
Manya Magnus, Ph.D., M.P.H., Jane Herwehe , M.P.H., Laura Andrews, M.P.H., R.N.,
Upload
crystal-morganCategory
view
218download
2
AHCCCS Data Sets Improve Population Heath Management
Rene Q. Lizarraga, B.S.Thomas M. Ball, M.D., M.P.H.
The University of Arizona Health Plans
Population Health Management
Iden
tify
At-
Risk
Mem
bers
Analytics
App
ly E
ffecti
ve In
terv
entio
n
Interventions
Hav
e M
embe
rs P
artic
ipat
e
Engagement
2

Data Provided by AHCCCS to Support Our Analytic Efforts
3
Behavioral HealthTribal HealthMedicare

Significant Delay Policy
Moderate DelayProgram Development
& Monitoring
Real Time Member Care
The University of Arizona Health Plans Primary Use of AHCCCS Blind Spot Data Sets
Pharmacy
4
Translating Data into Action: Timing is Critical

Behavioral Health Variables Of Interest
From 834 Enrollment File: RBHA indicator
From DBHS in Blind Spot Database: ICD-9/DSM diagnostic codes SMI determination identifier Behavioral health utilization
5

Key Variable: Use of RBHA indicator in 834 Enrollment File
Health Disparities Among Those With Behavioral Health Conditions
Maricopa Health Plan
Yearly Cost Per Diagnosed Member
CY 2012 CY 2013 % Change CY13 vs CY12
BH Non-BH BH Non-BH BH Non-BH
Diabetes $ 9,747 $ 7,228 $ 9,293 $ 6,093 -5% -16%
COPD $ 7,172 $ 4,763 $ 5,537 $ 3,571 -23% -25%
Asthma $ 7,366 $ 4,229 $ 5,403 $ 3,063 -27% -28%
6
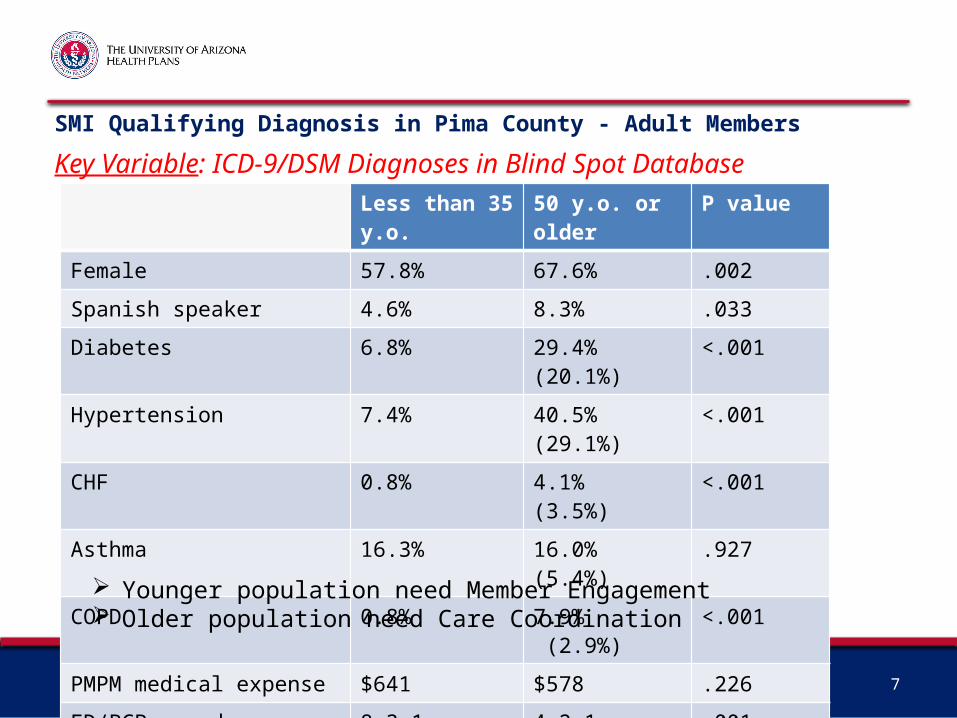
SMI Qualifying Diagnosis in Pima County - Adult Members
Less than 35 y.o. 50 y.o. or older P value
Female 57.8% 67.6% .002
Spanish speaker 4.6% 8.3% .033
Diabetes 6.8% 29.4% (20.1%) <.001
Hypertension 7.4% 40.5% (29.1%) <.001
CHF 0.8% 4.1% (3.5%) <.001
Asthma 16.3% 16.0% (5.4%) .927
COPD 0.8% 7.9% (2.9%) <.001
PMPM medical expense $641 $578 .226
ED/PCP spend 8.3:1 4.2:1 .001
Used BH services 61% 72% .001
7
Younger population need Member Engagement Older population need Care Coordination
Key Variable: ICD-9/DSM Diagnoses in Blind Spot Database

