Aging Cancers - Congrex Switzerland · Undertreatment of breast cancer. JCO 2003; ... geriatrician,...
40
1 Cancer in the elderly: where are we today ? Dr Gilbert B. Zulian, CC Médecine interne, gériatrie & oncologie médicale FMH Service de Médecine Palliative, Département de Réadaptation et de Médecine Palliative Hôpitaux Universitaires de Genève, [email protected] Aging Cancers Epidemiology Management Evaluation Organisation Clinical cases Conclusion
-
Upload
dangnguyet -
Category
Documents
-
view
215 -
download
3
Transcript of Aging Cancers - Congrex Switzerland · Undertreatment of breast cancer. JCO 2003; ... geriatrician,...

1
Cancer in the elderly: where are we today ?
Dr Gilbert B. Zulian, CCMédecine interne, gériatrie & oncologie médicale FMH
Service de Médecine Palliative, Département de Réadaptation et de Médecine PalliativeHôpitaux Universitaires de Genève,
Aging
Cancers
Epidemiology
Management
Evaluation
Organisation
Clinical cases
Conclusion

2
Reduction
of life expectancy
of stress tolerance
of functional reserves
Diversity
of life expectancy
of tolerance to treatments
of personal expectations
The aging process

3
« Prevention is much better than cure because it can save
the labour of being sick »
Thomas Adams, 1583-1652, writer and theologianThe Happiness of the Church (1618)

observed and expected age structure in CH
Adapted from OFS at http://www.statistik.admin.ch/
0%
20%
40%
60%
80%
100%
1910 1930 1950 1970 1990 2000 2020 2040 2060
80+65-7920-640-19

5
cancer incidenceHematol Oncol Clin North Am 2000;14:17-23
2’261 per 105 population > 65 years of age
207 per 105 population < 65 years of age
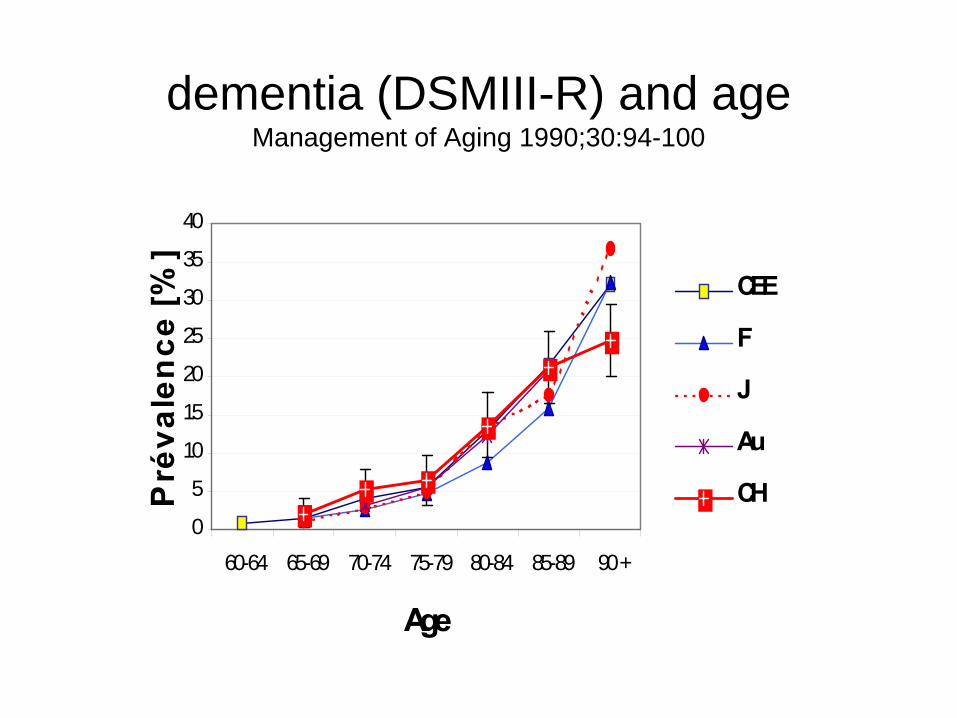
dementia (DSMIII-R) and ageManagement of Aging 1990;30:94-100
0
5
10
15
20
25
30
35
40
60-64 65-69 70-74 75-79 80-84 85-89 90 +
Age
Pré
vale
nce
[%]
CEE
F
J
Au
CH

