
Airway management
58
Dr. Mohamed Ibrahem El said Lecturer of Anesthesia Zagazig university
-
Upload
mohamed-ibrahem -
Category
Health & Medicine
-
view
47 -
download
0
Transcript of Airway management
Dr. Mohamed Ibrahem El saidLecturer of Anesthesia
Zagazig university
Breathing Systems delivery systems which conduct anesthetic gases from anesthesia machine to the patients. They include: Breathing tubes, Fresh gas inlets, Adjustable pressure-limiting [APL] valves reservoir bags) into the breathing circuit.
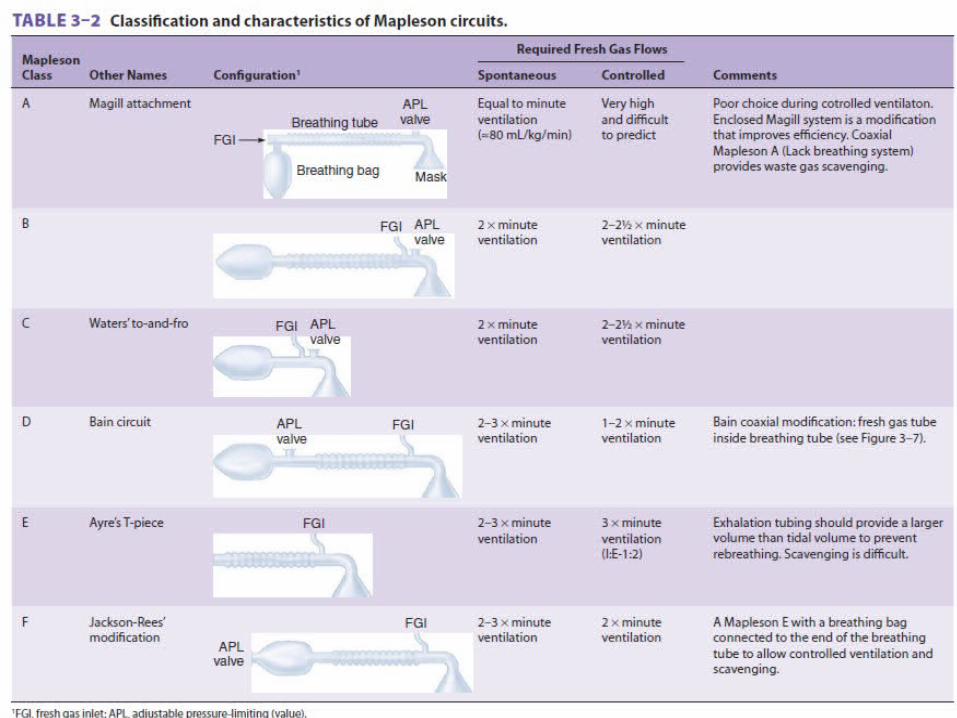
The relative location of these components determines circuit performance and is the basis of the Mapleson classification
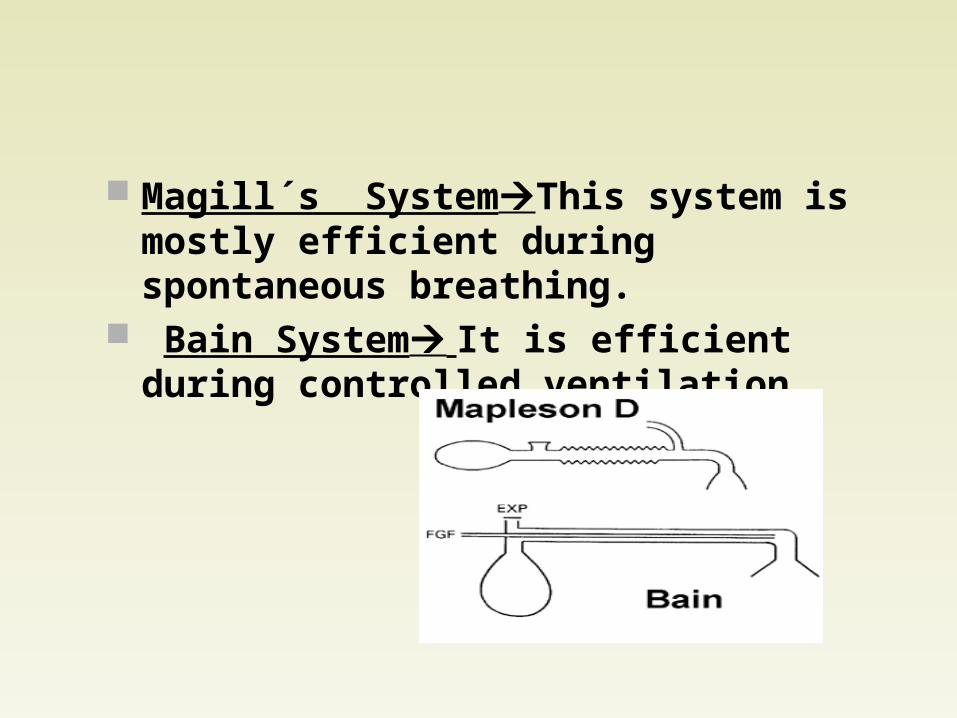
Magill´s SystemThis system is mostly efficient during spontaneous breathing.
Bain System It is efficient during controlled ventilation
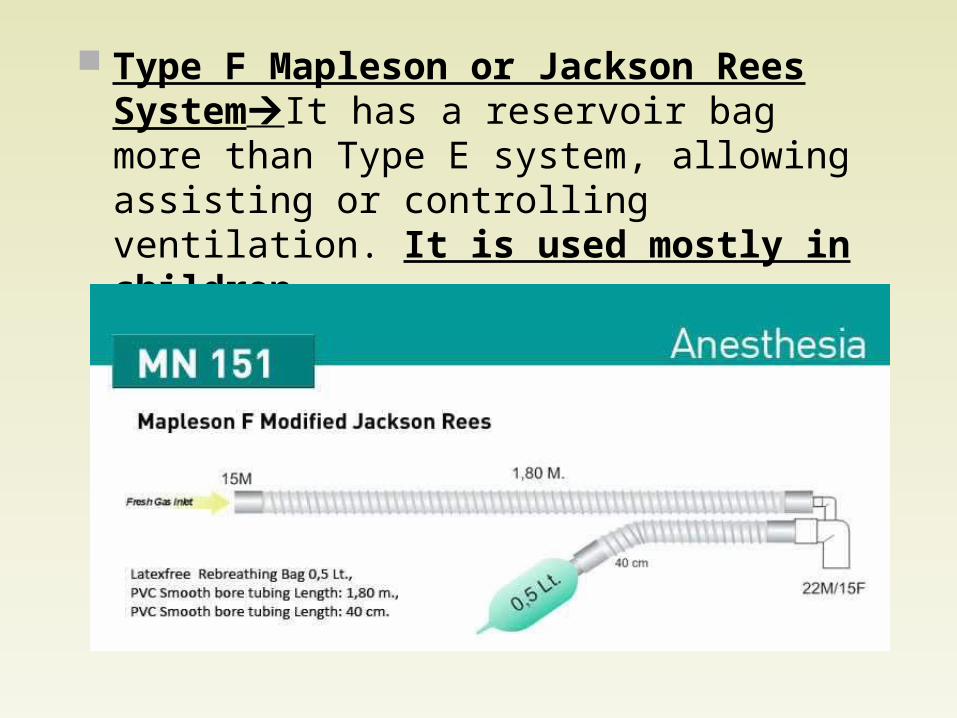
Type F Mapleson or Jackson Rees SystemIt has a reservoir bag more than Type E system, allowing assisting or controlling ventilation. It is used mostly in children.
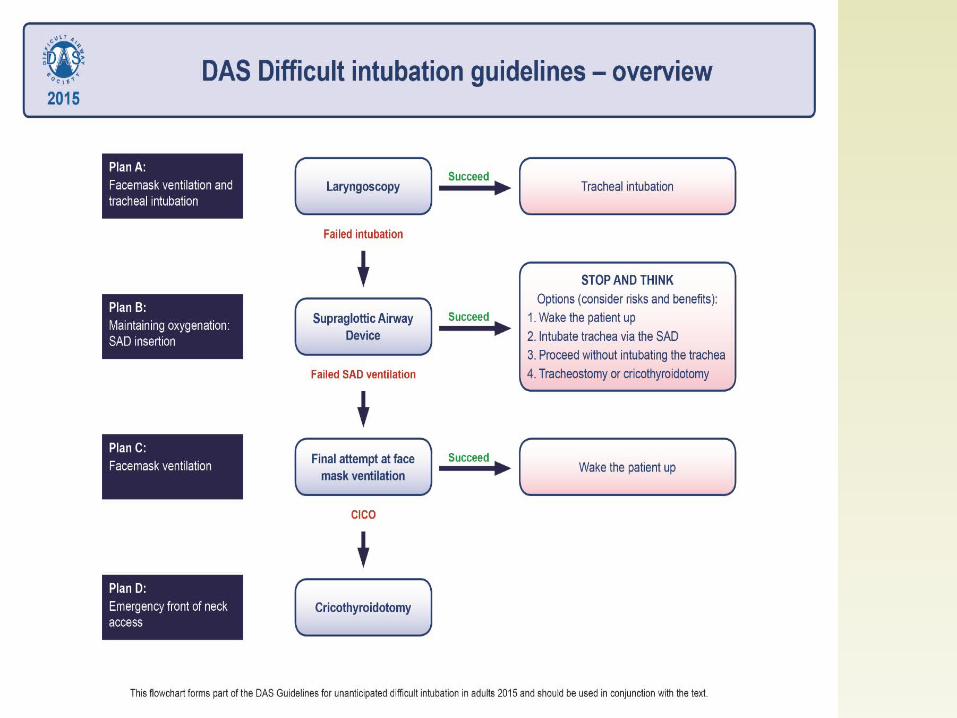
Difficult intubation Reported as up to 3% of airway Failed intubation in the OR 1 to 3 per 1000
patients Difficult airway :
A clinical situation in which a conventionally trained anesthesiologist experiences difficulty in mask ventilation, tracheal intubation or both
The American Society of Anesthesiologists Task Force on the Difficult Airway
Difficult mask ventilation incidence of difficult MV is approximately 1.4%, (ASA) defined difficult MV as a situation in which:It is
not possible for the anesthesiologist to provide adequate ventilation because of one or more of the following problems: inadequate mask seal, excessive gas leak, or excessive resistance to the ingress or egress of gas.
Factors affecting mask ventilationAnesthetic factors the experience of the clinician and the use of
equipment. The use of incorrectly sized oropharyngeal or
nasopharyngeal airways improperly sized mask being used or faults with the
anaesthetic machine or breathing circuit. inadequate depth of anaesthesia and inadequate
muscle relaxation may all lead to increased muscle rigidity, reduced chest wall compliance

