Latest Veritas VCS-261 Dumps Question & Answers | Veritas VCS-261

Wellbeing and Health Partnership Executive Thursday 12 May 2011 at 1.00 pm Meeting to be held: Committee Room, Newcastle City Council, Civic Centre, Newcastle upon Tyne NE99 2BN Contact Officer:
Helen Wilding, Wellbeing and Health Partnership Coordinator Tel: (0191) 211 6461 Email: [email protected]
Membership
B Douglas/A McNulty, Cllr L Langfield, M Khaw, G Tiller, E Weir, S Young, B Reid, G. O’Hare, J Collings, D Slater
AGENDA
Time Item Lead Paper For Page No.
1.
1.00pm Introduction and Apologies for Absence
2.
1.10pm Carers Action Plan (Issue arising from work of Carers Strategic Board)
CB KC
Yes Agreement 1 - 34
3.
1.30pm Community Development and Community Engagement: Distinctions and Synergies
HW Yes Information and Discussion
35 - 40
4.
2.00pm WHO European Healthy City - Review of work to date and emphasis moving forward
HW To Follow Discussion
5.
2.30pm Prevention SY Yes 41 - 58
Report from VCS Adult Wellbeing and Health Open Forum
6.
2.45pm Older People's Strategic Board Update Report
CW BD
Yes Information and Discussion
59 - 62
7.
3.00pm Establishment of Health and Wellbeing Board and Review of Wellbeing and Health Partnership Strategic Boards
CW Verbal Information and Agreement
8.
3.20pm Community Engagement: Recommendations of work by Peter Fletcher Associates
CW Yes Discussion 63 - 70
9.
3.40pm Co-ordinators Report HW To Follow Information

2
10.
Minutes of Previous Meeting - 17 March 2011
Not Available
11.
3.50pm Any Other Business
12.
Date and Time of Next Meeting
Wednesday 22 June 2011, 1pm - 4pm

Page 1 of 1
Wellbeing and Health Partnership – Wellbeing & Health Executive
Thursday 12 May 2011 – 1.00pm – 4.00pm
Report from: Carers Strategic Board
Topic: Executive sign up from all partners
1. Background
1.1 The Carers Strategic Board agreed in principle the priorities outlined in the carers action plan September 2011 – August 2013 (copy attached). The board recognises and values the work currently underway with the delivery groups which are demonstrating effective partnership working and progress in terms of achieving our shared outcomes for carers.
2 Executive sign up
2.1 The Carers Strategic Board has excellent working relationships with its partners and we wish to reinforce this further by ensuring that our effective partnership arrangements are supported at the highest level in all of our partner organisations.
2.2 We request the Wellbeing and Health Executives support in enabling our health partners ( NTW, PCT and Health Trusts) ‘sign up’ to our carers strategic action plan.
3. Recommendations
3.1 We request the Executive review and comment on the attached action plan.
3.2 We request the Executive recognise and support the activity of implementation both within the partnership and within individual organisations.
Report written by:
Cathy Bull, Director of Adult Social Care, Chair of Carers Strategic Board
Tel: 0191 2116318 Email: [email protected]
Agenda Item 2
Page 1

Page 2
This page is intentionally left blank

Newcastle Wellbeing and Health Partnership
Newcastle Carers Strategic Action Plan
September 2010 – August 2013
SETTING THE SCENE
One of the ambitions of the Newcastle Partnership is to improve the wellbeing and health of adults in
Newcastle. This work is led by the Wellbeing and Health Partnership, made up of people from
organisations such as Newcastle City Council, your NHS in Newcastle and the voluntary and community
sector. Together these partners want to make sure that all adults have long, happy lives. You can read
more about the partnership and its work on www.wellbeingforlife.org.uk.
The circumstances of carers’ lives mean it is more likely that they will experience problems with their
wellbeing and health. So, the Wellbeing and Health Partnership has a Carers Strategic Board within its
structure. The Board is responsible for leading the partnership’s work around carers – understanding
what they need and making sure changes are implemented to improve their quality of life. The Board
does not do this alone, it works through a network of organisations and services in the city all made up
of people who really care about improving the lives of carers.
The Wellbeing and Health Partnership is part of a wider Newcastle Sustainable Community Strategy
which sets out a vision for the future of the City over the next 20 years. The Sustainable Community
Strategy is a set of priorities based on a broad range of information and intelligence to understand the
needs of local people and communities and the problems they face. It is based around six themes. The
Carers Strategic Action Plan sits in Theme 2 – Adult Wellbeing and Health.
There are seven Adult Wellbeing and Health outcomes which are shared throughout Newcastle’s
Sustainable Community Strategy and the Carers Strategic Action Plan. You can read more about the
Sustainable Community Strategy on www.newcastle.gov.uk.
This Carers Strategic Action Plan sets out the work that the Carers Strategic Board will be leading on
through to 2013.
Page 3

2
WHAT THE ADULT WELLBEING & HEALTH OUTCOMES MEAN FOR CARERS
Improved health: for carers this means:
• Promoting good physical and mental health
• Helping carers deal with stress with swift access to therapeutic services
• Emotional support
• Support and advice to care in a way which does not damage their own health
• Having their own health needs addressed, for example health screening
• Opportunities for exercise and having accessible health services, including GP’s who fully understand the needs of carers
• Emergency and crisis cover which is planned, accessible and reliable
Have a good quality of life: for carers this means:
• Having a life outside of the caring role and the emotional support do this
• Having more control and choice over how services are planned and delivered
• Some free time to pursue leisure, social activities and life long learning
• Regular breaks to ‘re-charge their batteries’
• Access to ‘universal’ services and citizens rights as everyone else has
• Accessible transport
• Having aspiration and hope about their future
Page 4

3
3. Make a positive contribution: for carers this means:
• Acknowledgement that the skills and experiences carers acquire through their caring role is valued by professionals and services
• That a carer’s voice is heard individually and collectively and this is used to inform service design and planning at every stage of the process. More importantly that we hear from those carers least able to speak out for themselves
• The removal of barriers to carers’ involvement for example ‘common sense’ confidentiality
• Health and social care staff having a good understanding of the complexity and sometimes conflict /interdependency that can exist between the carer and cared-for relationship
• Ensuring involvement of carers during the hospital phase and in particular during discharge planning
• Developing open and honest relationships with carers built on trust so that carers are clear on eligibility for services for ‘cared for’. Being open and honest about what we can and can’t do.
• Real commitment form partners to make these principles a reality
4. Exercise of choice and control: for carers this means:
• Development of a ‘carer conscious community’, so that all people, and services both public and private have a better understanding of who carers are and what they do
• That carers’ access to services is fair and that they are safeguarded from abuse, in line with The Performance Assessment Guide and The Outcomes Framework (2008-09) and Equality Act (2010).
• Recognition that ‘transitions’ can be time of great stress for carers for example the needs of young adult carers are different to adult carers; and when caring comes to an end.
• Good assessments that adequately reflect the carer’s needs and wishes, which views the carer as a person first with a set of needs and a carer second.
5. Freedom from discrimination and harassment: for carers this means:
• Working with staff who are knowledgeable about the needs of carers who can demonstrate an empathic approach to their work and do not make assumptions about a carer’s willingness to care.
Page 5

4
• Having a compliments and complaints service that is accessible, that gets things sorted as quickly as possible.
• Equity of access for all carers particularly those who can be overlooked because they come from a particular group, for example, BME (black and minority ethnic) carers, young carers, working carers, carers living in poverty, carers who are socially isolated, disabled carers, gay, lesbian, bi-sexual and trans-gendered carers, carers of people with drug and alcohol misuse and carers in travelling, refugee and emerging community groups.
6. Economic well-being: for carers this means:
• Support to consider work and training opportunities, for example Job Centre Plus Care Partnership Managers
• Access to good quality information regarding benefits and finances, such as welfare rights services and debt counselling.
• Encouraging local employers to allow more flexible working
• Providing flexible services for the cared-for to enable the carer to maintain employment or consider returning to the jobs market.
• Minimising the impact of the costs of caring on families
• Acknowledging that carers have aspirations, hope and dreams like all people and supporting them to realise their potential in terms of personal and professional development.
7. Personal dignity and respect: for carers this means:
• Taking full account of the carer’s point of view, particularly where there is conflict with the cared-for’s wishes
• Acknowledging the expertise of the carer in relation to their skill and knowledge. Viewing the carer as co-worker
Page 6

5
NEWCASTLE CARERS ACTION PLAN OUTCOMES
The Carers Strategic Action Plan is a partnership between Newcastle City Council Adult and Culture
Services, Health Services and voluntary organisations to develop services and support for adults caring
for adults. It is a multi-agency strategy, which acknowledges that caring impacts on all aspects of your
life; such as health, housing, employment and training, leisure, exercising choice and having a life
outside of your caring role. This is known as a model of comprehensive carer support.
The direction of travel proposed in this action plan is based on information carers have shared with us,
evidence from the JSNA (joint strategic needs assessment). You can read more about the JSNA and its
work on www.newcastle.gov.uk. This is an analysis of the needs of the population in Newcastle
identified, in the main, from Census data, and evidence from research; and Government legislation. The
priorities within this strategy are guided not only by local intelligence, but also by national priorities.
Achieving the five outcomes in the National Carers’ Strategy 2008 via a model of comprehensive
carer support is a shared responsibility, which can be achieved by multi-agency partners working
together. The National Carers Strategy outcomes are:
1. Carers will be recognised as expert care partners and will have access to the integrated and
personalised services they need to support them.
2. Carers will be supported to stay mentally and physically well and treated with dignity
3. Carers will be supported so that they are not forced into financial hardship by their caring role
4. Carers will be able to have a life of their own alongside caring
5. Children and young people will be protected from inappropriate caring and have the support
they need to learn, develop and thrive, to enjoy positive childhoods and to achieve against all
the Every Child Matters Outcomes.
Page 7

6
WHAT DOES THE EVIDENCE TELL US ABOUT THE NEEDS OF CARERS IN NEWCASTLE?
Statistical information
Of the 26,267 carers living in Newcastle upon
Tyne 62% provide unpaid care for between 1-19
hours per week
13% provide unpaid care 20-49 hours per week
25% provide unpaid care 50 or more hours per
week which is 5% higher than the figure for
England
What does this mean for the action plan?
We must not ignore those who provide care for the
least number of hours per week as they form the
majority. However, we must also ensure that those
who provide the high levels of support can readily
access help and support.
We must ensure that we deliver universal services
for all carers, for example good quality information
and signposting at first contact; through to targeted
services providing specific support to those carers
at greater risk. Carers who are supported from the
outset of their caring journey are more likely to
enjoy good health and well-being.
The number of people with a LLTI (limiting long
term illness) is 21.6% for the City; however this
figure rises significantly from 27.7% in Byker to
30.9% in Walker. Moreover those carers who
provide 50 or more hours of care per week is 2.5%
for the City as a whole, though rises to 3.4% in
Byker and 3.9% in Walker. This data reflects
regional and national evidence which suggests
that carers who provide 20 hours of care or more
were considerably more likely to live in social
housing, live in a household with no working adult,
and live in a household with a person with a LLTI
(DOH, CIRCLE & University of Leeds 2010)
It tells us that carers in these areas may be facing
particular pressures due to poverty, higher levels of
disability and illness and social isolation due to
reduced opportunities for socialisation. Research
from Carers UK suggests not surprisingly that
carers providing ‘heavy end care’ 50 hours plus are
at a greater risk of ill health and carer breakdown
due to stress.
We must ensure equity of access for carers in all
Wards of the City; however we have a duty to
ensure that carers at greatest risk receive support
to prevent carer crisis and breakdown.
Evidence from the 2001 Census tells us that
Carers in Newcastle report higher than average
levels of poor health, not surprisingly compounded
by number of hours caring; with 15% of carers
reporting poor health compared with a national
average of 11%
We must ensure that carers who report poor health
are offered appropriate health and social care
services to enable them to carry on in their caring
role if they wish to.
Demand for care in Newcastle is growing. ONS
(office for national statistics) population predictions
for Newcastle upon Tyne predict a growth in the
population aged over 65 based on 2006 estimates.
This suggests more people will be providing
We must be prepared to cope with a rise in the
informal caring population and the impact this may
have on health and social care services. This is
particularly so for older carers where the increase
in numbers will be the steepest. We must ensure
that carers are a consideration in the development
Page 8
7
unpaid care year on year. and commissioning of services for older people in
the City.
Services must help to ensure that carers own
health does not suffer as a result of caring
46% of respondents to a local survey could not
work because of their caring role. Further work is
needed to better understand what some of the
issues are. From 2001 Census data, out of the
26,000 carers in the City, 14,067 are not in any
form of paid employment. 3,723 work part time
and 8,366 full time
We must look at ways to enable carers to mix paid
employment with their caring role. Employers need
to be encouraged to develop flexible working
patterns for carers. Newcastle City Council as an
employer can lead by example.
Feedback from local consultation events with
carers, for example the Carers Conference June
2010 tell us that access to training, personalised
services, accessible health services that
understand your needs and flexible employment
opportunities are really important. Moreover, you
told us that reaching ‘hidden’ carers for example
those from black and minority ethnic communities
and working carers is essential if we are to hear
the broadest view possible. Financial support and
having a break help to contribute to your health
and well-being. These messages are reinforced by
national research, e.g. Carers UK.
There is a perceived lack of success in engaging
with ‘hidden carers’. We know from research
(Carers UK) that many carers are ‘hidden’ because
they come from a particular ethnic group, traveller
or refugee community. Belong to a particular age
group, for example young carers and working
carers. Carers who have a disability themselves,
GLBT (gay, lesbian, bi-sexual and trans-gendered)
carers and carers supporting someone who
misuses drugs and alcohol as well as carers on a
low income.
We must make efforts to ensure that we reach
these ‘hidden’ groups through targeted activities
and support.
Page 9

