Federal Health Care Reform 2009: Affordable Health Care for All
Upload
careermindsCategory
view
133download
0description

Healthcare Reform Briefing: What HR Should Know
Sponsored by

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Discussion Topics
• What is happening in 2014?
• Employer interaction with public exchange
• Employer strategies for 2014 and beyond
• Emerging healthcare costs
• Closing thoughts

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
2 December 8, 2013 2 December 8, 2013
Benefits and/or compensation strategy and planning
Recruiting and/or outplacement, I never touch the benefits
HRIS and administration, I have to make sure benefits run
smoothly
All of the above
None of the above, I came for the free shirt
Who is here today? My main focus within HR is…
Choose all that apply.
Please Respond

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
What is happening in 2014

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
2014 is a significant year … Consequences of Affordable Care Act (ACA)
Design &
Marketplace
Changes
No lifetime
dollar limits/ pre-exiting
condition limits
Restricted annual
dollar limits
No waiting period
over 90 days
Out of Pocket Maximum
Wellness Incentives
Exchanges
Employer
mandate
and shared
responsibility
Minimum plan value
and contribution
requirements
(delayed)
Fees
Comparative
effectiveness
research (PCORI)
Fees on
insurers
Manufacturer’s
fees
Temporary
reinsurance
programs
Higher plan
enrollment
Dependents to
age 26
30-hour eligibility
Individual Mandate
Medicaid Expansion
Auto enrollment
(delayed)

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Employer Mandate and Shared Responsibility High Level Requirements…
Offer cover to “full-time employees” – “Minimum essential coverage”
– Coverage offer to 95% of FT employees and dependent children considered offer to “substantially all”
– FTE is any employee who works on average 30 or more hours per week
– Must offer to FTEs and their dependent children under age 26 (but not required to offer to spouses or domestic partners)
“affordable” health care coverage – An employee’s required contribution for self-only coverage cannot exceed
9.5% of the employee’s household income
with a “minimum value” – The actuarial value of the plan must be at least 60% - The calculation of the
anticipated percentage of the cost of the “essential health benefits” covered by a plan
or, face potential tax “penalties”

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
6
New in 2014: Individual Mandate
All individuals
must have health coverage
Pay penalty
2014
Greater of $95 (single) | $285 cap (family)
or 1% of household income
By 2016
Greater of $695 (single) | $2,085 cap (family)
or 2.5% of household income
OR

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Single
individual
Family
of four
% of
FPL** Annual household income
Household income >400% of FPL
not eligible for subsidy through
marketplace
400% $45,960 $94,200
300% $34,470 $70,650
200% $22,980 $47,100
150% $17,235 $35,325
138% $15,856 $32,499
100% $11,490 $23,550
* Not all States have agreed to expand Medicaid to 138% of FPL
** Based on 2013 FPL
7
Public Programs in 2014 Medicaid
Expanded to anyone below
138% federal poverty line
Not all states have agreed to expand coverage
• In these states, federal subsidies may be available for certain people to buy coverage
• Those ineligible for Medicaid or federal subsidies may have no option for subsidized coverage other than employer plan (if available)
Insurance plan options available on exchanges that are operated by states or federal government (or a state/federal partnership)
• Exchanges will conduct open enrollment: Oct 1, 2013 to Mar 31, 2014
• If household income is between 100%/138% and 400% of federal poverty level (FPL) – and individual does not have access to affordable employer coverage that provides minimum value– federal government will provide subsidies to buy insurance on exchanges
Medicaid Expansion Public Exchanges
Public Programs in 2014 Medicaid, Public Exchanges and Subsidies
Subsidies

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Employer Requirements in 2014
8
Ta
xe
s a
nd
Fe
es
• PCORI.
• Temporary Reinsurance Fee.
• Health Insurer Fee.
Co
mm
un
ica
tio
ns • SBCs.
• W-2 reporting of health care costs.
• Exchange Notice.
Pla
n D
es
ign
Re
qu
ire
me
nts
• Maximum 90 day waiting period.
• No limits on pre-existing conditions or essential health benefits.
• Limits on out-of-pocket maximums; counting copayments against OOP max.
• Expansion of Wellness incentives.
• Coverage for clinical trial related services.

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Interacting with the public exchange

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
10
Healthcare.gov

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
11 December 8, 2013 11 December 8, 2013
1%
10%
20%
40%
What percent of large employers (with over 500 ees) are going
to terminate medical coverage in the next three years?