Patient factors Physiological reactions Laryngospasm BronchospasmMMMMASK M Male gender M Mask seal M Mallampati 3 or 4 M Mandibular protrusion A Age > 55 S Snoring and obstructive
sleep apnoea K Kilograms (weight)
OBESE O Obese
(BMI>26kg/m2) B Bearded E Edentulous S Snoring E Elderly (>55 years)

Assessment of The Airway Taking an adequate history is necessary to
anticipate possible complicationsHistory should focus on:
Prior intubations Anesthetic history Drug allergies Confounding illnesses that may hinder airway
access A history of difficult intubation has the highest
positive and negative predictive value in predicting a difficult intubation.
Examination • Patency of nares: • Mouth opening of at least 2 large finger• Palate : A high arched palate or a long, narrow mouth• Protrude the lower jaw beyond the upper incisors (Prognathism).• Temporo-mandibular joint movement : It can be restricted
ankylosis/fibrosis, tumors, etc.• Measurement of submental space (thyromental length should
ideally be > 6 cm).• Patient’s neck : A short, thick neck is often associated with
difficult intubation. Any masses in neck, extension of neck, neck mobility and ability to assume ‘sniffing’ position should be observed.
Hoarse voice/stridor or previous tracheostomy may suggest stenosis.
Systemic or congenital disease Infections of airway (e.g. epiglottitis, abscess, croup,
bronchitis, pneumonia). Physiologic conditions: Pregnancy and obesity
=‘difficult-to mask ventilate OBES = Obese + Beard + Edentulous + Snoring
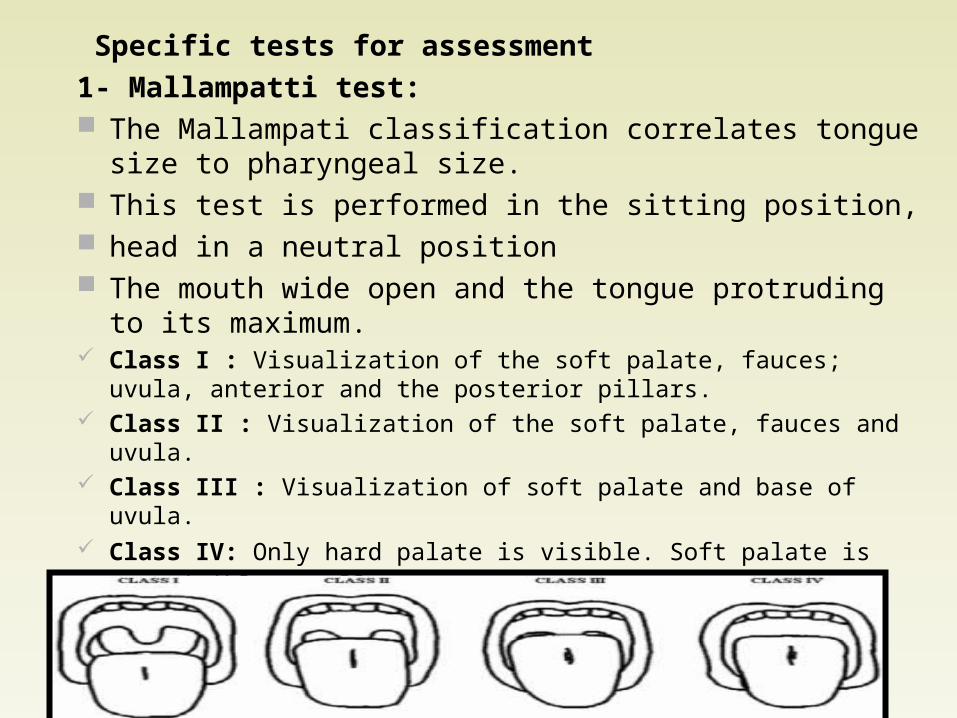
Specific tests for assessment1- Mallampatti test: The Mallampati classification correlates tongue size to
pharyngeal size. This test is performed in the sitting position, head in a neutral position The mouth wide open and the tongue protruding to its
maximum. Class I : Visualization of the soft palate, fauces; uvula, anterior and
the posterior pillars. Class II : Visualization of the soft palate, fauces and uvula. Class III : Visualization of soft palate and base of uvula. Class IV: Only hard palate is visible. Soft palate is not visible at all.

