Aging and Cardiovascular Disease Marek Smieja, MD PhD FRCPC.
13
Aging and Cardiovascular Disease Marek Smieja, MD PhD FRCPC
-
Upload
katrina-harrell -
Category
Documents
-
view
216 -
download
1
Transcript of Aging and Cardiovascular Disease Marek Smieja, MD PhD FRCPC.

Aging and Cardiovascular Disease
Marek Smieja, MD PhD FRCPC

Atherosclerosis and Cardiovascular Disease

Cardiovascular Disease• Heart attack (myocardial infarction)
– Death, bypass surgery or coronary angioplasty
– Heart failure, recurrent angina
• Stroke
– Death
– Disability: weakness, sensory, speech
• Renal: dialysis or transplant
• Peripheral vascular disease
– Gangrene, infections
– Impotence

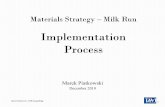
Heart Attacks increase with Age
Inc i
den
ce /
100
0 P
Y/
9 5%
CI
EventsPYFU
0 2 2 15 55 80 80 75 53 34 25 24 445 275 2322 7408 18012 32551 30991 18600 12209 7583 4024 1916 1413 137310
Age group
0
5
10
15
20
25
<2020-2
425-2
930-3
450-5
435-3
940-4
445-4
955-5
960-6
4
D:A:D study: Friis-Møller D:A:D study: Friis-Møller et alet al, NEJM, 2007, NEJM, 2007
Adjusted* relative rate: 1.32 (32%) / 5 years =
1.06 (6%) / year
>7065-6
9

Predicting Risk of Heart Disease
• Age
• Male
• Smoking
• Cholesterol
• Blood pressure
• Diabetes

*Framingham equationLaw et al, HIV Medicine, 2006
Observed and Predicted Heart Attack Rates
0
1
2
3
4
5
6
7
8
Duration of cART exposure (years)
Ra
tes
pe
r th
ou
sa
nd
pe
rso
n y
ea
rs
<1 1-2 2-3 3-4 4+
Observed rates
Best estimate of predicted
rates*
None
Copenhagen Risk Score underpredicted by 40%Copenhagen Risk Score underpredicted by 40%

…and now for the good news
• “Age as a modifiable risk factor”– Allen Sniderman– Years of risk factor acting, not age per se– Smoking, cholesterol, blood pressure
damage arteries– Almost NO progression of disease in
absence of risk factors

Smoking and Heart Attacks• Cui Qu (poster): 60% smokers vs. 20% Ontario
• Continue smoking: 3.0 X (90% lifelong!)• Former smoking: 1.8 X -DAD study
• Heavy smoking (>40 cig/day): 9.0 X• Second-hand smoking:
– 1-3 hours/day: 1.24 X– >3 hours/day: 1.62 X -InterHeart
• Scotland smoking ban (NEJM 2008):– 17% decrease in MI (versus 3% in England)– 21% never smokers, 19% former smokers

Cholesterol and Heart Attacks
• Total cholesterol, LDL (“bad”) cholesterol – Mediterranean Diet– Statins slow atherosclerosis, prevent heart attacks
• HDL (“good”) cholesterol protective– Lifestyle: smoking cessation, exercise– Drugs not very effective or even harmful
• Statin drugs most effective– No effect of Vitamin C, E, beta-carotene,
B6/B12/folate, fish oils?

Developing Canadian Evidence-Based Guidelines on
Cardiovascular Risk in HIVMarek Smieja
Astha RamaiyaGreg Bondy
Unrestricted educational grants from: Abbott, Astra-Zeneca, BI, BMS,
Gilead, GSK, Merck, Pfizer, Tibotec, CIHR

Participants
• Marek Smieja
• Astha Ramaiya
• Greg Bondy
• Jacques Genest
• Allan Sniderman
• Jean-Guy Baril
• Julian Falutz
• Marianne Harris
• Sean Hosein
• Mona Loutfy
• Anita Rachlis
• Linda Robinson

Canadian Guidelines SummarySmieja et al, CAHR 2008
• 1. HIV is a weak cardiac risk factor (B-II)(B-II)• 2. Smoking main cause (A-II)(A-II)• 3. HAART: PI (B-II(B-II) > NRTI (C-II)(C-II) > NNRTI
– Starting & stopping HAART (B-II)(B-II)• 4. Screening-Framingham (B-II)(B-II) + time on
HAART (C-II)(C-II)• 5. Treatment-statins (A-I),(A-I), switching (B-I)(B-I)
smoking cessation meds (A-I)(A-I)

Solutions to Aging & Heart Disease: S&M• Stop Smoking
– Avoid all smoking including passive smoking
• Start Statins– Best data on large benefit, low risks
• Switch HIV therapies– Maximize viral load suppression, – Minimize lipid abnormalities
• Stress management• Slim • Sweat: (s)exercise
&• Mediterranean diet