Algoritmo diagnostico e fattori prognostici - Siematologia · 2009-06-24 · Algoritmo diagnostico...
44
Algoritmo diagnostico e fattori prognostici Francesco Passamonti Clinica Ematologica Università di Pavia Fondazione IRCCS Policlinico San Matteo, Pavia
Transcript of Algoritmo diagnostico e fattori prognostici - Siematologia · 2009-06-24 · Algoritmo diagnostico...

Algoritmo diagnostico efattori prognostici
Francesco PassamontiClinica EmatologicaUniversità di Pavia
Fondazione IRCCS Policlinico San Matteo, Pavia
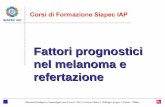
Molecular basis of MPNCytogenetic
abnormalitiesMutation ofoncogenesJAK2-V617FJAK2-ex12MPL-W515LMPL-W515KMPL-S505NMPL-A506TMPL-A519T
TET2
del13qdel20qdel7pdel7qdel12p
Normal cells
MPNphenotype
Phen
otyp
icle
sion
Non phenotypic
lesion
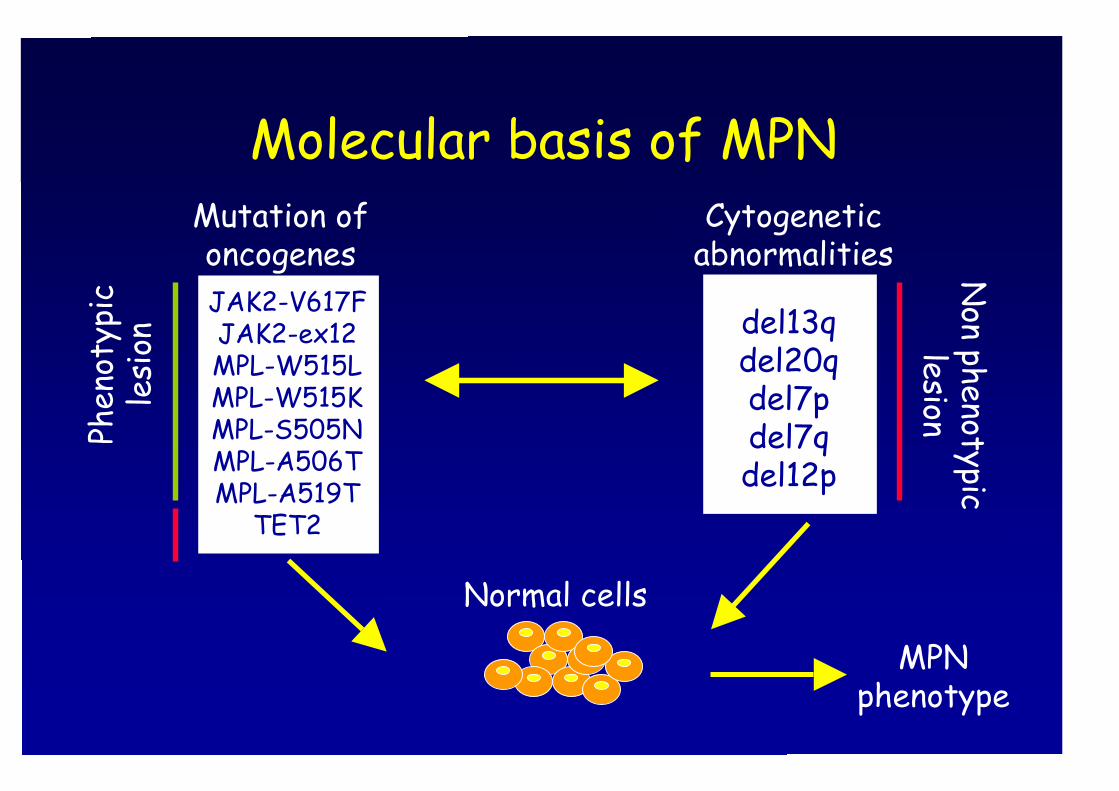
Mutational status in MPN: state of the art
0
20
40
60
80
100
!" #$ !%&
'()(*+(,-./0/1*(2
$#$3,-./0/1*(2
%!4,-./0/1*(2
5673,#8,93,-./0/1*(2
5673,:";9<&=,-./0/1*(
Updated criteria for diagnosis
ETPVPMF
Post-ET MFPost-PV MF
WHO, 2008
IWG-MRT, 2007

Policitemia veraCriteri maggiori1. Hb > 18,5 g/dL (M), > 16.5 g/dL (F)2. Mutazione JAK2 (V617F) o esone 12Criteri minori1. Ipercellularità midollare con iperplasia trilineare2. Bassi livelli serici di eritropoietina3. Crescita spontanea di colonie eritroidi
Diagnosi:2 criteri maggiori e 1 tra i minoriPrimo maggiore e 2 tra i minori
Trombocitemia essenzialeCriteri1. Piastrine > 450 x 109/L2. Proliferazione prominente megacariociti3. Esclusione PV, PMF, LMC, MDS4. Mutazione JAK2 (V617F) o altre anomalie
clonali; se assenti escludere cause secondarie
Diagnosi: 4 criteri

Mielofibrosi primariaCriteri maggiori1. Proliferazione megacariociti con atipie e fibrosi reticolinica;
se non fibrosi reticolinica proliferazione megacariociti conatipie, iperplasia granulocitaria, ipoplasia eritroide
2. Esclusione PV, LMC, MDS3. Mutazione JAK2 (V617F), o altre anomalie clonali (mutazioni
MPL); se assenti, escludere cause secondarieCriteri minori1. Screzio leucoeritroblastico2. Incremento LDH3. Anemia4. Splenomegalia palpabile
Diagnosi: 3 maggiori e 2 tra i minori
Comments on WHO classification• Based on practical and reproducible clinical,
histopathological and molecular findings• Evidence of clonal hematopoieis• Bone marrow findings• Erythropoietin• Increase of hemoglobin over time• Red cell mass (the end)• Prefibrotic myelofibrosis: a vanishing entity
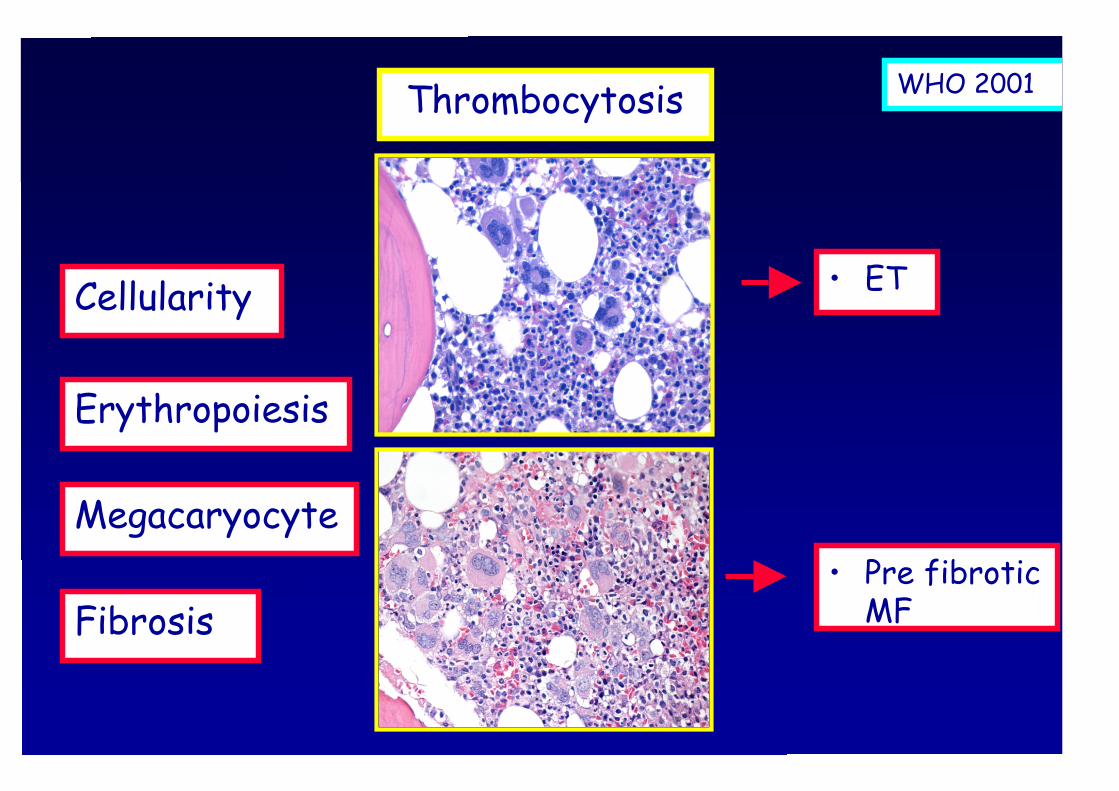
Cellularity
Erythropoiesis
Megacaryocyte
Fibrosis
Thrombocytosis
• Pre fibroticMF
• ET
WHO 2001
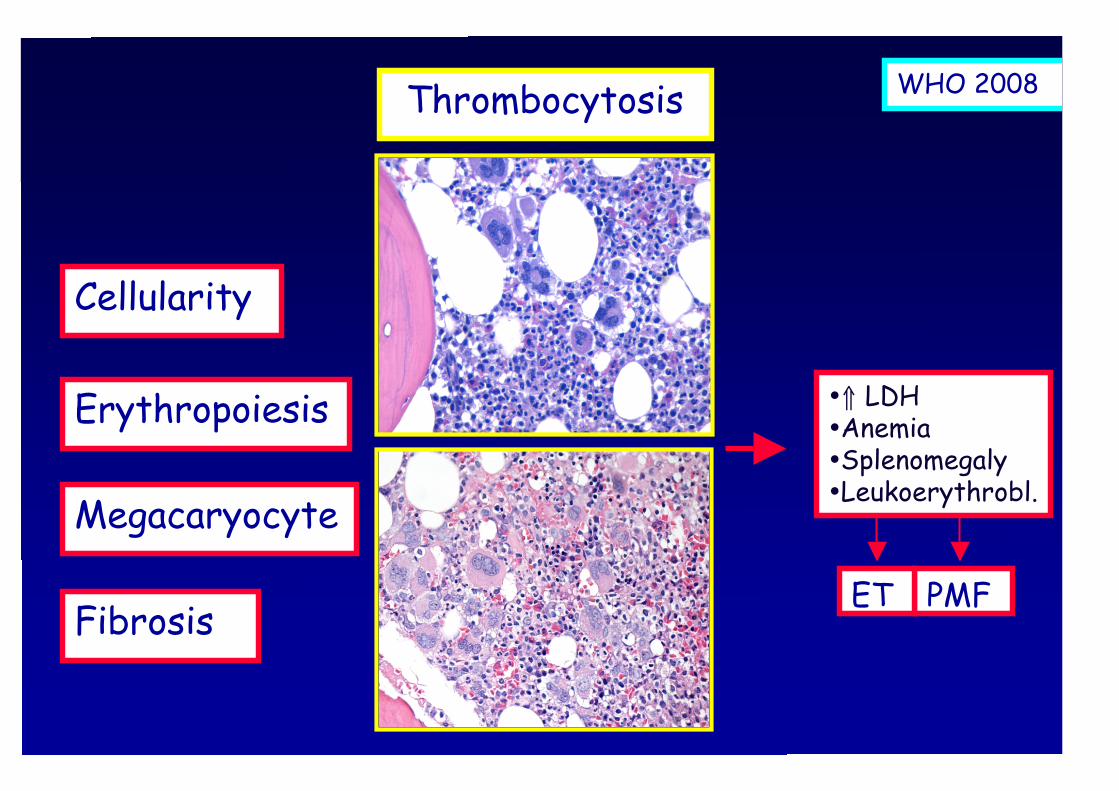
Cellularity
Erythropoiesis
Megacaryocyte
Fibrosis
Thrombocytosis
•⇑ LDH•Anemia•Splenomegaly•Leukoerythrobl.