2. Atlanto occipital joint (AO) extension : It assesses feasibility to make sniffing position for
intubation i.e. alignment of oral, pharyngeal and laryngeal axes into an arbitrary straight line.
The patient is asked to hold head erect, facing directly to the front, extend the head maximally and the examiner estimates the angle traversed by the occlusal surface of upper teeth. Measurement can be by simple visual estimate or more accurately with a goniometer. Any reduction in extension is expressed in grades: Grade I : >35° Grade II : 22°-34° Grade III : 12°-21° Grade IV : < 12° Normal angle is 35° or more
3. Mandibular space Thyromental (T-M) distance (Patil’s test): mentum to the
thyroid notch with patient’s neck is fully extended. difficult if the T-M distance is < 3 finger breadths or < 6 cm in adults; 6-6.5 cm is less difficult, while > 6.5 cm is normal.
Sterno-mental distance: suprasternal notch to the mentum with head fully extended on the neck with the mouth closed. A value of less than 12 cm is found to predict a difficult intubation.
Mandibulo-hyoid distance: Measurement of mandibular length from chin (mental) to hyoid should be at least 4 cm or three finger breadths. It was found that laryngoscopy became more difficult as the vertical distance between the mandible and hyoid bone increased.


LEMON airway assessment method :L = Look externally (facial trauma, large incisors, beard or moustache, large tongue)E = Evaluate the 3-3-2 rule (incisor distance-3 finger breadths, hyoid-mental distance-3 finger breadths, thyroid-to-mouth distance-2 finger breadths)M = Mallampati (Mallampati score > 3).O = Obstruction (presence of any condition like epiglottitis, peritonsillar abscess, trauma).N = Neck mobility (limited neck mobility) Patients in the difficult intubation group have higher

Direct laryngoscopy and fibreoptic bronchoscopy Difficulty in intubation can be classified to 4 grades of
laryngoscopic views were defined by Cormack and Lehane
Grade I – Visualization of entire laryngeal aperture. Grade II – Visualization of only posterior commissure of
laryngeal aperture. Grade III – Visualization of only epiglottis. Grade IV – Visualization of just the soft palate. Grade III and IV predict difficult intubation.
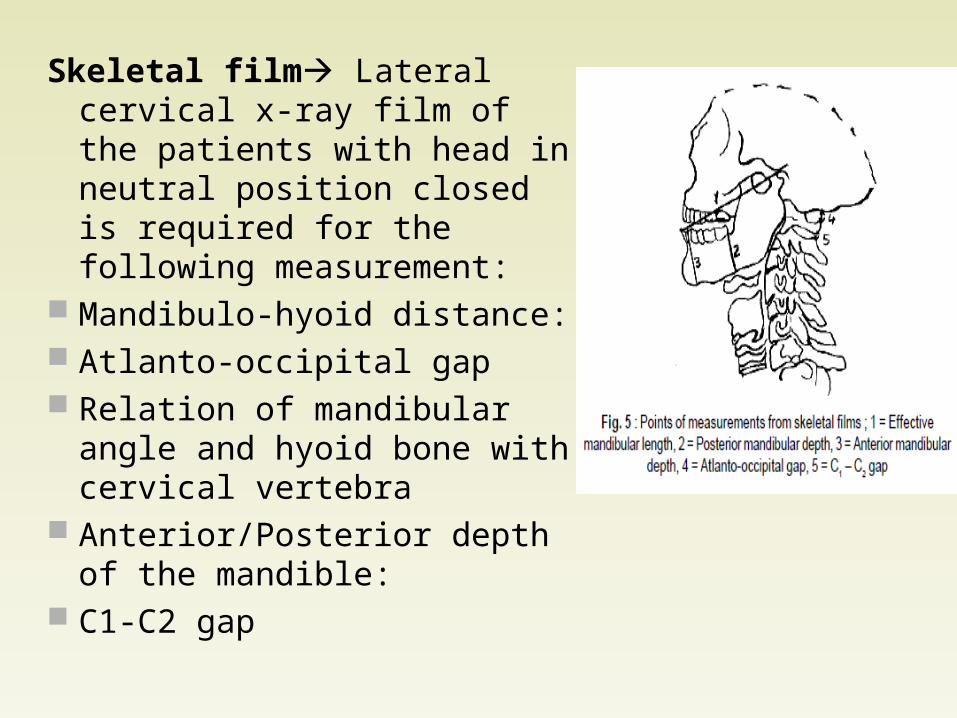
Skeletal film Lateral cervical x-ray film of the patients with head in neutral position closed is required for the following measurement:
Mandibulo-hyoid distance: Atlanto-occipital gap Relation of mandibular angle and
hyoid bone with cervical vertebra Anterior/Posterior depth of the
mandible: C1-C2 gap
Predictors of difficult airway in diabetics
Palm print: The patient is made to sit; palm and fingers of right hand are painted with blue ink, patient then presses the hand firmly against a white paper placed on a hard surface. It is categorized as:
Grade 0 – All the phalangeal areas are visible. Grade 1 – Deficiency in the interphalangeal
areas of the 4th and 5th digits. Grade 2 – Deficiency in interphalangeal areas of
2nd to 5th digits. Grade 3 – Only the tips of digits are seen.
Prayer sign: Patient is asked to bring both the palms together as ‘Namaste’ and sign is categorized as–Positive – When there is gap between palms.Negative – When there is no gap between palms
Assessment of pediatric airway Comprehensive history and physical examination. History: Questions regarding complaints of snoring, apnea, day time
somnolence, stridor, hoarse voice and prior surgery or radiation treatment to face or neck should be made.
This information may indicate hypoxemia and pulmonary hypertension.
History should also consist of a review of previous anesthetic records.
History of oropharyngeal injury, damage to teeth, awake tracheal intubation.
Postponement of surgery following an anesthetic. ildren.

