
Aims To encourage health professionals to use evidence based techniques to support children (and...
23
-
Upload
lance-croker -
Category
Documents
-
view
218 -
download
3
Transcript of Aims To encourage health professionals to use evidence based techniques to support children (and...


Aims
To encourage health professionals to use evidence based techniques to support children
(and their carer/s) psychologically through painful or distressing procedures.
To provide references to enhance practice.

1. To understand the importance of planning for painful or distressing procedures when working with children
2. To consider developmental stages of each child
3. To be aware of correct positioning and distraction techniques used in paediatric practice
Learning Objectives

What we’ll cover…
Planning the procedure
Medications to consider pre–procedure
Positioning for comfort
Age appropriate distraction techniques

Plan procedure• General approach ‘One Voice’• Place• Time • Staff involvement ; medical, nursing,
Child Life Therapist, parent or carer• Medications +/- fasting times • Equipment
… think about it …

One voice should be heard during procedures
Need for parent/carer involvement
Educate parent/carer before procedure
Validate child with words
Offer position of comfort
Individualise your approach
Choose appropriate distraction techniques
Eliminate unnecessary people from the room
‘One Voice’ Approach

• ‘Emla’ / topical anaesthetic agent
• Sucrose• Oral premedication;
analgesia, midazolam, ketamine
• Nitrous oxide
Medications to Consider

• Depends on procedure
• Sitting upright in a ‘hugging hold’ for IV cannula or bloods
• Lying on side for LP
• Swaddled/ wrapped (0-3 months)
Correct Positioning; promoting comfort

• Cuddling/ wrapping for 0-3 month infants promotes self caring and sense of security also prevents limbs from moving if distressed
• Offer breast feed / sucrose/ non nutritive sucking (dummy) to help minimise stress
Infants

• May like to sit upright on a parent’s lap facing the parent or facing the proceduralist whilst being distracted with bubbles, songs, toy or interactive book
• Hold in a ‘hugging hold’ to contain torso and limbs as parent soothes the child
• Parent’s free hand stabilises the limb being cannulated
Toddlers
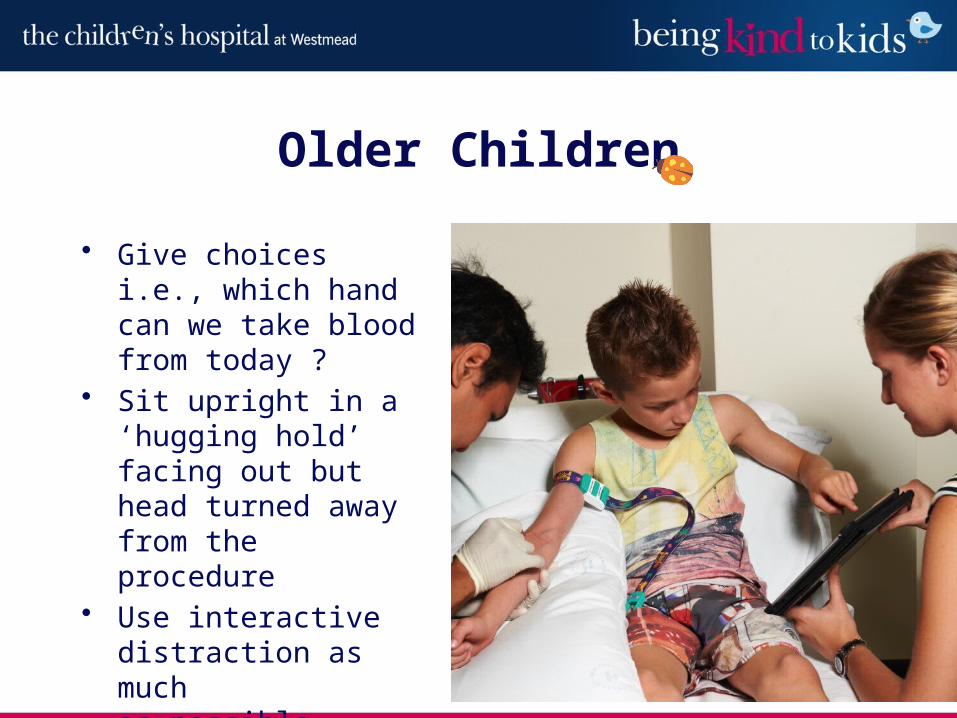
• Give choices i.e., which hand can we take blood from today ?
• Sit upright in a ‘hugging hold’ facing out but head turned away from the procedure
• Use interactive distraction as much as possible
Older Children



