Alarm for the Treatment of Enuresis: Review of Treatment ... · Nocturnal enuresis, or involuntary...
3
Journal of Sleep Medicine & Disorders Cite this article: Teles A, Lordêlo P (2016) Alarm for the Treatment of Enuresis: Review of Treatment Types and Treatment Efficacy. J Sleep Med Disord 3(6): 1066. Central *Corresponding author Patrícia Lordêlo, Pelvic Floor Care Center, Bahiana School of Medicine and Public Health, Av. Dom João VI, nº 275, Brotas, Salvador, Bahia, Brazil, Tel: 557133301640; Fax: 5571; Email: Submitted: 05 August 2016 Accepted: 29 September 2016 Published: 01 October 2016 ISSN: 2379-0822 Copyright © 2016 Lordêlo et al. OPEN ACCESS Keywords • Enuresis • Alarm treatment • Children • Adolescents Review Article Alarm for the Treatment of Enuresis: Review of Treatment Types and Treatment Efficacy Alcina Teles 1 , and Patrícia Lordêlo 2 * 1 Pelvic Floor Care Center, Social Faculty of Bahia, Brazil 2 Pelvic Floor Care Center, Bahiana School of Medicine and Public Health, Brazil Abstract Nocturnal enuresis, or involuntary urination while asleep, can have a huge impact on the quality of life of children, teenagers and even young adults, also generating stress in households, and thus, has a negative impact on the lives of entire families. A number of treatment types are available; such as medication, bladder training, uro therapy, positive reinforcement, and the enuresis alarm, the latter presenting higher cure rates, lower rates of relapse in the long term, and therefore being considered a gold standard treatment for enuresis. But it is a treatment with conditions; it requires motivation, patience and persistence. The method does not always get the support of the family, leading to a relatively high drop-out rate. The first publication on the therapeutic technique with night alarms came out in the 30´s of the last century, and since then, many ways and various methods have been suggested and studied in the search for a good and inexpensive treatment. The objective of this study is to present the alarm types as described in publications and to discuss their effectiveness in the treatment of nocturnal enuresis. INTRODUCTION Enuresis is defined as intermittent incontinence during sleep in children over five years [1], and its importance stems not only for its high incidence, but mainly from its highly negative impact on the quality of life and that of the affected people and their families. It is more prevalent in boys, with a ratio of three boys for every girl until the age of 15 [2]. Approximately 15% of children at the age of five have enuresis. Spontaneous resolution occurs in 15% of all cases per year, and this applies to children of all ages [3]. Nevertheless, up to 2% of young adults currently still have to deal with enuresis [4]. Despite being a discomfort that does not bring risks to physical health, enuresis leaves its traces on a social and emotional level, and leads to stress and inconvenient situations in the lives of the affected and their families [5]. The affected children and adolescents could experience the disapproval of parents and the provocation of siblings, which affects their relationship with their family, where recurring treatment failures could lead to low self-esteem [6]. All of this could bring social isolation, with the negative impact becoming more significant from the age of seven [7]. Bedwetting has a multifactorial etiology; from the difficulty in waking up when the bladder is filled; to excessive nocturnal urine production and nocturnal bladder hyperactivity. Besides these main causes, the genetic influence cannot be denied [8-10]. The lack of a clear etiological factor makes it difficult to find the right therapeutic treatment for these patients. It leads to a constant search for effective, low cost solutions with minimal risk to health. The treatment of enuresis is based on medical and behavioural treatment and should be started from the age of 6 [11] in children with at least one episode of enuresis per week [12]. The night alarm behavioural treatment is considered the gold standard for enuresis, with the highest cure rate in the long run [12]. The objective of this study is to present the alarm types as described in publications and to discuss their effectiveness. The Alarm The night alarm resulted in cure rates for enuresis of two- thirds, with Evidence level Ia, and relative risk of failure of 38% [13]. The device attempts to wake the child when the bladder is full. The treatment is based on the behavioural therapy technique [14]. The device consists of a moisture sensor connected to a sound system (possibly combined with other stimulus) that emits an alarm after the urine has been detected by the sensor [14]. Thus, in theory, the child would wake up and finish urinating in the toilet and begins to develop the awareness of a full bladder during sleep, thus preventing episodes of enuresis.
Transcript of Alarm for the Treatment of Enuresis: Review of Treatment ... · Nocturnal enuresis, or involuntary...

Journal of Sleep Medicine & Disorders
Cite this article: Teles A, Lordêlo P (2016) Alarm for the Treatment of Enuresis: Review of Treatment Types and Treatment Efficacy. J Sleep Med Disord 3(6): 1066.
