
Agenda item: Key decision - Meetings, agendas, and...
13
1 www.portsmouth.gov.uk Agenda item: Title of meeting: Health & Social Care Cabinet Decision Making Meeting Date of meeting: 24 th September 2015 Subject: 0-5 Public health services including Family Nurse Partnership Report by: Director of Public Health Wards affected: All Key decision: No Full Council decision: No 1. Purpose of report 1.1 This report is intended to inform the Cabinet Member for Health and Social Care of the new responsibilities for commissioning public health services for children aged 0-5 years. This includes the Family Nurse partnership, for which work is being undertaken to determine future requirements, based on the predicted number of mothers eligible for the service. 2. Recommendations 2.1 That the Cabinet Member for Health and Social Care notes that commissioning responsibility for public health services for children aged 0-5 years is transferring from NHS Wessex to the Local Authority on 1 st October 2015 2.2 That the Cabinet Member for Health and Social Care notes the recommendation that future funding for the Family Nurse Partnership should be based on the predicted number of mothers eligible for the service, recognising the financial pressures and other competing priorities for the ring-fenced public health grant. 3. Background 3.1 From 1 October 2015 responsibility for commissioning public health services for children aged 0-5 will transfer from NHS England to local authorities. The latter will therefore be responsible for commissioning the whole 0-19 years Healthy Child Programme, alongside the 5-19 programme which is already commissioned by the Local Authority and delivered by the school nursing and public health delivery teams. 0-5 services include health visiting (universal and targeted services) and Family Nurse Partnership (targeted service for teenage mothers). 3.2 Health Visitors lead the local delivery of the Healthy Child Programme for 0-5 year olds, providing all families with crucial evidence-based support, expert advice and intervention in the first years of life. The Healthy Child Programme (HCP) is a
Transcript of Agenda item: Key decision - Meetings, agendas, and...

1
www.portsmouth.gov.uk
Agenda item:
Title of meeting:
Health & Social Care Cabinet Decision Making Meeting
Date of meeting:
24th September 2015
Subject:
0-5 Public health services including Family Nurse Partnership
Report by:
Director of Public Health
Wards affected:
All
Key decision:
No
Full Council decision: No
1. Purpose of report 1.1 This report is intended to inform the Cabinet Member for Health and Social Care of
the new responsibilities for commissioning public health services for children aged 0-5 years. This includes the Family Nurse partnership, for which work is being undertaken to determine future requirements, based on the predicted number of mothers eligible for the service.
2. Recommendations 2.1 That the Cabinet Member for Health and Social Care notes that commissioning
responsibility for public health services for children aged 0-5 years is transferring from NHS Wessex to the Local Authority on 1st October 2015
2.2 That the Cabinet Member for Health and Social Care notes the recommendation
that future funding for the Family Nurse Partnership should be based on the predicted number of mothers eligible for the service, recognising the financial pressures and other competing priorities for the ring-fenced public health grant.
3. Background 3.1 From 1 October 2015 responsibility for commissioning public health services for
children aged 0-5 will transfer from NHS England to local authorities. The latter will therefore be responsible for commissioning the whole 0-19 years Healthy Child Programme, alongside the 5-19 programme which is already commissioned by the Local Authority and delivered by the school nursing and public health delivery teams. 0-5 services include health visiting (universal and targeted services) and Family Nurse Partnership (targeted service for teenage mothers).
3.2 Health Visitors lead the local delivery of the Healthy Child Programme for 0-5 year
olds, providing all families with crucial evidence-based support, expert advice and intervention in the first years of life. The Healthy Child Programme (HCP) is a

2
www.portsmouth.gov.uk
prevention and early intervention public health programme offered to all families that lies at the heart of the universal service for children and families. It aims to support parents, promote child development, reducing inequalities and thus contribute to improved child health outcomes and health and wellbeing, and ensure that families at risk are identified at the earliest opportunity. As part of the transfer, some universal health visitor reviews, which form part of the 0 to 5 Healthy Child Programme, are legally mandated for a period of 18 months.
3.2 Family Nurse Partnership
The Family Nurse Partnership programme (FNP) is an evidence-based, preventive public health home visiting programme for vulnerable first time young mothers aged 19 and under. Structured home visits, delivered by specially trained family nurses, are offered from early pregnancy until the child is twoiii.
3.3 FNP has been shown toiii,iv:
Reduce child abuse, neglect, A&E attendances and hospitalisation for injuries and ingestion.