PMFET
WHO 2008

Algoritmi diagnostici perl’inquadramento delle MPN
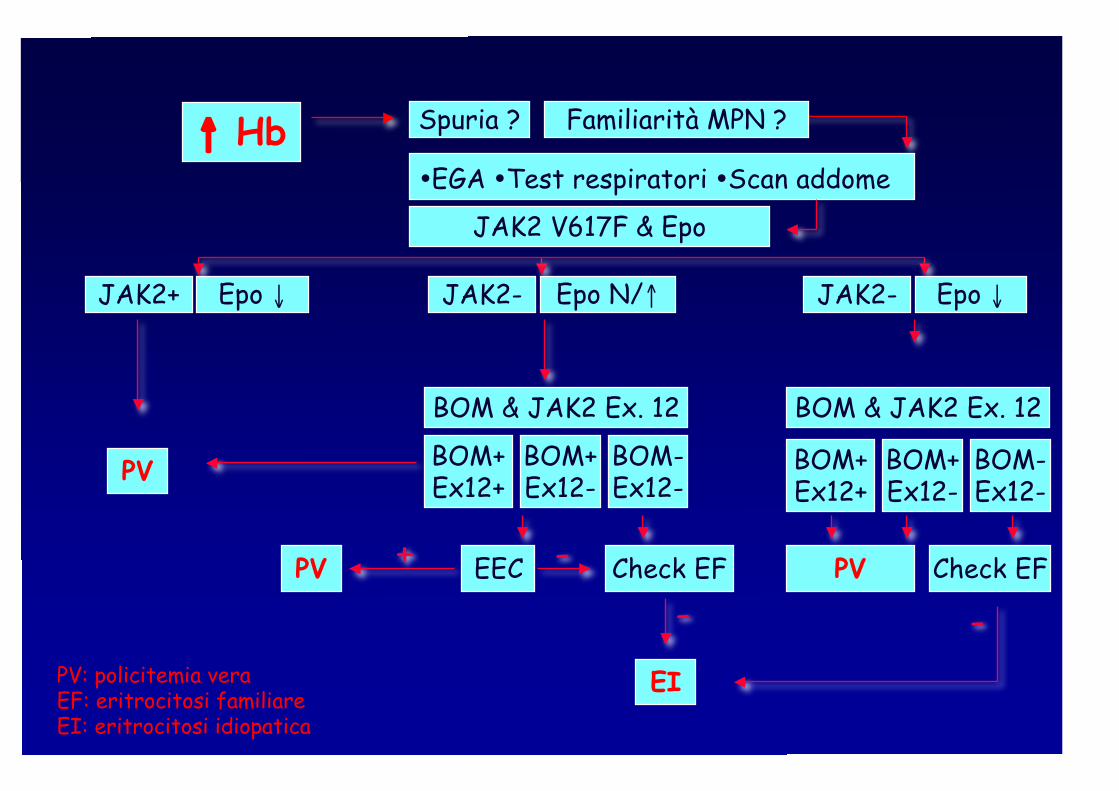
↑ Hb
JAK2 V617F & Epo
JAK2+ Epo ↓ JAK2- Epo N/↑ JAK2- Epo ↓
BOM+Ex12+
BOM+Ex12-
BOM-Ex12-
BOM & JAK2 Ex. 12
•EGA •Test respiratori •Scan addome
Spuria ?
PV BOM+Ex12+
BOM+Ex12-
BOM & JAK2 Ex. 12
BOM-Ex12-
PV
EI
Check EF
Familiarità MPN ?
EECPV + -- -
PV: policitemia veraEF: eritrocitosi familiareEI: eritrocitosi idiopatica
Check EF
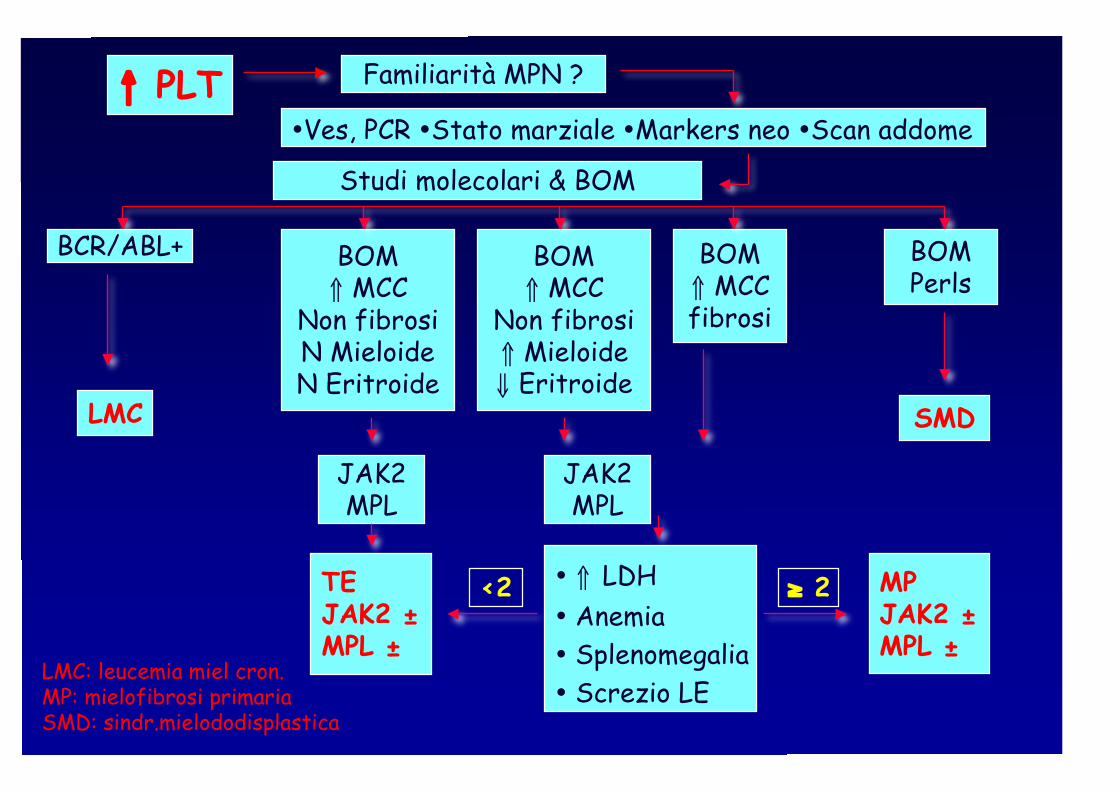
↑ PLT
Studi molecolari & BOM
BCR/ABL+
•Ves, PCR •Stato marziale •Markers neo •Scan addome
LMC
Familiarità MPN ?
BOM⇑ MCCfibrosi
• ⇑ LDH• Anemia• Splenomegalia• Screzio LE
MPJAK2 ±MPL ±
SMD
BOM⇑ MCC
Non fibrosi⇑ Mieloide⇓ Eritroide
BOM⇑ MCC
Non fibrosiN MieloideN Eritroide
TEJAK2 ±MPL ±
JAK2MPL
BOMPerls
≥ 2<2
LMC: leucemia miel cron.MP: mielofibrosi primariaSMD: sindr.mielododisplastica
JAK2MPL
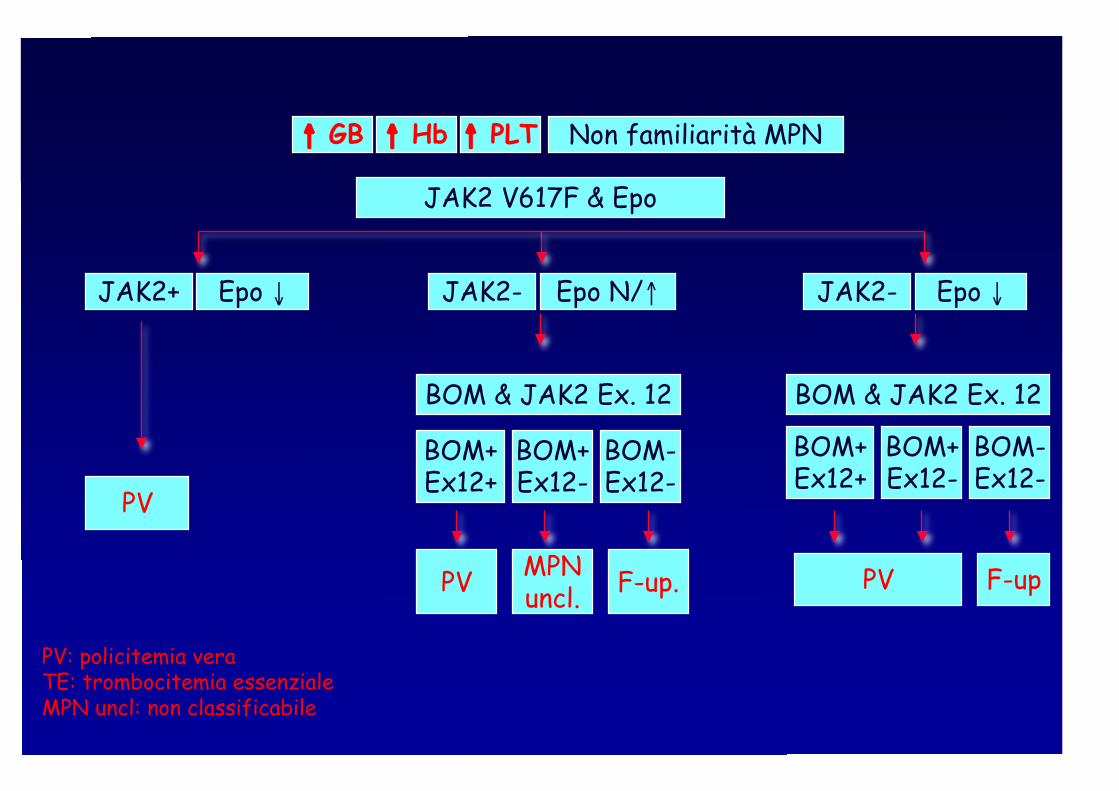
↑ GB ↑ Hb ↑ PLT
JAK2 V617F & Epo
Non familiarità MPN
JAK2+ Epo ↓ JAK2- Epo N/↑ JAK2- Epo ↓
BOM+Ex12+
BOM+Ex12-
BOM & JAK2 Ex. 12
PV
PV
MPNuncl.
BOM-Ex12-
F-up
BOM+Ex12+
BOM+Ex12-
BOM-Ex12-
BOM & JAK2 Ex. 12
PV F-up.