8
OUR DELIVERY ARRANGEMENTS
Organisations in which carers are a main user group are invited to use this action plan to inform their
own direction of travel. Organisations in which carers are not the main focus of activity may choose to
use this action plan to help them to embed the needs of carers within their organisational structures. The
Carers Strategic Action Plan will be delivered using the following principles:
• Carer-led, identifying and including all carers from all sections of the community in Newcastle.
• Maximum co-ordination between organisations to promote collaborative practice and ensure best
value for money.
• A real focus on the outcomes carers want to see in The 7 Outcomes identified by Our Health, Our
care, Our Say White Paper (2006) which are embedded within Newcastle’s Sustainable
Community Strategy and the outcomes from the National Carers Strategy 2008.
• This action plan will demonstrate where progress is, or is not, being made and what actions will
be taken to improve the position.
• Ensuring that carers are not seen as a ‘bolt-on’ issue put part of the public sector’s core business.
Such that the needs of carers become everyone’s business.
• Ensuring carers are not seen as a health and social care issue only but are fully acknowledged in
policies around Equality and Diversity, Social Inclusion, Economic Development and prosperity,
employment, leisure and community development.
• Carry out equality impact needs assessments to ensure that no specific group of carers are
excluded from benefiting from this action plan.
There will be five delivery groups, each with a specific focus to improve on our shared outcomes:
• Learning and work
• Health and well-being
• Information
• Breaks and Leisure
• Voice and choice
We will use outcome indicators (a measure which helps quantify the achievement of an outcome) to
help us recognise if we are getting it right. For example, in relation to Economic Wellbeing (page 30),
Page 10

9
action 5 states ‘access swift benefit calculations for carers, provided by a range of agencies’; we could
use the number of carers taking up carers’ premium, linked to pension credit and the number of carers
qualifying for carers’ allowance. If there is an increase in uptake of benefits then this is progress. What
you tell us is a measure of success, from surveys of your experience and for example attending any
consultation events or carer’s forums.
We will use performance measures to tell us how well service providers are working and that includes all
partners in this multi-agency strategy; by asking:
• How much did they do? (quantity), for example numbers of new carers using the service & range
of services provided
• How well did they do it? (quality), for example carer satisfaction surveys
• Is anyone better off as a result? Finding out what has improved for carers as a result of using
their service?
Page 11

Ca
rers
are
he
alt
hy
Ou
tcom
es: C
are
rs w
ill h
ave
he
alth
y life
sty
les a
nd
avo
id r
isky b
eh
avio
urs
C
are
rs a
re p
hysic
ally
he
alth
y
C
are
rs a
re m
en
tally
an
d e
mo
tion
ally
he
alth
y a
nd c
an d
ea
l w
ith
sig
nific
an
t lif
e c
ha
nge
s a
nd
ch
alle
nge
s
C
are
rs h
ave
he
lp t
o p
reve
nt
ill-h
ea
lth
an
d lo
ng t
erm
ca
re n
ee
ds
C
are
rs h
ave
exce
llen
t qu
alit
y t
rea
tme
nt a
nd
ca
re if
need
ed
Ke
y p
art
ne
rs: P
rim
ary
Ca
re T
rust/
Em
erg
ing G
P C
on
so
rtia
, N
TW
, A
du
lt &
Cu
ltu
re S
erv
ice
s,
Vo
lun
tary
& C
om
mu
nity S
ecto
r
De
live
ry G
rou
p:
He
alth &
We
llbe
ing
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By
wh
en
?
Wh
at
we a
lre
ad
y d
o/
kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t th
ere
?
1.
Pro
mo
te g
ood
ph
ysic
al &
me
nta
l he
alth
Prim
ary
Ca
re
Tru
st/E
me
rgin
g
GP
co
nso
rtia
De
ve
lop
he
alth
ch
ecks in
Ne
wca
stle
,
focu
s u
pon
ea
rly
inte
rve
ntio
n &
pre
ve
ntio
n o
f ill
he
alth
He
alth
ch
ecks
in p
lace
by e
nd
20
11
NH
S N
ort
h o
f T
yn
e h
eld
hea
lth
scre
en
ing p
ilots
fo
r ca
rers
in
No
rth
um
be
rlan
d w
ith
po
sitiv
e
ou
tcom
es
Ma
cm
illa
n h
ea
lth
an
d w
ellb
ein
g
ch
ecks
Diffe
ren
t str
oke
s c
vs p
rovid
es
he
alth
scre
en
ing f
or
patie
nts
an
d
Fe
we
r ca
rers
rep
ort
ing p
oo
r h
ea
lth
ba
sed
on J
SN
A d
ata
Page 12

11
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By
wh
en
?
Wh
at
we a
lre
ad
y d
o/
kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t th
ere
?
ca
rers
2.
Re
du
ce
th
e %
of
ca
rers
rep
ort
ing p
oo
r
he
alth
as
ind
ica
ted
in
JS
NA
data
PC
T/G
P
Co
nso
rtia
, N
HS
Tru
sts
De
ve
lop
acce
ssib
le
prim
ary
& s
eco
nd
ary
ca
re h
ea
lth
se
rvic
es
tha
t fu
lly u
nd
ers
tan
d
the
ne
ed
s o
f ca
rers
Ca
rers
are
reco
gn
ise
d d
urin
g
ho
sp
ita
l p
ha
se
&
dis
ch
arg
e p
lan
nin
g
20
11
JS
NA
da
ta
revie
we
d
an
nu
ally
RC
GP
’s s
en
t o
ut
‘su
ppo
rtin
g
ca
rers
’ a
re
sou
rce
& tra
inin
g p
ack
to a
ll G
P’s
in
En
gla
nd
Ca
rers
re
po
rtin
g
imp
rove
d h
ea
lth a
nd
we
ll-b
ein
g
3.P
rovid
e
em
otio
na
l
su
ppo
rt t
o c
are
rs
GP
Co
nso
rtia
&
Ad
ult,
Cu
ltu
re
se
rvic
es &
VC
S
org
an
isa
tio
ns
Ca
rers
to
acce
ss
IAP
T N
HS
in
itia
tive
(in
cre
asin
g a
cce
ss to
psych
olo
gic
al
the
rap
ies)
Re
vie
w
20
13
Ma
ny v
olu
nta
ry o
rga
nis
atio
ns
pro
vid
e e
ffe
ctive
em
otio
na
l
su
ppo
rt t
o c
are
rs.
NT
W e
mp
loy s
pe
cia
list ca
rers
su
ppo
rt n
urs
e f
or
old
er
pe
op
les’
se
rvic
es
NH
S N
ort
h o
f T
yn
e e
mp
loy
Ad
mira
l N
urs
es t
o s
upp
ort
ca
rers
of
pe
op
le w
ith
De
men
tia
& S
tro
ke
Se
lf r
epo
rtin
g
imp
rove
d s
tate
s o
f
em
otio
na
l w
ellb
ein
g
Page 13

12
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By
wh
en
?
Wh
at
we a
lre
ad
y d
o/
kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t th
ere
?
Info
rma
tion
/ad
vis
or
posts
4.
Pro
vid
e
op
po
rtu
nitie
s f
or
ca
rers
to
ta
ke
pa
rt in
ph
ysic
al
exe
rcis
e
NC
C,
Le
isu
re
Se
rvic
es/N
HS
Tru
sts
/hea
lth
pro
mo
tio
n
age
ncie
s,
Ad
ult
Se
rvic
es
Work
with
th
e
He
alth
y L
ife
sty
le
Bo
ard
& A
ctive
Ne
wca
stle
to
ena
ble
ca
rers
to
ta
ke
pa
rt in
ph
ysic
al e
xe
rcis
e
Re
vie
w
20
13
Le
isu
re C
ard
off
ers
re
du
ce
d
ad
mis
sio
n to
Ne
wca
stle
’s L
eis
ure
facili
tie
s.
Nu
mbe
r of
ca
rers
sig
nin
g u
p f
or
‘leis
ure
pa
sse
s’ w
elln
ess
ce
ntr
es
5.
Exp
and
em
erg
en
cy &
crisis
co
ve
r
wh
ich
is p
lan
ned
,
acce
ssib
le &
relia
ble
Ad
ult &
Cu
ltu
re
Se
rvic
es
De
ve
lop
Em
erg
en
cy
Ca
rd S
che
me
in
co
nju
nctio
n w
ith
British
Re
d C
ross
La
un
ch
Ja
n
20
11
Em
erg
en
cy p
lann
ing is p
art
of
the
ca
rers
’ a
sse
ssm
ent
pro
ce
ss
Sch
em
e la
un
ch
ed
an
d a
ctive
ly u
se
d b
y
ca
rers
Page 14

Ca
rers
ha
ve
a g
oo
d q
ua
lity
of
life
Ou
tcom
es: C
are
rs h
ave
frie
nd
s, fa
mily
an
d s
up
po
rt n
etw
ork
s
Ca
rers
ca
n g
et
ou
t a
nd
ab
out
ea
sily
Ca
rers
en
joy c
rea
tive
, cu
ltu
ral, s
po
rtin
g a
nd
le
isu
re a
ctivitie
s
Ke
y p
art
ne
rs: A
du
lt &
Cu
ltu
re S
erv
ice
s,
Ch
ildre
n’s
Se
rvic
es,
PC
T/G
P C
on
so
rtia
, N
CC
Le
isu
re S
erv
ice
s,
NT
W, V
CS
& H
ea
lth
Pro
motio
n A
ge
ncie
s.
De
live
ry G
rou
p:
Bre
aks &
Le
isu
re
Ac
tio
n
Le
ad
Pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t
the
re?
1.C
are
r re
ce
ive
a
‘ho
listic’ ca
rers
asse
ssm
en
t th
at
ide
ntifie
s h
ow
th
ey
ca
n b
e s
up
po
rte
d
with
in a
nd
ou
tsid
e
the
ir c
arin
g r
ole
Ad
ult &
Cu
ltu
re
Se
rvic
e
To in
cre
ase t
he
qu
antity
an
d
qu
alit
y o
f ca
rers
asse
ssm
ents
en
su
rin
g t
he
y a
re p
ers
on
-
ce
ntr
ed &
fo
cu
se
d o
n p
ositiv
e
ou
tcom
es f
or
ca
rers
Re
vie
w
pro
gre
ss
Ap
ril 2
011
Ad
ult &
Cu
ltu
re
Se
rvic
es h
as a
de
dic
ate
d
ca
rers
’ so
cia
l
wo
rk t
ea
m
The
re w
ill b
e a
n
incre
ase
in t
he
nu
mb
ers
of
ca
rers
rece
ivin
g a
n
asse
ssm
en
t
Mo
nito
r ho
w c
are
rs
are
ma
de
aw
are
of
the
ir r
igh
t to
an
Page 15

14
Ac
tio
n
Le
ad
Pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t
the
re?
asse
ssm
en
t
2.R
ais
e a
wa
ren
ess
of
the
so
cia
l ca
re
wo
rkfo
rce
of
the
ne
ed
s o
f ca
rers
, a
s
‘pa
rtn
ers
in
ca
re’
Ad
ult &
Cu
ltu
re
Se
rvic
es /
vo
lun
tary
org
an
isa
tio
ns
De
ve
lop
tra
inin
g c
ou
rse
s f
or
so
cia
l w
ork
/so
cia
l ca
re s
taff
aro
und
a ‘co
mp
reh
en
siv
e’
mo
de
l of
ca
rer
sup
po
rt;
inclu
din
g t
he e
ssen
tia
l n
atu
re
of
‘th
ink f
am
ily’ in
re
latio
n to
ide
ntify
ing c
hild
ren
& y
ou
ng
pe
op
le in
ca
rin
g r
ole
s
Re
vie
w
en
d 2
011
De
dic
ate
d
ca
rers
so
cia
l
wo
rk t
ea
m
Ca
rers
ne
ed
s
take
n a
ccou
nt of
du
rin
g s
erv
ice
use
r’s
asse
ssm
en
t
An
in
cre
ase
in
th
e
nu
mb
ers
of
ca
rers
asse
ssm
en
ts
co
mp
lete
d
Ca
rers
re
po
rtin
g
the
asse
ssm
ent
pro
ce
ss b
eneficia
l
in h
elp
ing th
em
ach
ieve
ca
re/life
ba
lan
ce
3. T
o d
eve
lop
inn
ova
tive
sh
ort
bre
aks s
erv
ice
fo
r
ca
rers
NH
S N
ort
h o
f T
yn
e
Prim
ary
Ca
re T
rust
NH
S N
ort
h o
f T
yn
e S
tra
tegic
pla
n h
as s
et
targ
et fo
r 9
5%
of
all
‘asse
sse
d’ ca
rers
to
rece
ive
su
pp
ort
or
sho
rt b
rea
k
20
14
C
are
rs r
ece
ive
resp
ite
bre
aks
as ‘b
y-p
rod
uct’
of
the
ca
red
-fo
r
su
ppo
rt p
lan
An
in
cre
ase
in
th
e
nu
mb
ers
of
bre
aks
ca
rers
re
ce
ive
4.D
eve
lop
pe
rso
na
lise
d
Ad
ult &
Cu
ltu
re
De
ve
lop
dire
ct
pa
ym
ents
fo
r
ca
rers
to
en
ab
le g
rea
ter
20
12
C
are
rs c
an
ap
ply
to
th
e
The
cre
atio
n o
f
ind
ivid
ua
l b
ud
ge
ts
Page 16

15
Ac
tio
n
Le
ad
Pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w
wh
en
we
ge
t
the
re?
se
rvic
es f
or
ca
rers
S
erv
ice
fle
xib
ility
& c
ho
ice
of
wh
at
co
nstitu
tes a
bre
ak
Co
nsid
er
oth
er
pe
rso
na
lise
d
op
tion
s f
or
exa
mp
le v
ou
ch
er
sch
em
es &
ca
sh p
aym
en
ts
Assis
tan
ce &
tra
inin
g f
und
fo
r
su
ppo
rt in
th
eir
ca
rin
g r
ole
Ma
ny e
xa
mp
les
of
go
od p
ractice
na
tion
ally
, fo
r
exa
mp
le ‘m
y
tim
e’ vo
uche
rs
for
ca
rers
5.
Sup
po
rtin
g c
are
rs
thro
ugh
cha
nge
an
d
tra
nsitio
ns. T
his
inclu
de
s y
ou
ng
ad
ult c
are
rs 1
8-2
5
Ad
ult &
Cu
ltu
re
Se
rvic
es,
Ch
ildre
n’s
Se
rvic
es &
VC
S
De
ve
lop
a s
pe
cific
‘tr
an
sitio
n’
gro
up
fo
r ca
rers
wh
o a
re n
o
lon
ge
r a
ctive
ly c
arin
g,
inclu
din
g f
orm
er
ca
rers
.
De
ve
lop
a s
pe
cific
se
rvic
e t
o
ma
na
ge
the
tra
nsitio
n fro
m
yo
un
g c
are
r to
yo
un
g a
du
lt
ca
rer
Esta
blis
h
tra
nsitio
n
gro
up
by
en
d 2
012
So
me
VC
S
pa
rtn
ers
su
ppo
rt
ca
rers
th
rou
gh
tra
nsitio
na
l lif
e
sta
ge
s.
An
in
cre
ase
in
th
e
nu
mb
ers
of
yo
un
g
ad
ult c
are
rs
ide
ntified
by
age
ncie
s
An
in
cre
ase
in
ca
rers
re
po
rtin
g
red
uced
str
ess
leve
ls d
ue
to
att
en
din
g
tra
nsitio
n/n
ext
ste
p
Page 17