Improve maternal education, employment and economic independence
Reduce domestic abuse
Improve child health and school readiness
Improve children's social, emotional and behavioural development
Improve maternal health and healthy behaviours
Reduce crime and anti-social behaviour
Support father's involvement in their children's lives
Provide substantial return on investment
3.4 FNP is part of the Healthy Child Programme. When a mother enrols on FNP, the HCP is delivered by the family nurse instead of by health visitors. The family nurse also plays an important role in any necessary safeguarding arrangements, alongside statutory and other partners, to ensure children are protected.
3.5 FNP is a licensed programme, with a clear service delivery model which must be adhered to. This is to ensure that the programme is implemented to maximise its' impact, based on the evidence base. This includes the number of visits nurses should make, topics they should cover; structure of the team, their qualifications and supervision requirements; monitoring and data collection requirements; access to copyrighted materials, clinical methods and tools; and a requirement that FNP should be funded until children on it reach the age of two.
4. Portsmouth's FNP service 4.1 The prebirth to 5 Board of the Children's Trust Board recognised the value of the
FNP programme and jointly applied for a service, with funding from Portsmouth City Council, maternity services and NHS commissioners. Due to the rigorous application process Portsmouth's application was not successful until the third attempt.
3
www.portsmouth.gov.uk
4.2 The service commenced in October 2011 and was expanded in January 2013 to a
total of 8 nurses. The service is now rated as one of the top performing in the
country.
4.3 Cost of the service The total annual cost of the FNP service is £410,000 per year. There are currently
139 teenage mothers in the local FNP caseload, with a maximum capacity of 200.
Nationally the average cost of the service is £3,100 - £3,600 per case per yearv.
4.4 Return on investment The Social Research Unit vi have estimated return on investment for the FNP of
£1.94 for each £1 invested. To be cost neutral, the Portsmouth service would need
to prevent the equivalent of two children going into care each year. Whilst this
cannot be proven, the low numbers of clients and their children seen by FNP in
care, suggest cost effectiveness on this measure alone. This is a conservative
estimate as it does not include other costs likely to be saved by the service such as
children in need, child protection cases, unemployment, education, health and crime
costs. Case studies from the FNP programme are provided in appendix 1 and 2,
and show some of the outcomes achieved through the programme.
4.5 FNP is a cost effective preventative programme. New programmes are being
established across the country; locally this includes Gosport and Havant, and
Rushmore and Basingstoke.
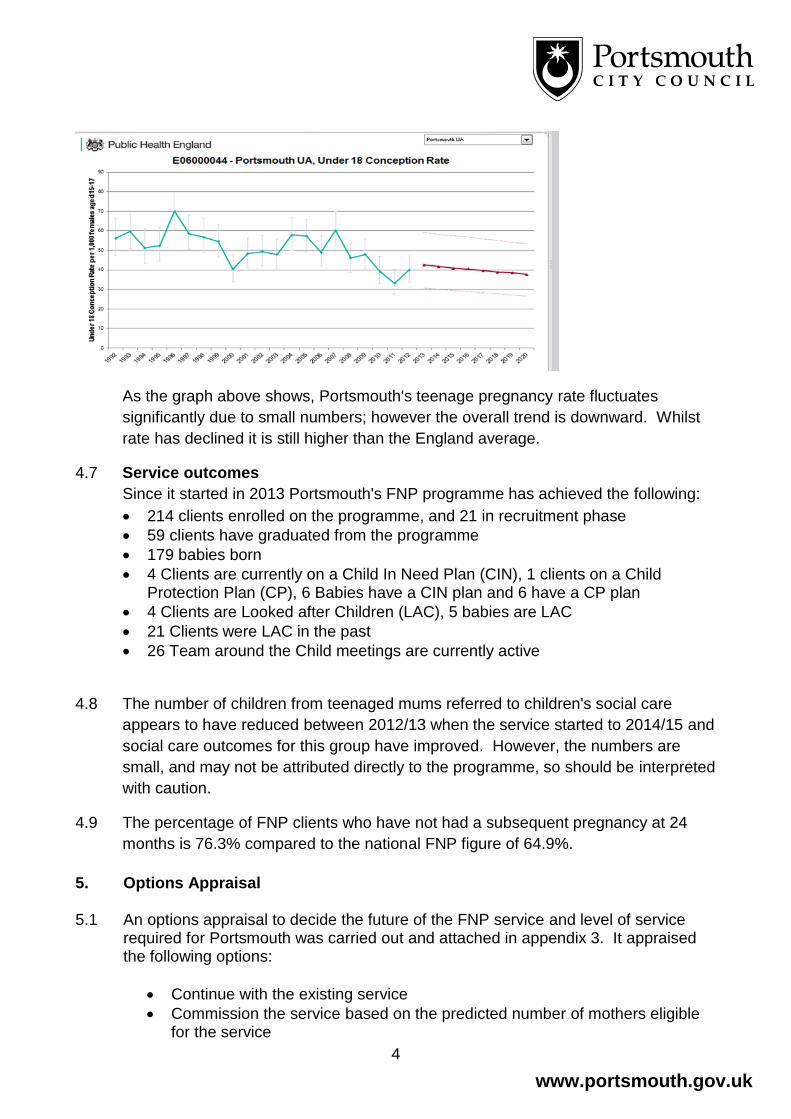
4.6 Quantifying the need in Portsmouth Portsmouth's under 18's teenage conceptions rate reduced between 2010 - 2013 as
the table and graph below shows. The number of pregnancies in this age group
decreased from 23.9 per 1000 to 15.4 in this time period. Data for 2014 will be