PV: policitemia veraTE: trombocitemia essenzialeMPN uncl: non classificabile

Disease evolution
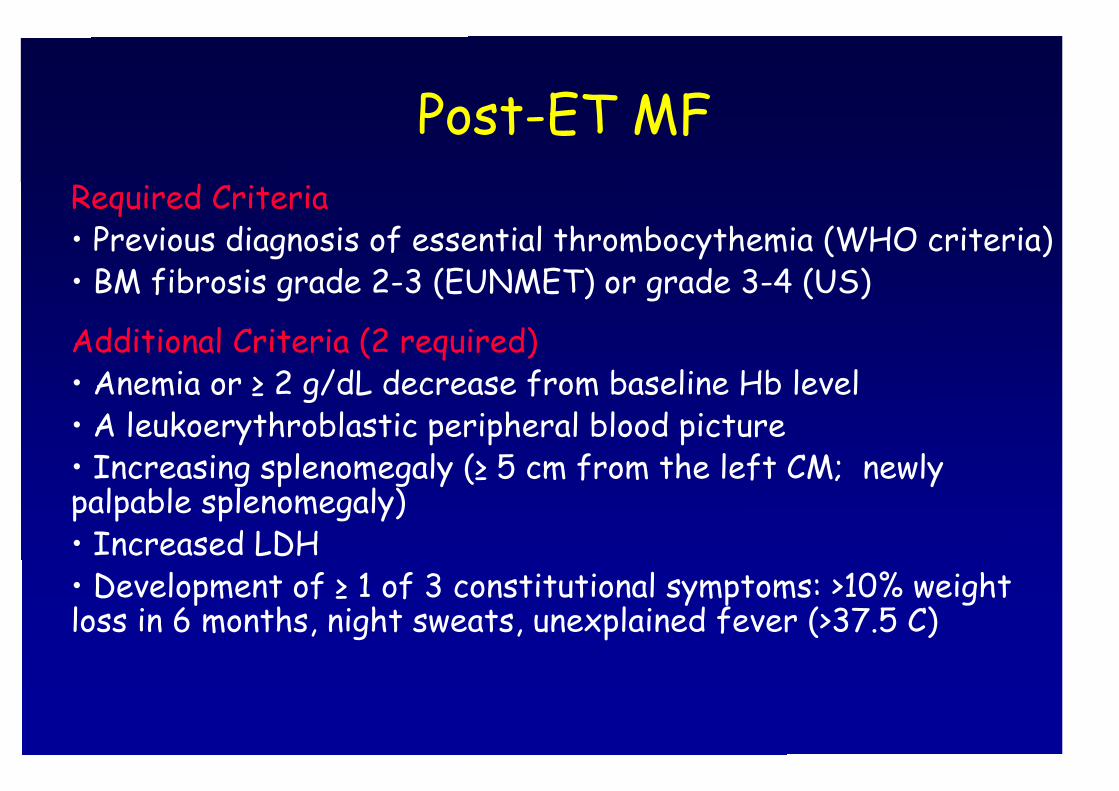
Post-ET MFRequired Criteria• Previous diagnosis of essential thrombocythemia (WHO criteria)• BM fibrosis grade 2-3 (EUNMET) or grade 3-4 (US)
Additional Criteria (2 required)• Anemia or ≥ 2 g/dL decrease from baseline Hb level• A leukoerythroblastic peripheral blood picture• Increasing splenomegaly (≥ 5 cm from the left CM; newlypalpable splenomegaly)• Increased LDH• Development of ≥ 1 of 3 constitutional symptoms: >10% weightloss in 6 months, night sweats, unexplained fever (>37.5 C)
Post-PV MFRequired Criteria• Previous diagnosis of polycythemia vera (WHO criteria)• BM fibrosis grade 2-3 (EUNMET) or grade 3-4 (US)
Additional Criteria (2 required)• Anemia; no requirement of phlebotomy or cytoreduction• A leukoerythroblastic peripheral blood picture• Increasing splenomegaly (≥ 5 cm from the left CM;newly palpable splenomegaly)• Development of ≥ 1 of 3 constitutional symptoms: >10%weight loss in 6 months, night sweats, unexplained fever(>37.5 C)
Prognostic factorsfor disease evolution
Risks and risk factors in ET(n=605, 4596 person-years of f-up)
ThrombosisThrombosis10-year 10-year riskrisk: 14%: 14%RiskRisk factorsfactors: : ageage >60; >60; priorprior thrombosisthrombosis
Myelofibrosis10-year risk: 3.9%Risk factor: Anemia
Leukemia10-year risk: 2.6%Risk factor: Age >60