Central
*Corresponding authorPatrícia Lordêlo, Pelvic Floor Care Center, Bahiana School of Medicine and Public Health, Av. Dom João VI, nº 275, Brotas, Salvador, Bahia, Brazil, Tel: 557133301640; Fax: 5571; Email:
Submitted: 05 August 2016
Accepted: 29 September 2016
Published: 01 October 2016
ISSN: 2379-0822
Copyright© 2016 Lordêlo et al.
OPEN ACCESS
Keywords•Enuresis•Alarm treatment•Children•Adolescents
Review Article
Alarm for the Treatment of Enuresis: Review of Treatment Types and Treatment EfficacyAlcina Teles1, and Patrícia Lordêlo2*1Pelvic Floor Care Center, Social Faculty of Bahia, Brazil2Pelvic Floor Care Center, Bahiana School of Medicine and Public Health, Brazil
Abstract
Nocturnal enuresis, or involuntary urination while asleep, can have a huge impact on the quality of life of children, teenagers and even young adults, also generating stress in households, and thus, has a negative impact on the lives of entire families. A number of treatment types are available; such as medication, bladder training, uro therapy, positive reinforcement, and the enuresis alarm, the latter presenting higher cure rates, lower rates of relapse in the long term, and therefore being considered a gold standard treatment for enuresis. But it is a treatment with conditions; it requires motivation, patience and persistence. The method does not always get the support of the family, leading to a relatively high drop-out rate. The first publication on the therapeutic technique with night alarms came out in the 30´s of the last century, and since then, many ways and various methods have been suggested and studied in the search for a good and inexpensive treatment. The objective of this study is to present the alarm types as described in publications and to discuss their effectiveness in the treatment of nocturnal enuresis.
INTRODUCTIONEnuresis is defined as intermittent incontinence during sleep
in children over five years [1], and its importance stems not only for its high incidence, but mainly from its highly negative impact on the quality of life and that of the affected people and their families.
It is more prevalent in boys, with a ratio of three boys for every girl until the age of 15 [2]. Approximately 15% of children at the age of five have enuresis. Spontaneous resolution occurs in 15% of all cases per year, and this applies to children of all ages [3]. Nevertheless, up to 2% of young adults currently still have to deal with enuresis [4].
Despite being a discomfort that does not bring risks to physical health, enuresis leaves its traces on a social and emotional level, and leads to stress and inconvenient situations in the lives of the affected and their families [5].
The affected children and adolescents could experience the disapproval of parents and the provocation of siblings, which affects their relationship with their family, where recurring treatment failures could lead to low self-esteem [6]. All of this could bring social isolation, with the negative impact becoming more significant from the age of seven [7].
Bedwetting has a multifactorial etiology; from the difficulty in waking up when the bladder is filled; to excessive nocturnal urine production and nocturnal bladder hyperactivity. Besides
these main causes, the genetic influence cannot be denied [8-10].
The lack of a clear etiological factor makes it difficult to find the right therapeutic treatment for these patients. It leads to a constant search for effective, low cost solutions with minimal risk to health.
The treatment of enuresis is based on medical and behavioural treatment and should be started from the age of 6 [11] in children with at least one episode of enuresis per week [12]. The night alarm behavioural treatment is considered the gold standard for enuresis, with the highest cure rate in the long run [12]. The objective of this study is to present the alarm types as described in publications and to discuss their effectiveness.
The AlarmThe night alarm resulted in cure rates for enuresis of two-
thirds, with Evidence level Ia, and relative risk of failure of 38% [13]. The device attempts to wake the child when the bladder is full. The treatment is based on the behavioural therapy technique [14].
The device consists of a moisture sensor connected to a sound system (possibly combined with other stimulus) that emits an alarm after the urine has been detected by the sensor [14].
Thus, in theory, the child would wake up and finish urinating in the toilet and begins to develop the awareness of a full bladder during sleep, thus preventing episodes of enuresis.

Lordêlo et al. (2016)Email:
J Sleep Med Disord 3(6): 1066 (2016) 2/3
Central
Like a first-line treatment, it should be given to all children. But the approach comes with some conditions, and it is extremely important that parents are motivated, as it will be necessary to be persistent and to treat the children involved with care and proper intention. Especially because of the expected reoccurrence of episodes of enuresis; they need to show a lot of support and tolerance to them [11]. Raising children with enuresis can be more difficult for some [10], because of the need to bring the children to the bathroom once the alarm is activated [14] and all this time the child can still persists presenting episodes of bedwetting [15].
The above can cause tension in the family environment, with possible reduction of work capacity of those responsible for the child because of the stress at night [16].Because of these issues, the bedwetting alarm withdrawal rate can range from 10% to 30% [13] and therefore a large number of different studies exist, describing different types of alarm, in an attempt to minimize these difficulties.