7
Why are elderly cancer patients badly treated ? Lancet 1990;335:1020-2
Undertreatment of breast cancer. JCO 2003;21:3580-7
407 women > 80 years, 1989-1999, RGT
five-year survival• 12% 0 tt 46%• 32% tamoxifen single agent 51%• 7% conservative surgery (bcs) 63%• 33% mastectomy 82%• 14% bcs + adjuvant tt 90%• 2% various tt 42%

8
life expectancyJAMA 2001;285:2750-6
0
2
4
6
8
10
12
14
16
70 80 85
UPPERMEANLOWER

9
the managing physiciansLancet 353:1179, 1999
The five E’s
• Efficacy – is the treatment active ?• Effectiveness – is the treatment effective ?• Efficiency – is the maximum obtained with minimal resources ?• Equity – are the most in need receiving tt ?• Economy – are the incidental costs justified ?

10
attitudes towards chemotherapyBMJ 1990;300:1450-60
Treatment medical oncologists patientsacceptance + radio-oncologists
--------------------------------------------------------------------------
• Low possibility of cure 24 % 60 % • Survival > 3 months 15.3 % 47.9 %• Symptoms improvement 4.5 % 50.5 %

11
Small Cell Lung CancerBJC 2006;94:18-21
• 322 pts > 70 years treated with chemotherapy
1982-1994 1995-2003
• Median survival 25sem 43sem• 1-year survival 14% 27% P<0.001
platinum combinations vs others (P<0.001)cisplatin vs carboplatin (P=0.7)
changes due to platinum and to supportive care
12
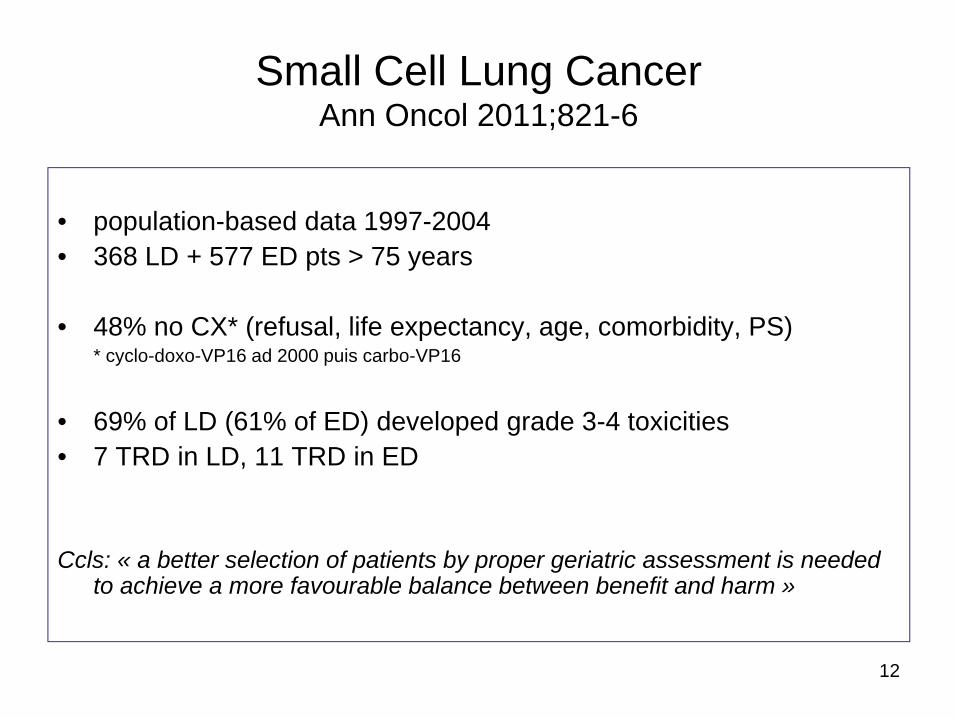
Small Cell Lung CancerAnn Oncol 2011;821-6
• population-based data 1997-2004• 368 LD + 577 ED pts > 75 years
• 48% no CX* (refusal, life expectancy, age, comorbidity, PS)* cyclo-doxo-VP16 ad 2000 puis carbo-VP16
• 69% of LD (61% of ED) developed grade 3-4 toxicities• 7 TRD in LD, 11 TRD in ED
Ccls: « a better selection of patients by proper geriatric assessment is neededto achieve a more favourable balance between benefit and harm »
13
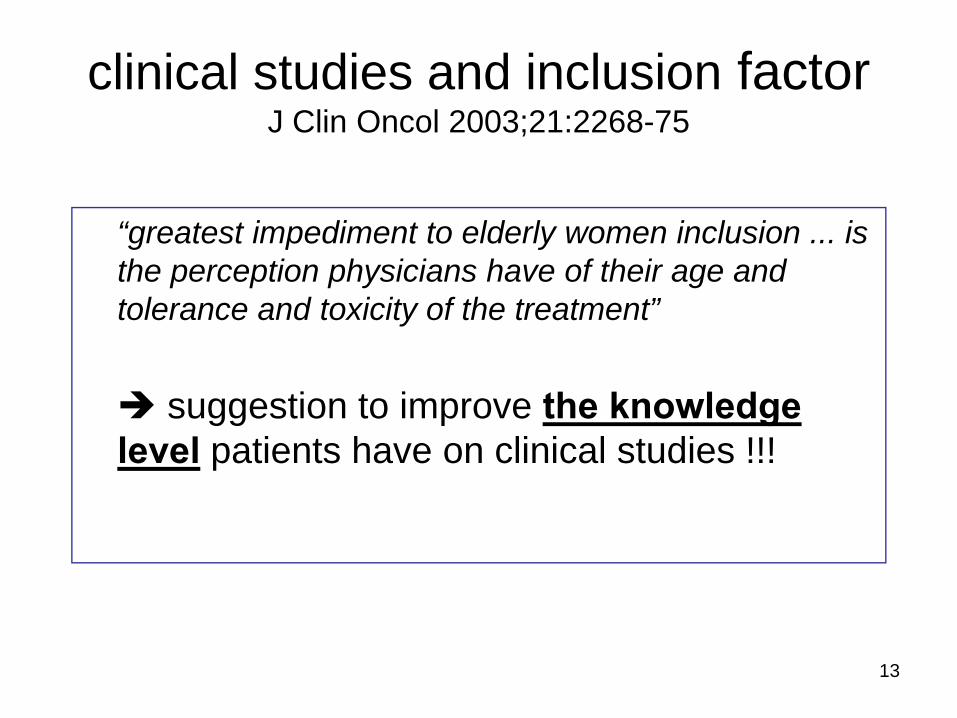
clinical studies and inclusion factorJ Clin Oncol 2003;21:2268-75
“greatest impediment to elderly women inclusion ... is the perception physicians have of their age and tolerance and toxicity of the treatment”
suggestion to improve the knowledgelevel patients have on clinical studies !!!