Passamonti et al, Haematologica 2008
Passamonti et al, Haematologica 2008
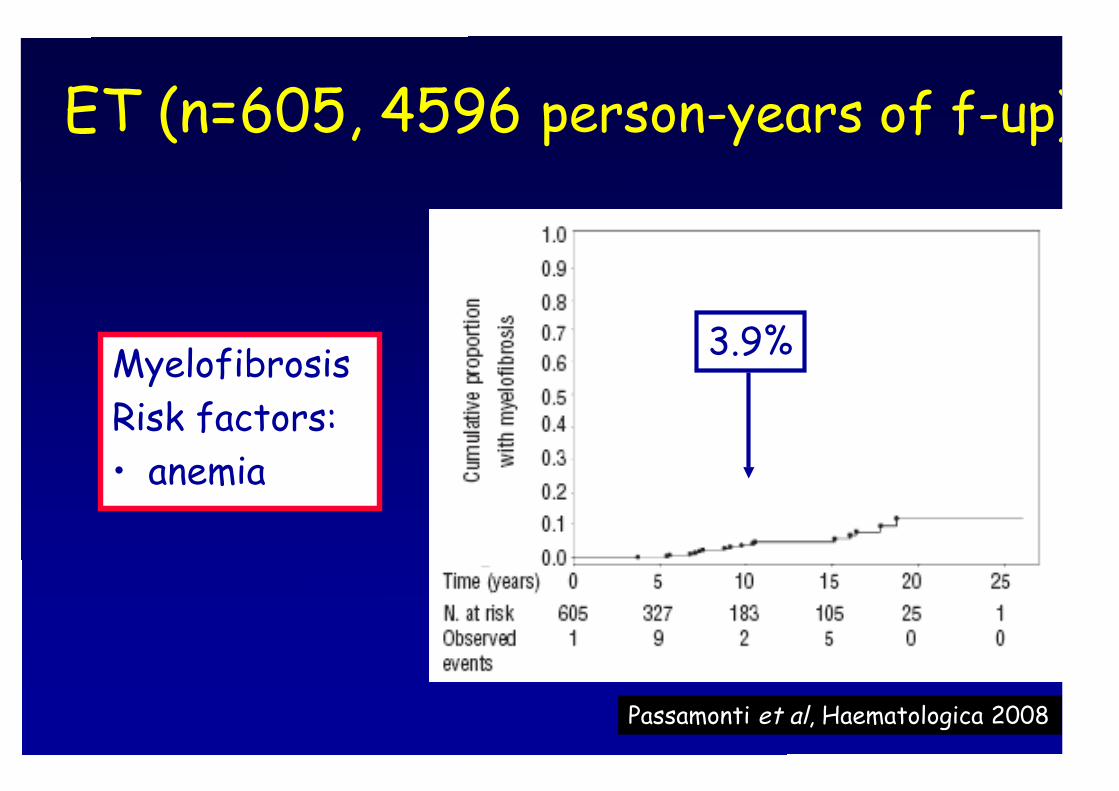
ET (n=605, 4596 person-years of f-up)
3.9%MyelofibrosisRisk factors:• anemia
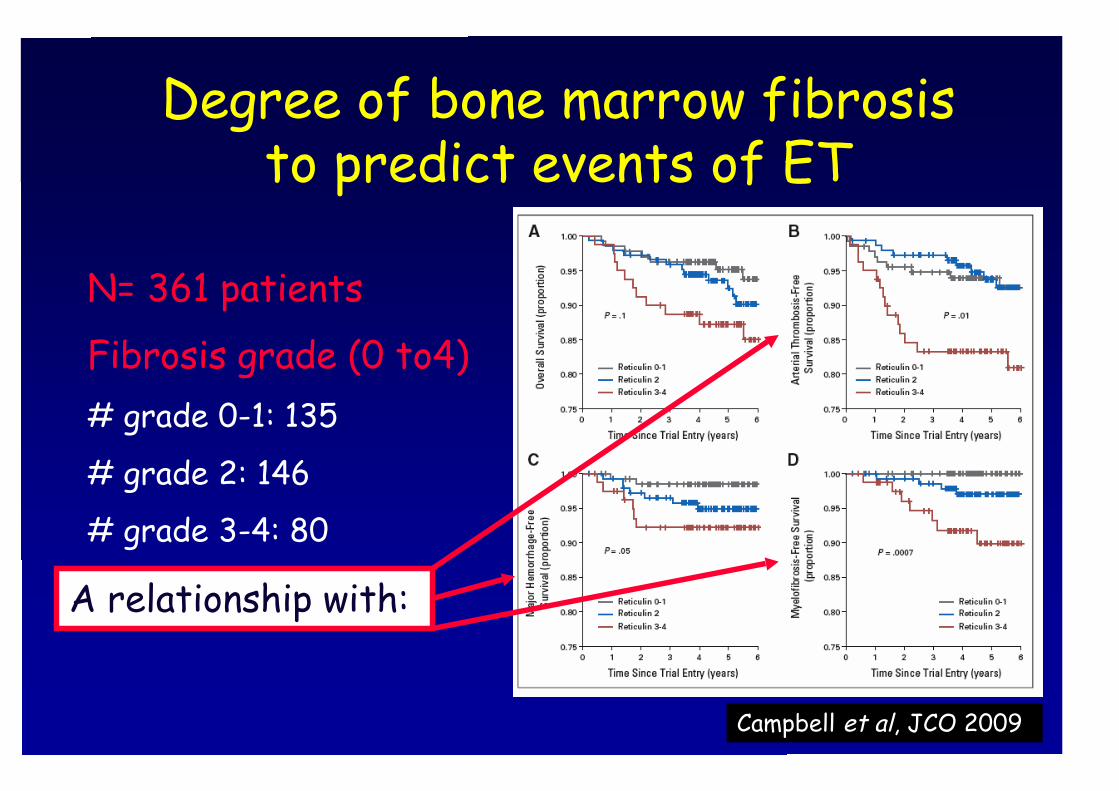
Degree of bone marrow fibrosisto predict events of ET
Campbell et al, JCO 2009
N= 361 patients
Fibrosis grade (0 to4)# grade 0-1: 135
# grade 2: 146
# grade 3-4: 80
A relationship with:
Passamonti et al, Haematologica 2008
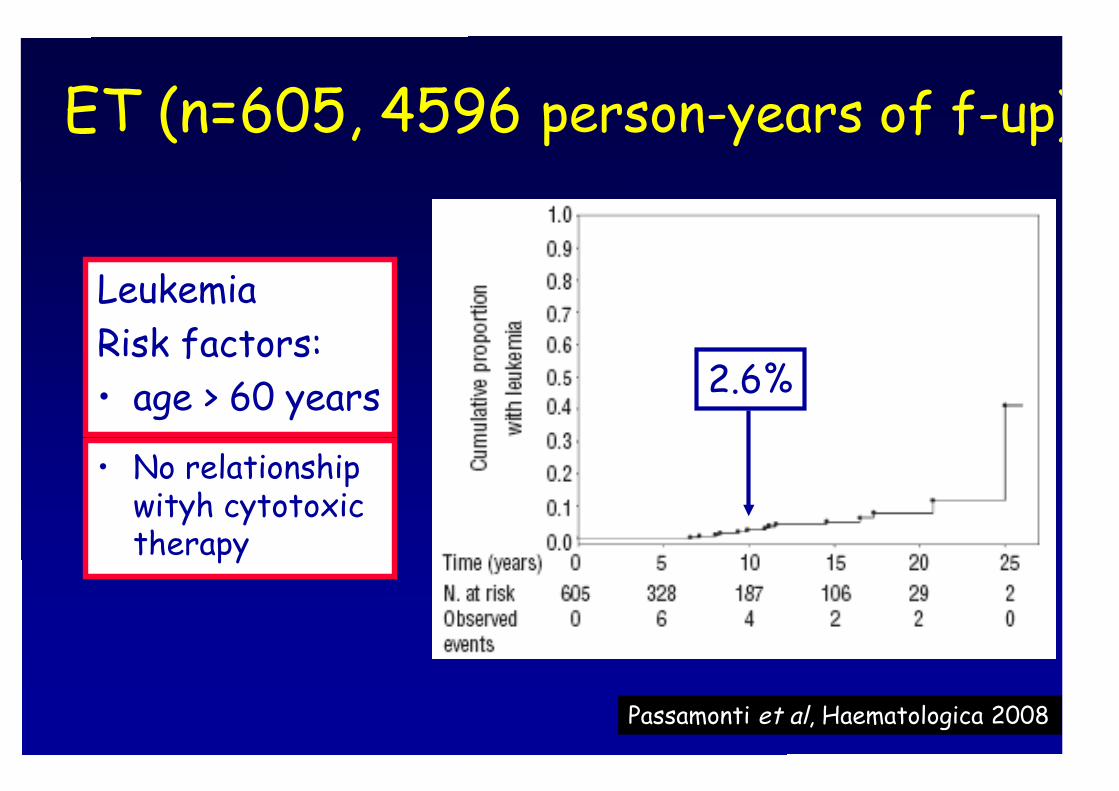
ET (n=605, 4596 person-years of f-up)
2.6%
LeukemiaRisk factors:• age > 60 years
• No relationshipwityh cytotoxictherapy
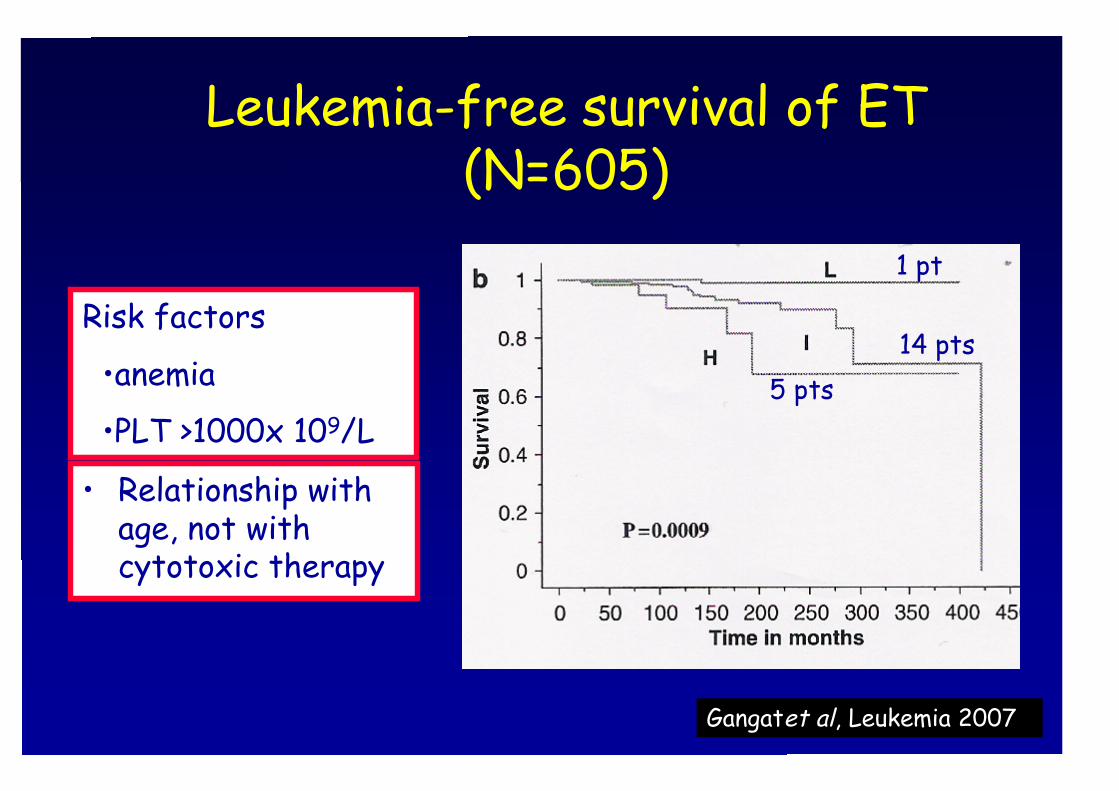
Leukemia-free survival of ET(N=605)
Gangatet al, Leukemia 2007
Risk factors
•anemia
•PLT >1000x 109/L
1 pt
14 pts5 pts
• Relationship withage, not withcytotoxic therapy
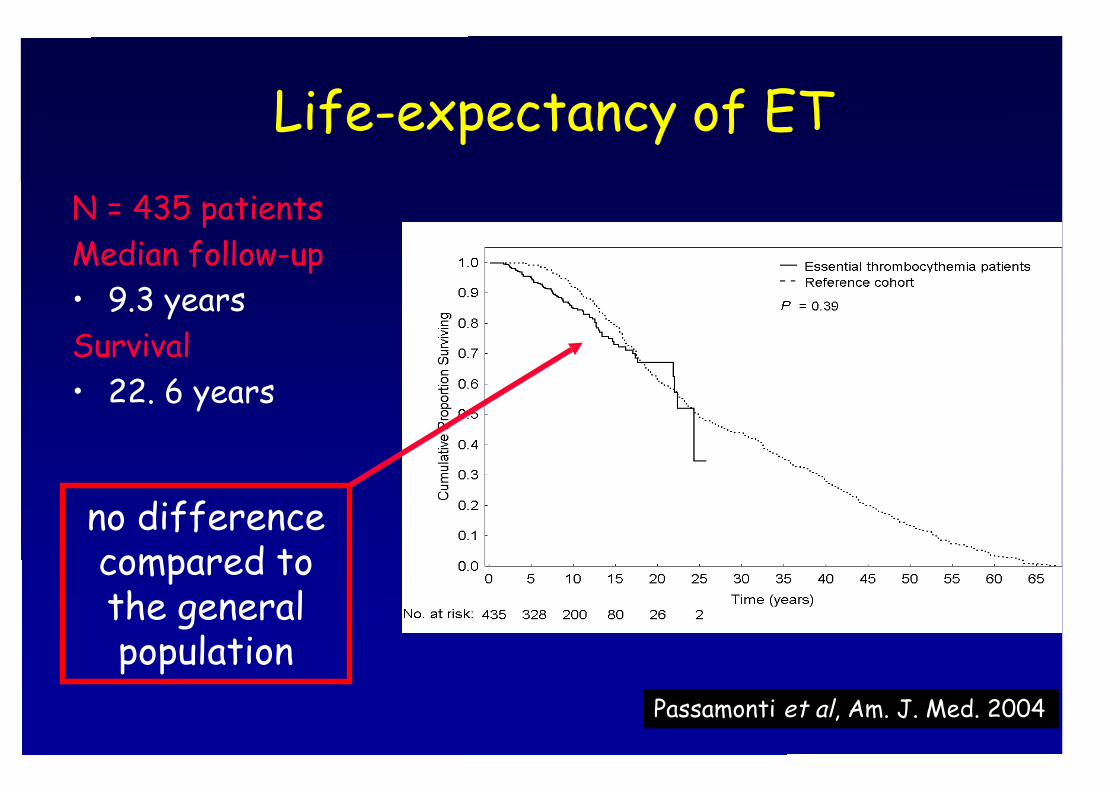
Life-expectancy of ET
Passamonti et al, Am. J. Med. 2004
N = 435 patientsMedian follow-up• 9.3 yearsSurvival• 22. 6 years
no differencecompared tothe generalpopulation
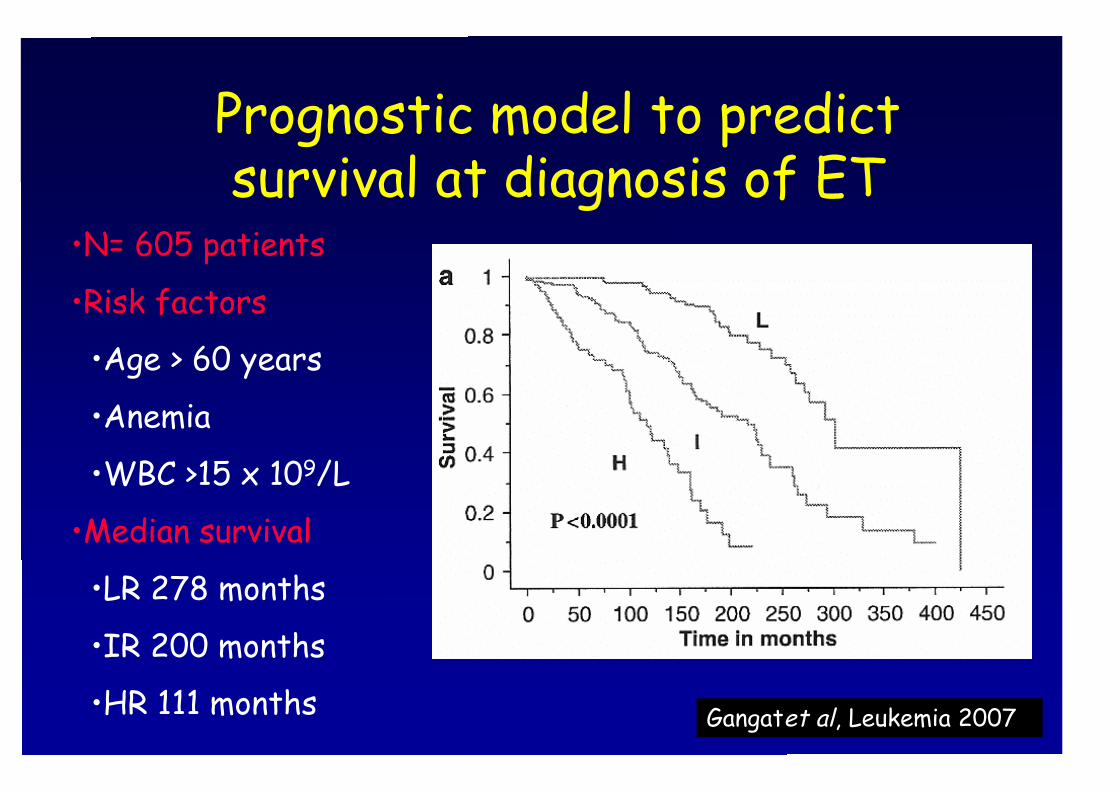
Prognostic model to predictsurvival at diagnosis of ET
Gangatet al, Leukemia 2007
•N= 605 patients
•Risk factors
•Age > 60 years
•Anemia
•WBC >15 x 109/L
•Median survival
•LR 278 months
•IR 200 months
•HR 111 months
Risk factors of PV at diagnosis(ECLAP study 1638 patients)
ThrombosisIncidence: 5.5 x 100 p/yRisk factors: age >65 years; prior thrombosis