Physical examination: It should focus on the anomalies of face, head, neck and spine.
Evaluate size and shape of head, gross features of the face; size and symmetry of the mandible, presence of sub-mandibular pathology, size of tongue, shape of palate, prominence of upper incisors, range of motion of jaw, head and neck.
The presence of retractions (suprasternal/sternal/ infrasternal/ intercostal) should be sought for they usually are signs of airway obstruction.
Breath sounds – Crowing Blood gas and O2 saturation ability to compensate
for airway problems.
Size of tongue relative to oral cavity and pharynx and laryngoscopy as determined by Cormack and Lehane.
Mallampati with poor view of glottis during direct laryngoscopy in pediatric patients due to lack of cooperation in infants and young children.
The mandibular space assessment is mainly suitable for older children Thus values for thyromental, hyomental and horizontal mandibular lengths do not exist for the pediatric population.
This places the pediatric anesthesiologist at a disadvantage and increases the likelihood of being confronted with an unexpected DA.





Equipment
Oral & Nasal Airways Face Mask Laryngeal Mask Combitube Tracheal Tube Laryngoscope Flexible Fiberopitc Bronchoscope
Oral & Nasal Airways
The most common cause of airway obstruction is the tongue
To overcome the obstruction: Head tilt Jaw thrust
To maintain the patency of the airway: Create airway passage by:
Oral airway Nasal airway
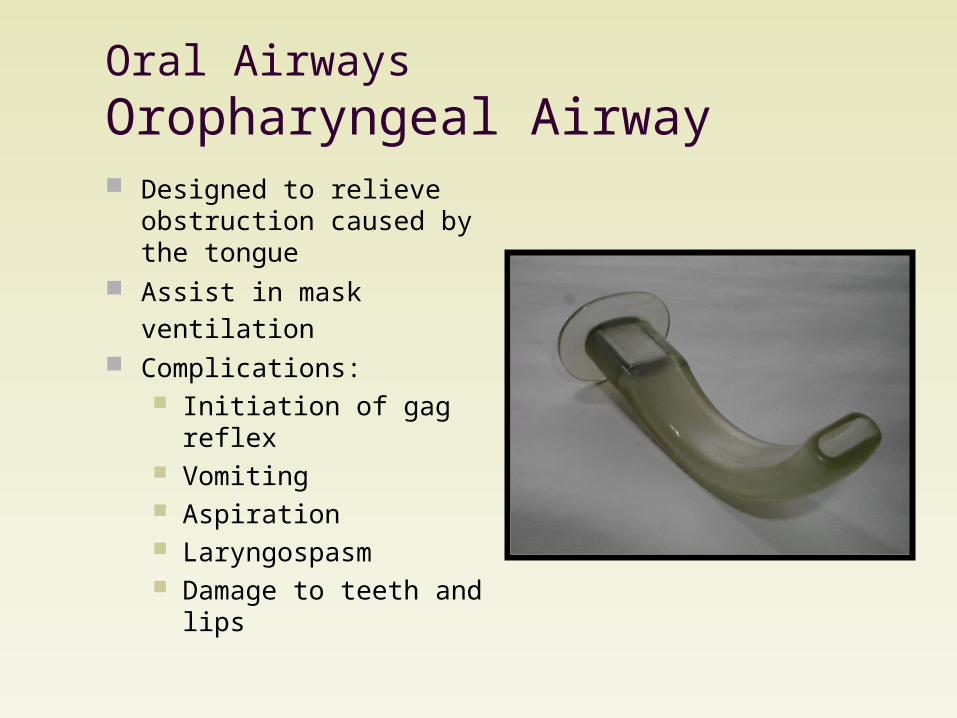
Oral AirwaysOropharyngeal Airway Designed to relieve
obstruction caused by the tongue
Assist in mask ventilation Complications:
Initiation of gag reflex Vomiting Aspiration Laryngospasm Damage to teeth and lips
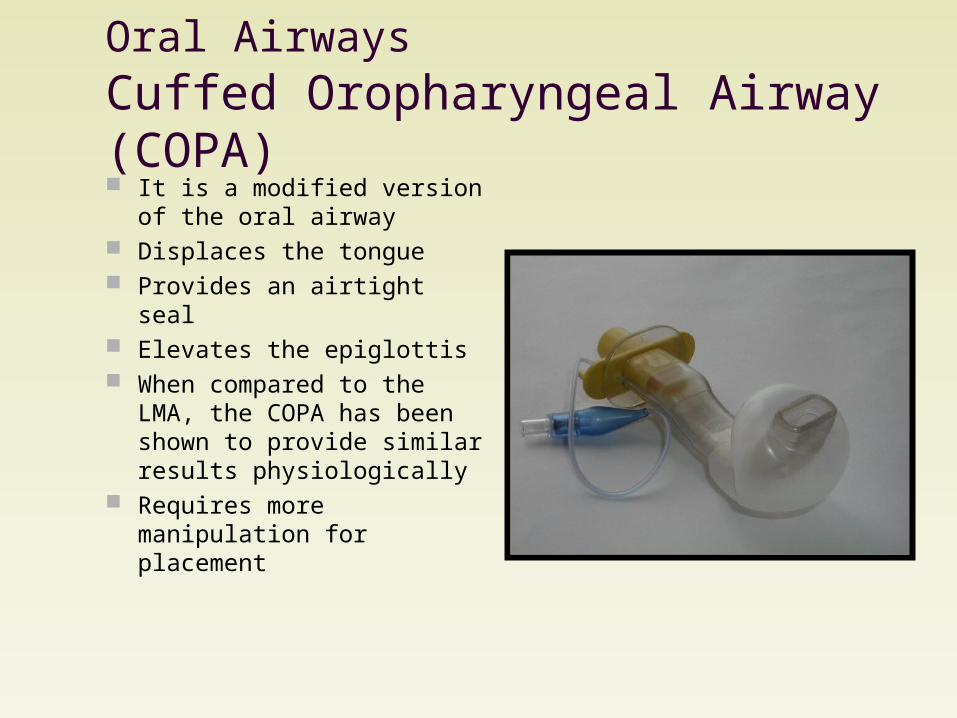
Oral Airways Cuffed Oropharyngeal Airway (COPA) It is a modified version of the
oral airway Displaces the tongue Provides an airtight seal Elevates the epiglottis When compared to the LMA,
the COPA has been shown to provide similar results physiologically
Requires more manipulation for placement
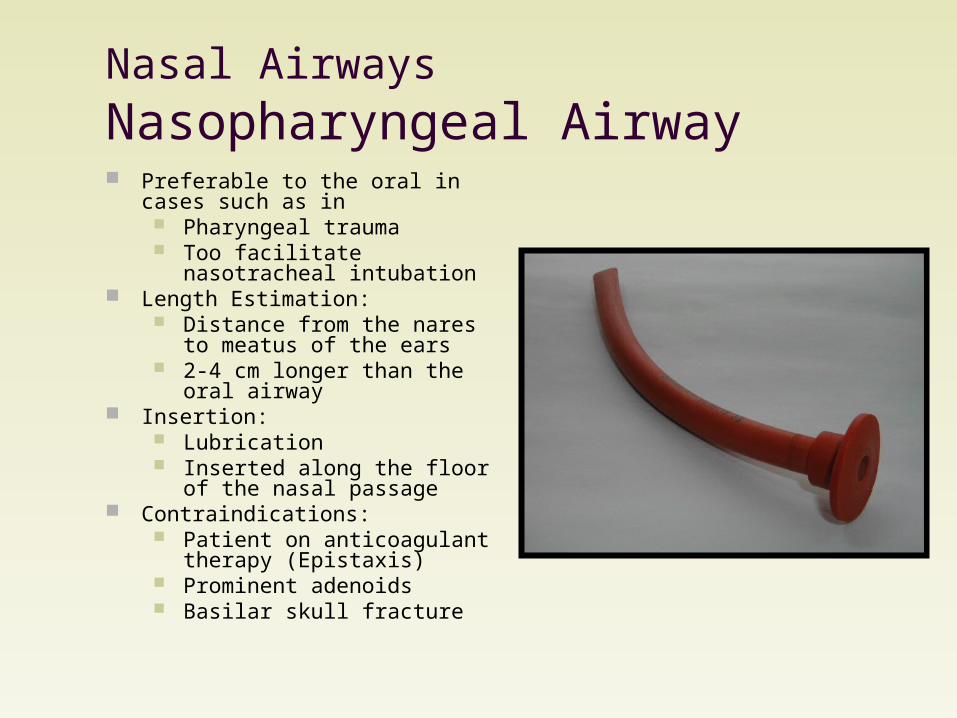
Nasal Airways Nasopharyngeal Airway Preferable to the oral in cases such as
in Pharyngeal trauma Too facilitate nasotracheal
intubation Length Estimation:
Distance from the nares to meatus of the ears
2-4 cm longer than the oral airway Insertion:
Lubrication Inserted along the floor of the
nasal passage Contraindications:
Patient on anticoagulant therapy (Epistaxis)
Prominent adenoids Basilar skull fracture
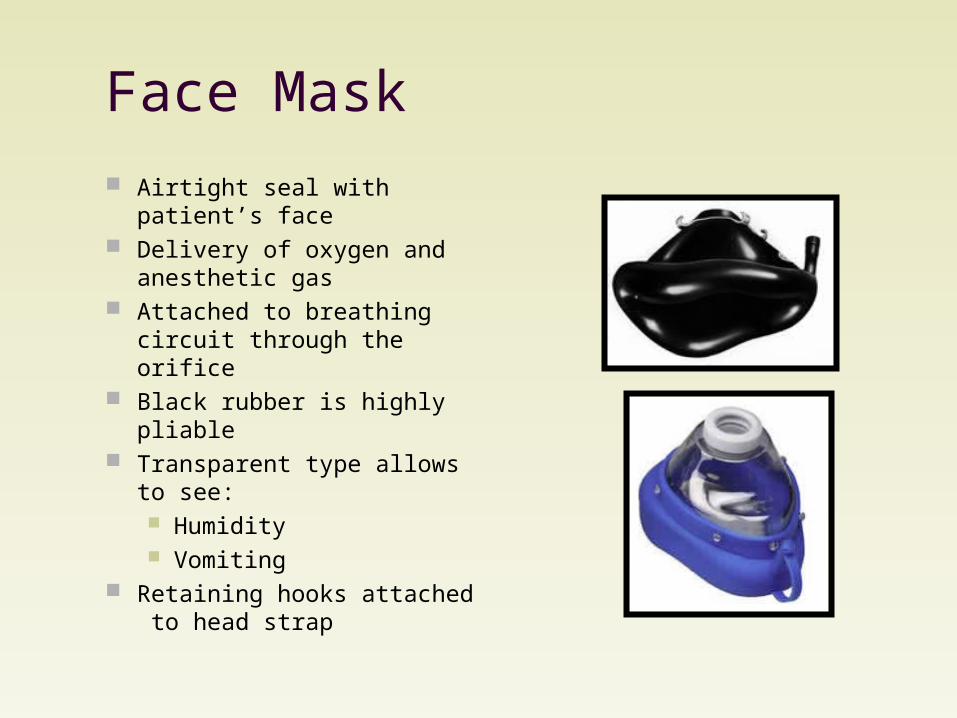
Face Mask Airtight seal with patient’s
face Delivery of oxygen and
anesthetic gas Attached to breathing circuit
through the orifice Black rubber is highly pliable Transparent type allows to
see: Humidity Vomiting
Retaining hooks attached to head strap
Face Mask Technique:
Usually: The mask is held in place with the left hand Thumb and index finger press on the body of the mask Middle and ring finger grasp the bony part of the mandible Little finger is placed under the angle of the jaw to thrust it
anteriorly Right hand to squeeze the bag
Difficult cases: 2 hands:
Jaw thrust (by finger tips to displace the jaw forward) Mask seal (by the thumbs pressing the mask) Assistant to squeeze the bag
