteristics:
1. They can renew themselves by simple
cell division;
2. They can differentiate themselves, be-
come different in the process of growth
or take on properties of several different
cell structures and tissues based on need;
3. They can be transplanted into other
organisms where they will continue to
divide and differentiate.
Adult stem cells can be found in the skin,
bone marrow, brain, blood vessels, liver and
skeletal muscle. Theoretically, stem cells can
be used to heal, or even regenerate, damaged
tissue. It was believed that there were no
stems cells in the lungs themselves. Recently
researchers at Brigham Women’s Hospital
found stem cell evidence in 12 adult donor
lungs and nine lungs from fetuses that had
died of natural causes. And much to every-
one’s amazement, these stem cells were able
to divide and form new lung structures!
Stem cell replacement therapy is not being
offered to patients with any form of lung dis-
ease in the United States. Stem cell pioneers
see this therapy as perhaps a promising new
direction to take in finding new ways to treat
all lung disease, including COPD. Finding
adult stem cells in adult human lungs elim-
November/December 2014 www.pulmonarypaper.org 23
inates at least one of the powerful ethical
dilemmas concerning stem cell replacement
therapies – the need for fetal blood from
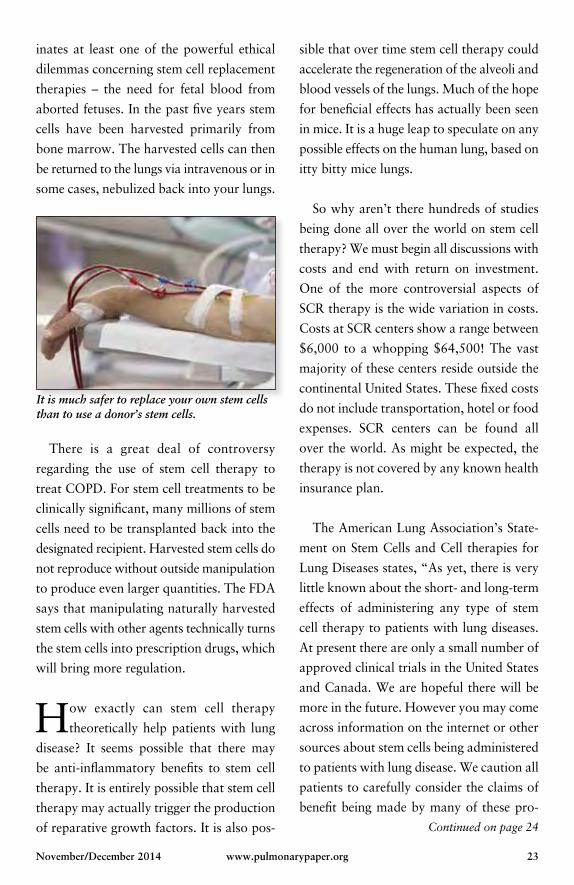
aborted fetuses. In the past five years stem
cells have been harvested primarily from
bone marrow. The harvested cells can then
be returned to the lungs via intravenous or in
some cases, nebulized back into your lungs.
sible that over time stem cell therapy could
accelerate the regeneration of the alveoli and
blood vessels of the lungs. Much of the hope
for beneficial effects has actually been seen
in mice. It is a huge leap to speculate on any
possible effects on the human lung, based on
itty bitty mice lungs.
So why aren’t there hundreds of studies
being done all over the world on stem cell
therapy? We must begin all discussions with
costs and end with return on investment.
One of the more controversial aspects of
SCR therapy is the wide variation in costs.
Costs at SCR centers show a range between
$6,000 to a whopping $64,500! The vast
majority of these centers reside outside the
continental United States. These fixed costs
do not include transportation, hotel or food
expenses. SCR centers can be found all
over the world. As might be expected, the
therapy is not covered by any known health
insurance plan.
The American Lung Association’s State-
ment on Stem Cells and Cell therapies for
Lung Diseases states, “As yet, there is very
little known about the short- and long-term
effects of administering any type of stem
cell therapy to patients with lung diseases.