Myelofibrosis & LeukemiaIncidence: 1.3 x 100 p/yRisk factors for MF: long disease durationRisk factors fo AL: age >70
Marchioli et al, JCO 2005
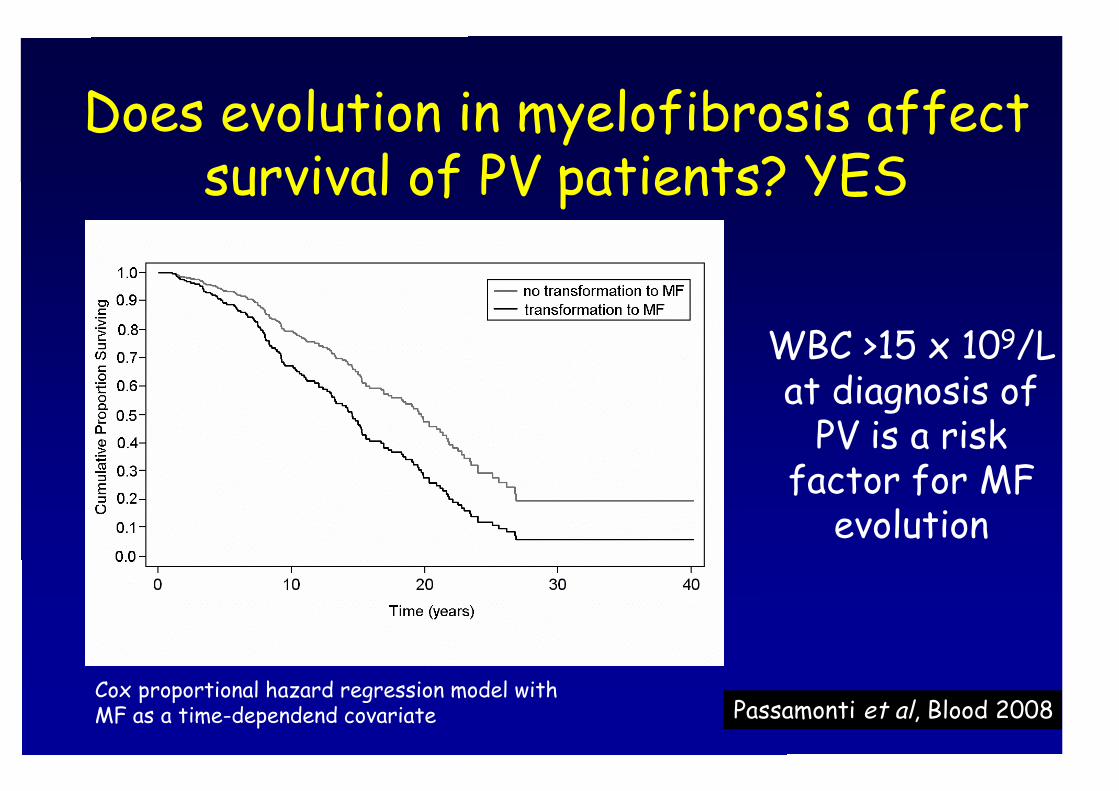
Does evolution in myelofibrosis affectsurvival of PV patients? YES
Passamonti et al, Blood 2008
WBC >15 x 109/Lat diagnosis of
PV is a riskfactor for MF
evolution
Cox proportional hazard regression model withMF as a time-dependend covariate
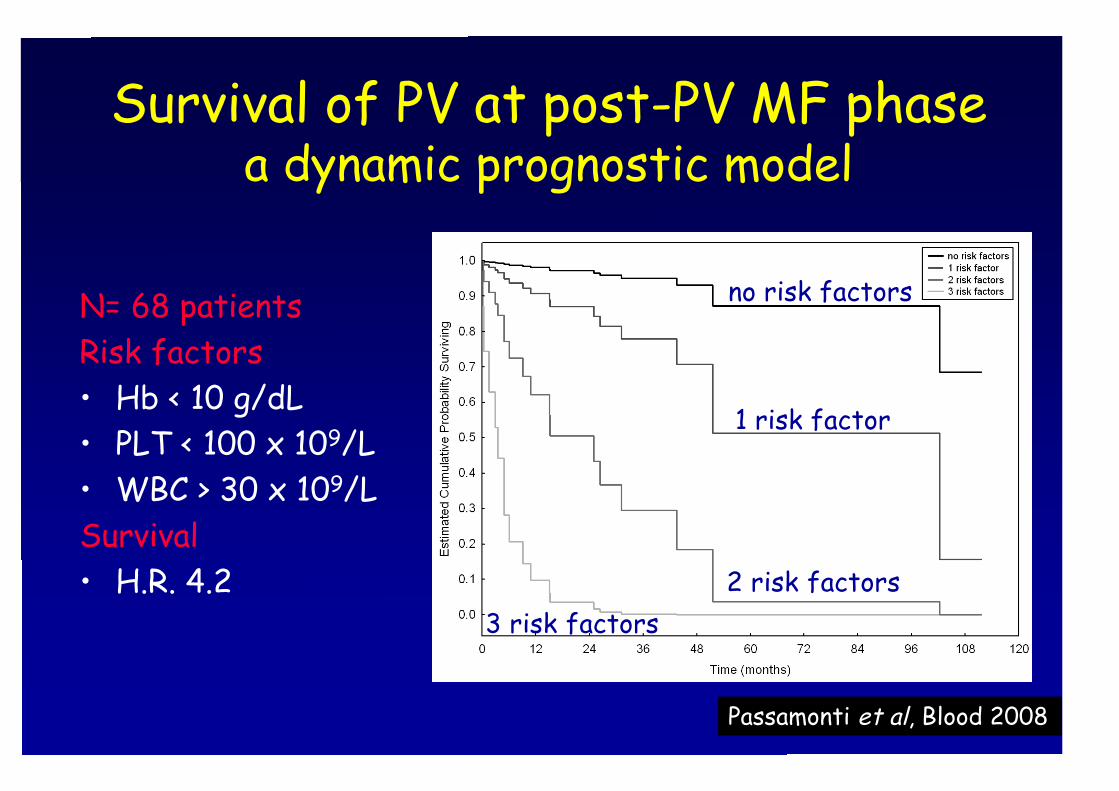
Survival of PV at post-PV MF phasea dynamic prognostic model
Passamonti et al, Blood 2008
N= 68 patientsRisk factors• Hb < 10 g/dL• PLT < 100 x 109/L• WBC > 30 x 109/LSurvival• H.R. 4.2
no risk factors
1 risk factor
2 risk factors3 risk factors
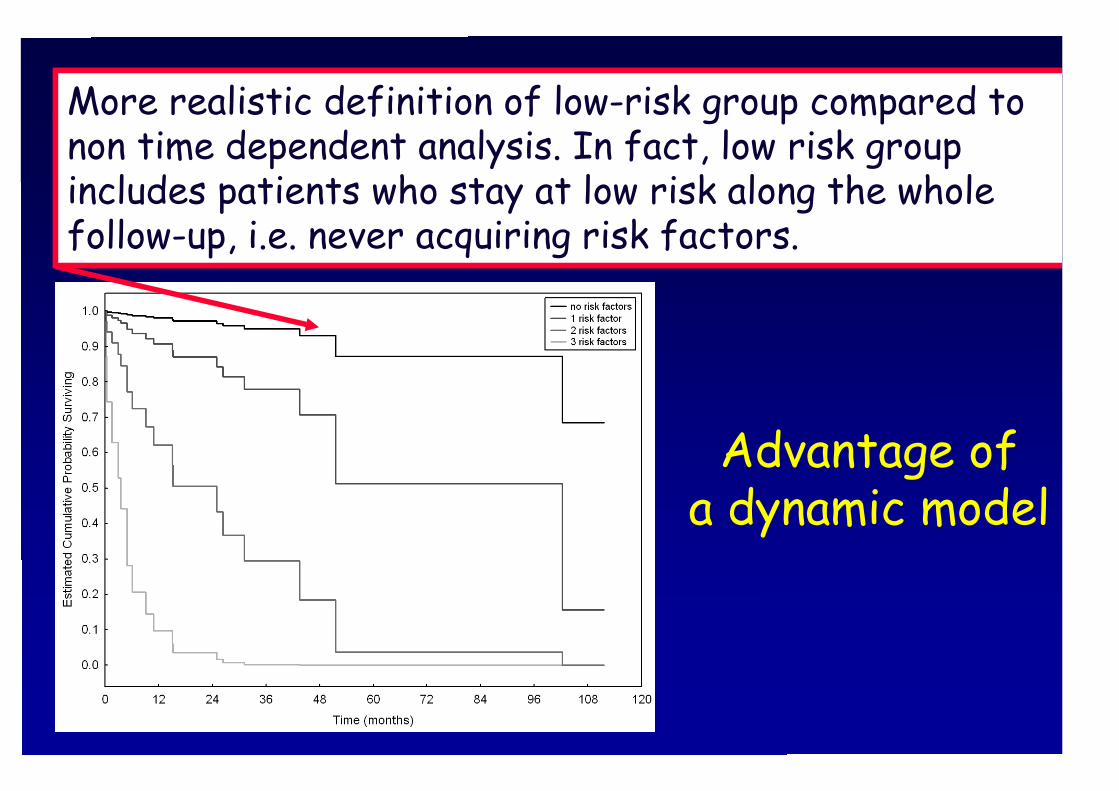
Advantage ofa dynamic model
More realistic definition of low-risk category comparedto non time dependent analysis. In fact, low risk groupincludes patients who never acquire risk factors duringfollow-up.
More realistic definition of low-risk group compared tonon time dependent analysis. In fact, low risk groupincludes patients who stay at low risk along the wholefollow-up, i.e. never acquiring risk factors.
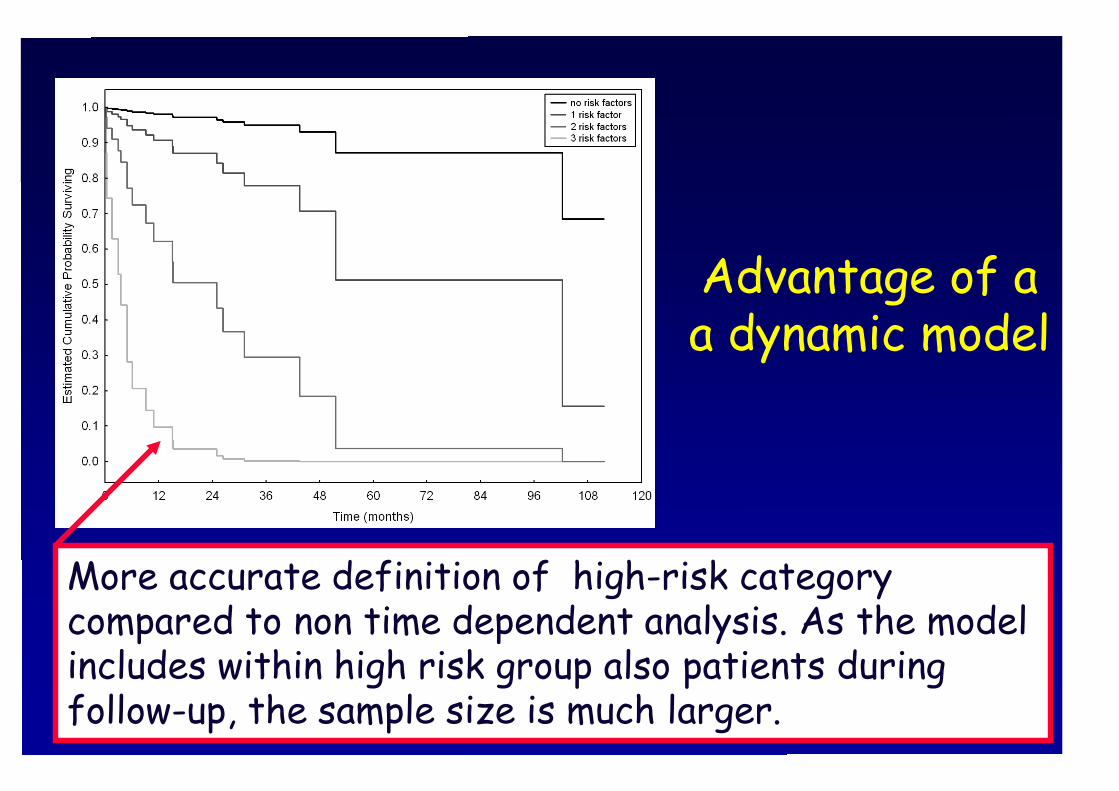
Advantage of aa dynamic model
More accurate definition of high-risk categorycompared to non time dependent analysis. As the modelincludes within high risk group also patients duringfollow-up, the sample size is much larger.
