eHealth Procurement: eHealth for Sustainable Healthcare Delivery
Upload
noor-orfahlyCategory
view
233download
1
AI & eHealth
Noor Orfahly

Overview
Definition
Forms of eHealth
The 10 e’s in eHealth
AI-Based MDSS

Definition
eHealth is a new term dating back to 1999.
eHealth Strategy Office – UBC: Using modern information and communications technologies in the areas of health services, health education and health research.
The World Health Organization: The transfer of health resources and health care by electronic means. E-health provides a new method for using health resources – such as information, money, and medicines – and in time should help to improve efficient use of these resources.
Health Canada: An overarching term used today to describe the application of information and communications technologies in the health sector. It encompasses a whole range of purposes from purely administrative through to health care delivery.

Forms of eHealth
Primary care: The use of computer systems by general practitioners and
pharmacists for patient management, medical records and electronic prescribing.
Hospital care: ePatient administration systems Laboratory & radiology information systems Electronic messaging systems Telemedicine
Home care: Teleconsults Remote vital signs monitoring systems used for diabetes medicine,
asthma monitoring and home dialysis systems

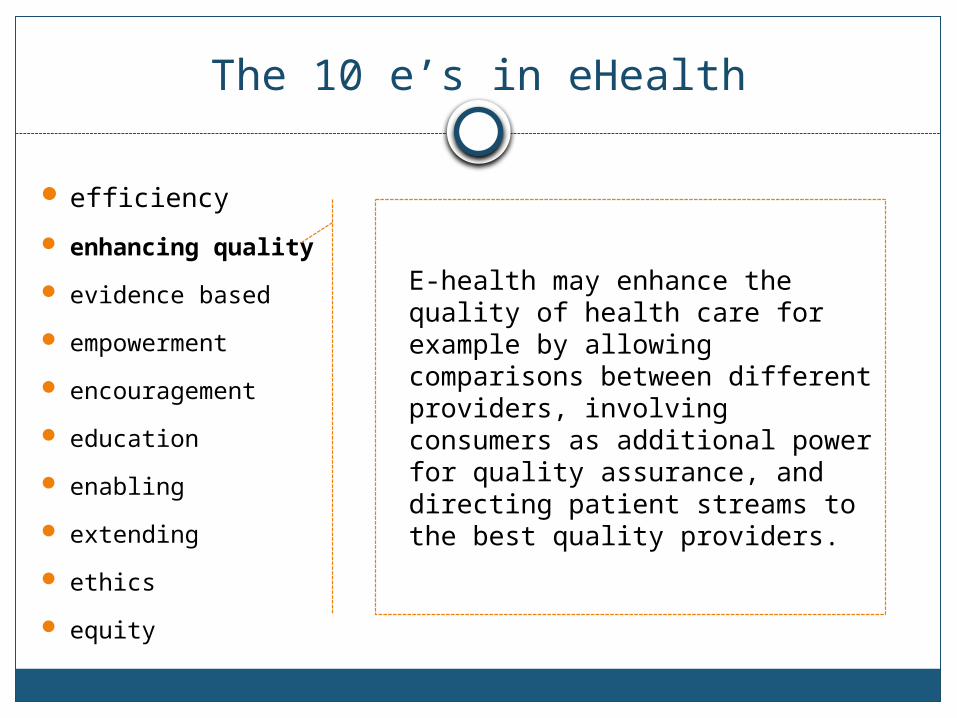
The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Increase efficiency in health care:
Decreasing costs: avoiding duplicative or unnecessary diagnostic.
Therapeutic interventions: through enhanced communication possibilities between health care establishments, and through patient involvement.
The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
E-health may enhance the quality of health care for example by allowing comparisons between different providers, involving consumers as additional power for quality assurance, and directing patient streams to the best quality providers.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
eHealth interventions should be evidence-based in a sense that their effectiveness and efficiency should not be assumed but proven by rigorous scientific evaluation.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
By making the knowledge bases of medicine and personal electronic records accessible to consumers over the Internet, e-health opens new avenues for patient-centered medicine, and enables evidence-based patient choice.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Encouragement of a new relationship between the patient and health professional, towards a true partnership, where decisions are made in a shared manner.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Education of physicians through online sources (continuing medical education) and consumers (health education, tailored preventive information for consumers).

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Enabling information exchange and communication in a standardized way between health care establishments.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Extending the scope of health care beyond its conventional boundaries.
Geographical sense: e-health enables consumers to easily obtain health services online from global providers.
Conceptual sense: These services can range from simple advice to more complex interventions or products such a pharmaceuticals.