At present there are only a small number of
approved clinical trials in the United States
and Canada. We are hopeful there will be
more in the future. However you may come
across information on the internet or other
sources about stem cells being administered
to patients with lung disease. We caution all
patients to carefully consider the claims of
benefit being made by many of these pro-
It is much safer to replace your own stem cells than to use a donor’s stem cells.
There is a great deal of controversy
regarding the use of stem cell therapy to
treat COPD. For stem cell treatments to be
clinically significant, many millions of stem
cells need to be transplanted back into the
designated recipient. Harvested stem cells do
not reproduce without outside manipulation
to produce even larger quantities. The FDA
says that manipulating naturally harvested
stem cells with other agents technically turns
the stem cells into prescription drugs, which
will bring more regulation.
How exactly can stem cell therapy
theoretically help patients with lung
disease? It seems possible that there may
be anti-inflammatory benefits to stem cell
therapy. It is entirely possible that stem cell
therapy may actually trigger the production
of reparative growth factors. It is also pos- Continued on page 24
24 www.pulmonarypaper.org Volume 25, Number 6
grams as they have not been substantiated.
Because of the potential for harm, the lack
of any proven benefit, and the high fees that
many of these programs charge, we caution
you not to participate in these or any other
comparable unauthorized or unapproved
stem cell administrations, unless indepen-
dent, credible, reliable and objective sources
of information are available to substantiate
the information and claims being made.”
The ALA recommends the International
Society for Stem Cell Research (ISSCR) as a
reliable source for information. If you’d like
more detailed information please visit www.
closerlookatstemcells.org.
ISSCR, in its recently published hand-
book, tells us, “The ISSCR is very concerned
that stem cell therapies are being sold around
the world before they have been proven safe
and effective. Stem cell therapies are nearly
all new and experimental. In these early
stages, they may not work, and there may
be downsides. Like any new drug, stem cell
therapies must be assessed and meet certain
standards before receiving approval from
national regulatory bodies to be used to
treat people.”
This leads me to a topic sometimes
known as “Stem Cell Tourism.”
Stem cell tourism is when people travel
to another country to receive treatments
unavailable to them at home. It exists chief-
ly because most stem cell “treatments” are
unproven and not readily available from rep-
utable local medical services. Stem cell tour-
ism is sustained because of a religious-like
belief in the promise of the regenerative
powers of stem cells.
Continued from page 23
Medical Tourism is also becoming
popular with United States companies.
We learned of a furniture and auto
parts manufacturer in western North
Carolina who gave employees a choice
for their surgery: Pay a co-pay in the
United States or have the procedure
done abroad for free. One lady had
weight loss surgery and another man
had a knee replacement at a private hos-
pital in Costa Rica. Nearly one million
Americans go overseas for procedures
every year, according to the U.S. Centers
for Disease Control and Prevention.
While it all sounds too good to be true,
medical experts cautioned that there
are serious concerns about “medical
tourism” and having procedures done
overseas. Glenn Cohen, co-director of
the Petrie-Flom Center for Health Law
Policy at Harvard University, said there
is a risk of post-operative complications
and said there have been documented
cases of people dying or developing in-
fections after having surgeries in foreign
countries.
The problem of “questionable” stem cell
clinics has been growing over the past five to
10 years. Stem cell centers can be found in
November/December 2014 www.pulmonarypaper.org 25
many countries around the word. Since they
are outside the purview of the FDA, they can
make all kinds of claims and offer stem cell
treatments for fatal or incurable diseases like
ALS, spinal cord injury and even strokes.
Targeting mostly affluent westerners, costs
can easily exceed $100,000. Look closely at
the various Internet ads for stem cell centers.
You will most commonly find testimonials
from patients who have had near miraculous
responses. A logical question might be “Why
not then publish your data and undergo
rigorous peer review?” It is not unusual to
find stem cell centers just over the border
from modern medicine practiced here in the
United States. Mexico is convenient for both
medical staff and most patients. There are
around 20 stem cell replacement clinics in
Tijuana alone. Are they selling desperate pa-
tients a 21st century version snake oil? There
will always be someone who swears they got
better from whatever ailed them in the first
place by taking a couple of teaspoons. You
can read testimonial after testimonial on the
websites of the replacement centers describ-
ing fantastic results. It would seem there is
no better indication for Caveat Emptor – Let
the Buyer Beware!