available at the end of August. New data from the Office for National Statistics will
include maternal age, so enable us to better model the number of teenage mothers
eligible for the FNP service.
Portsmouth teenage conceptions 2010-13 (Source ONS)
Age Year Conceptions per 1,000
Under 16 2013 7.3
2012 8.1
2011 6.1
Under 18 2013 24.8
2012 39.9
2011 33.3
2010 39.4
4
www.portsmouth.gov.uk
As the graph above shows, Portsmouth's teenage pregnancy rate fluctuates
significantly due to small numbers; however the overall trend is downward. Whilst
rate has declined it is still higher than the England average.
4.7 Service outcomes
Since it started in 2013 Portsmouth's FNP programme has achieved the following:
214 clients enrolled on the programme, and 21 in recruitment phase
59 clients have graduated from the programme
179 babies born
4 Clients are currently on a Child In Need Plan (CIN), 1 clients on a Child Protection Plan (CP), 6 Babies have a CIN plan and 6 have a CP plan
4 Clients are Looked after Children (LAC), 5 babies are LAC
21 Clients were LAC in the past
26 Team around the Child meetings are currently active
4.8 The number of children from teenaged mums referred to children's social care
appears to have reduced between 2012/13 when the service started to 2014/15 and
social care outcomes for this group have improved. However, the numbers are
small, and may not be attributed directly to the programme, so should be interpreted
with caution.
4.9 The percentage of FNP clients who have not had a subsequent pregnancy at 24
months is 76.3% compared to the national FNP figure of 64.9%.
5. Options Appraisal 5.1 An options appraisal to decide the future of the FNP service and level of service
required for Portsmouth was carried out and attached in appendix 3. It appraised the following options:
Continue with the existing service
Commission the service based on the predicted number of mothers eligible for the service

5
www.portsmouth.gov.uk
Stop the service
Commission/develop an alternative service
Review referral criteria to further target the FNP programme
5.2 The options appraisal identified the option with optimal cost benefit ratio is to commission the service on the basis of the predicted number of mothers eligible for the service. This does carry a risk of under/ over supply due to fluctuations in teenage conceptions. However, it is the most cost effective option, and the one with the best health outcomes and that carries the least financial and reputational risk.
5.3 The officer recognises the severe financial pressures the Council faces and that this
service needs to be considered against other competing priorities, for the ring-fenced public health grant.
6. Legal implications 6.1 There are no relevant legal comments with respect to the aims of the proposed
plan. 7. Finance 7.1 If the Cabinet Member for Health and Social Care agrees that the number of FNP
nurses should be determined by predicted number of mothers eligible for the service, financial implications will vary with teenage conception rates. The overall trend in the city is downward. Numbers of nurses required and the financial implications of this will be calculated once teenage conception data is available at the end of August 2015.