14
education and inclusion rate J Clin Oncol 2005;23:2201-7
• CALGB : 73 institutions = standard information vs 53 institutions = specialized interventional education
(workshop, documentation, list of protocols, monthly recall emails during 1 year, case discussion)
% patients ≥ 65 years effectively included into tt studies
T0 1 year 2 yearsEducated group 37% 36% 31% Standard group 32% 31%

15
patients’ opinionMedical Care 2005;43:173-181
Self-assessment of the present state of health
49 HR prostate cancer 51 metastatic breast cancer
Age 69.8 (45-85) 53.5 (33-77)
• Very good 82% 61%• Good 18% 26%• Fair 0 14%• Poor 0 0

16
primum non nocere
• Is the patient going to die of the disease ?
• Is the patient going to suffer of the disease ?
• Is the patient going to tolerate treatmentwith no fatal complications ?
Hippocrates oath (-460 à -377)Geneva oath (1948, 1968, 1983)

Multidimensional Geriatric EvaluationCrit Rev Oncol Hematol 2005;55:241-52
• MMSE• ADL, IADL• GDS 15• MNA• CIRS-G, Charlson• Timed get up and go test• MIF (FIM)• Social evaluation• QLQ-C30• …• Patient’s opinion
17

18
Cancer du sujet âgé: quelle évaluation préalable à la prise de décision thérapeutique ?Martial Coutaz & Jérôme Morisod (Centre Hospitalier du Chablais, RSV). Rev Med Suisse 2011;7:963-7

19
clinical organisation of geriatric oncologyCrit Rev Oncol Hematol 2007;62:62-73
58 SIOG members60% MGE (CGA)21 GOP (18 oncology and 3 in geriatrics)>60% wanted to include patients >70 ans in clinical studies whereas
the proportion actually included was 20%
Onco-geriatrician trained in both disciplines of oncology and geriatrics, thereforeable to perform CGA
Onco-geriatrician integrated in a team able to perform CGA in continuouscollaboration with a geriatrician
Onco-geriatrician capable to perform part of CGA in continuous collaboration witha geriatrician.
GOP-Geriatric Oncology Program (medical oncologist, surgical oncologist, radiation therapist, geriatrician, advanced nurse, social worker, dietician, researchnurse, physiotherapist, pharmacist, residents, students)