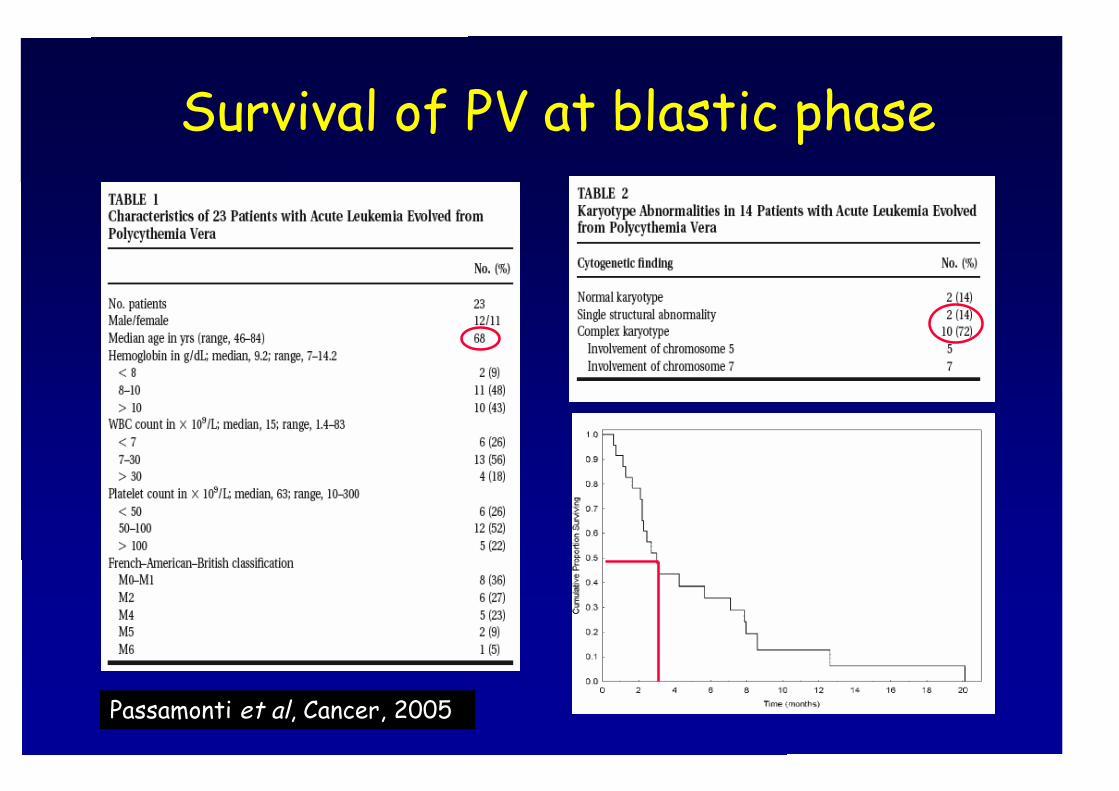
Survival of PV at blastic phase
Passamonti et al, Cancer, 2005
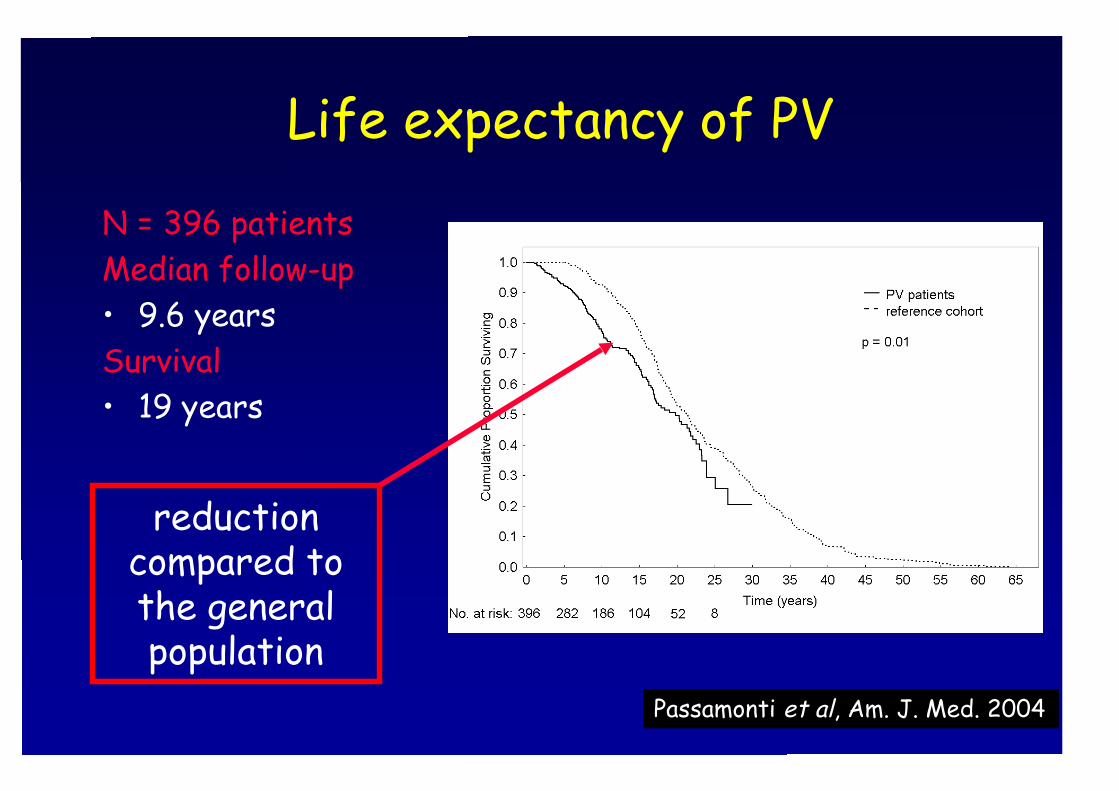
Life expectancy of PV
N = 396 patientsMedian follow-up• 9.6 yearsSurvival• 19 years
Passamonti et al, Am. J. Med. 2004
reductioncompared tothe generalpopulation
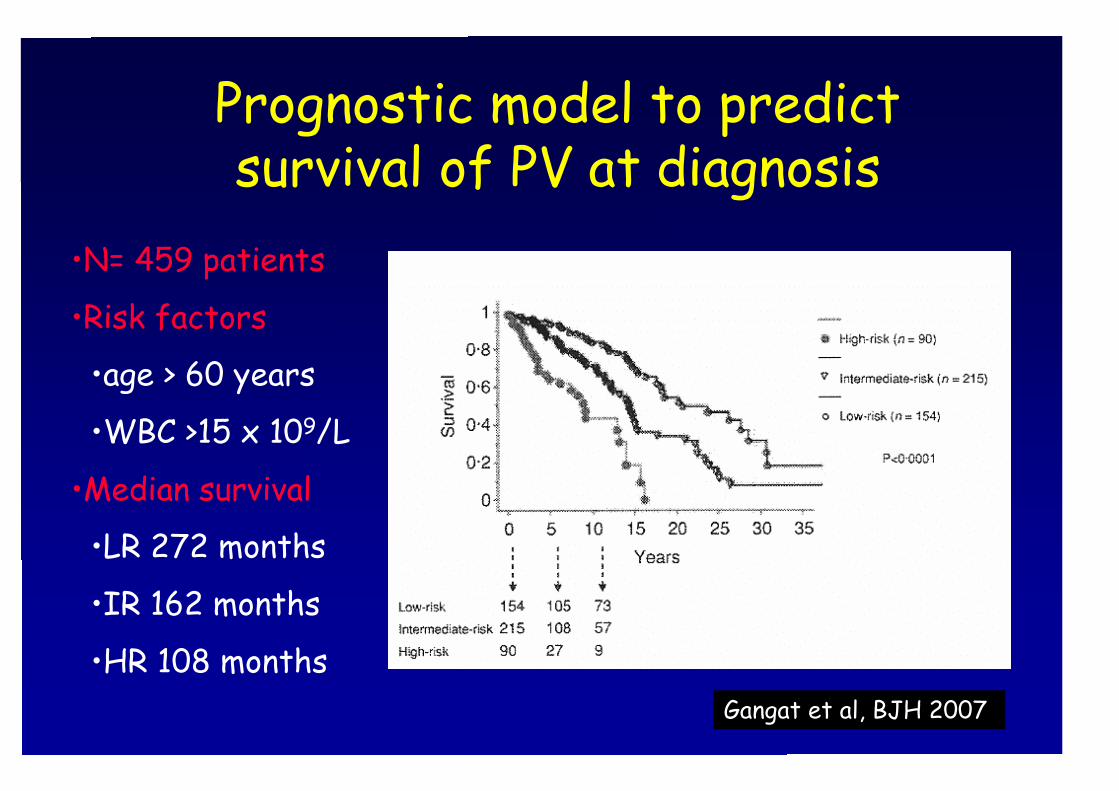
Prognostic model to predictsurvival of PV at diagnosis
Gangat et al, BJH 2007
•N= 459 patients
•Risk factors
•age > 60 years
•WBC >15 x 109/L
•Median survival
•LR 272 months
•IR 162 months
•HR 108 months
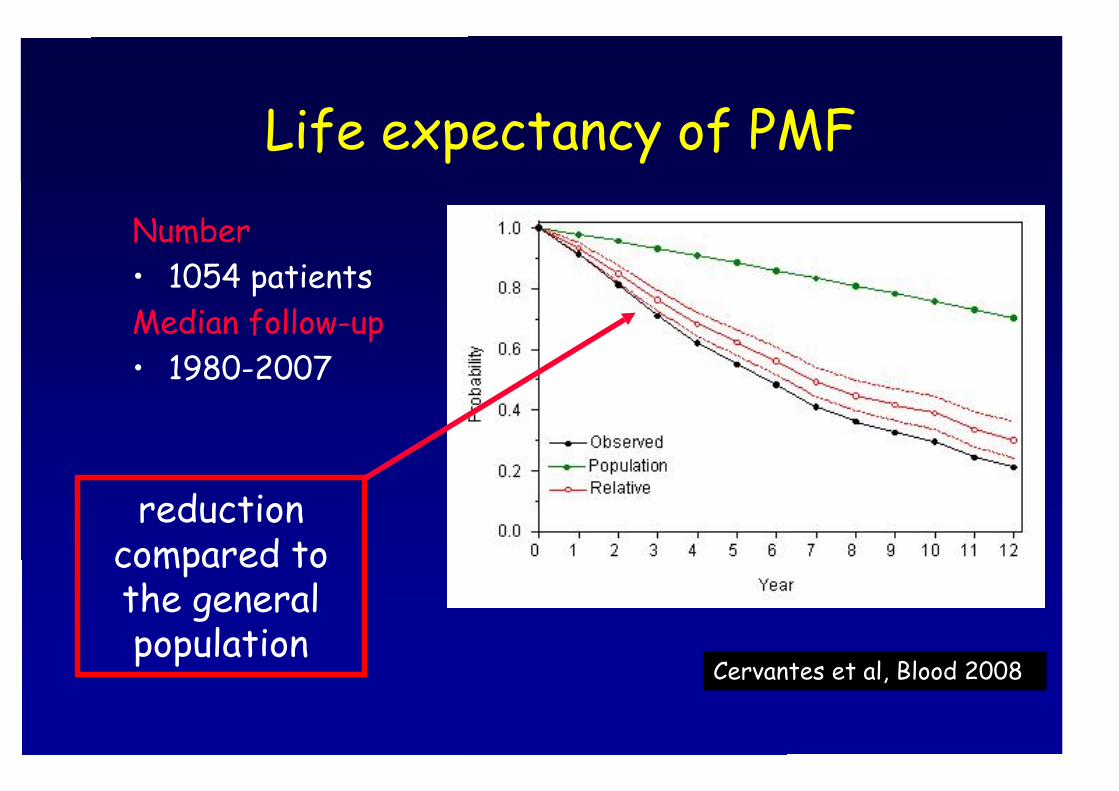
Life expectancy of PMF
Number• 1054 patientsMedian follow-up• 1980-2007
Cervantes et al, Blood 2008
reductioncompared tothe generalpopulation
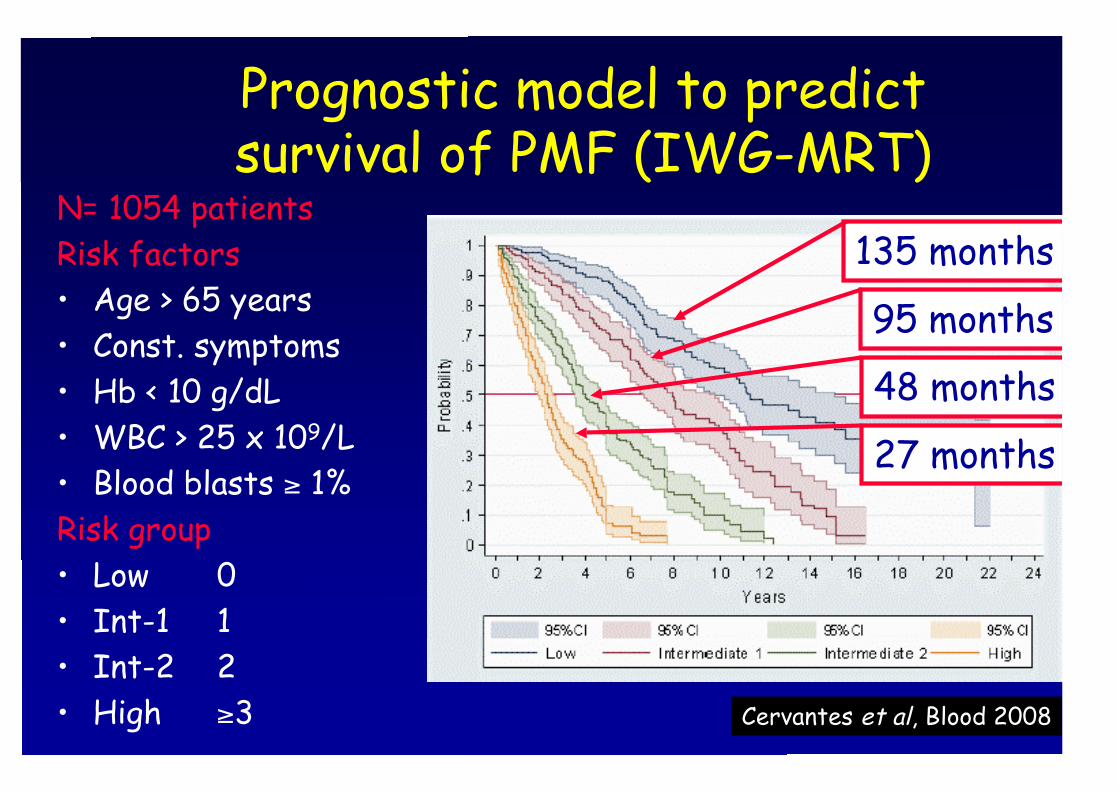