Low positive-pressure ventilation (20 cm H2O)
Face Mask
Complications: Airway obstruction:
Too much pressure on mask Ball-valve effect of jaw thrust
Pressure injury to branches of Trigeminal or Facial nerves
Corneal abrasions: Tape the eyes shut to avoid it
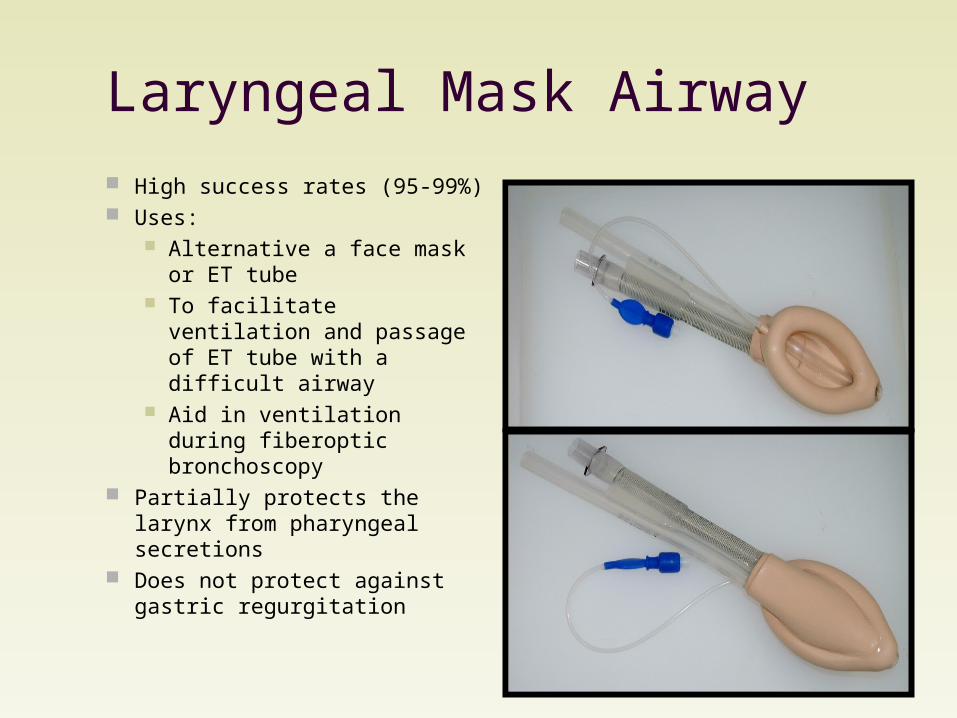
Laryngeal Mask Airway High success rates (95-99%) Uses:
Alternative a face mask or ET tube
To facilitate ventilation and passage of ET tube with a difficult airway
Aid in ventilation during fiberoptic bronchoscopy
Partially protects the larynx from pharyngeal secretions
Does not protect against gastric regurgitation
Laryngeal Mask Airway Insertion:
Requires a slightly greater anesthetic depth than that of the oral airway
Lubrication of the deflated cuff Blind insertion until it reaches the hypopharynx Inflate the cuff → low-pressure seal around the
entrance of the larynx Secured in place by tape Should remain in place until patient regains airway
reflexes Insertion under direct visualization (laryngoscope,
fiberoptic laryngoscope) is beneficial in difficult cases Partial inflation before insertion may be helpful
Laryngeal Mask AirwayLMA vs Face Mask
Advantages Hands-Free Better seal in bearded
patient Less cumbersome in
ENT surgery Easier to maintain airway Protects against airway
secretions Less facial nerve and
eye trauma Less operating room
pollution
LMA vs Tracheal Tube Advantages
Less invasive Useful in difficult
intubation Less tooth and laryngeal
trauma Less laryngospasm and
bronchospasm Does not require muscle
relaxation Does not require neck
mobility No risk of esophageal or
endobronchial intubation