After consulting with many experts, they
are not aware of any stem cell research
being done. This does not mean that some-
where within the academic community of
the United States there isn’t solid research
happening as I write this. Undoubtedly there
are legitimate studies being done.
Stem cell therapy for lung disease is in its
infancy. Theoretically it has the possibility
of bringing great hope to many patients
who have exhausted other forms of medical
therapy to treat their lung disease. On paper,
stem cell replacement therapy looks like it
may be the next “BIG” thing. However, the
biochemical, and technical bridges that need
to be crossed are substantial.
Do you remember when Fen-phen was
the hottest new diet pill? It was actu-
ally on the September 1996 cover of Time
magazine, the same year it was placed on
the market. Sales in that first year were $300
million as more than 18 million prescriptions
were filled. Fen-phen was pulled off the mar-
ket in September 1997 by the FDA as there
were at least 75 reports of Fen-phen induced
heart injuries. Some patients had taken the
drug for as little as a month and developed
serious cardiac complications including the
uni formly fatal Primary Pulmonary Hyper-
tension.
Let us heed the message so powerfully sent
by the Fen-phen disaster. Stem cell research
is so very promising in the possible treatment
of so many diseases and chronic conditions.
If you or a loved one is contemplating stem
cell replacement therapy, spend the time
investigating your particular situation. Make
sure you meet and talk with your family
physician, specialist, and certainly spend
your time wisely in gathering your data.
Happy Holidays!
John R. Goodman BS RRT is Executive Vice President of Technical / Profes -sional Services at Transtracheal Ser-vices, Denver, CO, who says “All You Need Is Love!”
26 www.pulmonarypaper.org Volume 25, Number 6
Readmission PenaltiesMore than 2,600 hospitals have been fined
because too many Medicare patients being
treated for heart failure, heart attack, pneu-
monia, elective hip and knee replacement
readmissions and chronic lung disease. As
What Exactly is Ebola?The American Association for Respiratory
Care tells us the first case of Ebola outside of
Africa was reported in Dallas, Texas earlier
this year. Ebola is a rare and deadly disease
caused by infection with a strain of Ebola
virus. The 2014 Ebola epidemic is the largest
in history, affecting multiple countries in
West Africa. The risk of an Ebola outbreak
affecting multiple people in the United States
is very low.
The virus is spread from human to human
by direct contact with the blood or body
fluids of a person who has been infected with
Ebola. Needles and syringes that have been
contaminated with the virus can be a source
of transmission as well. Ebola is not spread
through the air, water, food or mosquitoes.
It can be spread by infected animals.
First symptoms are the sudden onset of
fever, fatigue, muscle pain, headache and
sore throat. This is followed by vomiting,
part of their Hospital Readmission Reduc-
tion Program, Medicare reduced payments
to hospitals that had high readmission rates.
The program intended to provide incen-
tives for hospitals to reduce readmissions
and improve the quality of their care, but
research has shown that patients are often
readmitted for reasons beyond the control
of hospitals. Poor or medically complex
patients are at a higher risk for readmissions
because of socioeconomic and health factors.
If patients can’t afford medications, or have
unstable housing situations, they may end
up being readmitted. No interventions to
date have effectively reduced COPD read-
missions, so it’s unclear what a hospital can
do to prevent them.
diarrhea, rash and symptoms of impaired
kidney and liver function. The symptoms
will not show up right after exposure, most
people show signs and symptoms around the
eighth to tenth day after exposure.
The Centers for Disease Control and
Prevention states, “Recovery from Ebola
depends on good supportive clinical care
and the patient’s immune response. People
who recover from Ebola infection develop
antibodies that last for at least 10 years.”
November/December 2014 www.pulmonarypaper.org 27
What to Say and What Not to Say!
Don’t say this:You don’t look sick. (We are not quite
sure what “sick” looks like.)