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Online professional practice
Informed consent
Privacy

The 10 e’s in eHealth
efficiency
enhancing quality
evidence based
empowerment
encouragement
education
enabling
extending
ethics
equity
Equitable health care is one of the promises of e-health.
People, who do not have the money, skills, and access to computers and networks, cannot use computers effectively.
The digital divide currently runs between
rural vs. urban rich vs. poor young vs. old male vs. female neglected/rare vs. common
diseases.

A FRAMEWORK FOR AI-BASED CLINICAL DECISION SUPPORT
Example
Enable medical decision making in the presence of partial information

AI-Based Clinical Decision Support Framework
Introduction
Medical decision support systems (MDSS) map patient information to promising diagnostic and treatment paths.
Knowledge-based systems can suffer a significant loss of performance when patient data is incomplete: Patients omit details Access restrictions prevent viewing of remote medical records
The output of learning-based systems cannot be easily explained.
Hybrid System

AI-Based Clinical Decision Support Framework
Knowledge Base
Patient Records
Prescription
Protocol
Drug Interaction Registry

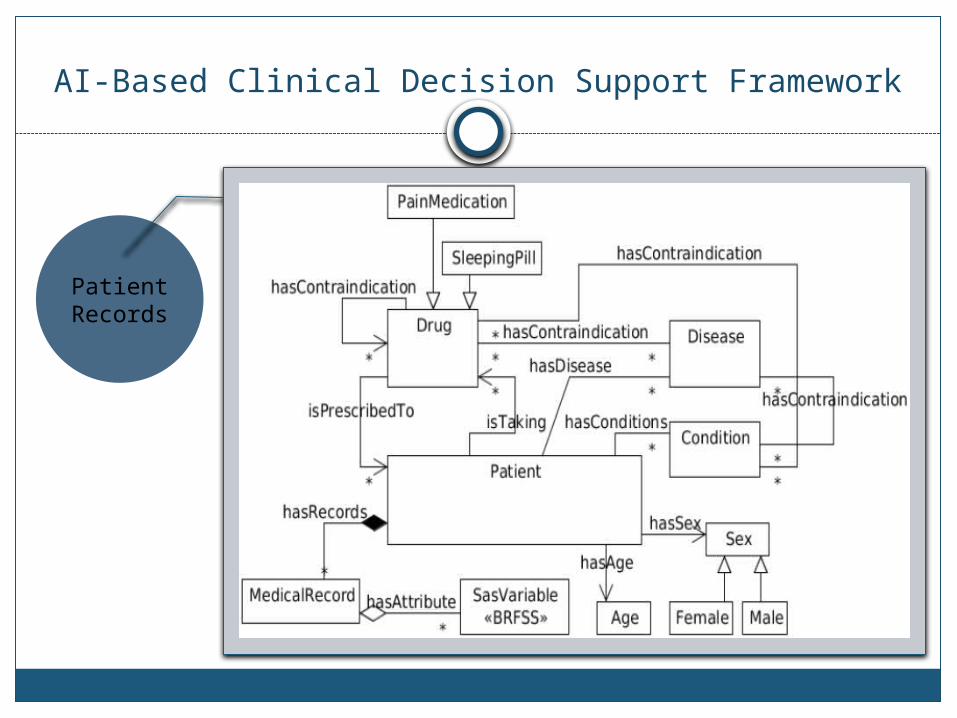
AI-Based Clinical Decision Support Framework
Patient Records
Insomnia treatment.
Patient records drawn from the Center for Disease Control (CDC). Dataset: Behavioral Risk Factor Surveillance System (BRFSS) telephone survey for 2010.
BRFSS dataset contains: Respondent information: age, race, sex, and geographic
location. Common medical conditions: cancer, asthma, mental
illness, and diabetes. Behavioral risk factors: alcohol consumption, drug use,
and sleep deprivation. BRFSS: 450,000 individuals.
Relational database.
AI-Based Clinical Decision Support Framework
Patient Records

AI-Based Clinical Decision Support Framework
Patient Records

AI-Based Clinical Decision Support Framework
Prescription
Protocol
Identify a subset of sleep aids and apply the Mayo clinic sleep aid prescription protocol to identify the conditions under which each drug should be prescribed.
Inference Rules examples:1. drug-to-drug interaction rule:If a patient is currently taking an existing drug D1, and D1
cannot be given with drug D2, then the patient cannot be given drug D2.
2. drug-to-condition interaction rule:If a patient has some existing medical condition C, and a drug D has contraindication to the condition C, then the patient cannot be given drug D.
3. drug-to-disease interaction rule:If a patient has a disease E, and a drug D has contraindication to the disease E, then the patient cannot be given drug D.
Drug Interacti
on Registry