20
evaluation decision treeApparently in good
health May be not exactly in good health
Definitely not in good health
Detection (screening) +/- Multidimensional Geriatric Evaluation
Frailty confirmed
ADAPTED TREATMENT or SYMPTOMATIC
TREATMENT
Vulnerability detected
TREATMENT ADAPTED
Good health confirmed
STANDARD TREATMENT

screening tools
• VES 13 (USA)
• G 8 (France)
21

Vulnerable Elders Survey (VES-13)JAGS 2001;49(12):1691-1699
22
1. Age_____ (One point for age 75-84, 3 points for age 85 or greater)2. Compared to other people of your age, would you say that your health is: Poor * (1 Point), Fair* (1 Point), Good, Very Good, or Excellent3. How much difficulty do you have with the following physical activities: (SCORE 1 POINT FOR EACH * , MAXIMUM OF 2 POINTS)
No difficulty A little difficulty Some difficulty* A lot of difficulty* Unable to do*- Stooping, crouching or kneeling- Lifting, or carrying objects as heavy as 10 pounds- Reaching or extending arms above shoulder level- Writing, or handling and grasping small objects- Walking a quarter of a mile- Heavy housework such as scrubbing floors or washing windows
4. Because of your health or a physical condition, do you have any difficulty: (SCORE 4 POINTS FOR ONE OR MORE * YES RESPONSES IN THIS SECTION)Shopping for personal items (like toilet items or medicine)?
YES>> Do you get help with shopping? YES* NONODON”T DO>> Is that because of your health YES* NO
Managing money (like keeping track of expenses or paying bills)?YES>> Do you get help with managing money? YES* NONODON’T DO>> Is it because of your health? YES* NO
Walking across the room? USE OF CANE OR WALKER IS OKAYYES>> Do you get help with walking YES* NONODON”T DO>> Is that because of your health? YES* NO
Doing light housework (like washing dishes, straightening up, or light cleaning?YES>> Do you get help with light housework? YES* NONODON’T DO>> Is that because of your health? YES* NO
Bathing or showering?YES>> Do you get help with bathing or showering? YES* NONODON”T DO>> Is that because of your health? YES* NO
Scoring 3 or greater identifies an individual that has 4,2 times the risk of death or functional decline over the next two years.

23
Cancer du sujet âgé: quelle évaluation préalable à la prise de décision thérapeutique ?Martial Coutaz & Jérôme Morisod (Centre Hospitalier du Chablais, RSV). Rev Med Suisse 2011;7:963-7

24
Cancer du sujet âgé: quelle évaluation préalable à la prise de décision thérapeutique ?Martial Coutaz & Jérôme Morisod (Centre Hospitalier du Chablais, RSV). Rev Med Suisse 2011;7:963-7

G 8. Soubeyran P, ASCO 2009 (abstract)
25
Abnormal ≤ 14
Sensibility 89,6%Specificity 60,4%

26
Protocole Oncodage (Soubeyran, Rainfray)
27
Oncodage study1650 patients, Aug 2008 - Jan 2010
1st presentationClinical Science Symposium
4th June ASCO 2011Abstract #9001
(under embargo)

28
ethic principles
autonomy justice
beneficiency non-maleficiency

29
Mr B, 86 ans
Marié, 2 enfants de 54 et 58 ansDéménageur, retraité depuis 1 anPas d’antécédents médico-chirurgicauxTabac actif, OH modéré, 0 médicaments
T-1 mois: toux, expectorations, baisse EGT0: RX 1 bronchopneumonie
ttt antibiotique ?T1: pas d’amélioration
RX2 élargissement médiastinalnéoplasie ?
T2: RX3 opacité para-hilaire droitenéoplasie probable ?
T3: RX4 néoplasie certaine mais expectorations –

30
avis pneumologique ? avis oncologique ? investigations supplémentaires ?
T4: RX5 épanchement pleural D vs atélectasie
T5: RX6 poumon D blanc
T6: 0RX décès au 4e jour d’hospitalisation
pas d’autopsie

31
Mr A, 92 ansHTA. Hypothyroïdie. Hernie hiatale. Fibrose pulmonaire idiopathique.
Veuf depuis l’âge de 54 ans, 2 filles âgées de 56 et 58 ansAncien tailleur reconverti dans l’horlogerieDomicile, indépendant pour les AVQ et AIVQ1 aide-ménagère 1x/semLecture, membre d’un club de joueurs de cartes0 tabac, 0 toxiques. Amlodipine 5mg/j, Eltroxin 50mg/j