Prognostic model to predictsurvival of PMF (IWG-MRT)
Cervantes et al, Blood 2008
N= 1054 patientsRisk factors• Age > 65 years• Const. symptoms• Hb < 10 g/dL• WBC > 25 x 109/L• Blood blasts ≥ 1%Risk group• Low 0• Int-1 1• Int-2 2• High ≥3
135 months
95 months
48 months
27 months
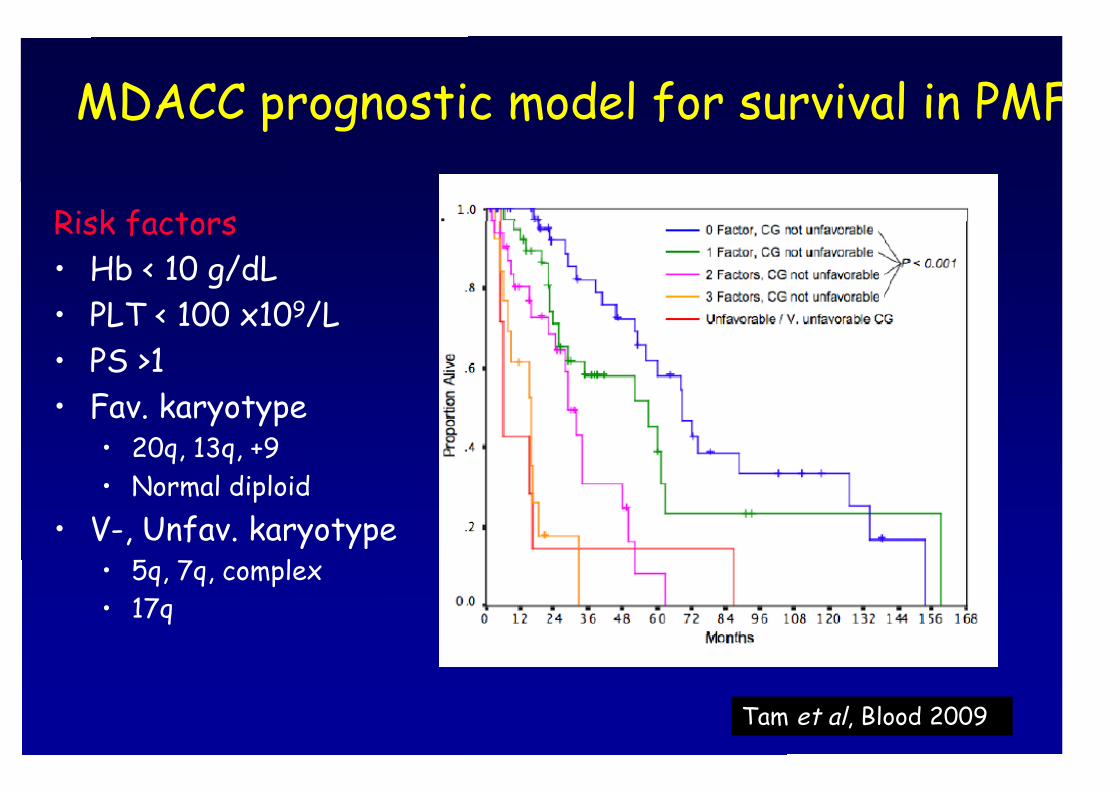
Risk factors• Hb < 10 g/dL• PLT < 100 x109/L• PS >1• Fav. karyotype
• 20q, 13q, +9• Normal diploid
• V-, Unfav. karyotype• 5q, 7q, complex• 17q
MDACC prognostic model for survival in PMF
Tam et al, Blood 2009
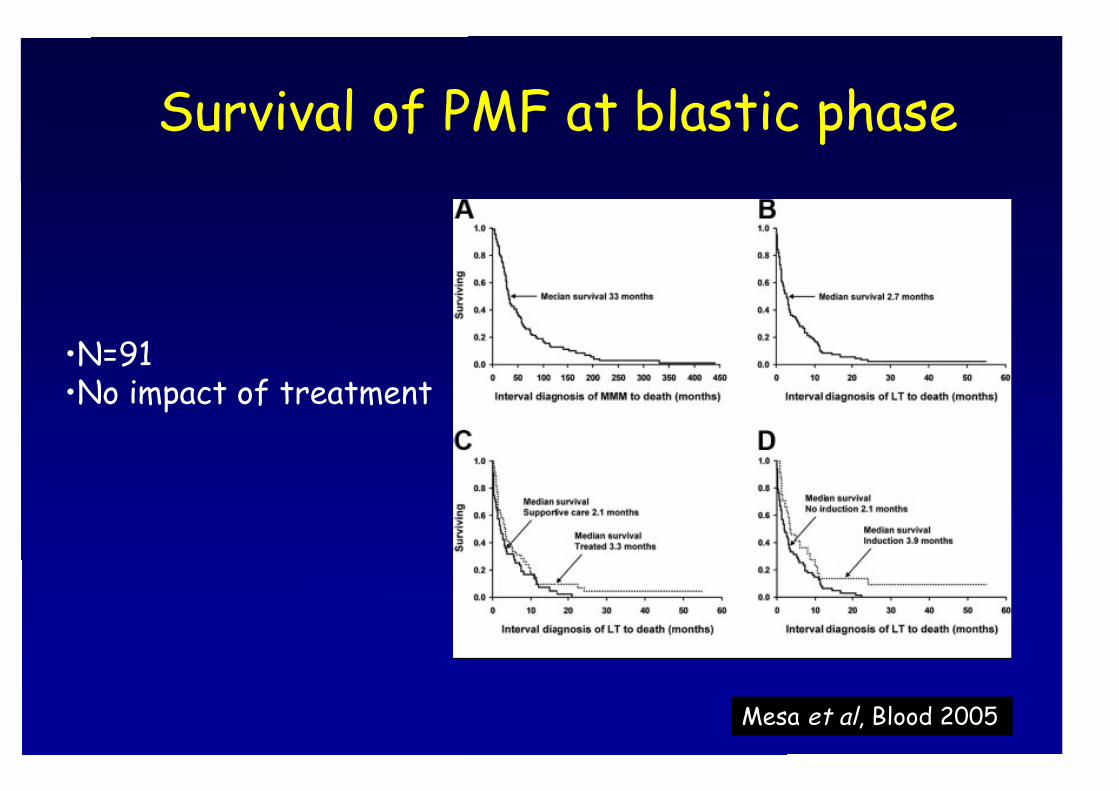
Survival of PMF at blastic phase
Mesa et al, Blood 2005
•N=91•No impact of treatment
Is JAK2 (V617) a risk factorfor disease evolution in MPN?
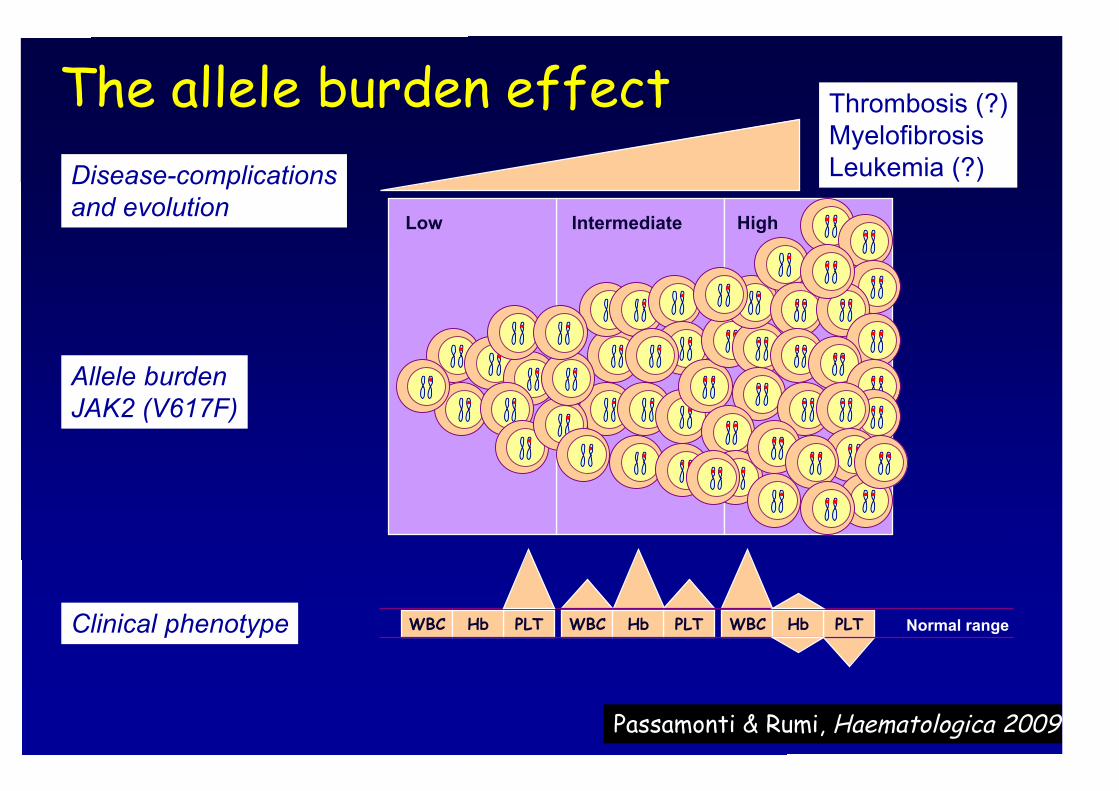
Thrombosis (?)MyelofibrosisLeukemia (?)