8. Equality Impact Assessment 8.1 If the service is commissioned according to predicted number of mothers eligible for
the service, there will be no change to the service in terms of equality. ……………………………………………… Signed by Director of Public Health: Background list of documents: Section 100D of the Local Government Act 1972 The following documents disclose facts or matters, which have been relied upon to a material extent by the author in preparing this report:
Title of document Location

6
www.portsmouth.gov.uk
The recommendation(s) set out above were approved/ approved as amended/ deferred/ rejected by ……………………………… on ……………………………… ……………………………………………… Signed by Cabinet Member for Health and Social Care

7
www.portsmouth.gov.uk
Appendix 1 - Case Study 1 Names have been changed. Sarah was 16yrs old when she was referred to me by her midwife. She lives with her mother; her father left her mother when she was born and no contact with him to date. Home conditions were observed to be poor, and Sarah’s mother is often off work with ongoing ailments. Sarah had a history of non-attendance at school for the past 2 years, and non-engagement with CAMHS service, after being referred for anxiety around school attendance. Relationship breakdown with partner since pregnancy; he has a history of substance misuse and DV in previous relationship. Sarah’s relationship with her mother was volatile, and Sarah was prone to aggressive outbursts towards her mother. Sarah’s mother works full-time, and Sarah had a reversed sleep pattern, where she slept during the day, and was awake through the night. Sarah had low self-esteem and anxiety which meant that she chose not to leave the home unless she was with a friend or relative. Sarah was identified as being at risk of PND due to isolation, and history of poor engagement with external agencies to date. Upon meeting her, she presented as quiet and distracted by ‘texting’ on her mobile phone; little eye-contact, and little verbal engagement – but she let me in!! It became clear that Sarah was not engaging with the midwife or attending for antenatal care, and concerns were raised about her ability to put her baby’s needs above her own in a safe, stable and loving home environment. The unborn baby was placed on a CP Plan with a view to a mother & baby foster placement following birth. Sarah continued to meet with me, and gradually she started to make eye contact with me, have opinions about topics I brought up and started to share her thoughts and feelings with me. Sarah and her mother have managed to improve and maintain home conditions. They prepared appropriately for the arrival of baby Ruby, and it was felt Sarah and Ruby could remain at home following the birth. Using Motivational Interviewing, and the Programme facilitators, we were able to build a relationship that put Ruby’s needs as a priority. PIPE activities to date with Sarah have supported Sarah’s learning to be the best mum she can to Ruby. I have seen Sarah gain self-confidence as an individual and as a parent. I have seen baby Ruby, who is now 8mnths old, form a positive attachment with Sarah, and they appear to have a positive bond with each other. Sarah now has good engagement with professionals, and Ruby’s immunisations are up-to-date. Sarah is now confident enough to make health appointments for herself and Ruby – long term contraception was in place 3 weeks post birth.(Impact: no repeat pregnancy) The Programme promotes self-efficacy to bring about ‘change’, and Sarah has now applied to start college in September.(Impact: not NEET). Work around positive relationships, lifestyle choices, appropriate patterns and routines for Ruby, and Sarah’s own goals and aspirations, has enabled Sarah to work through conflict in the home with her mother. She and her mother have a calm and positive relationship with each other,
8
www.portsmouth.gov.uk
and enjoy living together. Sarah often takes Ruby to meet with me at the sensory room of the local children’s centre. She has successfully turned around her reverse sleep pattern to meet Ruby’s needs. (Impact: good bonding and attachment) Ruby has stepped down to a CIN Plan, with a view to stepping down to TAC meetings if plan requirements continue to be met. Sarah now actively engages with professionals and talks positively about the FNP Programme. She takes pride in her achievements and capacity to parent Ruby, and Ruby is developing and progressing appropriately for her age. She is looking forward to returning to education, and continues (mostly) to let me in!!!!!
Appendix 2 - Case Study 2 For client protection the names of the clients have been altered.
Sally was 17 years of age when she was referred to the FNP programme by her YOT worker in
April 2014. She was reported to be approximately 8 weeks pregnant but this had not been
confirmed because she had not attended her GP or Midwife. It was reported that Sally had a very
‘troubled’ past and had been a child looked after since the age of 5years, the YOT worker reported
poor engagement with professionals and that Sally and her boyfriend Chris were known to be
aggressive and confrontational and were currently homeless, sleeping on friends sofa’s. I was
supplied with a mobile telephone number for Sally and her last known address which was the
Foyer in Portsmouth.