16
Page 18

17
Ca
rers
ma
ke
a p
os
itiv
e c
on
trib
uti
on
Ou
tcom
es: C
are
rs a
re in
form
ed
an
d e
mp
ow
ere
d to
sha
pe t
he f
utu
re o
f N
ew
ca
stle
and
its
ne
igh
bo
urh
oo
ds
Ke
y p
art
ne
rs: A
du
lt &
Cu
ltu
re S
erv
ice
s,
PC
T/G
P C
on
so
rtia
, N
HS
Tru
sts
, A
du
lt E
du
ca
tio
n, V
CS
De
live
ry G
rou
p:
Vo
ice a
nd
Ch
oic
e
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
1.I
nd
ivid
ua
l
ca
rers
are
reco
gn
ise
d a
s
exp
ert
s in
the
ir
ca
rin
g r
ole
an
d
are
co
nsu
lted
an
d in
vo
lve
d in
ca
re p
lan
s f
or
the
pe
rso
n(s
)
the
y c
are
fo
r
an
d in
the
ir o
wn
Ad
ult &
Cu
ltu
re
Se
rvic
es,
NH
S
Tru
sts
, G
P’s
&
vo
lun
tary
org
an
isa
tio
ns
All
su
ppo
rt
pla
ns,
ca
re
pla
ns; p
acka
ge
s
of
ca
re,
me
dic
al/n
urs
ing
no
tes w
ill r
efle
ct
the
ca
rer’s
pe
rsp
ective
,
inclu
din
g t
he
vie
ws o
f a y
ou
ng
Re
vie
w e
nd
20
11
Ca
rers
vie
ws a
nd
wis
he
s a
re
so
ugh
t a
s p
art
of
the
se
rvic
e u
se
r’s
agre
em
en
t
Incre
ase in
nu
mb
er
of
ca
rers
de
tails
on
Ca
re F
irst
da
taba
se
Page 19

18
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
asse
ssm
en
t ca
rer.
2.I
nvo
lve
ca
rers
in t
he
co
mm
issio
nin
g
pro
ce
ss to
en
su
re th
eir
vie
ws in
flu
en
ce
se
rvic
e
de
ve
lop
me
nts
All
age
ncie
s w
ith
co
mm
issio
nin
g
resp
on
sib
ilitie
s
Ca
rers
giv
en
th
e
op
po
rtu
nity b
y
co
mm
issio
nin
g
team
s t
o
pa
rtic
ipa
te in
the
ir s
tra
tegic
pla
nn
ing
Re
vie
w e
nd
20
12
The
re is
evid
en
ce
of
go
od
pra
ctice
in
oth
er
regio
ns o
f ca
rers
info
rmin
g t
he
co
mm
issio
nin
g
pro
ce
ss
Nu
mbe
r of
ca
rers
wh
o f
ee
l th
eir
vie
ws s
ha
pe
d th
e
co
mm
issio
nin
g p
roce
ss
3.O
rga
nis
ation
s
to s
up
po
rt
pe
op
le t
o
reco
gn
ise
the
y
ma
y b
e c
are
rs
VC
S o
rga
nis
ation
to t
ake
lea
d w
ith
su
ppo
rt o
f a
ll
pa
rtn
ers
De
ve
lop
inn
ova
tive
wa
ys
for
ca
rers
to
se
lf-ide
ntify
, e
.g.
ad
ve
rtis
ing o
n
ph
arm
acy b
ags
Re
vie
w e
nd
20
13
The
re is lo
ts o
f
go
od
wo
rk g
oin
g
on
to
he
lp c
are
rs
se
lf-ide
ntify
–
e.g
. N
ort
h W
est
Re
gio
n
An
in
cre
ase
in
th
e n
um
be
rs o
f
ca
rers
re
gis
terin
g w
ith
pa
rtn
er
age
ncie
s,
su
ch
as C
are
rs
Ce
ntr
e &
oth
ers
5.
De
ve
lopm
ent
of
rep
rese
nta
tive
ca
rers
ba
se
Ad
ult &
Cu
ltu
re
Se
rvic
es
Ca
rers
Le
ad
is
de
ve
lop
ing a
‘ma
p’ of
org
an
isa
tio
ns
Esta
blis
h
rep
rese
nta
tive
foru
m b
y e
nd
Ca
rers
fo
rum
’s
exis
t in
ma
ny
form
s a
cro
ss t
he
co
un
ty a
nd
An
esta
blis
he
d c
are
r’s f
oru
m
me
etin
g r
egu
larly w
ith
a b
road
mem
be
rsh
ip o
f ca
rers
fro
m a
ll
se
ctio
ns o
f th
e c
arin
g
Page 20

19
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
from
wh
ich
to
he
ar
a
‘co
llective
’ ca
rer
vo
ice
rep
rese
ntin
g
ca
rers
fro
m a
ll
se
ctio
ns o
f th
e
co
mm
un
ity;
from
wh
ich
to
de
ve
lop
a r
ep
rese
nta
tive
ca
rers
fo
rum
20
11
e
vid
en
ce
go
od
pra
ctice
in
rela
tio
n to
invo
lve
me
nt &
pa
rtic
ipa
tion
co
mm
un
ity.
Page 21

20
Ca
rers
ex
erc
ise
ch
oic
e a
nd
co
ntr
ol
Ou
tcom
es: C
are
rs a
re w
ell
info
rmed
ab
ou
t serv
ice
s,
activitie
s a
nd
op
po
rtun
itie
s
Ca
rers
of
all
ba
ckgro
un
ds a
re info
rme
d a
nd
em
po
we
red
to
en
ga
ge
in
de
cis
ion
ma
kin
g a
bo
ut
the
ir liv
es
Ca
rers
are
in
co
ntr
ol of
the s
erv
ice
s t
he
y w
an
t so
th
ey c
an
liv
e t
he
life
th
ey w
an
t
Ke
y p
art
ne
rs: A
ll p
art
ne
rs a
cro
ss a
ll se
cto
rs
De
live
ry G
rou
p:
Vo
ice a
nd
Ch
oic
e
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
wh
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
1.
De
ve
lop
ing a
ca
rer
co
nscio
us
co
mm
un
ity
Ad
ult &
Cu
ltu
re
Se
rvic
es w
ith
su
ppo
rt o
f a
ll
pa
rtn
ers
En
co
ura
ge
th
e
de
ve
lop
me
nt of
‘ca
rer
ch
am
pio
ns’
acro
ss a
ll
se
cto
rs,
so t
ha
t
ca
rers
be
com
e
ma
instr
eam
ed
Re
vie
w e
nd
20
11
Evid
en
ce
of
go
od
pra
ctice
in
oth
er
regio
ns o
f ‘c
are
r
ch
am
pio
ns’
acro
ss
pu
blic
/priva
te &
vcs s
ecto
rs
De
dic
ate
d m
em
be
r of
sta
ff in
ea
ch
pa
rtne
r o
rga
nis
atio
n
ch
am
pio
nin
g c
are
rs r
igh
ts
Invo
lve
me
nt
of
pu
blic
an
d
priva
te s
ecto
rs in
en
gagin
g
with
ca
rers
issu
es
2.E
nsu
re c
are
rs
Ad
ult &
Cu
ltu
re
Use
Th
e
Re
vie
w e
nd
N
ew
ca
stle
A
re
du
ctio
n in t
he
nu
mb
er
of
Page 22

21
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
wh
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
acce
ss to
se
rvic
es a
re f
air
& t
he
y a
re
safe
gu
ard
ed
from
ab
use
an
d
su
ppo
rte
d to
pro
vid
e c
are
tha
t is
safe
Se
rvic
es w
ith
su
ppo
rt o
f a
ll
pa
rtn
ers
Pe
rfo
rma
nce
Asse
ssm
en
t
Gu
ide
an
d T
he
Ou
tcom
es
Fra
me
wo
rk
(20
08
/09
) a
s a
gu
ide
to
en
su
re
go
od
pra
ctice
&
Equ
alit
ies A
ct
20
10
.
Co
mp
lem
en
t th
e
wo
rk o
f th
e
Safe
gu
ard
ing
Ad
ults S
tra
tegic
Bo
ard
20
12
S
afe
gu
ard
ing
Ad
ults S
tra
tegic
Bo
ard
ha
s r
ob
ust
pro
ce
du
res &
pra
ctice
s in
pla
ce
.
safe
gu
ard
ing a
lert
s.
3.
Co
nsid
er
the
ne
ed
s o
f o
lde
r
ca
rers
,
pa
rtic
ula
rly
tho
se w
ho
are
‘mu
tua
lly
Ad
ult &
Cu
ltu
re
Se
rvic
es,
NT
W &
vo
lun
tary
se
cto
r
pa
rtn
ers
De
ve
lop
sp
ecific
‘pla
nn
ing’
se
rvic
e a
rou
nd
the
ne
ed
s o
f
old
er
ca
rers
&
the
ir f
utu
res &
the
fu
ture
of
the
Re
vie
w e
nd
20
12
LD
PB
ha
s fa
mily
& c
are
rs t
hem
ed
gro
up
& b
rid
gin
g
do
c ‘S
up
po
rtin
g
LD
PB
’s t
o
imp
lem
ent
Na
tio
na
l C
are
rs
Fe
ed
ba
ck f
rom
old
er
ca
rers
tha
t p
lan
s a
re in p
lace
fo
r th
e
futu
re o
f th
eir lo
ve
d o
ne
Page 23
22
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
wh
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
ca
rin
g’
pe
op
le t
he
y c
are
for
com
ple
men
t
the
wo
rk o
f th
e
LD
Str
ate
gic
Pa
rtn
ers
hip
Bo
ard
Str
ate
gy’
Page 24

23
Ca
rers
are
fre
e f
rom
dis
cri
min
ati
on
an
d h
ara
ss
me
nt
Ou
tcom
es: C
are
rs h
ave
fa
ir a
nd
equ
al a
cce
ss t
o p
lace
s, b
uild
ings, se
rvic
es a
nd
op
po
rtu
nitie
s
Ke
y p
art
ne
rs: A
du
lt &
Cu
ltu
re S
erv
ice
s,
VC
S,
NH
S T
rusts
, E
mp
loye
rs f
oru
m
De
live
ry G
rou
p:
Info
rma
tio
n
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
1.
Sup
po
rt t
o
sta
ff to
wo
rk
em
pa
thic
ally
with
ca
rers
&
vie
w t
he
m a
s
‘co
-wo
rke
rs’.
Ad
ult &
Cu
ltu
re
Se
rvic
es &
All
pa
rtn
ers
De
ve
lop
mu
lti-
age
ncy t
rain
ing
co
urs
e fo
r sta
ff
usin
g a
co
mp
reh
en
siv
e
mo
de
l of
ca
rer
su
ppo
rt
Re
vie
w e
nd
20
11
Eff
ective
so
cia
l
wo
rk p
ractice
take
s a
ho
listic
ap
pro
ach
to
co
mm
un
ity c
are
asse
ssm
en
ts
an
d ta
ke
s
acco
un
t of
the
ca
rers
’
pe
rsp
ective
Ca
rers
re
po
rtin
g a
n in
cre
ase
d
se
nse
of
pa
rtic
ipa
tio
n a
nd
inclu
sio
n in
th
e s
erv
ice
use
r
asse
ssm
en
t p
roce
ss
3.
Equ
ity o
f
acce
ss,
loca
tin
g
Ad
ult &
Cu
ltu
re
De
ve
lop
gre
ate
r
links w
th V
CS
Re
vie
w e
nd
A
nge
lou
Cen
tre
su
cce
ssfu
lly b
id
An
in
cre
ase
in
th
e n
um
be
r of
ca
rers
id
en
tifie
d f
rom
BM
E
Page 25

24
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t w
e
alr
ea
dy
do
/kn
ow
th
at
wo
rks
well
Ho
w w
ill w
e k
no
w w
he
n w
e
ge
t th
ere
?
ca
rers
fro
m
hid
den
gro
up
s,
as id
en
tifie
d in
se
ttin
g t
he
sce
ne
Se
rvic
es,
VC
S
org
an
isa
tio
ns
rep
rese
ntin
g
‘hid
de
n c
are
rs’
gro
up
s
De
ve
lop
ne
ed
s
an
aly
sis
20
12
fo
r U
De
cid
e
fun
din
g t
o
ide
ntify
bla
ck
wo
me
n c
are
rs
co
mm
un
itie
s,
gre
ate
r
pa
rtic
ipa
tion
of
wo
rkin
g
ca
rers
, yo
un
g a
du
lt c
are
rs
ide
ntified
4.
Ca
rers
will
ha
ve
acce
ss to
go
od
qu
alit
y
info
rma
tio
n to
he
lp th
em
to
ma
ke info
rmed
de
cis
ion
s
Ad
ult &
Cu
ltu
re
Se
rvic
es,
NT
W,
NH
S T
rusts
&
vo
lun
tary
se
cto
r
pro
vid
ers
De
ve
lop
w
ays in
wh
ich
in
form
ation
is p
rovid
ed
to
ca
rers
in
a r
an
ge
of
form
ats
, e
.g.
on
lin
e, W
eb
ca
sts
an
d c
ha
t
roo
m a
nd
acce
ssib
le
form
ats
, e.g
.
diffe
rent
lan
gu
age
s &
larg
e p
rin
t
Re
vie
w e
nd
20
11
Ca
rer’s
Info
rma
tion
bo
okle
t p
rod
uced
by A
du
lt &
Cu
ltu
re S
erv
ice
s
& C
are
rs
Info
rma
tion
we
bsite
ru
n b
y
NT
W, V
CS
pa
rtn
ers
pro
vid
e
ran
ge
of
info
rma
tio
n in
diffe
rent fo
rma
ts
for
ca
rers
Ca
rers
co
mp
limen
tin
g
se
rvic
es o
n q
ua
lity o
f
info
rma
tio
n
Page 26