In the literature we already find projects that are aimed at a remote, individualized care of patients. These projects are based on the use of devices that provide reminders to patients with guidelines and advice that should be followed. The devices offer an individual program, according to the particular case of a patient and are set up for patients with chronic diseases and a long term treatment process. The use of these devices seems to come with an improved patient compliance and self-care, an improved support from the family during the treatment and an improved relationship with the health service during treatment [17]. As the standard treatment of enuresis is long term as well, such devices could be incorporated to enuresis therapy and potentially improve results. To the best of our knowledge, there have been no studies evaluating the impact of this technology in enuresis patients.
Alarm TypesFour types of nocturnal alarms were found in studies: the
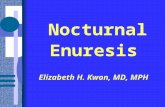
sound [13, 18], the vibration [19], which combines an electrical impulse with a sound [20-23] and code words [24]. The most commonly used alarm is the one that produces a sound, a device that has been tested with different volumes, with or without associated light, waking the child immediately or with a delay of three minutes, putting the humidity sensor on the bed or in the child’s underwear and currently alarming the children or only the parents [13]. Figure (1) presents three alarm types for enuresis.
The vibrating alarm was tested in a study and consisted of a small device that was set in the inner child clothing tab, getting in direct contact with the skin, used by both boys and girls.
The humidity sensor was positioned close to the urethra, and when the child urinated, instead of sounding the alarm, intermittent vibrations were activated in the child’s skin in an attempt to wake them. Children reported more discomfort with the use of this alarm than by the use of a buzzer [19].As for the alarm associated with electrical stimulation, there are two different approaches. The oldest, in studies published between1950 and1980, was electrical stimulation in the suprapubic region of both sexes, besides the thigh region of the boys [20], in the chest or lateral abdominal region [21,22].
In one study, special underwear was developed [20], which contained both the moisture sensor and the electrodes for electrical stimulation for when the child began to urinate.
In these studies unacceptable side effects were described; such as fear, burns and other skin lesions, which made these alarms fall into disuse by low acceptance of users and their caregivers. The electric current used in these studies was monophasic, with a higher risk of skin lesions.
More recently, our group published a different alarm mode associated with electrical stimulation. In this case, the child used a pair of self-adhesive electrodes in the perianal region with a humidity sensor inside the underwear. When the urination started, electrical stimulation triggered a contraction of the pelvic floor muscles in order to stop the urination, and 20 seconds later, the alarm sounded to try to wake the child and to check whether he or she had reacted on the muscle stimulation in the right way [23]. In this pilot study, adverse or side effects have not been described, probably because of the use of biphasic current, already widely studied and used in clinical practice for muscle functional electrical stimulation [23].
A more recent alarm system was suggested and described by the University of Sydney, Australia. The technique is based on the association of the buzzer with code words, recorded by parents on the device. In this case, children are rewarded when they remember the word that was recorded by the device (with the voice of the parents) the night before, instead of being rewarded for having a night without the episode of bedwetting. The theoretical rationale of these authors is that motivation is an important factor during the awakening process of individuals, and by using a codeword at night decreases the threshold to raise these children, by activating them in a playful way, by a game [24].
DISCUSSION & CONCLUSIONAlthough it is regarded and recommended as the first
treatment option, and its use for many years already, the alarm is
Figure 1 (A) –[Alarm with electrical muscle stimulation], (B) –[Wireless sound alarm with sensor in underwear] , (C) –[Wired sound alarm].

Lordêlo et al. (2016)Email:
J Sleep Med Disord 3(6): 1066 (2016) 3/3
Central
not regarded as the optimal resolution of the problem, because of the numerous factors that may hinder the time of the therapeutic response. There are reports of technical problems with the alarm, with perspiration of the child; or the battery does not have adequate durability. Some devices only provide a moisture sensor, causing problems when trying to use the alarm again after an episode of enuresis. Another factor is the type of fabric used for the moisture sensor, entailing larger or smaller absorption rates [23, 25], and the technical quality of the alarm also being an important factor in therapeutic efficacy.
To conclude, in the overall assessment, there is no important difference between the types of alarm in terms of efficacy [13]. The most recent studies, with innovative solutions such as the electrical stimulation as described in the pilot study [23], seem to have the potential to bring a faster response to adolescents with enuresis. And the alarm with code words [24], although improving the awakening process in the ones with enuresis studied, brings no significant difference in therapeutic efficacy.
In general, after many tests with various forms of alarm devices (sound with all its variations, vibrating with electro stimulation and code words), there is still no consensus on the optimal volume of the sound. At present, the most widespread type of alarm is sounding immediately, when the humidity sensor (placed in the underwear) is activated. All this in an attempt to wake the child timely, enabling he continuation of urinating on the toilet, or to inhibit bladder contraction and to continue to sleep without urinating.