After several attempts I was able to contact Sally and we agreed to meet in a café in Portsmouth,
Sally was very closed and suspicious about my role and why I wanted to meet her. I was able to
reassure her that the programme was voluntary and we discussed the benefits to mothers and
their babies if they were to undertake the programme. We arranged to meet again and Chris was
invited as well if he wanted to attend. Engagement over the next few weeks was difficult but I
remained in contact via texts, calls and visits in community café’s. In this time I learnt about Sally’s
past childhood, both her parents had issues with alcohol and drug dependencies, she had an older
brother whom she had never meet as he was adopted at the age of 3, he was reported to be in and
out of prison. Her parents separated when she was a baby and she spent time with both of her
parents, their lifestyle was reported as chaotic and frightening with numerous incidents of Domestic
Abuse. Sally did not recall feeling loved or safe as a child and there were many times when she
was left alone hungry and cold. Her case is well known to Children’s social care and she was on a
child protection plan for a lot of her childhood. She was taken into care at 5 when her mother left
her locked in a flat on her own for 2 days when she was with her friends on a drug and alcohol
binge. Sally was intermittently reunited with her parents but on each occasion this broke down, her
father died of an overdose when Sally was 8 and her mother‘s whereabouts have been unknown
since Sally was 12. There was no other family member known to Sally.
Sally has lived in approximately 3 different care homes and 15 different foster homes, she reported
herself to be ‘hard work ‘was excluded from all of her schools, she first drank alcohol when she
was 9 (supplied by her mother and her then partner), cannabis at 11 and harder drugs such as
ketamine, heroin and cocaine at approximately 13. She recalls being sexually abused by various
male adults in her life 2 of these males were her mother’s partners. She was sexually active at 12

9
www.portsmouth.gov.uk
and whilst she did not recognise herself at being sexually exploited she had attended drug and sex
parties from the age of 12/13. She had a termination at the age of 14. She did not regularly attend
school and had no qualifications, she was known to the police for various incidents of theft and
anti-social behaviour. Sally was asked to leave the Foyer due to her behaviour and had been sofa
surfing since that time.
Sally had met her partner Chris aged 19 at the Foyer, he too had a troubled past, he had served 2
prison sentences for robbery and assault, he reported being sexually abused for most of his
childhood by his paternal Uncle and Grandfather , his father was a drug addict and there was a lot
of violence in his family home. He too had very poor school attendance, no formal qualifications
and was homeless. Sally had been in a relationship for approximately 6 months before she
became pregnant. Sally reported to smoking 20 cigarettes a day when I met her and having about
1 to 2 joints a day, Chris admitted to smoking, regularly using cannabis and some cocaine along
with legal highs, when he could afford to he drank alcohol and boasted that on one occasion he
drank 2 bottles of vodka. They both had poor diets and drank several high energy drinks a day.
They were distrustful of professionals as they both felt that they had been let down in the past.
What struck me very early on in the relationship was how open they both were with me and they
talked in great depth about their pasts but they appeared to be removed from their own
experiences and almost spoke in the 3 party. I was also very open with them about my
safeguarding responsibilities and how I worked very much alongside other agencies. We explored
what it felt like to them to be parents and we talked about their developing baby, I was able to
support both Sally and Chris to attend the GP and the midwifery clinic, after a proper medical
assessment it was confirmed that Sally was a further 6 weeks along in her pregnancy than she had
originally thought .
I was in contact with other agencies such as Social Care, Housing, YOT and Probation I completed
a CAF with Sally and we arranged our first Team around the Child meeting when she was 22
weeks pregnant at a local Children’s Centre. Housing was identified as a priority and an application
to supported housing was made and within 4 weeks a joint place at a hostel was secured. Both
Sally’s and Chris’ behaviour could be erratic at times but they both were making some positive
changes, Sally had cut down on her smoking and had completely stopped the cannabis and Chris
reported only to smoking and using cannabis on occasion. They were eating more healthily and
regularly and had significantly cut down the high energy drinks, they both were very proud of
themselves when they made their first spaghetti bolognese. The programme materials supported
the exploration of attachment and bonding and enabled Sally and Chris to think about what was
best for their baby, their engagement with me was good and they achieved over 90% dosage of
the programme in the Pregnancy phase. Sally and Chris at times revealed their fear about being
parents and not wanting to repeat their own childhood’s experiences for their child. Trust was a
particular difficulty for them and whilst they worked with me and the programme their relationship
with other professionals was strained especially after a section 47 assessment was completed and
their unborn baby was placed on the child protection register.