AI-Based Clinical Decision Support Framework
Imputation
Bayesian multiple imputation Assume a particular joint probability model over the feature values.
a1, a2, …, an , P(a1 = x, a2 = y, …, an = z) = prop., etc Draw imputed datasets from the posterior distribution of the
missing data given the observed data.
Make multiple imputed datasets, then take the average of the imputed values.
a1 a2 … an
id1 x y zz
id2 x yyy z
id3 xx yy zzzz
a1 a2 … an
id1 x y ?
id2 ? ? z
id3 ? yy zzzz

AI-Based Clinical Decision Support Framework
Experimental Comparison
Patients who should be given sleep aids were labeled as ‘positive’ exemplars and those who should not as ‘negative’ exemplars.
When a system labeled a patient correctly in response to a query, a ‘true positive’ (tp) or ‘true negative’ (tn) was produced.
Otherwise, a ‘false positive’ (fp) or ‘false negative’ (fn) was produced.
The results were evaluated in terms of: Sensitivity: rate of positive exemplars labeled as positive. Specificity: rate of negative exemplars labeled as negative. Balanced accuracy: simple average of specificity and sensitivity.

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based System
Evaluate the impact of missing information on the performance of the learning-based system by removing known values from the patient records.
Defined e as the average number of attribute values removed from a patient’s record.
For each value of e, train an AdaBoost-based classifier using 50 sets of 5000 exemplars from the partially-missing data.

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based SystemAdaBoost
AdaBoost helps you combine multiple “weak classifiers” into a single “strong classifier”.
A weak classifier is simply a classifier that performs poorly, but performs better than random guessing (accuracy is greater than 50%).
AdaBoost can be applied to any classification algorithm.
What does AdaBoost do for you?1. It helps you choose the training set for each new classifier that you train
based on the results of the previous classifier.2. It determines how much weight should be given to each classifier’s proposed
answer when combining the results.

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based SystemAdaBoost
Training Set Selection: Each weak classifier should be trained on a random subset of the total training
set. The subsets can overlap. AdaBoost assigns a “weight” to each training example, which determines the
probability that each example should appear in the training set. After training a classifier, AdaBoost increases the weight on the misclassified
examples so that these examples will make up a larger part of the next classifiers training set, and hopefully the next classifier trained will perform better on them.
Classifier Output Weights: After each classifier is trained, the classifier’s weight is calculated based on its
accuracy. A classifier with 50% accuracy is given a weight of zero A classifier with less than 50% accuracy is given negative weight.

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based SystemAdaBoost
Formal Definition: The equation for the final classifier:
No. of weak classifiers
Output of weak classifier ‘t’ {-1 , +1}
Weight applied to classifier ‘t’
We make our final decision simply by looking at the sign of
this sum

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based SystemAdaBoost
Formal Definition: Weight of classifier:
The first classifier (t = 1) is trained with equal probability given to all training examples.
After it’s trained, we compute the output weight (alpha) for that classifier.
error rate (e_t ) is just the number of misclassifications over the training set divided by the training set size.

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based SystemAdaBoost
Formal Definition: Updating examples’ weights:
If the predicted and actual output agree, y * h(x) will always be +1 (1*1 or -1*-1) If they disagree, y * h(x) will be negative. Misclassifications by a classifier with a positive alpha will cause this training example to be given
a larger weight. And vice versa. If a weak classifier misclassifies an input, we don’t take that as seriously as a strong classifier’s
mistake.
Vector of weightsTraining example
number
Sum of all the weights
(normalization)
Correct output
predicted output

AI-Based Clinical Decision Support Framework
Experimental Comparison – Learning-based System

AI-Based Clinical Decision Support Framework
Experimental Comparison – Knowledge-based System
Use EulerSharp semantic reasoner for the knowledge-based reasoning

AI-Based Clinical Decision Support Framework
Conclusion
This approach of Integrating machine learning with ontological reasoning makes use of the inherent advantages of both approaches in order to offer the required accuracy for the medical domain.
This approach supports interoperability between different health information systems. A decision making process should use all relevant data from many distributed systems instead of a single data source to maximize its effectiveness.
This approach provides a framework that is generic enough to be used in other medical applications.

Thank You