25
Ca
rers
ha
ve
ec
on
om
ic w
ellb
ein
g
Ou
tcom
es: C
are
rs a
re e
nga
ge
d in
em
plo
ym
en
t, e
du
ca
tio
n o
r tr
ain
ing
Ca
rers
ha
ve
skill
s a
nd
kn
ow
led
ge
re
leva
nt
to c
urr
en
t a
nd
fu
ture
job
ma
rke
t
Ca
rers
are
fre
e f
rom
po
ve
rty a
nd
its
im
pa
ct
Ke
y p
art
ne
rs:
Jo
b C
en
tre
Plu
s,
Ad
ult E
du
ca
tion
, F
urt
he
r E
du
ca
tion
Co
llege
s, W
elfa
re R
igh
ts S
erv
ice
, V
olu
nta
ry
& C
om
mun
ity S
ecto
r, C
ha
mb
er
of
Com
me
rce
De
live
ry G
rou
p:
Lea
rnin
g a
nd
Work
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t d
o w
e
alr
ea
dy
do
/kn
ow
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
1.
Assis
t ca
rers
& e
x-c
are
rs in
to
em
plo
ym
en
t,
off
erin
g a
dvic
e
& g
uid
an
ce
on
vo
ca
tio
na
l
tra
inin
g &
so
urc
es o
f
Jo
b C
en
tre
Plu
s
& A
du
lt &
Cu
ltu
re
Se
rvic
es
Ra
ise
the
pro
file
of
Skill
s a
ccou
nts
& t
he w
ork
of
Ca
re P
art
ne
rsh
ip
Ma
na
ge
rs w
ith
DW
P
Re
vie
w e
nd
20
11
So
me
VC
S
org
an
isa
tio
n
ha
ve
exa
mp
les
of
go
od p
ractice
loca
lly
An
in
cre
ase
in
the
num
be
rs o
f
ca
rers
in
em
plo
ym
en
t
Page 27

26
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t d
o w
e
alr
ea
dy
do
/kn
ow
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
fun
din
g
2. W
ork
with
em
plo
ye
rs t
o
de
ve
lop
po
licie
s a
nd
pra
ctice
s th
at
su
ppo
rt c
are
rs
into
an
d
alre
ad
y in
wo
rk
JC
P,
De
pt. W
ork
& P
en
sio
ns &
Ad
ult &
Cu
ltu
re
Se
rvic
es
Ma
ke
lin
ks w
ith
loca
l ch
am
be
r of
co
mm
erc
e,
NC
VS
and
pub
lic
se
cto
r
org
an
isa
tio
ns to
ma
instr
eam
the
ca
rer
age
nda
Re
vie
w e
nd
20
11
Na
tio
na
l ‘T
op
10
0 E
mp
loye
rs
for
ca
rers
’
Ca
rers
Le
ad
Off
ice
r p
rese
nte
d
to C
orp
ora
te
Equ
alit
y G
rou
p t
o
rais
e c
are
rs a
s
‘pro
tecte
d’ gro
up
Nu
mbe
r of
ca
rers
in
em
plo
ym
en
t,
ca
rer
po
licie
s
de
ve
lop
ed a
nd
imp
lem
ente
d
Le
agu
e ta
ble
of
top
em
plo
ye
rs
for
ca
rers
3.
En
co
ura
ge
em
plo
ye
rs t
o
join
Ca
rers
UK
‘Em
plo
ye
rs f
or
ca
rers
’
fed
era
tio
n
Vo
lun
tary
se
cto
r
pa
rtn
ers
, JC
P,
Lo
ca
l e
mp
loye
r
foru
ms w
ith
su
ppo
rt o
f a
ll
pa
rtn
ers
De
ve
lop
gu
ide
alo
ng t
he lin
es o
f
Ca
rers
UK
‘Em
plo
ye
rs f
or
Ca
rers
’ fo
rum
Re
vie
w e
nd
20
12
Ca
rers
UK
‘Em
plo
ye
rs f
or
ca
rers
’ fe
de
ratio
n
of
pu
blic
&
priva
te
org
an
isa
tio
n
An
in
cre
ase
in
em
plo
ye
rs
de
ve
lop
ing
ca
rers
frie
nd
ly
wo
rk p
ractice
s
4.
De
ve
lop
tra
inin
g c
ou
rse
s
for
ca
rers
to
assis
t th
em
Vo
lun
tary
se
cto
r
pa
rtn
ers
, e
.g.
Ca
rers
Ce
ntr
e,
JC
P,
Lo
ca
l
Ide
ntify
sp
ecific
tra
inin
g
pro
vid
ers
/co
urs
es
for
exa
mp
le
Re
vie
w e
nd
20
11
Le
arn
ing L
inks,
An
ge
lou
Cen
tre
,
City &
Gu
ilds,
OU
an
d o
the
r
Nu
mbe
rs
att
en
din
g
tra
inin
g c
ou
rse
s
Page 28

27
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
imp
rove
me
nt
By w
he
n?
W
ha
t d
o w
e
alr
ea
dy
do
/kn
ow
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
tow
ard
s
em
plo
ym
en
t
Tra
inin
g
pro
vid
ers
e.g
.
F.E
. co
llege
s
pe
rso
na
l
de
ve
lop
me
nt
skill
s/C
V b
uild
er
etc
VC
S
org
an
isa
tio
ns
Ou
tcom
es
me
asu
red in
term
s o
f jo
bs,
vo
lun
tary
wo
rk
etc
5.
Acce
ss t
o
sw
ift
be
nefit
ca
lcu
latio
ns f
or
ca
rers
,
pro
vid
ed
by
ran
ge
of
age
ncie
s
Welfa
re R
igh
ts
Se
rvic
e,
Vo
lun
tary
org
an
isa
tio
ns,
Ne
wca
stle
Fin
an
cia
l
Inclu
sio
n
Pa
rtn
ers
hip
De
ve
lop
acce
ss
to c
om
pre
he
nsiv
e
mo
ne
y &
ben
efits
ad
vic
e f
or
ca
rers
Ma
ke
lin
ks w
ith
Ne
wca
stle
Fin
an
cia
l
Inclu
sio
n
pa
rtn
ers
hip
Re
vie
w e
nd
20
12
Ad
ult &
Cu
ltu
re
se
rvic
es h
as
de
dic
ate
d
Welfa
re B
en
efits
Tim
ely
be
nefit
ch
ecks
Page 29
28
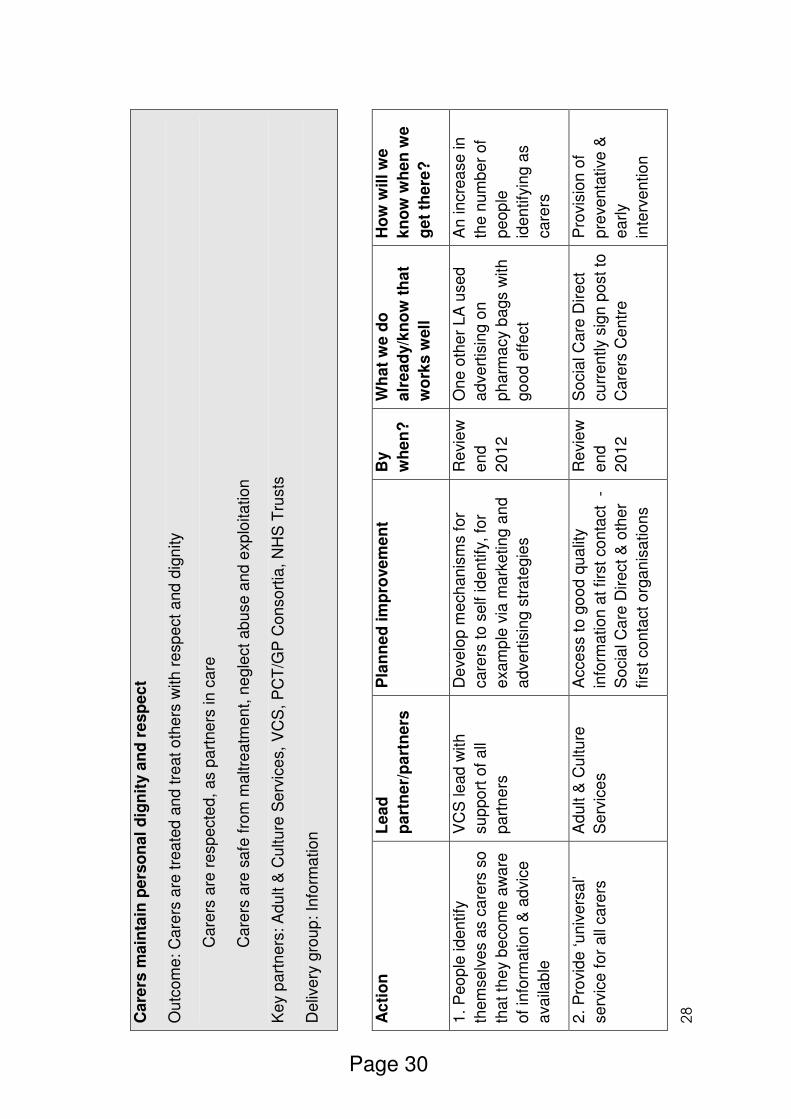
Ca
rers
ma
inta
in p
ers
on
al
dig
nit
y a
nd
re
sp
ec
t
Ou
tcom
e: C
are
rs a
re tre
ate
d a
nd
tre
at o
the
rs w
ith
re
sp
ect
and
dig
nity
C
are
rs a
re r
esp
ecte
d, a
s p
art
ne
rs in
ca
re
C
are
rs a
re s
afe
fro
m m
altre
atm
en
t, n
egle
ct
ab
use a
nd
exp
loita
tion
Ke
y p
art
ne
rs: A
du
lt &
Cu
ltu
re S
erv
ice
s,
VC
S,
PC
T/G
P C
on
so
rtia
, N
HS
Tru
sts
De
live
ry g
rou
p:
Info
rma
tio
n
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By
wh
en
?
Wh
at
we d
o
alr
ea
dy/k
no
w t
ha
t
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
1.
Peo
ple
id
en
tify
them
se
lve
s a
s c
are
rs s
o
tha
t th
ey b
eco
me
aw
are
of
info
rmatio
n &
ad
vic
e
ava
ilab
le
VC
S le
ad
with
su
ppo
rt o
f a
ll
pa
rtn
ers
De
ve
lop
me
ch
an
ism
s fo
r
ca
rers
to
se
lf id
en
tify
, fo
r
exa
mp
le v
ia m
ark
etin
g a
nd
ad
ve
rtis
ing s
tra
tegie
s
Re
vie
w
en
d
20
12
On
e o
the
r L
A u
se
d
ad
ve
rtis
ing o
n
ph
arm
acy b
ags w
ith
go
od
eff
ect
An
in
cre
ase
in
the
num
be
r of
pe
op
le
ide
ntify
ing a
s
ca
rers
2.
Pro
vid
e ‘u
niv
ers
al’
se
rvic
e f
or
all
ca
rers
Ad
ult &
Cu
ltu
re
Se
rvic
es
Acce
ss t
o g
oo
d q
ua
lity
info
rma
tio
n a
t firs
t co
nta
ct
-
So
cia
l C
are
Dire
ct &
oth
er
firs
t con
tact
org
an
isa
tio
ns
Re
vie
w
en
d
20
12
So
cia
l C
are
Dire
ct
cu
rre
ntly s
ign
po
st
to
Ca
rers
Ce
ntr
e
Pro
vis
ion
of
pre
ve
nta
tive
&
ea
rly
inte
rve
ntio
n
Page 30

29
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By
wh
en
?
Wh
at
we d
o
alr
ea
dy/k
no
w t
ha
t
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
se
rvic
e
4.
Pro
vid
e info
rmatio
n to
ca
rers
in
a r
an
ge
of
form
ats
Ad
ult &
Cu
ltu
re
Se
rvic
es
De
ve
lop
de
dic
ate
d c
are
r
pa
ge
s o
n N
CC
we
bsite
Webca
st fu
ture
ca
rer
co
nfe
ren
ce
s to
en
ab
le
wo
rkin
g c
are
rs t
o p
art
icip
ate
Re
vie
w
en
d
20
11
Ad
ult &
Cu
ltu
re
Se
rvic
es h
ave
Ca
rers
Info
rma
tion
Pa
ck,
in w
ritt
en
fo
rm
an
d o
n-lin
e. N
TS
ha
ve
ca
rers
we
bsite
an
d c
are
rs c
ha
rte
r
Nu
mbe
r of
hits
NC
C w
eb
site
(ca
rers
se
ctio
n)
ha
s
6.
En
su
re info
rma
tio
n is
pro
vid
ed
in
a r
an
ge
of
form
ats
, be
cu
ltu
rally
se
nsitiv
e a
nd
in
a r
an
ge
of
lan
gu
age
s
Ad
ult &
Cu
ltu
re
Se
rvic
es
Asse
ss t
he
ne
ed
an
d q
ua
lity
of
info
rmatio
n p
rovid
ed is
cu
ltu
rally
sp
ecific
an
d
ap
pro
pria
te
Re
vie
w
en
d
20
12
Info
rma
tion
is
tra
nsla
ted
in
to a
ran
ge
of
lan
gu
age
s
on
re
qu
est
Info
rma
tion
is
acce
ssib
le a
nd
be
ing r
equ
este
d
by c
are
rs w
ith
En
glis
h a
s a
n
ad
ditio
na
l
lan
gu
age
7.
Age
ncie
s p
rovid
ing
info
rma
tio
n, a
dvic
e &
su
ppo
rt t
o c
are
rs w
ill b
e
ava
ilab
le t
o c
are
rs
thro
ugh
ou
t th
e c
ity,
by
All
pa
rtne
rs
De
ve
lop
su
ppo
rt s
erv
ice
s
for
wo
rkin
g c
are
rs s
o t
ha
t
the
y a
re n
ot
exclu
ded
fro
m
acce
ss, fo
r e
xa
mp
le o
ffe
rin
g
eve
nin
g
Re
vie
w
en
d
20
11
Evid
en
ce
of
go
od
pra
ctice
els
ew
he
re
ind
ica
tes v
cs
org
an
isa
tio
n o
ffe
rin
g
eve
nin
g
Work
ing c
are
rs
fee
l th
ey a
re
inclu
de
d in
th
e
ma
instr
eam
pro
vis
ion
of
Page 31