Whilst Sally and Chris continued to make some health changes in their life, their past also
impacted upon on them, Chris was arrested and charged with aggravated burglary and did not
receive bail, he was kept in custody, Sally felt very alone and missed Chris, it was apparent how
much she relied on him for emotional support although she recognised that he was not a positive
influence in her life. Although distracted at times Sally really enjoyed the programme materials
including my doll and PIPE activities, she loved to hear about how baby was developing and felt
10
www.portsmouth.gov.uk
very proud of herself for making changes, her aspiration was to be the best mum and have a
happy home that was filled with love.
There was conflict with her key worker in the Hostel and concerns that Sally was not adhering to
the rules, she was often out late and did not always return at night, a decision was made at the
core group to secure a mother and foster baby placement for Sally when the baby was born for
more intensive support and assessment of her parenting ability. Sally was very opposed to this as
she expressed she had not had a positive experience of foster homes as a child.
Baby Paul was born in October 2014 at term, he was a healthy weight and Sally breast fed him for
3 weeks, she reluctantly moved to the mother and baby foster placement. Initially Sally cared for
Paul well, sensitive attuned parenting was observed by professionals and Paul was thriving
meeting all of his milestones. Sally enjoyed attending Children Centre’s with Paul especially the
sensory room. When baby Paul was 5 months old, Sally’s behaviour was erratic and this was
intensified when Chris was released from prison following the collapse of his trial. It was a
condition that Chris was not to have unsupervised access to Paul but social workers became
aware of Sally bringing Paul to meet Chris. Sally was very torn between wanting to be with Chris
but also wanting to be a good mum to Paul, she disclosed to me again her fears of failing as a
mum and felt that she was not old enough and needed to work more on becoming settled, she was
able to identify Paul’s needs and was aware how important consistency and security was for him,
she was unsure whether or not she was the right person to provide this. When Sally was
challenged a further time about meeting with Chris, she left the foster placement leaving Paul
behind; no professional had contact with her for over a week. Sally was not taking my calls or
answering my texts, after about 2 weeks I had a call from her to say that she was staying at friends
with Chris and wanted to have contact with Paul, social care arranged supervised contact which
Sally attended. At this time care proceedings had commenced, I met with Sally weekly and we
were able to explore her feelings towards Paul and the internal conflict that she felt, she made a
decision to voluntarily place Paul for adoption, she loved him but recognised that it was not the
best time for her to have a baby, the weeks leading up to his adoption were very difficult and with
the support of the adoption social worker and myself Sally was able to prepare as best as she
could for goodbye.
Sally demonstrated great reflective skills and insight into the needs of her baby, she desperately
wanted to be the best mother she could and wanted to change the trajectory of intergenerational
disadvantage for him. A visit she was keen to undertake with me was to contraception services to
have an implant fitted as she stated she believed she would not be ready to be a mother again for
at least another 5 years, if at all. Sally demonstrated that she was able to access services that
could support her and she was able to recognise services in the community that would allow her to
plan for her future, she agreed to attend some counselling and also attend Housing in order to
reapply for a more secure tenancy. Her relationship with Chris ended as she felt his drug taking
had escalated and that he did not support her when she was making the decision to have Paul
adopted.
Whilst Sally’s case study may sound as though she failed, I believe it demonstrates the power that
the FNP programme has to foster a trusting relationship with a very damaged teenager, and to
allow her to explore the concepts of love and security and the needs of a child’s being paramount.
This case highlights the complexity of a child having a child and professionals working with these
vulnerable teenagers so that the best outcomes can be achieved for both the baby and the parent.

11
www.portsmouth.gov.uk
Appendix 3 - Options appraisal
Options for the Future of FNP Service Due to the time it takes for FNP nurses to be trained, and the commitment required to work with
families for 2 ½ years, until the child is 2 years old, when the programme was established
commissioners across the health and social care system committed to the programme initially for
four FNP nurses and one supervisor in 2012 and then in Jan 2013 the service was added to by
funding an additional four nurses. This time period will end in early 2016 when the last babies are
two years old , therefore the Local Authority is asked to renew its commitment to the programme
for a further 2 ½ years.
Option 1 - Continue service as before Make no changes to the current service of 8 FNP nurses other than recruiting to fill the vacant post
so that they can build up to working at full capacity.
Strengths
No change, therefore no risk of destabilising the currently established system.
Limitations
This will mean a commitment to funding a full 2.5 year cycle. If the teenage pregnancy rate
continues to decrease then this may mean that this option is decreasingly cost effective during the
duration of the 2.5 year funding cycle.
Costs and benefits
Costs are expected to remain the same as the previous funding cycle - £410000.