You’re too young to be sick. (Like you
have some control over this!)
Don’t worry, everyone gets tired.
(There are different kinds of tired –
tired from running a race or tired from
taking a shower.)
You’re just having a bad day. (They
sound as if they are brushing off your
symptoms.)
It must be nice not having to go to
work. (They don’t know how much
you miss it!)
You need to get more exercise. (Good
idea but they sound like this is going to
be the cure for everything.)
It could be worse. (And it could be
better!)
I’m sorry, or You’re so brave. (Don’t
pity me, just support me!)
Just push through it. (Do I have an-
other choice?)
It will get better! (Unless they have a
cure we don’t know about, we would
rather be the best we can with what
we have!)
Have you tried … My second cousin
has lung problems and is doing great!
(Just smile and agree to try whatever
they suggest you try.)
The worst thing you can say to some-
one who is coughing or short of breath
… Are you okay?
But do say or do this:Can I come over and hang out? or Can
I bring you food? or Can I come over
and help out around the house?
I know how hard you are trying. I
believe in you.
A call, email, card or text message just
to let you you know they are thinking
of you.
You are so strong. This must be frus-
trating for you.
How does it feel when …? Tell me
about …?
How can I help?
Don’t feel bad if you have to cancel
plans at the last minute, I understand.
Let’s pencil them in.
Sometimes the best thing you can say
is nothing – just listen.
I missed you when you weren’t able to
come to the event.
Forget the guilt about smoking – this
isn’t your fault.
I wish I knew what to say, but I care
about you and I’m here for you.
We bet you have heard many of the comments that are listed here. People mean well, but many times don’t understand what they are really saying to a person dealing with a chronic medical condition! Are you nodding your head in agreement as you read?
October 18–28, 2015 Take this incredible 11-day journey round trip from Fort Lauderdale to the Panama Canal – an undisputed bucket list trip aboard the Coral Princess!
Panama Canal 11 DAYS
July 25–August 1, 2015 Explore Alaska’s Inner Passage, round trip from Seattle on our annual vacation to Alaska, aboard Holland America’s Westerdam!
Alaska Inner Passage 7 DAYS
Mexican Riviera 7 DAYS
West Coast Departure
Visit www.seapuffers.com for more information!
January 17–24, 2015 Start the New Year right with a 7-day cruise on the Grand Princess, round trip from Los Angeles. Enjoy relaxing sea days and visits to Puerto Vallarta, Mazatlan and Cabo San Lucas!
28 www.pulmonarypaper.org Volume 25, Number 6
March 20–30, 2015 Enjoy 10 days of Spring on Holland America’s Noordam, leaving round trip from Fort Lauderdale.
Oxygen Guru Ryan Diesem will be our guest speaker!
Southern Caribbean 10 DAYS
GIVE THE GIFT OF A LIFETIME!
2015Sea Puffer Group Cruises

FST–
ST39
068
Member
TAKE A WORRY-FREE VACATION AND EXPLORE THE WORLD!CALL TODAY!Join the Sea Puffers on one of our group cruises escorted by respiratory therapists! Call 1-866-673-3019 to also arrange your own cruise or tour! We make it easy to travel with oxygen! Join the Sea Puffers family for life-long friendships and support.
November/December 2014 www.pulmonarypaper.org 29
30 www.pulmonarypaper.org Volume 25, Number 6
Respiratory NewsTreatment with 400 mcg Tudorza Pres-
sair – aclidinium bromide inhalation powder
– daily over a year-long period appears to
bring relief of symptoms associated with
COPD. Findings were presented at the 2014
Annual Meeting of the American College of
Chest Physicians.
An FDA advisory committee voted that
Varenicline (Chantix), a drug to help people
stop smoking, should continue to carry a
boxed warning about the risk of side effects,
with several panel members suggesting it
should be strengthened.
Chantix is not addictive but some people
may experience irritability and sleep distur-
bance if the drug is abruptly discontinued.
Psychiatric symptoms such as behavioral
changes, agitation, depressed mood and
suicidal behavior have been reported while
using Chantix.
The drug’s effectiveness was not ques-
tioned.