30
Ac
tio
n
Le
ad
pa
rtn
er/
pa
rtn
ers
Pla
nn
ed
im
pro
ve
me
nt
By
wh
en
?
Wh
at
we d
o
alr
ea
dy/k
no
w t
ha
t
wo
rks
well
Ho
w w
ill w
e
kn
ow
wh
en
we
ge
t th
ere
?
tele
ph
one
, fa
ce
-to
-fa
ce
an
d fo
r ca
rers
wh
o
ca
nno
t att
en
d
ap
po
intm
ents
du
rin
g
wo
rkin
g h
ou
rs
me
etin
gs/c
oun
se
llin
g
se
ssio
ns
ap
po
intm
ents
to
wo
rkin
g c
are
rs
se
rvic
es
Page 32

Where we have been and where we are going
Where have we been?
There have been many achievements to date from the Newcastle Carers Strategic
Action Plan which came to an end in August 2009, they included:
• The development of the Newcastle Carer’s Information Booklet, which was
widely circulated and received positive feedback.
• A carers information event was held to celebrate Carers Rights Day, this has
now been formalised as an annual event.
• The carers section of Newcastle City Council Website was updated to include
a web version of the Newcastle Carer Information Booklet.
• Active links were made with Council’s Social Inclusion Unit and Health and
Race Equality Forum where ‘hard to reach out to’ carers were identified.
• Training and development opportunities to support carers to consider their
learning and development needs, for example Caring with Confidence and the
Stronger Voice programmes.
• The development of a dedicated Carers Social Work Team which carries out
carers assessments with a therapeutic focus to support and enable carers to
explore any concerns or issues associated with their caring role.
• Plans agreed for emergency support to carers as part of the New Deal for
Carers and the development of a carers contact card.
• A strategy was agreed for the use of a Carers Assistance and Training Fund
for individual carers and groups to access.
Where are we going?
The actions outlined in this latest strategic action plan, build on the success and
achievements of the previous strategic plan and a strong emphasis is placed on the
essential nature of partnership working to achieve our shared values and outcomes.
It should not be underestimated that we face particular challenges in the years to
come, not least the financial climate that affects us all. That said it is important to
have an optimistic perspective and believe that good things can happen when
people are willing to share ideas, good practice and resources. It is these things that
build strong partnerships, and it is strong partnerships that will deliver change for
carers.
Page 33

32
Page 34
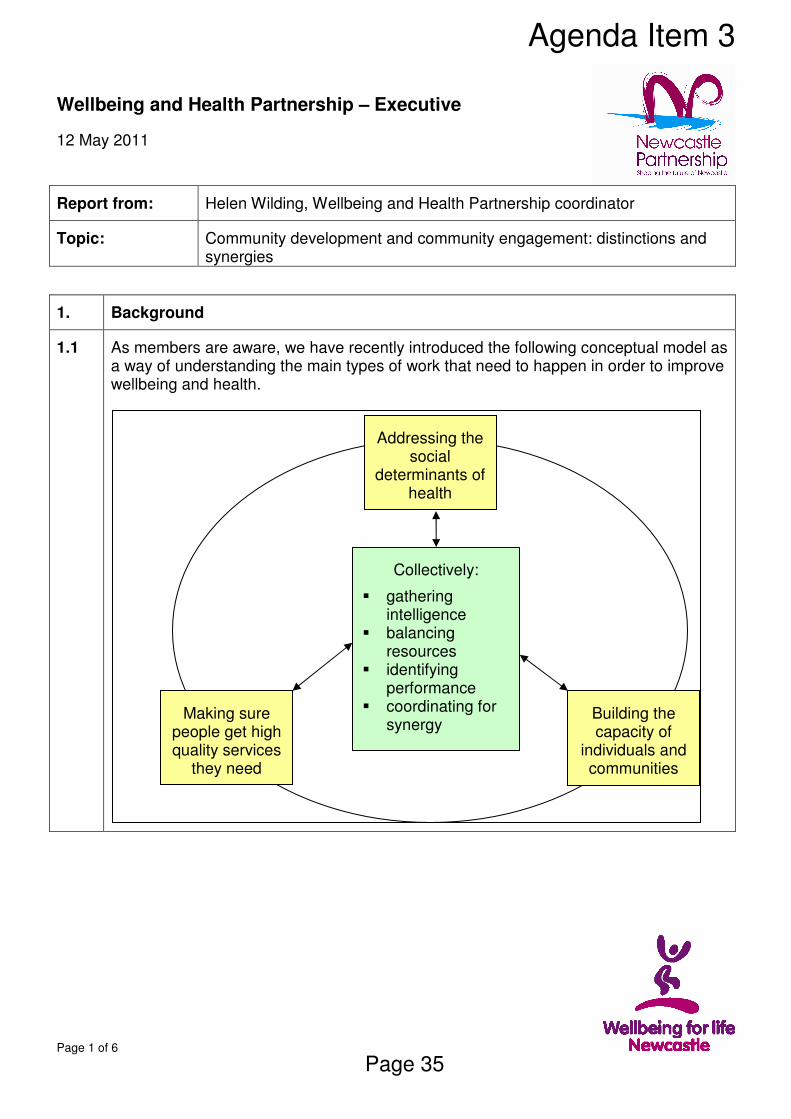
Page 1 of 6
Wellbeing and Health Partnership – Executive
12 May 2011
Report from: Helen Wilding, Wellbeing and Health Partnership coordinator
Topic: Community development and community engagement: distinctions and synergies
1. Background
1.1 As members are aware, we have recently introduced the following conceptual model as a way of understanding the main types of work that need to happen in order to improve wellbeing and health.
Making sure people get high quality services
they need
Building the capacity of
individuals and communities
Addressing the social
determinants of health
Collectively:
§ gathering intelligence
§ balancing resources
§ identifying performance
§ coordinating for synergy
Agenda Item 3
Page 35

Page 2 of 6
1.2 The model has proven a useful way of stimulating conversation and developing stakeholders understanding of the breadth of work entailed in improving wellbeing and health. However, as I have done so, I have realised that people do not have a shared understanding of the role of community development in ‘building the capacity of individuals, families and communities’. There is a tendency to equate this with community engagement/participation approaches linked to co-production of services.
1.3 This paper brings together some of the key definitions to act as a basis for discussion. It is not intended to be a full ‘literature review’ but to bring together some key points to trigger dialogue and shared understanding. It builds on a paper and discussion held at the Healthy Lifestyles Strategic Board on 28 April 2011.
2. Building the capacity of individuals, families and communities: the role of community development
2.1 Wellbeing and Health Partnership is increasingly promoting community development as one of the areas of work we need to invest in to improve wellbeing and health. This has relevance for all of our strategic areas of work.
2.2 The work we have done to date within the Wellbeing and Health Partnership uses the following explanation:
“a long-term process whereby people in the community work together, with facilitation and support of people from organisations, to identify their own assets, create change, exert more influence in the decisions which affect their lives and work to promote health and wellbeing for themselves, the community in which they live and the society of which they are a part”
We adapted this from the explanation at www.combatpoverty.ie/povertyinireland/glossary.htm
2.3 Community development methods and values are identified by Community Development Foundation as one of four key principles that underpin community empowerment.
The others are leadership and management; building partnerships; and, building the capacity of partners. They state “adopting a community development approach to empowerment will go a long way to ensuring that individuals and communities develop the capacity and confidence to become partners and co-producers […] in building and maintaining healthy communities” (Gregson and Court, 2010, page 18/19).
2.4 Labonte (1999) highlights that communities frequently self-organise to take actions that they anticipate will improve their lives. Often these actions are about health determinants, even if communities do not take those actions in the name of health. Communities themselves do not think of this as community development.
Community Development therefore needs to be thought of as the actions that organisations take to improve the capacity of groups to act on their issues of concern – in this context organisations need to be primarily concerned with the process of the work, rather than the content (the actual topic communities want to work on). Community development needs to be accountable for the contribution it makes to improving capacity of groups to act on concerns – not necessarily what the concern is or whether the concern is actually achieved. This poses challenges for organisations in
Page 36

Page 3 of 6
terms of ‘traditional’ means of understanding and measuring outcomes.
2.5 A recent Health Inequalities National Support Team report says “Community development is one way of facilitating communities’ awareness of the factors and forces that affect their wellbeing, health and quality of life” so it is a way of improving health literacy and can lead to health-enhancing action.
In addition, the community development process can be thought of as a ‘health intervention’ in its own right. Regardless of the topic of concern the community chooses to focus on, the process helps in addressing psychosocial risk factors to health, such as low perceived power, poor social networks, isolation and low meaning and purpose.
2.6 There has been a recent resurgence in moving away from ‘deficit’ based approaches to community development, which focus on needs and problems, as these approaches can lead to communities being more disempowered and reliant on public services. As a result, there is growing awareness of the need for asset-based approaches.
2.7 Assets are best thought of as:
“any factor or resource which enhances the ability of individuals, communities and populations to maintain and sustain health and wellbeing. These assets can operate at the level of the individual, family or community as protective and promoting factors to buffer against life’s stresses.” (Morgan, 2009 cited in I&DeA, 2010).
2.8 It is often thought that an asset based approach is framing as a positive rather than a negative (e.g. stating % who don’t smoke, rather than % who do smoke!).
But, at the WHO conference in Sandnes, Norway in 2010, Ziglio spoke of the need to identify both assets and needs as two different dimensions. The ‘ideal’ is to have high assets with low needs, but getting there will be different depending on your starting point - high assets with high needs; low assets with high needs; or, low assets with low needs.
The WHO Collaborating Centre at Liverpool University is also looking at issues of societal resilience to poor health as it seems that different countries have different degrees of resilience – e.g. poverty has a greater impact on health outcomes in the UK than in Sweden.
2.9 A number of ‘techniques’ have been developed that community development workers can use to support communities in discovering and mobilising assets. These techniques can be thought of as the ‘tools’ of community development practice. These specific community development tools need to compliment a wider range of practices that support individual and small group development such as person centred planning and enabling people with support needs to become part of life in their local community.
2.10 In Newcastle, work is taking place to develop and introduce a tool that communities can use for identifying and mapping their assets. Newcastle City Council has been looking at the Signature approach developed by BusinessLab1. This approach takes communities through a series of questions relating to assets and then uses a visual
1 For background info see http://www.businesslab.co.uk/signatures/community-signature
Page 37

Page 4 of 6
‘traffic-light’ way of summarising the discussions. Different communities within an overall geographical area can complete a Signature so different perspectives can be brought forth. Communities can use the Signatures to determine the issues they would like to work on as well as the assets they have to work on them. The process of discovering assets is an important way of communities developing new relationships and new possibilities.
The existing Signatures already developed by BusinessLab are not fit for purpose for what we want to do in Newcastle so there will be some work to modify and pilot a Newcastle health and wellbeing Signature as part of improving wellbeing and health through geographically based approaches work. (NB these developments are subject to procurement)
2.11 There are also some challenging issues to consider given that community development is interdependent with the way organisations work, allocate and use their resources.
• The Marmot principle of proportionate universalism is important here – are we putting proportionately more scale and intensity of community development effort into supporting those communities who have less access to money, power and resources, and in reaching the ‘easy to overlook’ within any geographical community?
• How can organisations shift their traditional power base (particularly control of money and people resources as well as information and decision power) and work collaboratively with communities? This is important if we are to expect community members to participate in settings where there is an imbalance of power and information (Gregson and Court, 2010, page 23)
• How do we resource, and evaluate the success of, community development in a way that emphasises the value of the long-term process, rather than the content of the work and whether or not it is achieved in the short-term?
• How do we work in a way that communities can take the lead rather than become dependent on the support provided? The ultimate aim is to aim not to be needed which is quite a challenge to the way we traditionally work!
3. Making sure people get high quality services they need: the role of engagement, co-production and participation
3.1 It is important to distinguish community development from:
• Consultation/engagement: the primary purpose of community development is to improve the capacity of groups to identify and act on their concerns. It is not first and foremost a way of organisations ‘finding out’ about communities’ needs to improve or co-produce decisions about services or other areas of work.
• Community-based or outreach approaches to service delivery or health promotion. In these approaches, the ‘concern’ is identified by organisations usually on the basis of data analysis (Labonte, 1999)
These types of activity are more associated with making sure people get the high quality services they need through the processes of engaging actual or potential users of services in the commissioning, design, management, improvement and delivery of
Page 38

Page 5 of 6
services
3.2 The council and NHS organisations have duties placed on them to engage with communities and involve them in decision making. The nature of the duties placed on public bodies in respect of engagement has resulted in resources and ways of working being developed to meet these duties. For example, the conceptual model that is commonly used is the ‘ladder of engagement’ which emphasises a shift from information provision through to community control.
3.3 For those service users who are actively engaged, the process can play a role in addressing psycho-social risk factors to health such as low perceived power. However, for the most part ‘success’ of engagement is understood to be services that are appropriate, accessible and have improved uptake.
3.4 In April 2010, Newcastle City Council Adult and Culture Services Directorate commissioned Peter Fletcher Associates (PFA) to undertake a time limited piece of work to ensure that a wide range of engagement opportunities exist and to locate these in a coherent infrastructure. PFA have now presented a report of the work to the Directorate’s Management Team, along with a range of papers and other documents to help take this work forward.
3.5 The Directorate’s Management Team is now considering the key recommendations arising from the work and is aware that they would need to be implemented as part of a partnership approach to engagement. Therefore they would welcome comments from members of the Partnership Executive. This is the topic of another item on today’s agenda.
4. Summary and recommendations
This paper draws a distinction between community development and engagement activities. It is important that both of these are valued for their contribution to improving wellbeing and health and that we develop and implement ways of working that enable both to flourish. Historically there has been a greater focus on engagement activities, so it is important that we can start to re-dress the balance and see community development as a distinct area of work in its own right.
Partnership Executive are asked to:
• Continue to develop engagement practices, building on the recommendations of the PFA work
• Use the distinctions covered in this paper to raise awareness with others about the different nature of community development and enter into discussions about the challenges we face in developing this approach.
Report written by:
Helen Wilding, Wellbeing and Health Partnership Coordinator
Tel: 0191 211 6461 Email: [email protected]
With Karen Inglis, Project Manager, Adult & Culture Service Directorate
Background Papers
Gregson, R. and Court, L. (2010) Building Healthy Communities: a community empowerment approach. London: Community Development Foundation
Page 39