Clinical phenotype
Disease-complicationsand evolution
Allele burdenJAK2 (V617F)
IntermediateLow High
PLTWBC Hb PLTWBC Hb PLTWBC Hb Normal range
The allele burden effect
PassamontiPassamonti & Rumi,& Rumi, HaematologicaHaematologica 2009 2009
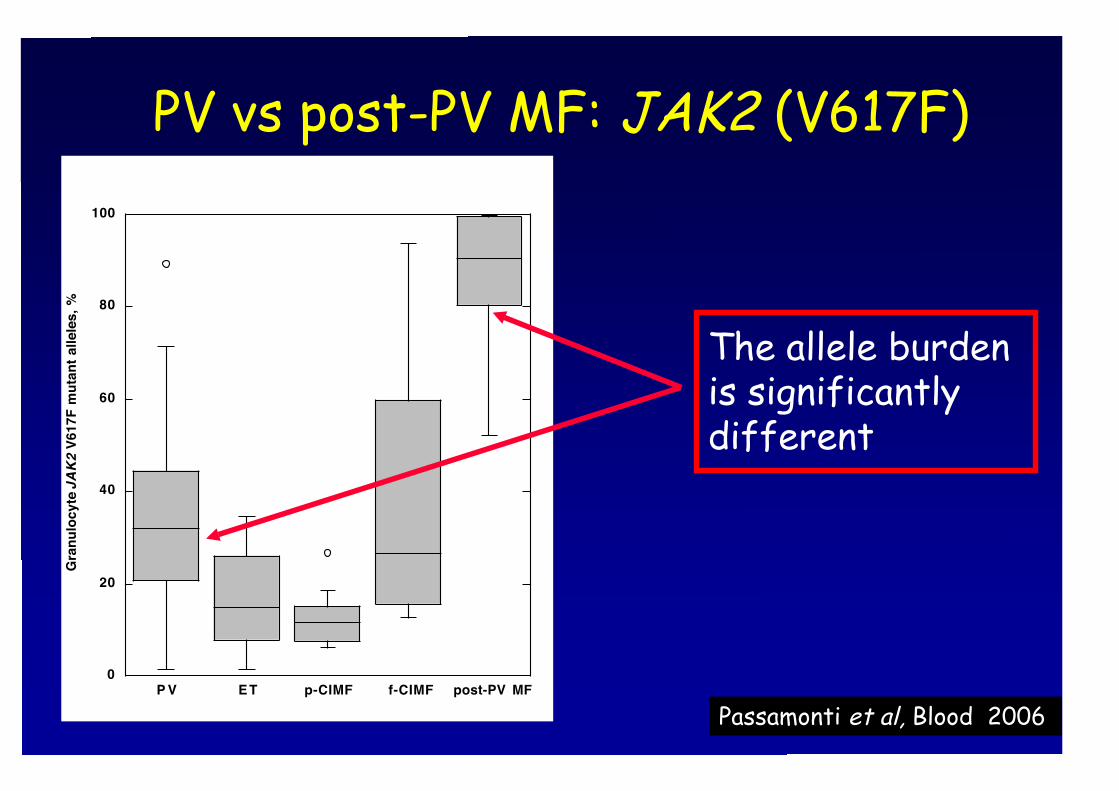
PV vs post-PV MF: JAK2 (V617F)
0
20
40
60
80
100
P V ET p-CIMF f-CIMF post-PV MF
Gra
nu
loc
yte
JAK2 V
61
7F
mu
tan
t a
lle
les
, %
PassamontiPassamonti et al, et al, Blood 2006
The allele burdenis significantlydifferent
Disease evolution in PV and ET(GIMEMA-MPD WP)
•Post-PV MF occurred more frequentlyamong homozygous (11.5%) thanheterozygous (1.4%) PV patients.
•Post-ET MF occurred more frequentlyamong homozygous (14.3%) thanheterozygous (4.7%) and WT (1.6%) ETpatients.
VannucchiVannucchi et al, et al, Blood 2007
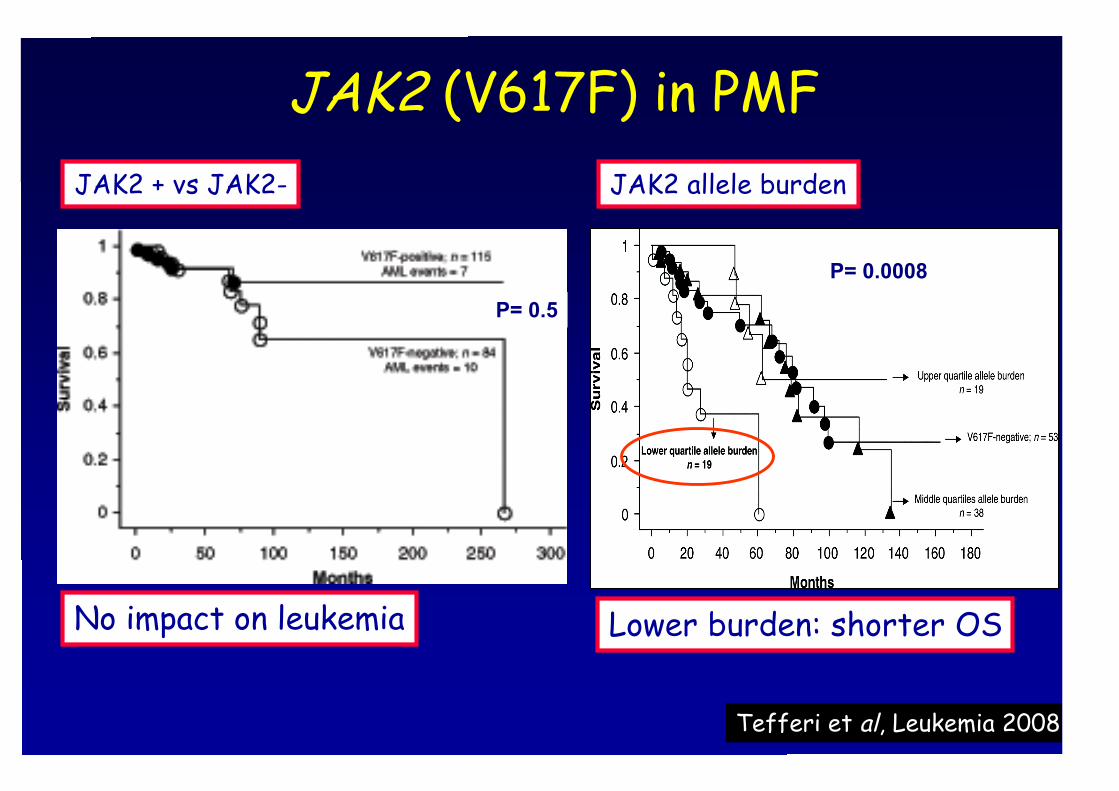
JAK2 (V617F) in PMF
P= 0.0008
No impact on leukemia
P= 0.5
Lower burden: shorter OS
JAK2 + vs JAK2- JAK2 allele burden
Tefferi et al, Leukemia 2008

• Age > 60 years• Thrombosis/hemorrage• PLT count > 1500 x 109/L
Caveat if:• Leukocytosis• JAK2 (V617F) burden
Patients with PV and ET at diagnosis
Post-PV MF Post-ET MF AL
• Hb < 10 g/dL• PLT < 100 x 109/L• WBC > 30 x 109/L
• PMF-like score • Candidatefor BMT
Monitor: CBC count, blood smear, spleen size, serum LDH, circulating CD34+
• Cardiovascularfactors
• Age > 65 years• Const. symptoms• Hb < 10 g/dL• WBC > 25 x 109/L• Blood blasts ≥ 1%
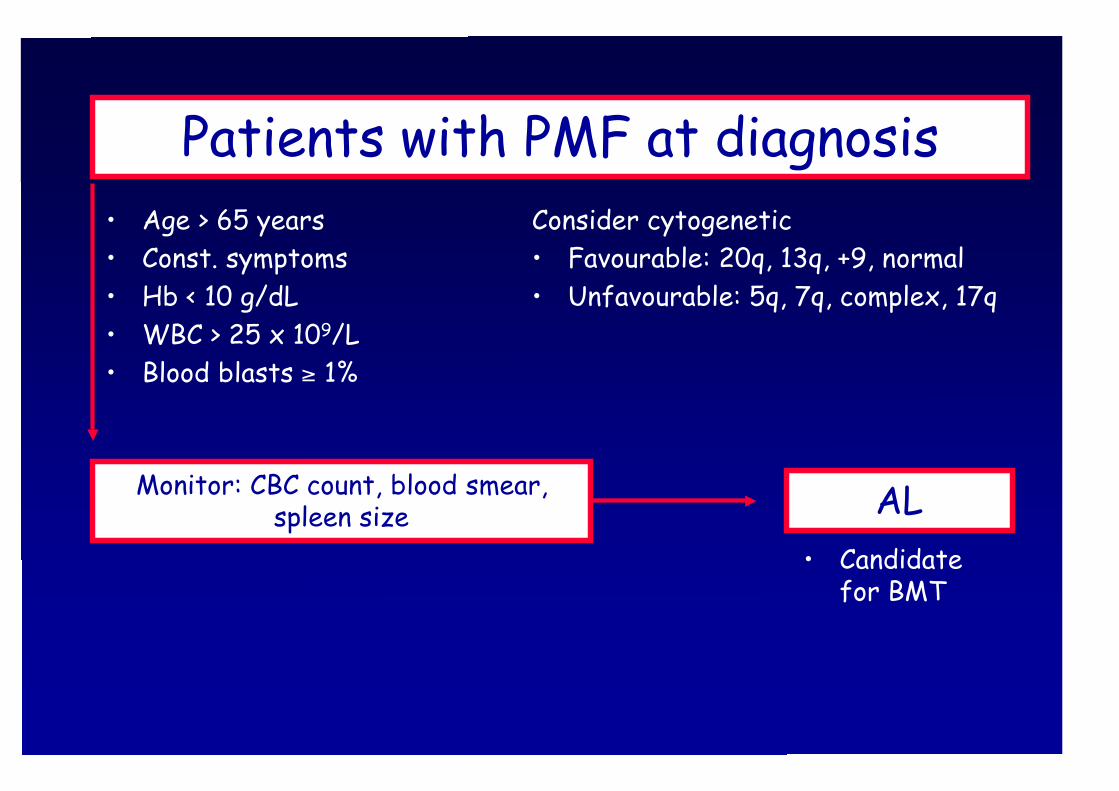
Patients with PMF at diagnosis
AL• Candidate
for BMT
Monitor: CBC count, blood smear,spleen size
Consider cytogenetic• Favourable: 20q, 13q, +9, normal• Unfavourable: 5q, 7q, complex, 17q