Stresses-parent separation, stranger anxiety• involve a parent or caregiver
who can comfort the child• comfort positioning• talking gently before
touching; use dummy, consider oral sucrose for non-nutritive sucking
• wrap/ swaddle, rhythmic patting, toy
Infant

Separation anxiety, scared of injury or pain• family member support/ (stranger danger)• comfort positioning• give sensory information, talk before touching• provide an alternative focus and involve child
as much as possible• play; favourite games, stories, songs, rhymes,
own toys
1 – 3 years

3 – 5 years
Separation, fear of blood and needles, perceived punishment, misconception of words• caregiver support/(stranger danger)• gentle concrete preparation/ social stories• give the child choices/ a perceived role/participation• use of play and distraction; iPad, bubbles, counting,
own toys• validate throughout• involve Child Life Therapy

Loss of control, pain, altered body image• explanations and participation/control where
possible• be perceptive to child’s cues• give structure • use of guided imagery, relaxation/ controlled
breathing, hobbies and interests• validate appropriately
6 – 11 years

Loss of body image, control, functions, peer acceptance, death…• include in decision making and give
choices where possible• honest explanations about procedure
(photos to explain)• coping strategies; music, relaxation,
focused breathing, iPad• other teens or caregiver• respect privacy
Teenagers

Establish rapport
A large part of communication is non-verbal;• get down to their level• use eye contact• Speak in a clear and calm voice
Age related distraction techniques

Encourage an alternative focus• stories, books,• songs, music, nursery rhymes• Guided imagery/ relaxation• deep breathing, blowing
bubbles, coaching• child’s own interests• TV/ video• iPod, iPad• Toys/ puppets
Age related distraction techniques

Finally
• stay calm
• be sensitive to child’s cues and refocus as needed
• reinforce coping strategies
• validate – ‘you’re doing really well’ / ‘it’s ok to cry’
• Association of Paediatric Anaesthetists of Great Britain and Ireland. Good
Practice in Postoperative and Procedural Pain Management 2nd Edition, 2012.
Paediatric Anaesthesia, 22 (Suppl.1),1-79.
• Breiner, Sandra M. Preparation of the Paediatric Patient for Invasive Procedures.
Journal of Infusion Nursing.2009;32(5): 252-256.
• Crain, William. Theories of Development: Concepts and Applications. Prentice
Hall, New Jersey, 2000 (217-294).
• Fox, S (2012) Paediatric Pain and Distress in the ED; New Management Tips.
Paediatrics.130e1391- e1405.
• RCH Melbourne factsheet; Infant positioning, promoting comfort, 2013
• http://www.onevoice4kids.com/index.html
• Wolheiter, Karen A &Dahlquist, Lynnda M. Interactive versus Passive Distraction
for Acute Pain Management in Young Children. J Paediatric
Psychology.2013;38(2): 202-212.
Resources

Sucrose Guidelines
http://chw.schn.health.nsw.gov.au/o/documents/policies/guidelines/2006-8241.pdf
Procedural sedation guidelines
http://chw.schn.health.nsw.gov.au/o/documents/policies/guidelines/2011-9017.pdf
Thank you to Fairfield RSL for sponsoring the ‘Being Kind to Kids’ project.
Resources


