REFERENCES1. Austin PF, Bauer SB, Bower W, Chase J, Franco I, Hoebeke P, et al. The
Standardization of Terminology of Lower Urinary Tract Function in Children and Adolescents: Update Report From the Standardization Committee of the International Children’s Continence Society. Neurourol Urodyn. 2016; 35: 471-81.
2. Thiedke CC. Nocturnal Enuresis. American Family Physician. 2003; 67: 1499-1506.
3. Forsythe WI, Butler RJ. Fifty years of enuretic alarms. Arch Dis Child. 1989; 64: 879-885.
4. Rogers J. An overview of the management of nocturnal enuresis in children. Br J Nurs. 2003;12: 898-903.
5. Fitzwater D, MackninML. Risk/benefit ratio in enuresis therapy. ClinPediatr (Phila).1992; 31: 308-310
6. Nevéus T, Von Gontard A, Hoebeke P, Hjälmås K, Bauer S, Bower, et al. The Standardization of Terminology of Lower Urinary Tract Function in Children and Adolescents: Report from the Standardization Committee of the International Children’s Continence Society. J Urol. 2006;176: 314-24.
7. Arantes MC, Silvares EFM. A comparison between children and adolescents with primary nocturnal enuresis: impact and behavior problems. Estud. Psicol. 2007; 24: 155-160.
8. Yeung CK. Nocturnal enuresis. Curr Opin Urol. 2003;13: 337-343.
9. Nevéus T. Enuretic sleep: deep, disturbed or just wet? Pediatr Nephrol. 2008; 23:1201-1202.
10. Yeung CK, Diao M, Sreedhar B. Cortical arousal in children with severe enuresis. N Engl J Med. 2008; 358: 2414-2415.
11. Nevéus T, Eggert P, Evans J, Macedo A, Rittig S, Tekgül S et al. Evaluation of and Treatment for Monosymptomatic Enuresis: A Standardization Document From the International Children’s Continence Society. J. Urol. 2010; 183: 441-447.
12. Netley C, Khanna F, McKendry JB, Lovering JS. Effects of different methods of treatment of primary enuresis on psychologic functioning in children. Can Med Assoc J. 1984;131: 577-579.
13. Glazener Cathryn MA, Evans Jonathan HC, Peto Rachel E. Alarm interventions for nocturnal enuresis in children. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Cochrane Database Syst Rev Issue. 2005 ; 2 :CD002911.
14. Meneses R. Enurese noturna monossintomática. J. Pediatr. 2001; 77: 161-168.
15. Rogers J. An overview of the management of nocturnal enuresis in children. Br J Nurs. 2003;12: 898-903.
16. Kawauchi A, Naitoh Y, Yoneda K, Soh J, Seki H, Okihara K, et al. Refractory enuresis related to alarm therapy. J Pediatr Urol. 2006; 2: 579-582.
17. Ciccone MM, Aquilino A, Cortese F, Scicchitano P, Sassara M, Mola E, et. al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc Health Risk Manag. 2010; 6: 297-305.
18. Özgür B C, Özgür S, Doğan V, Örün UA. The efficacy of an enuresis alarm in monosymptomatic nocturnal enuresis. Singapore Med J. 2009; 50: 879-880.
19. Tobias NE, McCain GC. A comparison of two enuresis alarms. Urologic Nursing. 2001; 21: 349-53.
20.
21. Mc Kendry JB, Stewart DA, Khanna F, Netley C. Primary Enuresis: relative success of three methods of treatment. Can Med Assoc J. 1975; 113: 953-955.
22. Netley C, Khanna F, McKendry JB, Lovering JS. Effects of different methods of treatment of primary enuresis on psychologic functioning in children. Can Med Assoc J. 1984;131: 577-579.
23. Hojsgaard A, Genster H. Effect of Uristop in children with enuresis. A prospective randomized clinical trial. Ugeskr Laeger. 1979; 141: 647-648.
24. Barroso U, Lordêlo P, Teles A, Silveira DM, Renson C, Hoebeke P. New device and new concept for treating nocturnal enuresis: preliminar study of a phase one study. J Pediatr Urol. 2014;10:1273-1276.
25. Caldwell PHY, Sureshkumar P, Kerr MI, Hamilton S, Teixeira-Pinto A, Macaskill P,Craig JC. A randomised controlled trial of a code-word enuresis alarm. Arch Dis Child. 2016;101: 326–331.
26. Goel KM, Thomson RB, Gibb EM, Mc AinshTF. Evaluation of nine different types of enuresis alarms. Arch Dis Child. 1984; 59: 748-753.
Teles A, Lordêlo P (2016) Alarm for the Treatment of Enuresis: Review of Treatment Types and Treatment Efficacy. J Sleep Med Disord 3(6): 1066.
Cite this article