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
New in 2014: Public Exchange (aka Public Marketplace)
0 5 10 15 20 25 30 35 40 45 50
Employer
Individual
Uninsured
Medicaid/CHIP
Medicare/Gov't
Percent of Population by Current Health Insurance Source*
*Source: U.S. Census, 2011
• Almost all large employers say they will continue to provide health care
benefits in 2014 and beyond.
• Created by ACA.
• Structured marketplace to sell and purchase health insurance operated by states or
federal government (or a state/federal partnership).
• Government subsidized medical coverage for low income individuals and families.
• Exchanges will conduct open enrollment: Oct 1, 2013 to Mar 31, 2014.
Will benefit from government programs – Expanded
Medicaid and Public Exchanges in 2014
12

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
What do the public exchanges do?
13 December 8, 2013
Manage Plan Activities
Determine eligibility, enroll individuals
Assist consumers
Provide financial management
Ensure plan accountability
© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
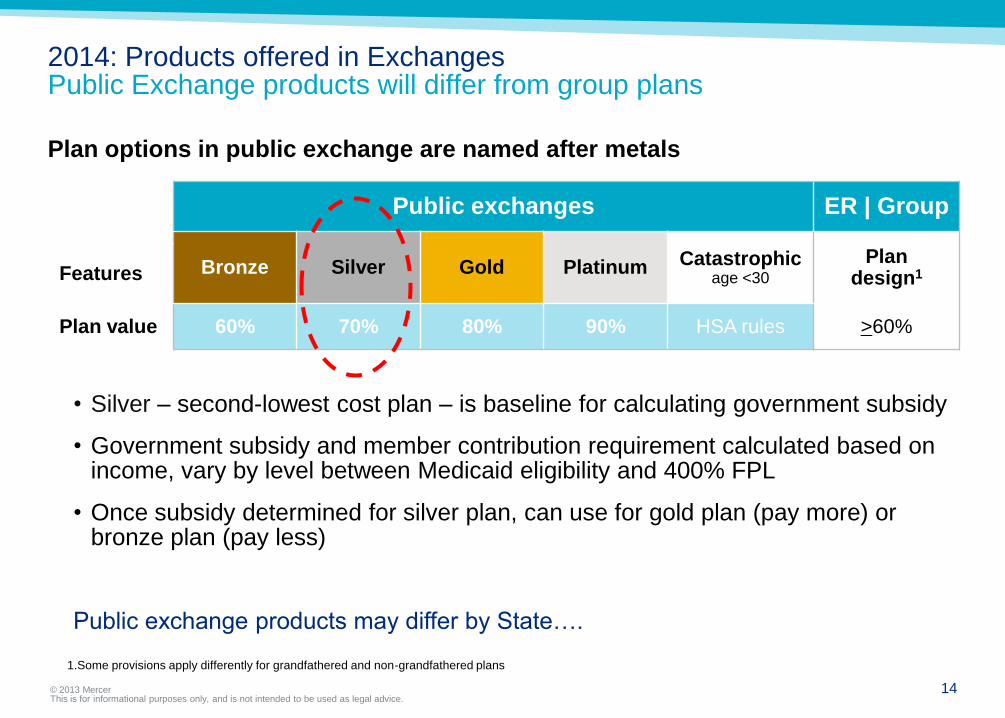
2014: Products offered in Exchanges Public Exchange products will differ from group plans
Plan options in public exchange are named after metals
Public exchanges ER | Group
Bronze Silver Gold Platinum Catastrophic age <30
Plan design1 Features
Plan value 60% 70% 80% 90% HSA rules >60%
14
1.Some provisions apply differently for grandfathered and non-grandfathered plans
• Silver – second-lowest cost plan – is baseline for calculating government subsidy
• Government subsidy and member contribution requirement calculated based on income, vary by level between Medicaid eligibility and 400% FPL
• Once subsidy determined for silver plan, can use for gold plan (pay more) or bronze plan (pay less)
Public exchange products may differ by State….

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Public Exchanges Status of State Exchanges (as of March 2013)
15 15
Sources: Kaiser Family Foundation (states); HHS, HealthCare.gov (territories)
Default to federal exchange 27 Declared state exchange 22 Planning partnership exchange 7

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Employers and Public Exchanges How Will It Work When Employees Apply For Subsidies?
Individual applies to Exchange
Provides & attests to certain info including:
• income and family size
• lowest cost employer plan option that meets minimum value (employee only cost)
1 Exchange verification
Verifies income and other info
Verification process for employer coverage (statistical sample only)
Individual can enroll during verification process
2 Exchange Eligibility Notice
• Notice to individual of eligibility determination after verification complete
• Notice to employer if individual determined eligible for exchange subsidies after verification complete
3
Employer Appeal 4 IRS reporting &
reconciliation
After close of calendar year, IRS has at least three sources of info to confirm subsidies were provided correctly:
• Employer reporting
• Exchange reporting
• Individual tax filing
5
16
• Employer requests appeal within 90 days of notice described in step 3
• Exchange tells employee of appeal request
• Written appeal decision w/in 90 days of receipt of appeal request
IRS Employer Shared Resp process
6
IRS has said, after employee tax returns for coverage year are due:
• IRS will contact employer about possible liability
• Employer response
• IRS notice & demand for payment