Laryngeal Mask AirwayLMA vs Face Mask
Disadvantages More invasice More risk of airway
trauma Require new skill Deeper anesthesia
required Requires some TMJ
mobility N2O diffusion into cuff Multiple contraindications
LMA vs Tracheal Tube Disadvantages
Increased risk of gastrointestinal aspiration
Less safe in prone position
Limits maximum PPV Less secure airway Greater risk of gas leak
and pollution Can cause gastric
distention
Laryngeal Mask Airway
Contraindications: Pharyngeal pathology (abscess) Pharyngeal obstruction Full stomachs (pregnancy, hiatal hernia) Low pulmonary compliance
Requiring peak inspiratory pressure > 30 cm H2O Bronchospasm High airway resistance

Tracheal Tubes Uses
Deliver anesthetic gases to the trachea
Control ventilation & oxygenation
Made of polyvinyl chloride Murphy tubes have Murphy
eyes → decrease risk of occlusion
Resistance: Tube diameter Tube length Tube curvature
Tracheal Tubes Cuffs
Valve, pilot baloon, inflating tube Creats a tracheal seal
allowing PPV Deacrease likelihood of aspiration.
Pressure High pressure
more ischemic damage Low pressure
sore throat Aspiration Spontaneous extubation Difficult insertion (floppy cuff) More commonly used
Tracheal Intubation Correct placement is confirmed by:
Direct visualization of the ET tube cuff passing the vocal cords
Presence of ETCO2 on three consecutive breaths Absence of stomach “gurgling” sound made by
air entering the stomach Equal bilateral breath sounds over the lungs Fogging of the ET tube Refilling of the ventilatory bag with expiration Chest x-ray may be used to confirm placement of
tube

Combitube Consists of 2 fused
tubes The longer tube:
Occluded distal tip Side perforations
The shorter tube: Open tip No side perforations
2 inflatable cuffs: 100 ml proximal cuff 15 ml distal cuff
Combitube Technique:
Blindly inserted through the mouth Black rings have to be between the upper & lower
teeth Both cuffs should be fully inflated after insertion The distal part of the tube will lie in the esophagus 95%
of the time: The longer tube forces air to the larynx through
perforations The shorter tube acts as a gastric decompressor
If it entered the trachea: Gas will be directed into the trachea through the
perforations

Combitube
Uses: Managing difficult airway in ACLS It is rarely used LMA and others are preferred
Laryngoscope Uses in general:
Examine the larynx Facilitate intubation of the trachea
Rigid Laryngoscope: Composed of:
Handle Flange Blade Bulb
Different Types Choice depends on preference
and patient anatomy

Laryngoscope Specialized Laryngoscope:
Bullard Laryngoscope Wu Laryngoscope Both have:
Fiberoptic light sources Curved blades with elongated tips
Uses & Advantages: Visualize glottic opening in patients
with large tongues Visualize very anterior glottic
opening Anticipated difficult intubation Trauma settings Easy portability
Disadvantages: Unfamiliarity Cost
Bullard Laryngoscope
Wu Laryngoscope
Alternative Airway Techniques
Transtracheal Jet Ventilation Placing a large bore catheter (14-gauge) through the
cricothyroid membrane into the trachea Confirmed by aspiration of air before connecting to
the ventilation system Provides a temporary airway until an alternate airway
is established Complications:
Aspiration Bleeding Pneumothorax Subcutaneous emphysema Inadequate ventilation

Fiberoptic Bronchoscopy The bronchoscope may facilitate the placement of an ET tube
both nasally and orally The scope is passed through the glottis for indirect visualization
of the vocal cords, at which time the trachea is entered The bronchoscope may identify causes of acute hypoxia, and
may help to remove secretions in the airway Indications:
History of difficult intubation Upper airway abnormality Poor range of motion of TMJ Cases of impossible neck extension (unstable cervical
spine) Awake intubation


Lightwand A malleable stylet with a small light bulb on the end An ET tube is placed over the lightwand and is
inserted into the mouth Once at the tip of the larynx, the ET tube is slipped
into the larynx If the ET tube happens to enter the esophagus, the
light dims The ET tube may then be withdrawn, and another
attempt at placement is attempted This technique must be practiced in a darkened
room, limiting its use to a controlled setting

Surgical Airway Indications:
When other means of establishing an airway fail Laryngeal trauma Facial injuries Long term need of ventilatory support
Technique: Cricothyroidotomy is the preferred method of a surgical airway
It involves the opening of the cricothyroid membrane for placement of a tracheal tube Complications:
Bleeding Infection Vocal cord damage Tracheal stenosis
Contraindications: Age <12 years Laryngotracheal disruption Coagulopathy
Tracheostomy: Indicated when cricothyroidotomy is contraindicated Percutaneous dilational tracheostomy is a faster procedure with fewer complications
than a surgical tracheostomy

THANK YOU