Page 6 of 6
I&DeA (2010) A glass half-full: how an asset approach can improve community health and wellbeing. London. I&DeA.
Labonte, R. (1999) Mutual accountability in partnerships: health agencies and community groups, Promotion and Education; 6; 3; pp 2 – 8.
National Institute for Health and Clinical Excellence (2008) Community Engagement to improve health, NICE public health guidance 9.
Department of Health (2011) Health Inequalities National Support Team: A generic diagnostic framework for addressing inequalities in outcome at population level from evidence-based interventions.
Page 40
1
Prevention A voluntary and community sector perspective
Prepared by NCVS for the Newcastle Wellbeing and Health Open Forum February 2011
Agenda Item 5
Page 41

2
Contents
1 Background 3
2 What is Prevention? 3
3 Summary of main points 4
4 Why is Prevention so important? 5
5 VCS strengths 7
6 VCS activity 8
7 VCS priorities for action? 9
8 Recommendations 11
Appendix 1 Case studies 12
Appendix 2 Stories and quotes 16
Page 42

3
1 Background
In 2010, voluntary and community sector (VCS) partners in Newcastle’s Wellbeing and Health Partnership developed a new structure for the sector’s participation in the Wellbeing and Health agenda with the intention of delivering a more proactive and influential involvement.
This structure is centred around the newly formed Wellbeing and Health Open Forum, which provides a platform for the sector to develop ideas, strategies, responses and proposals on key themes under wellbeing and heath.
These key themes are chosen through a Leads Network of VCS representatives and other sector leaders involved in the Wellbeing and Health Partnership, and for the first forum, held on October 13 at Central Square, the chosen subject was Prevention.
To facilitate discussion the delegates were asked three questions:
! Why is prevention so important?
! What is the VCS already doing and what are its strengths?
! What are our priorities for implementing a prevention strategy?
This report arises from the lively debate these questions prompted.
2 What is Prevention?
Defining prevention can be problematic because there are many versions out there:
! Newcastle City Council in their presentation to the Open Forum defined it as:
o Promoting people’s wellbeing and quality of life and access to universal services
o Preventing or delaying the need for high cost specialist or more intensive supports.
! A medical definition is ‘actions directed to preventing illness and promoting health to reduce the need for secondary or tertiary health care.’
! A more detailed definition identifying four levels is:
o Primary - strategies that intend to avoid the development of conditions
o Secondary - strategies that attempt to diagnose and treat an existing condition in its early stages before it results in critical outcomes
o Tertiary - strategies that aim to reduce the negative impact of established conditions by restoring function and reducing complications
o Quartenary -activities that mitigate or avoid the consequences of unnecessary or excessive interventions
Page 43

4
3 Summary of main points
Before getting into the detail, there were four strong themes running through the discussion that should really be identified as overarching principles.
Make prevention the top priorityPrevention should be the top priority for delivering the wellbeing and health agenda. Currently a large proportion of the resources are directed towards interventions that tackle the symptoms rather than the causes. The defining characteristic of preventative action is that it tackles causes.
The challenge in an environment of fewer resources is to place a greater emphasis on prevention while at the same time continuing to deliver services to those who need them. This challenge is all the greater when timescales are taken into account. Prevention is a long term strategy with long term outputs and outcomes, but the reward for the future is that, with effective interventions, the need for higher cost services is delayed or avoided.
Prevention is everybody’s businessThe Wellbeing and Health Partnership has the lead role both for developing and implementing strategies for the wellbeing and health of the citizens of Newcastle, but it also takes the lead in articulating the wider determinants of health to the whole Newcastle Partnership and all its stakeholders. The underlying causes of bad health outcomes cover every aspect of Partnership work from housing and employment to community safety. The challenge here is to embed prevention into everyone’s thinking and planning.
Measuring impact and effectivenessWhilst the benefits of preventative action seem obvious, arguing for greater investment in prevention has always suffered from the lack of hard evidence for those benefits. It is difficult to answer ‘what if’ questions such as “what if we stopped doing this?” and “What if we started doing that?” because it’s about what could happen rather than what is happening. Because the primary principle of prevention is taking actions before problems arise, what evidence there is will be indirect and separated in time from the actions. This is especially true of activity that falls under the heading of social capital, much of which is delivered by local and often small community groups. There are many ways to define social capital but it is essentially about the involvement of people in cooperative relationships in communities that facilitates both collective action and promotes wellbeing for individuals.
However hard it is to achieve, a strong evidence base is an essential first step to ensuring prevention is resourced as a priority.
Sharing intelligence and planning investmentGiven the crosscutting nature of preventative action it is vital that strategies, investment decisions and delivery are undertaken in partnership. Good mechanisms are needed to share intelligence and make collective decisions.
Page 44

5
4 Why is Prevention so important?
Nips problems in the budThe Open Forum workshops produced some interestingly subtle variations on this theme that point to an intriguing conclusion. They include:
! Stops bad things happening.
! Timely prevention stops problems from becoming worse.
! Helps stop the same problems from recurring.
! Creates an opportunity and mechanism to identify early stages.
These can be translated into:
! Making sure it never happens.
! Making sure it hardly gets off the ground.
! Making sure it doesn’t happen again.
! Making sure it doesn’t get worse.
This strongly suggests a continuum that ranges from creating an environment for lifestyle choices that promote healthy lifestyles, all the way through to treating bad health outcomes that already exist.
In the context of helping the individual this would mean identifying where they are on that continuum, halting further deterioration, and ultimately supporting that person to head as far back towards a healthy lifestyle as its possible for them to go.
There is a concept in the employability agenda of the “journey to work” in which individuals are supported to overcome what are often multiple barriers to employment. This same principle could be used in prevention to support people on their journey to the healthiest possible life for them. As with the employability agenda, this would help decision making bring interventions together in a sensible way that focuses on the individual, and would involve identifying barriers that could well be the responsibility of other themes in the Newcastle Partnership and all stakeholders.
Saves Resources This is essentially the principle of “invest to save”, but it isn’t just about health services:
Services save - The pressure on health and care services will clearly be significantly reduced if healthier communities can be achieved.
People save – For many people in excluded communities bad health means not working, not being productive and needing help that is not always freely available. A healthier life can turn all those things around, enabling people to value themselves, to enjoy a better quality of life and for some people giving them more disposable income as well as containing the cost of health provision.
Page 45
6
Communities save – This is a potentially huge benefit. More health means more participation, more people in work and more money in the local economy. Not only does this result in a healthier and more vibrant community able to sustain local economic and social activity, but it could also produce massive savings in the provision of non health related support services. Most importantly it results in people enjoying a better quality of life and contributing to their communities.
Promotes and sustains quality of lifeAchieving a good quality of life is an end in itself quite independent from considerations of cost and service provision. The workshops identified a number of specific outcomes for individuals and communities:
! Empowers and enables
! More self esteem
! Promotes self responsibility
! Promotes happiness
! Encourages positivity
! Promotes behavioural change
! Better educational attainment
! Less pain
! Less disability
! Less emotional distress
! Less mental health problems
! Less depression
Information and education are at the heart of prevention and can delivery a sustainable increase in social capital. An increase in social capital will be the result of individuals in communities being more confident, empowered and enabled. Dealing only with symptoms and not causes will not do this. Sustainable communities can only be built around genuinely stable improvements to all of the above.
Operational BenefitsA preventative approach is a much more sustainable model, in contrast to many current interventions that have more of the flavour of crisis management. If a vision can be achieved that recognises the long term nature of the task it will allow service providers to plan more effectively and maintain focus on the most vulnerable and excluded.
If designed in the right way, a prevention strategy could create a framework in which a robust knowledge and evidence base can be established. Service providers, including the VCS will be able to more easily spot trends and place them in a wider partnership-wide context. It should promote a more holistic approach to needs and deliver what people really need, rather than what individuals or service providers think they need, although this will require a more collaborative approach to how service users and providers engage with each other.
Page 46

7
5 Voluntary and Community Sector strengths
IntelligenceThe sector is very close to communities and already has a wealth of knowledge about local need and expertise around practical solutions. In this sense the sector can make a strong contribution to strategy, design and planning. This knowledge also means that the sector can be very responsive at community and individual level.
CostThe sector has a long history of working within tight funding limitations, which tends to make its services comparatively cost effective and creative. However the work of the sector also brings added value to statutory provision and makes a significant contribution to increases in social capital in our most deprived communities. The sector also has the advantage of being able to access grant funding that is often denied to others.
Most VCS organisations operate via multiple funding sources and in consequence are often able to lever in other funding streams to a particular activity.
CreativityAlthough the funding environment has become increasingly prescriptive over the years the VCS still enjoys more freedom to innovate than other sectors. Responding to changing needs in individuals and communities has always required fleetness of foot, flexibility and a willingness to try different ways of doing things. The VCS can be a vehicle for exploring different approaches, particularly through grant funding.
Co-production can also be a strong driver for creative and innovative ways to do things.Co-production is about delivering services in an equal and reciprocal relationship between professionals, people using services, their families and their neighbours. Where activities are co-produced in this way, both services and neighbourhoods become far more effective agents of change. Co-production emphasises that people are not passive recipients of services and have assets and expertise which can help improve those services. It is a potentially transformative way of thinking about power, resources, partnerships, risks and outcomes, not an off-the-shelf model of service provision or a single magic solution.
TrustSuccessful prevention requires communities and individuals to change the way they do things, and the role of providers is to support and facilitate those changes. A vital ingredient for this to work is trust, and it is one of the unique selling points of the VCS that they enjoy the trust of local people. Because engagement is built on trust and local knowledge, it can be holistic, person centred, enabling and user led. It can also help to foster social capital and build community links. For the most isolated people in our communities the VCS are often the first point of contact.
QualityPreventative action is the voluntary and community sector’s core business. It has a long history of seeking to understand the underlying causes of deprivation, exclusion and inequality and turning that understanding into action. It is motivated by strong values and
Page 47

8
driven by a genuine passion for the interests of the most vulnerable. These things, together with a willingness to work collaboratively, underpin the quality of what the sector does.
6 VCS activity
Below is a list of the kind of preventative work that the sector does, produced by delegates to the Open Forum event. It is indicative rather than exhaustive, and other areas of activity will be picked up through the case studies
! Raising awareness
! Volunteering
! Information and advice
! Befriending
! Leisure services
! Carer support
! Safeguarding
! Advocacy and advice
! Giving people a voice, representation, u decide, ward charter, citizens assembly
! Behaviour change
! Physical activity opportunities
! Green environment improvements
! Housing
! Children and young people
! Campaigning about policy and decision making
! Campaigning for change
Case StudiesA call for case studies and stories was put out to the sector as part of the development of the report. This was in response to the clearly identified need to establish an evidence base for prevention as a priority (discussed elsewhere). The studies are divided into 2 sections in an appendix to this report.
! Project profiles
! Stories and quotes
These few studies are examples only and a starting pint for future work. The gathering of intelligence about the preventative impact of the sector’s activities is a longer term objective that needs to be planned, designed and utilised to maximum effect. A part of this, not explored here, is to find ways of showing how the activities all providers for a particular geographical area or target group interconnect and complement each other.
Page 48

9
7 VCS priorities for action?
IntelligencePreventative action requires a strong evidence base because outcomes and outputs are longer term and harder to measure, yet most funding opportunities need a robust justification. So a first and vital task is to build that evidence base. There will be additional benefits to this:
! We will have a better understanding of the true costs of care in the community.
! In an environment of huge cuts we will be able to articulate the consequences of services disappearing.
! We will be able to contrast the cost of prevention against the cost incurred in the future if we don’t do anything.
! We will be able to tell the stories that articulate the direct impact on vulnerable people and communities.
Action planningCase studies provide good evidence in the sense of telling real illustrative stories, but we also need to gather and collate statistical data around the comparative impact of preventative action. This should also involve embedding impact evaluation into VCS activity as routine.
There is some national data around. For example:
! A Communities and Local Government report1 “Research Into the Financial Benefits of the Supporting People Programme” which estimates that a programme expenditure of £1.55 billion brings an overall financial benefit of £2.77 billion. For some of the vulnerable groups in this report, such as drug users, people with mental health problems and older people, the financial benefits outweigh the investment by up to 4 times.
! A report by SP Solutions2 looking at Supporting People provision in the North East comes to a similar conclusion. It should be noted though that the methodology for these two reports does not take into account the long term benefits, but only compares a year with SP to a year without it.
! A Department of Health report3, “Measuring Social Value” measures social return on investment (SROI) for 5 social enterprises showing that for each £1 invested, a social return of between £2.52 and £5.67 was achieved.
Perhaps good starting points would be the Joint Strategic Needs Assessment (JSNA) Project Board, approaching the universities to see if new work could be undertaken and exploring the opportunities to carry out Social Return on Investment evaluations.
1
Tom Ashton & Dan Turl (January 2008) for the Department for Communities and Local Government -
“Research Into the Financial Benefits of the Supporting People Programme”http://www.communities.gov.uk/publications/housing/supportingpeoplefinance2
Kathy Bee & Helen Woods (September 2010) “North East Region Cost Benefit analysis and Lessons
Learnt From Supporting People” - http://www.northeastiep.gov.uk/adult/supportingpeople.htm3 Central Office of Information (November 2010) for the Department of Health “Measuring Social Value”
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/DH_122355
Page 49

10
Once enough intelligence has been generated to put to good use, a strategic approach to how it is used will be needed. In particular how it is used to influence prevention strategies, action plans and programmes with public sector partners.
It is also vital that the sector establishes robust mechanisms for communicating between organisations and sharing intelligence within the sector, but also across the wider provider community and other partnership stakeholders.
CommunicationHow we communicate is fairly fundamental to prevention, particularly where it involves changing behaviours. There is a wide range of ways to disseminate and share information from the internet to face-to-face engagement. Here are some of the issues raised:
! Making sure information is correct, relevant and timely.
! Making sure information is tailored to its target audience.
! Promote anti discrimination practices in provision.
Action planningWe need to ensure that we communicate with our beneficiaries in a way that has the greatest impact on health outcomes. In the past information campaigns have often not worked, and this may be a good opportunity to think about better ways to influence behaviour change than those traditionally employed.
CollaborationIt is very important that preventative work is effectively co-ordinated between statutory, private and VCS partners and commissioners. This will ensure a genuinely strategic approach that avoids gaps and duplication:
! All partners, including the VCS, should be involved in strategic development from the beginning.
! VCS organisations, and indeed all partners, should work together and be less predatory and competitive; be more appreciative of the skills and knowledge of others and the different contributions made by sectors and agencies to the collective aims of prevention. The work, and its beneficiaries, are more important than the wellbeing of providers.
Action planningSome delegates to the forum event felt that the sector should have been involved earlier in the development of the Council’s prevention strategy. Recent government changes, particularly the future formation of a statutory Health and Wellbeing Board, will be an opportunity to continue and strengthen the role of the sector in the agenda.
Value the VCSAs noted earlier, prevention is very much the core business of the voluntary and community sector. Historically we have not been very good at blowing our own trumpet, and the need to get better at it could not be more urgent.
Page 50