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
17 December 8, 2013 17 December 8, 2013
Few will be eligible
10%
20%
40%
All employees are eligible
What percent of your organization’s employees are going to
be eligible for the subsidy on the public exchange?
Choose all that apply.
Please Respond

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
18
What household income is needed to receive subsidized government insurance?
May be eligible for subsidy
Single
individual
Family
of four
% of
FPL** Annual household income
Household income >400% of FPL
not eligible for subsidy through marketplace
400% $45,960 $94,200
300% $34,470 $70,650
200% $22,980 $47,100
150% $17,235 $35,325
138% $15,856 $32,499
100% $11,490 $23,550
* Not all States have agreed to expand Medicaid to 138% of FPL ** Based on 2013 FPL
Medicaid eligible*
Income segments
under health reform
No government subsidy

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
Employer Strategies – 2014 and Beyond

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
*Projected
Source: Mercer’s National Survey of Employer-Sponsored Health Plans; Bureau of Labor Statistics, Consumer Price Index, U.S. City Average of Annual
Inflation (April to April) 1990-2013; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey (April to April)
1990-2013.
The Good News: employers expect to hold per-employee health benefit cost growth to 4.8% in 2014 But the increase in per-employee cost does not reflect rising enrollment
17.1%
12.1%
10.1%
8.0%
-1.1%
2.5%
0.2%
6.1%
8.1%
11.2%
14.7%
10.1%
7.5%
5.5% 4.8%*5.0%*
4.1%
6.1%6.9%
6.3%6.1%6.1%6.1%7.3%
2.1%
-2.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Workers' earnings
Annual change in total health benefit cost per employee
Overall inflation

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
21
Issues That Are Top of Mind for Employers as They Look Beyond 2014
Continued cost increase due to Affordable Care Act.
Educating employees about their choices and supporting informed
decisions.
Handling employee questions about the public exchange.
Administrative issues (tracking employee hours, look-back period).
Staying on top of all the Affordable Care Act requirements.
Anticipation of the excise tax in 2018.
Source: Mercer Survey, HCR Road to Implementation, June 2013

© 2013 Mercer This is for informational purposes only, and is not intended to be used as legal advice.
Employers React to Affordable Care Act in 2014 & Make the News…
UPS drops coverage for working
spouses and estimates covering
children to age 26 will cost $60M
Starbucks announced that it will not be
cutting benefits for spouses/partners or
reducing hours for workers so that they do
not qualify for benefits
Darden and Sears joined a fully insured
private exchange and Darden stopped
offering full time qualifying hours to many
employees
Delta Airlines faces an increase of $100M
in medical costs in 2014 between normal
trend and ACA requirements (appears to
be at least 38% of the increase)
Xerox is increasing their working
spouse surcharge to $1,500 annually in
2014
Walmart has been focusing on hiring
temporary employees to manage
healthcare costs under ACA
The Hamilton School District in
Trenton, NJ will be limiting substitute
teachers to 4 days per week to avoid
30 hour per week threshold
Clothing retailer Forever 21 (27,000
employees total) announced
reclassification of non-management
positions from FT to PT effective Sept. 1,
2013 based on a reduction of hours to a
maximum 29.5 hours per week
22

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
23 December 8, 2013 23 December 8, 2013
Status quo – perhaps tweak the current approach and monitor
Introducing High Deductible Health Plans (HDHPs)
Adding a 60% plan or “low” option
Focusing on health management or wellness incentives
Other changes such as adjusting eligibility for spouses, etc.
Is your organization thinking or considering any of the
following to manage costs?
Choose all that apply.
Please Respond

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
December 8, 2013
Employers’ responses are all over the board!
24
24% Make all
employees
eligible for
the FTE plan
17% Offer the FTE plan
to some, but not
all, newly eligible
employees
27% Add a
lower-cost
plan for
newly
eligible
hourly
employees
31% Add a low-
cost plan
as the
default for
auto-
enrollment
13% Where contributions
are “unaffordable”
add a less
expensive plan
51% Change workforce strategy so fewer employees work 30+ hours/week