A new study, ‘Continuing to Confront
COPD International Patient Survey: Meth-
ods, COPD Prevalence and Disease Burden
2012–2013,’ published this year in the Inter-
national Journal of COPD, puts a new face
to the disease – and it is a feminine one. The
study reveals that COPD rates in the United
States are higher among females than males.
Just so you know, the National Institutes
of Health published a report that states there
is unequivocal evidence that habitual or
regular marijuana smoking is not harmless.
A caution against regular heavy marijuana
usage is prudent. The medicinal use of mar-
ijuana is likely not harmful to lungs in low
cumulative doses, but the dose limit needs
to be defined.
Recreational use is not the same as medic-
inal use and should be discouraged.
Even though it doesn’t get much publicity,
lung cancer is the leading cancer killer for
both men and women in the United States.
Medicare recently determined that people
who meet three criteria: 55 to 74 years of
age, a smoking history of 30 pack years, and
still smoking or have quit smoking within
the last 15 years are considered high risk
and will be eligible for an annual low-dose
CT scan. Medicare also proposes high risk
individuals will need to go to a radiology
imaging center whose experts have signifi-
cant experience in recognizing lung cancer
on CT scans. Show your support for lung
cancer screening with the American Lung
Association by going to this website http://
bit.ly/1EmKM9M

November/December 2014 www.pulmonarypaper.org 31
Would you or a friend like to receive our newsletter every other month? Complete and mail this form or visit our website today! www.pulmonarypaper.org
ANNUAL DONATION o Check here if renewal
• Individual with lung problems:
o $25 o $50 o Other ___________
• Health Professional: o $50 (1 copy/issue/year)
o $250 (25 copies/issue/year)
o $400 (50 copies/issue/year)
o Check (Payable to: The Pulmonary Paper)
o VISA o AMEX o MasterCard o Discover
Card No.:
Exp. Date:
Signature:
Name
Address
City State Zip
Phone
Respiratory Diagnosis
Please fill out this form and mail back to The Pulmonary Paper at the address below with your donation information.
11/1/14
The Pulmonary Paper, PO Box 877, Ormond Beach, FL 32175-0877 1-800-950-3698 • Fax 386-673-7501 • www.pulmonarypaper.org
The Pulmonary Paper is a 501 (c)(3) not-for-profit corporation and supported by individual contributions. Your donation is tax deduct ible to the extent allowed by law.
I I
The
PulmonaryPaperDedicated to Respiratory Health Care
Dedicated to Respiratory Care
Volume 25, No. 6
November/December 2014
The Pulmonary Paper PO Box 877Ormond Beach, FL 32175 Phone: 800-950-3698Email: [email protected]
The Pulmonary Paper is a 501(c)(3) not-for-profit corporation supported by individual gifts. Your donation is tax deduc tible to the extent allowed by law.
All rights to The Pulmonary Paper (ISSN 1047-9708) are reserved and contents are not to be reproduced without permission.
As we cannot assume responsibility, please contact your physician before changing your treat ment schedule.
The Pulmonary Paper StaffEditor . . . . Celeste Belyea, RN, RRT, AE-C, FAARC
Associate EditorDominic Coppolo, RRT, AE-C, FAARC
Design . . . . . . . . . . . . . . . . . . . . . Sabach Design
Medical Director . . . . . . . . . . Michael Bauer, MD
The Pulmonary Paper is a membership publica-tion. It is published six times a year for those with breathing problems and health profession-als. The editor encourages readers to submit information about programs, equipment, tips or services.
Phone: 800-950-3698 • Fax: 386-673-7501www.pulmonarypaper.org
The
PulmonaryPaper

Ded
icat
ed to
Res
pira
tory
Hea
lth
Car
e
PO B
ox 8
77, O
rmon
d Be
ach,
FL
3217
5-08
77Pa
per
ThePu
lmon
ary
Non-
Profi
tOr
gani
zatio
nUS
Pos
tage
PAID
Dayt
ona
Beac
h, F
LPe
rmit
#275


