11
Action planning We need to promote and celebrate the quality and relevance of our work. We should also champion the notion that good and relevant work already being done should be retained. In other words get away from short term funding where it is appropriate, and instead recognise that some activities can be characterised as a community resource.
The case studies currently being gathered will be a key component of the above actions.
Levels of PreventionSome feedback from the Open Forum suggests that there needs to be a better understanding of the new definitions for levels of preventive action that were described in the presentations. Some delegates said they found it difficult to identify their activities in this new model. A strategic approach for the sector about priorities for action on the ground cannot be clearly articulated without a robust understanding of the model and how the sector fits into it.
Action planning A priority for the Open Forum should therefore be to develop a good description of the model that is meaningful to VCS activity.
8 Recommendations
The capacity of NCVS, the Leads Network and the sector as a whole to take these priorities forward is uncertain in the current economic climate. It is therefore essential that the Leads Network, together with NCVS explore what is achievable in the short to medium term of the actions listed below.
! We recommend the Wellbeing and Health Partnership Executive develop a definition to be agreed by public sector and voluntary and community sector partners of what prevention and preventative work means in Newcastle. In particular there should be a common understanding of what the different levels of intervention (primary, secondary etc) are so that providers can clearly see where their interventions fit
! We recommend officers responsible for producing the Joint Strategic Needs Assessment work with voluntary and community sector organisations to enable their contribution to the JSNA and as a means of providing evidence of the preventative work of the voluntary and community sector.
! We recommend commissioners note the recommendations of the Wellbeing and Health Open Forum task and finish group report on public sector commissioning (Nov. 2010) as a means to promote more collaborative working and the involvement of voluntary and community organisations at each stage of the commissioning cycle
! We recommend the Wellbeing and Health Partnership Executive lead the development of alternative strategies for achieving behavioural change, taking into account recent research about how individuals make life choices. To be effective this should involve a wide range of agencies and sectors and take into account for example regeneration, housing, economic development and children and young people as well as health and social care
Page 51

12
Appendix 1 Case studies – Project profiles
Healthworks Community Health TrainersA Community Health Trainer is a local person recruited and trained from their community, so they understand first hand the concerns of local people. Health Trainers are trained to support individuals to make health related changes in their lifestyle. They support people to identify what they want to do and how they want to do it; perhaps taking up physical activity, stopping smoking, healthy eating, or joining a local community group. They define health in its widest sense, including:
! Heart health
! Eating well
! Basic Cooking skills
! Family health
! Managing your weight
! Belonging to a community
! Sexual health
! Daily physical activity
! Managing life ok
! Feeling good
! Understanding your body
! Sensible use of alcohol
! Not smoking
They support people to achieve change; perhaps going with them to the gym, going through a food diary with them or explaining what stop smoking services can offer. Health trainers also signpost people to mainstream services when necessary.
Research shows that a higher level of poor health is found in areas where there is high unemployment, poor housing, and where families have lower than average incomes. Individuals therefore face an often wide range of barriers to being in better health. The work of the trainers demonstrates the importance of one to one support, perseverance, being flexible and group support. This is particularly true where people have mental health issues and learning difficulties. The programme achieves positive outcomes:
! Being physically healthier (weight loss, healthy eating, safe and developmental exercise, etc)
! Being mentally healthier (confidence, motivation, more control, more positive, being able to overcome barriers and being happier in themselves)
! More active and engaged (better family life, setting others an example, making new friends, looking forward to activities and meeting people)
This is an example of work that increases social capital in disadvantaged areas. It also demonstrates the principle of taking individuals from where they are to the best place they can be. For someone with dementia, the benefit is in slowing deterioration and increased quality of life, while for others it can mean permanently leading a normal, healthy and productive life.
Page 52

13
Tyne Housing
Tyne Housing provides supported accommodation and day care services for vulnerable, isolated, and socially excluded adults. They also provide therapeutic employment from a furniture renovation project and retail shop. The Joseph Cowen Health Care Centre provides drop in services for rough sleepers, as well as on site access to a GP, Nurse, and CPN for individuals who are unable to register with mainstream medical services.
Accommodation includes a Direct Access Hostel, a “wet hostel” (for those who’s alcohol use has caused them to be excluded from other accommodation options), a hostel run in partnership with the Forensic Mental Health Team and a hostel that provides the final stage of rehabilitation for those who have been released from long-term secure units. These housing projects are run in a variety of ways including with a residential support worker living in a community setting and shared supported housing with visiting support provided by a support worker specifically assigned to each project. A large number of their residents do not like living alone. Many of them have long-term mental health problems that can be exacerbated by the feeling of isolation, which can then lead to crisis. A large proportion of residents are made up of those with a history of substance misuse where the boredom of living alone can lead to relapse. One of the key features of the shared housing is that they mix people with a variety of support needs and issues.
A number of schemes have been developed for those residents who have reached a stage in their lives where they feel ready to live alone, but whose support needs would not allow them to sustain full independence. This has lead to a total of 38 residents living in single tenancies in purposely developed schemes, again with residential workers providing on site support.
The final stage is full independence in 29 flats in a former department store in the heart of Newcastle’s East End.
Due to the nature of their problems, the vast majority of service users are long term unemployed or have never worked. Previous convictions rule them out of a vast section of the labour market. Tyne Housing has their own social enterprise company, Better By Half property maintenance, capital funded by Places of Change. The aim is to provide the organization with it’s own building, grounds maintenance and repair service, cutting costs and providing employment training opportunities for service users. This is good for service users as, unlike employment training schemes provided by external agencies, Tyne Housing know them and the individual issues that they face. Service users are often dissuaded from taking part in positive activities and fall back into drug use and offending etc. Better By Half has taken off due to the efforts of a core group of service users who tell their fellow hostel residents in Byker to get out and do something more productive than sitting around all day. This is a lot more persuasive than when it comes from their support worker, probation officer, or the adviser from Job Centre Plus.
Better By Half also offers training in basic literacy and numeracy, and skills such as CV writing. This enables trainees to be better prepared to sell themselves in the employment market. They can make the transition from long term unemployment, through being supported through the uncertainties of becoming financially independent.
Page 53

14
Age UK
Age UK offers a range of services to meet the needs of older people across the whole spectrum of later life. Their main base is MEA House where they run the Healthy Living Centre with a multi-purpose hall and coffee shop. The shop includes a Cyber Café.
Care at Home Service120 care workers provide about 3000 hours of care a week. This includes personal services, help with medication routines, trips out, shopping, housekeeping and meal preparation. This is mostly under contract to Newcastle City Council.
Fit as a Fiddle ProjectThe Fit as a Fiddle Project runs within Age UK’s Day Services. The project is funded by the Big Lottery. This provides a range of activities including gentle exercise, Tai Chi, yoga, beauty treatments, healthy eating sessions, and Wii Fit classes. Older people really enjoy taking part in the activities, as well as having a home cooked meal and spending time with their friends.
Lunch groups Within Day Services, Age UK runs supported lunch groups for older people who are frailer and unable to get out and about to groups running within their community. Specialised transport brings older people to lunch group venues throughout Newcastle. A lunch is provided, and an activity (funded by Fit as a Fiddle) takes place. A member of staff runs the groups with the support of a team of volunteers.
Computer classesThe Cyber Cafe computer facilities are available to people aged 50 and over. Computer classes are provided to enable older people to acquire basic and intermediate computer skills across a range of software packages. Classes generally run for six to ten weeks and there is also a weekly staffed drop-in session.
BefriendingThis service is for older people who live alone and are isolated, perhaps by bereavement, ill health, disability or loss of social networks. All volunteers are mature, friendly people. They normally visit once a week and will provide support and friendship. They may also assist an older person to go out. Service users will be invited to attend social outings and discussion events. Our aim is to provide them with opportunities to contribute to their community to meet new people and to have fun, and volunteers continue to offer support until the service user feels able to cope.
Advice and informationInformation and advice is provided on a range of subjects including welfare benefits, housing, legal issues, community care and residential care. If they are not the most appropriate organisation to advise on a particular subject, they can be referred to another agency. The service is also available to friends, family and carers.
ImpactOlder people are a growing proportion of the population and a major user of mainstream services. This work clearly helps to minimise the need for those services and enhances the quality of life of older people.
Page 54

15
Disability North
Disability North’s purpose is to promote inclusion, independence and choice for disabled people. It does this by providing information and advice that enables people to make informed decisions about the choices in their lives.
Benefits advice The service team provides advice and guidance on benefit claims from initial application through to representation at appeals. This includes:
! Disability Living Allowance
! Employment Support Allowance
! Carer's Allowance
! Attendance Allowance
Supporting people to access the benefits they are entitled to contributes to reducing emotional distress and can lead to a more positive outlook for an individuals.
Independent living The organisation provides information on all aspects of independent living, such as personal care and leisure. The Dene Centre has a wide range of equipment and demonstration areas, including an accessible bathroom and living area, stairlifts and a mobility track. Free assessments are carried out by therapists who can give independent guidance on the most suitable equipment.
Access Auditing and Equality TrainingThe Service Team also provides a comprehensive access auditing and disability equality training service to private, public sector and voluntary organisations.
Falls reduction Local falls groups attend a series of meetings which include a talk on:
! Equipment, which can help them in the prevention of further falls and their consequences.
! Details of possible benefits they may be entitled to.
Reducing the risk of falling can help a person be more confidant and positive about carrying out their everyday activities.
Advice is also given on disability legislation and human rights for disabled people.
Page 55

16
Appendix 2 Stories and quotes
Tyne Housing – Better By Half project – Supported housing for homeless people
Better By Half helps some of their skilled service users to reacquaint themselves with their trade. One such person, who has been resident with their association for a number of years, is a highly skilled plasterer. Spells in prison, followed by ill heath have lead to long term unemployment and a reliance on supported accommodation. The chance to use these skills again have provided him with a level of satisfaction that is, in his own words “better than sitting in a hostel waiting to die”.
West End Befrienders - helps older and disabled people to live independently
Mrs D is 69 years old and has lived on her own since her husband’s death 5 years ago. Her only daughter, who was also her carer died unexpectedly after an operation. Due to language barriers, Mrs D's daughter looked after all of her mother’s needs, which her mother relied on. West End Befrienders had already been involved with Mrs D as part of our carer support work and now had to step in and do much more with her. She was matched up with a volunteer of the same language, culture and faith. The volunteer had completed a bereavement counselling course and was able to help Mrs D. work through her grief and come to terms with her situation. The volunteer is still visiting her and doing lots of things her daughter used to do for her.
J has been a volunteer for West End Befrienders for nineteen years during which time she has visited hundreds of people bringing them her happy-go-lucky smile. For fourteen of them, she has supported H to lead a happy, independent life. Although H now has dementia, J. still visits her and uses the training she received about dementia. J. and her daughter take H to the coast once a week for a trip out and they help with her shopping on the way home. H has been able to join us on some of our summer outings. J.’s kindness enables H to enjoy these activities and lead a more independent life.
Better Days – A group run by and for people with learning diabilities
We know from work we have done before that lots of people are interested in history. We organised a course for 30 people with learning disabilities and other disabilities to learn about our local history. It was at the new City Library. It ran for 3 months, one day a week. In the mornings we went out with the City Guides to different places. Some of the places we went were St. Nicholas’ Cathedral, Grainger Market, Gateshead Civic Centre and Leazes Park. The guides told us about the history of the places we visited. We took photographs. In the afternoon we came back to the City Library and the Sage to do different activities to do with what we had seen. We did drama, research in the local studies section, poetry, photography, crafts and singing and music. We had 2 performances at the end. We did a play about the history of Cullercoats, a song we had made up about Newcastle and performed the poems we had written about the area. One performance was in the City Library. One performance was in the Sage Gateshead. We also had an exhibition of our work in the City Library. Since it finished Newcastle City Library has started running a history group for learning disabled people. It is for people who came on the course and other people too. We got money from the Learning Revolution Transformation Fund to run the course.
Page 56

17
Kids Kabin – an arts centre in Walker for local young people
We asked some young parents who had attended Kids Kabin when they were children what they got out of going to Kids Kabin, and if this had made them feel happier about their own children going to the centre. We did this during semi-structured focus groups during September 2010 in community venues. We also asked young volunteers about the training and responsibilities they had had, what skills they had gained as a result, and how they had taken these skills forward in their own lives.
The parents felt that their time at Kids Kabin was a positive one filled with learning new skills and making new friends, which in turn boosted their confidence and made them believe they could do anything they wanted to. One comment in particular summed up the fond memories of using the centre and its services: “If you were lucky enough to live beside Kids Kabin it was a fun place to be - it is a friendly place the, staff always have time for you and encourage you to achieve and be the best you can.” Some of the
parents went onto volunteer with the Princes Trust and have a real sense of
community.
Age Uk - quote
“I think it is so nice that we just need to pick up the phone and there is someone we can ask for advice. I am lucky I have a family that I can turn to, but there’s an awful lot of people who don’t.”
Page 57

18
Newcastle Council for Voluntary Service MEA House
Ellison Place Newcastle upon Tyne
NE1 8XS www.cvsnewcastle.org.uk
February 2011
Page 58