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
Public Vs. Private Exchanges What is the Difference?
December 8, 2013 25
Medical,
prescription
Dental, vision, life,
voluntary, plus more
Government
sponsored
Employer, broker,
TPA, association
Actives, retirees
PUBLIC PRIVATE
Open Closed
Single or
multiple carrier
Individuals Group plans
Insured or
self-funded
Standalone
dental
Insured only

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
Private Exchanges In a Picture
EXCHANGE
Ven
do
rs
& c
arr
iers
Medical Dental Ancillary
Ben
efi
ts
ad
min
Eligibility &
enrollment
Consolidated
billing
Additional
features
Co
ns
um
er
ex
pe
rie
nc
e
Full product suite with choice of plans
Health Life, accident
& disability Voluntary
26
$
$
Employer
contribution
Consumer
enrollment portal
Decision tools
&/or call center
Multiple payment
models
27 December 8, 2013
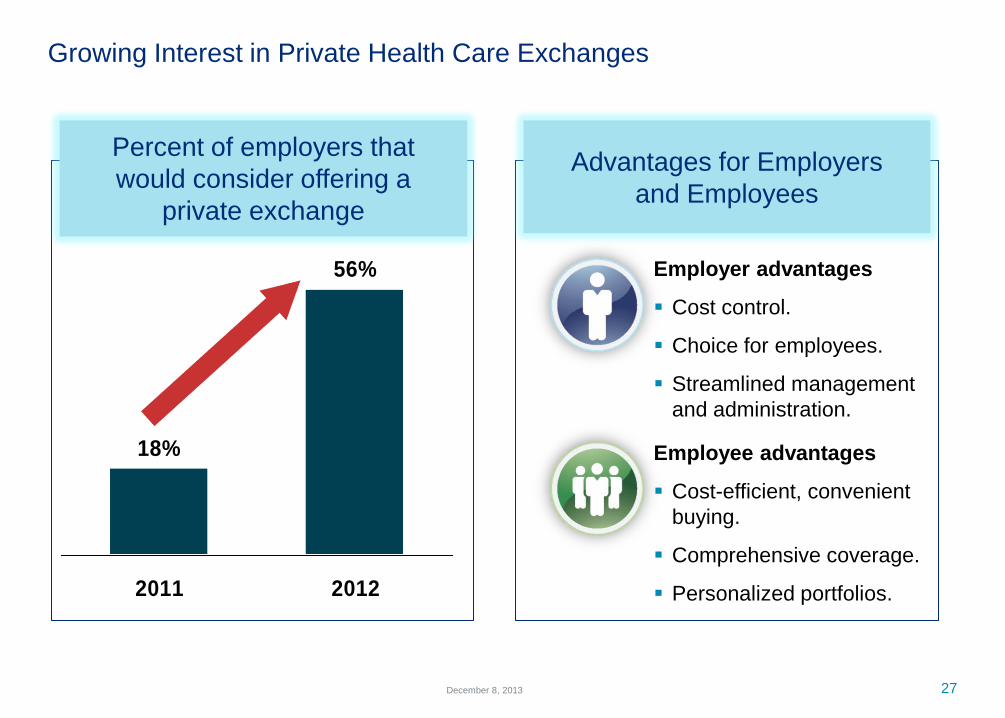
Growing Interest in Private Health Care Exchanges
18%
56%
2011 2012
Percent of employers that
would consider offering a
private exchange
Employer advantages
Cost control.
Choice for employees.
Streamlined management
and administration.
Employee advantages
Cost-efficient, convenient
buying.
Comprehensive coverage.
Personalized portfolios.
Advantages for Employers
and Employees
© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
Closing thoughts

© 2013 Mercer This is for informational purposes only and is not intended to be used as legal advice.
Closing Thoughts…
• Short term – Employers focused on cost management
and ACA compliance
– Expanded eligibility, minimum plan design, and affordable
contributions in 2015.
– Excise tax in 2018.
• Still some unknowns about the ACA
– Auto-enrollment.
– Reporting and disclosure.
– Could there be more delays?
• Longer term – things will change!
– New products/approaches.
– Funding changes.
– Delivery system transformations.
29

MERCER
Services provided by Mercer Health & Benefits LLC.
Thank You

MERCER
Mercer is not engaged in the practice of law and this presentation, which
may include commenting on legal issues or regulations, does not
constitute and is not a substitute for legal advice. Accordingly, Mercer
recommends that employers secure the advice of competent legal
counsel with respect to any legal matters related to this report or
otherwise.
The information contained in this document and in any attachments is
not intended by Mercer to be used, and it cannot be used, for the
purpose of avoiding penalties under the Internal Revenue Code or
imposed by any legislative body on the taxpayer or plan sponsor.