8
Physical Health Medical Expense & Hospitalizations by Behavioral Health Category
BH Group PMPM Cost
No BH utilization Comparison Group
BH utilization by non-SMI + 47%
SMI qualifying diagnosis + 78%
SMI diagnosis in Pima County
Where do they get admitted?
BH facility only 13%
PH facility only 82%
Both BH & PH facilities
5%
Use of behavioral health services and an SMI qualifying diagnosis incrementally increase physical health medical expense
Behavioral health issues need to be addressed during care transitions from PH facilities
Key Variables: Use of both RBHA indicator, SMI qualifying diagnoses & admission data
P<.001 P<.001

Determined v. Non-determined Adults (≥18) with SMI
SMI-Determined
Use of RBHA
SMI-Qualifying Diagnosis
4.6%
1.3%
6.1%1.4%
Not in a group – 86.5%
Key Variables: Use of both RBHA indicator, SMI qualifying diagnoses & SMI determination information
9

Total Admissions by Whether Member with SMI has Completed Determination Process
0%30%60%90%
2 or moreOneZero
10
P=0.36
*No significant differences for PH or BH Admissions, Readmissions or ED use

Tribal Claims Data Of >120,000 UFC members, 2.8% (3,618) report their Race as NA/AI Of UFC members, 0.3% (370) have IHS as a secondary FSC (Payer) Of UFC members, 56 members received a service paid for by IHS
Represents 454 claims 6 ED visits 1 inpatient hospital stay
Consequences outside of Maricopa County are: 75.4% of those with an IHS FSC are over 18 years of age compared to 56.5% of
those without an IHS FSC
11
Hypothesis: receiving services from both Health Plan and IHS is only likely for members living geographically close to both IHS services within their service delivery area and Health Plan services outside of their service delivery area.

Next Steps Continue use of data sets provided by AHCCCS for population health management
Identify opportunities to target care coordination efforts most effectively
Develop new programs for specific high risk subgroups
Utilize pharmacy data for member-specific interventions Identify members needing metabolic monitoring
Identify members with dangerous utilization patterns
Review patterns of care between AHCCCS and IHS within Maricopa County
Investigate potential uses of Medicare (Part C and Part D) data
12

Summary AHCCCS provided data sets allow identification of vulnerable populations to guide
program development initiatives.
These data sets can be used to monitor impact of interventions focused on whole-person care, such as Super Utilizer initiatives.
October 1, 2015 provides the opportunity to assess the value of integrated care for members with SMI determination and co-morbid chronic physical health conditions by comparison to members with SMI qualifying diagnoses without determination who will remain with their chosen health plan.
NA/AIs (living outside of Maricopa County in Southern or Central Arizona) with UFC are unlikely to utilize IHS services.
AHCCCS provided supplementary data sets serve a critical function until completion of a well functioning state-wide HIE.
13

Questions?
14


