An induction loop system is available on request for meetings in the Committee Suite at the Civic Centre. Anyone wishing to use this facility should ring the Contact Officer.
Wellbeing and Health Partnership – Executive
Thursday 12th May 2010
Report from: Older People’s Strategic Board
Update report
1. Background
The role of the Older People’s Strategic Board (OPSB) is to provide strategic leadership to improve the wellbeing of older people and address the challenges and opportunities of an ageing population.
Membership of the OPSB includes representatives from the Elders Council; Newcastle City Council, NHS North of Tyne, Age Concern Newcastle, Voluntary Sector Representative (currently HealthWorks), University of Newcastle, University of Northumbria, Nexus and Your Homes Newcastle. The Board is chaired by the Newcastle City Council representative, who is Colin Williams (Adult and Culture Services). The Vice Chair is the Chair of the Elders Council, currently Mary Nicholls.
2. Outline of recent & current work
During 2010/11, the OPSB has undertaken the following activity:
• Improve partnership working and strengthen the relationship between the Board and the Local Strategic Partnership. The OPSB Co-ordinator has continued to play an active part in the Wellbeing and Health Partnership Co-ordinators group and to support joint work such as the Wellbeing and Health Partnership Summit and the Getting Out and About Easily event (February 2011).
• Review progress on Everyone’s Tomorrow – Newcastle’s Strategy for Older People and an Ageing Population The OPSB has reviewed progress against the five outcomes of Everyone’s Tomorrow.
The OPSB was satisfied with the progress being made in relation to access to information, advice and advocacy and access to health and social care services.
The OPSB was particularly interested in focusing on the other outcomes in Everyone’s Tomorrow, to which less attention had been paid and which could be grouped together under the umbrella of Newcastle – an age friendly city. As part of this work the Elders Council held its AGM in June 2010 on the theme of an age-friendly city and held a workshop with 100+ older people, seeking their
Agenda Item 6
Page 59

2
views on their homes and neighbourhoods. The information gathered at this session, together with data from the Residents’ Survey provided the starting point for a multi-agency workshop on the theme of Newcastle – An Age-Friendly City held in September 2010.
This work provided us with substantial evidence of the key issues affecting older people, but also highlighted that older people’s experiences vary widely depending on the neighbourhood in which they live. This led to a proposal to take a geographical approach to the age-friendly city work. At the same time, other initiatives were being proposed within the Wellbeing and Health Partnership on geographical approaches to wellbeing and health. After discussion with partners, it was concluded that it would be best to take this forward as a single, integrated piece of work and a project team has now been set up to scope and develop the work.
The OPSB continues to contribute to citywide initiatives which impact significantly on older people. These include:
One Core Strategy;
Older People’s Housing Strategy (including the Older People’s Housing Impact Assessment);
Movement and Access Plan (including contributing to the Local Sustainable Transport Fund bid).
• Joint Strategic Needs Assessment
The OPSB is currently working with Newcastle City Council to agree the process for the development of the Joint Strategic Needs Assessment. This will be a priority for the OPSB during 2011/12.
• Research into Practice
Prompted by a paper from the Elders Council, the OPSB has been working towards building stronger relationships between our academic partners and the work of the OPSB. Whilst older people have ample opportunity to participate in research, we are seeking ways of influencing the research agenda and finding more immediate and practical ways of putting research findings into practice. This concern is shared with the Wellbeing and Health Executive as illustrated in the Knowledge Exchange in Public Health planned for June 2011.
• Partnership Assurance Statement. The OPSB reviewed the Partnership Assurance Statement at its meeting in February 2011 and there are no major areas of concern.
• Engagement with older people. The Elders Council provides the main link with older people in the city and makes a significant contribution to ensuring that the voices of older people influence policy and service development through its on-going activity.
3 Areas of concern
Page 60

3
There are no significant areas of concern.
4 Next steps
Key priorities for the OPSB during 2011 are:
To progress the work on an age-friendly city through the work on geographical approaches to health and wellbeing;
To develop the Joint Strategic Needs Assessment for older people; and
To keep a watching brief on the development and implementation of the Older People’s Housing Strategy.
Report written by:
Colin Williams, Chair, Older People’s Strategic Board Adult and Culture Services [email protected] Barbara Douglas, Co-ordinator, Older People’s Strategic Board Quality of Life Partnership [email protected] 0191 233 0200
Page 61

Page 62
This page is intentionally left blank

Building user engagement: report to DMT, April 2011 Page 1
Building user engagement in Newcastle
Report to Adult and Culture Services Directorate Management Team 21st April
20111
Report by Peter Fletcher Associates Ltd
Introduction
In April 2010 Peter Fletcher Associates Ltd (PFA) was commissioned by the Council to undertake a time-limited piece of work to "ensure that a wide range of engagement opportunities exist and to locate these within a coherent infrastructure." That work has now largely been completed and this report sets out what we have done and makes a number of recommendations about how the work should be taken forward.
Overall approach
In the original invitation to tender the requirements for the work were set out as being to:
• Identify any gaps in existing engagement opportunities drawing on existing mapping information, and where necessary to create new arrangements.
• Establish a coherent network to link these engagement opportunities together.
• Establish a methodology to enable Adult and Culture Services to consult the network in a meaningful and representative way.
• Ensure that the arrangements put in place are sustainable in the medium term with no or minimal financial investment beyond the life of this project.
In other words there was an emphasis on putting in place structures to allow for effective engagement with service users (carers were at this stage explicitly excluded).
Service users that we talked to, however, said that the main problem with existing engagement was that it was difficult to see that it made an impact and they often felt that what they said was ignored. A lack of appropriate structures was not the issue. Rather what was needed was to embed an approach within the Directorate that led
1 Abridged version of the report for presentation and discussion at Wellbeing and
Health Partnership Executive.
Agenda Item 8
Page 63

Building user engagement: report to DMT, April 2011 Page 2
to effective engagement whatever the structures happened to be. Part of our work, therefore, has been to explore the concept of co-production as a core way of working within social care.
We took this point on board and whilst we are recommending some structural change, such as setting up a network, we have concentrated on changing practice in order to:
• Support users and carers to be able to speak up effectively, and
• Make user and carer engagement a part of the Directorate and service provider's day-to-day business.
We also proposed, and commissioners agreed, that the work should cover both users and carers. Whilst it is true that their interests are sometimes different in reality they are more often the same and some users will require the support of their carer in order to become engaged.
The current position
In October 2010 we produced an interim report where we looked at the current position with user and carer engagement in the City. These were our main conclusions:
1. There are examples of good practice in user engagement in Newcastle. However these are not widespread and the learning that comes from them is not shared across all services and user groups.
2. There are a number of different user groups that relate to specific client groups e.g. Launchpad, Elders Council etc. They are funded and supported in different ways and to very different levels, and some are not funded directly by the Council e.g. Youth Independence Forum. There are a number of gaps e.g. homeless single people, and families.
3. No-one in the Directorate has a clear view across current engagement activity. Engagement activities were described to us as being largely consultative in nature. The methods used are very traditional relying heavily on attendance at meetings.
4. Groups are most often currently involved in needs assessment. There is much less, if any, involvement in other parts of the commissioning cycle.
5. The Council has a Community Engagement Strategy that focuses on engaging with local communities and provides an overall strategic framework for engagement work across the Council. The Newcastle Partnership has agreed a Community Empowerment Framework which sets out how it will empower communities. There is no strategic framework specifically for engagement in adult social care and the Adult Social Care Directorate is not well tied in to the city-wide mechanisms.
Page 64
Building user engagement: report to DMT, April 2011 Page 3
6. There is little joint work between the Council and the PCT on this issue.
7. The Directorate does not have a clear policy on the payment of expenses to users and carers who get involved, and there is no reward or recognition policy.
8. There is no systematic mechanism in place to make sure that providers have effective user engagement mechanisms. The views of service users are not aggregated to inform future commissioning strategies.
9. There is little connection between approaches that engage with people as citizens and at the level of communities or neighbourhoods ('place') and those that engage people as service users ('people').
10. There is a clear recognition that the current approach towards engagement is no longer fit for purpose and needs to change. Furthermore it is understood that this is as much, if not more, about changing the culture within the Directorate as it is about setting up new mechanisms.
What we have done
One of our first steps was to set up a Planning and Reference Group to work with us throughout the contract. This had a broad membership including:
• Users and carers
• User and carer and citizen organisations (e.g. the Elder's Council)
• Organisations that represent or work with users and carers (such as Launchpad, Quality of Life Partnership, Drug User Forum and Your Voice Counts)
• Existing engagement mechanisms (Community Action on Health, Newcastle LINk, Citizens Assembly)
• Newcastle City Council - Adult and Culture Services Directorate and Community Engagement and Empowerment Service
• Newcastle Partnership
• NHS North of Tyne
The Group has been an invaluable help to us throughout the process and we wish to record our thanks to all the people who took part.
Early work focussed on interviewing key people to get an understanding of the current state of engagement in adult care and support services, mapping existing groups and the resources that were available to support this work.
In November we organised a large event to discuss how we could build engagement. This was attended by 120 people. One-third of the attendees were users and carers. Out of this a number of further areas of work were identified and we set up 8 action planning groups to look at these. All of these groups had a mixed membership involving workers from statutory and voluntary sectors and, in most cases, an input
Page 65

Building user engagement: report to DMT, April 2011 Page 4
from users and carers or organisations that work closely with them. We also organised a workshop for members of the Planning and Reference Group and the action planning groups to look at the issue of co-production.
Out of all of this have come the proposals and products that we consider in the next section.
Proposals and products
The output from our work consists of a number of documents that address the
following areas:
• Setting standards and principles for engagement.
• Establishing mechanisms to engage users and carers and promote dialogue
and joint working between users and carers and the Council.
• Putting in place policies and practices that will support effective engagement.
• Supporting information to inform engagement.
The full report includes all the documents that have come out of our work.
Key recommendations
Taken together, the outputs from this work constitute a comprehensive approach to building user and carer engagement. It will take time to implement them fully. We would urge the Council to adopt all of these proposals but these are the key ones where progress needs to be made quickly if this approach is to have credibility and deliver change.
1. Agencies (initially the Council and Council funded organisations) formally sign up to the standards and principles for user engagement as set out in the document agreed by the Planning and Reference Group. These provide an overarching framework for this work.
2. The Directorate agrees to support setting up a network of user and carer groups and organisations. This would be established as part of the arrangements HealthWatch but would have a distinct identity ('CareWatch'). To immediately start discussions with Newcastle LINk on setting up the network in advance of HealthWatch being commissioned.
3. The Directorate convenes a forum to bring users, carers and the Council together in a formal process to discuss issues of common concern. To invite the PCT and GP Consortia to join this forum.
Page 66

Building user engagement: report to DMT, April 2011 Page 5
4. A senior member of the Directorate's Management Team is given overall responsibility for ensuring effective arrangements are in place to support user and carer engagement.
5. Action is taken to fill in the gaps in existing groups to ensure that all people who use care and support services have a voice.
6. All service providers are required to put in place mechanisms for encouraging their service users to have a say in how services are provided by April 2012. The contract monitoring process will be used to ensure this happens.
7. The policies and good practice guidelines set out in the various documents produced by PFA and endorsed by the Planning and Reference Group are adopted by the Council. Other organisations are also encouraged to do the same. In particular the following policies should be implemented as quickly as possible:
a. reward and recognition
b. involving service users and carers in recruitment
c. involving users and carers in commissioning and procurement
8. Adopt co-production as a core way of working throughout the Directorate building on the actions identified in the workshop.
Resource implications
We have been conscious of the need to avoid, if at all possible, calling for additional resources to support user engagement. However given the current state of user engagement, the fact that there are gaps, that information is not always available in appropriate formats and that not all groups can engage effectively there are some resource implications arising from our proposals.
• Additional resources will be required to ensure users and carers can engage in current mainstream and social care engagement mechanisms e.g. by making information available in different formats.
• There are resource implications in the reward and recognition policy e.g. in paying out-of -pocket expenses to users and carers.
• There will be some resource implications for keeping information updated.
• Additional resources will be required to build engagement where there are gaps e.g. homeless people.
• Developing CareWatch as the overall network for engagement for adult social care.
Page 67
Building user engagement: report to DMT, April 2011 Page 6
The Council has already recognised the importance of some of these issues e.g. through its Information for All policy. Some can come from using existing resources differently e.g. funding for training to come from existing workforce development. Resourcing CareWatch should be considered as a part of the arrangements for establishing HealthWatch.
A key part of our approach is to build engagement into the culture and roles of existing staff, both within the Council, and with service providers. This will not cost more money and should be viewed as a key component in delivering on the Council's personalisation agenda through promoting choice, control and independence for service users and carers.
Overall therefore, we believe that there will be minimal resource implications, and considerable payback by creating a dynamic and inclusive set of engagement arrangements, as well as the culture change to go with this.
There is an issue with the current uneven spread of resources amongst existing funded user and carer groups. Some are relatively well-funded whilst others receive minimal support. There is no easy way to deal with this. We suggest the following steps:
• PFA to update the audit of resources to take account of the 2011/12 budget settlement.
• The Council, GP Consortia, NHS North of Tyne and YHN make a commitment to pool their resources for supporting user and carer engagement, creating a single pot.
• Existing funding is reviewed to identify any duplication and the biggest gaps in support and a commitment made by the above organisations to address these over a three year period. This may include shifting resources between existing groups. Wherever possible this will be done by agreement.
Next steps
The Planning and Reference Group discussed the next steps. They saw these points as being key to making progress:
• The importance of the City Council’s leadership
• The resource implications: it is more important than ever to highlight the need for resources to support this work.
• It is important that there is feedback given to everyone involved in this project – service users and staff – about what the Council decides to do, as well as what was learnt
• It is vital that the learning from this work does not go to waste (there are raised expectations at the same time as some cynicism about whether anything will change!)
We propose the following:
Page 68

Building user engagement: report to DMT, April 2011 Page 7
1. Following today's meeting the Directorate agrees how it can formally sign-up to these proposals and make it known that it has done so.
2. Other agencies will be asked to sign-up to supporting and implementing them as well. A meeting is being arranged with the two GP consortia to get their agreement. This should be followed by getting sign-up through the Newcastle Partnership and other forums.
3. PFA will put the outputs into a more coherent and user friendly format. They will be posted on the Community Empowerment website with a link from the health and Wellbeing website.
4. PFA will draft feedback to go to everyone who has been involved setting out what has been achieved and what will change as a result.
5. The Council should draw up an action plan showing where and when decisions are to be made on which recommendations to adopt, and how these will be implemented. This will form part of the feedback.
6. The Planning and Reference Group should be invited to continue to meet for a further six months, to support adoption and implementation.
Iain Kitt
Sheila Spencer
Richard Corkhill
Peter Fletcher
Peter Fletcher Associates Ltd
18 April 2011
Page 69

Page 70
This page is intentionally left blank