Potential benefits include changing the trajectory of intergenerational disadvantage, reducing the
numbers of future teen pregnancies, increasing sensible use of contraception, increasing numbers
of infants that are safely and responsively fed, reducing harmful behaviours such as abuse of
alcohol, nicotine and other unhealthy substances, increasing education attainment and
employment, improve mental health, reduce crime, less reliance on benefits system, reduce
domestic abuse and neglect, improve parental and infant attachment and prevent a rise in LAC,
reduce demands on health care system.
Option 2 - Review need and commission current service based on this As FNP services are targeted specifically at mothers of 19 and below, and there are strict licensing
guidelines outlining FNP nurses caseload, teenage conception data could be used to calculate
current needs, and predict what is needed in future.
Strengths
Most cost-effective option.
Limitations
It takes year to train a FNP nurse to the point where they can carry a full caseload of 25. If the
service is re-commissioned with significantly fewer FNP nurses then decide that we need to
increase the service capacity we will have a considerable training lag time before the service is
fully functional. Teenage pregnancy rates do fluctuate, and whilst modelling should make some
account for this, there is a risk demand may exceed supply at times.
12
www.portsmouth.gov.uk
Costs and benefits
Potential for cost savings assuming that the reducing teenage conception rate equates to reduced
need for FNP nurses over time.
Benefits might be seen in relation to short term cost savings, skill sharing, peer education / learning
and team working across the wider public health team
Option 3 - Stop the service
Strengths
Could release short term cost savings to the PCC budget.
Limitations
The FNP service is delivering measurable public health improvements and it would be difficult to
justify discontinuing this as it could lead to poorer public health, educational, social care and
employment outcomes to some of the most vulnerable teenagers and children in Portsmouth.
Costs and benefits
Relatively small short term saving in relation to potential for increased costs as detailed below:
Social care
o Foster care - up to £33,000 per child / year
o Residential care - up to £154,100 per child / year
o Children in Need - up to £11,458 per child / year
Education, training and employment costs
o NEET - up to £4528 / year
o Improved school readiness - up to £1,023 / year
Health
o Conduct disorder - up to £150,000 per child / lifetime
o Mental health services - £2,148 / year
o Anxiety and depression - up to £956 per adult / year
o A&E attendance with treatment - up to £130 / attendance
Criminal justice
o Domestic violence incident - up to £2,766 / incident
o Time in Young Offenders' Institute - up to £21,268 / year
o Incident of crime - up to £647
Option 4 - Deliver a different service using the FNP principles
Strengths
Potentially marginally cheaper in the long-term if the new service was continued for long enough
for these savings to be demonstrated.
Limitations
This is not feasible as the FNP principles of care are clearly linked to the FNP license / contract of
use.
13
www.portsmouth.gov.uk
The start-up costs would be high as a new programme would have to be written and it is not clear
where we would be able to get the skills and expertise required for this.
FNP practitioners are highly trained and skilled. A new model risks losing and destabilising the
current existing workforce.
Reputational risks - Portsmouth is currently seen as one of the highest performing FNPs in the
country. Significant changes therefore run a high risk of challenge and potentially negative
attention.
Costs and benefits
As the majority of the FNP is staff costs, a local service is unlikely to be significantly cheaper.
Option 5 - Change the referral criteria to target FNP further
Strengths
Possibility of short term financial savings.
Limitations
The FNP programme is already targeted very specifically at mothers 19 and under, and are
targeted at this level based on national evidence/ modelling. These are some of the most
vulnerable parents in the City, so it would be challenging to restrict this criteria.
Reputational risks as Portsmouth has a high profile as one of the highest performing FNPs in the
country. Changes to criteria without a strong evidence base to support the decision run the risk of
negative attention.
Costs and benefits
Reduced costs to the public health budget if FNP were targeted further.
High probability of increased costs to other PCC services, and the wider welfare/ social care/
health/ other systems as highlighted above.
i http://www.fnp.nhs.uk/about ii https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/407645/overview2-health-
visit.pdf iii http://fnp.nhs.uk/research-and-development
iv http://fnp.nhs.uk/research-and-development/proven-results
v https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213369/Apteligen_FNP-
costs-study_SUMMARY-REPORT_FINAL_310113_FOR-WEB.pdf vi Social research unit (2013) Investing in Children http://investinginchildren.eu/interventions/family-nurse-
partnership


