32
T0 : essoufflement, toux lors des promenades, dorsalgies irradiant dans les jambes RX : opacité pulmonaire para-trachéale droite
T+1 mois : biopsie trans-thoracique sous CTscan: carcinome peu différencié à grandes cellules du LSD avis oncologique : obtenir un … avis chirurgical par téléphone: inopérable en raison de l’âge et du mauvais état général (!), FA
T+3 à +9 : cf étude ELVISVRLB 30 mg/m2 iv J1, J8 q29 sans ESAucun effet visible ou mesurableEPO, Sertraline, Acenocoumarol, Amlodipine, Eltroxin

33
T+10 : décès sur diverticulite aiguë perforée avec péritonite stercorale
Autopsie :
1. carcinome à grandes cellules du LSD (5.6 x 4.5 x 3.7cm), nécrose tumorale centrale >50%, multiples nodules satellites <1cm, lymphangite carcinomateuse, pas de métastases ganglionnaires ni parenchymateuses
2. maladie diverticulaire du sigmoïde avec une perforation de 0.4 cm entourée d’un abcès et d’une inflammation chronique

34
Mr C, 72 ans, prêtre dans une paroisse, pas d’antécédent
T-4: baisse EG, dégoût alimentaire, perte de poidsT0: urgences pour asthénie et pâleur extrème (Hb 52)
ADK caecal et rectosigmoïdien M+ (foie, poumons)0 chirurgie, 0 chimio, RX hémostatique en R
T1: transfusions, fer + folates, INFORMATION et EVALUATIONMMS 28/30, indépendant AVQ et AIVQ, GDS-15 = 2, ESAS 0
T2: capecitabine 2000 mg/m2 J1-14 et oxaliplatine 75 mg/m2 J1 x 5
T6: + 4kgs, 0 transfusiontransfert en EMScapecitabine 2000 mg/m2 J1-14 x 4

35
Mr C, 72 ans, prêtre dans une paroisse, pas d’antécédent
T10: adénome tubulo-villeux dysplasique du rectumT12: troubles cognitifs (perte de mémoire et difficultés
d’orientation) T18: récidive/progressionT24: décès en EMS

36
Mr D, 88 ans
T-6 ans: glossectomie partielle pour carcinome épidermoïdeT-3 ans: leucémie tricholeucocytaire non traitée en raison de l’âgeT-X ans: cancer prostate non traité
démence modérée (donepezil), IRC
T0 : hospitalisé car sa femme est hospitalisée en raison d’uneinfection pulmonaire
: fatigue et inconfort abdominal: pâle, masse abdominale sensible: AIVQ 0/8, AVQ 2/6, MMS 16/30, GDS 7/15: Hb 105 g/l, GB 71.5 G/l (94% tricholeucocytes), Th 62 G/l: créatinine 130 μmol/l, albumine 36 g/l: splénomégalie 21x16cm à l’echographie

37
Mr D, 88 ans
Consensus professionnel avec avis hématologique spécialisé, familial (épouse et 2 enfants)et patient
T+2 mois: RAD, pas de plaintes (sauf troubles mnésiques)Hb 131 g/l, GB 3 G/l (0 tricholeucocytes), Th 80 G/l
T+18: admission du couple dans un EMS

feasibility of "specific" ttJournal d’OncoGériatrie 2011;2:41-45
• 16 patients (80 – 93 years) fragile (CGA)• Advanced and/or metastatic cancers• CX, HX, RX, Ø SX
• 2 deaths unrelated to tt• 14 discharged home or to nursing home
• 9 alive 12 months after discharge
38
feasibility of "specific" tt Journal d’OncoGériatrie 2011;2:41-45
• ESAS* from 27.7 to 24.4, ns
• FIM from 99.0 to 107.2, ns
39

40
conclusion« Knowledge of ethics would make us more aware of issues
concerning the appropriate balance between respect for personsand individual autonomy and the beneficient paternalism which isenshrined in not only health care provision but also mirrored in normal human existence with regard to the elderly.
If we are to improve the care elderly people with cancer receive, we must begin to explore some of our basic assumptionsregarding the need of this patient group. Ensuring that weprovide an equitable service to older people with cancer is indeedan ethical challenge and the justice of providing optimal care to these patients should not be considered a dilemma. »
Nora Kearney, Macmillan Professor in Cancer Nursing, Glasgow, Scotland(Critical Reviews in Oncology/Hematology 33:149-154, 2000)