RED ROCKET RED ROCKET FLY HIGH, RED ROCKET RED ROCKET PUT MONEY IN MY POCKET YEAH!
AF in 2014
Andrew Staniforth
Mayo Course
March 2014
European Heart Journal 2010; 31: 2369–2429
www escardio.org/guidelines

For stroke prevention in AF, which of the following is true?
1. Aspirin is adequate for atrial flutter with normal heart
2. Aspirin only reduces the stroke risk by 40%
3. Paroxysmal and persistent AF should generally be treated the same
4. Aspirin should generally be given if CHADS2 = 1
5. Patients with CHADS-VASC ≥2 should definitely be anticoagulated
Q1 (Indications for anticoagulation)
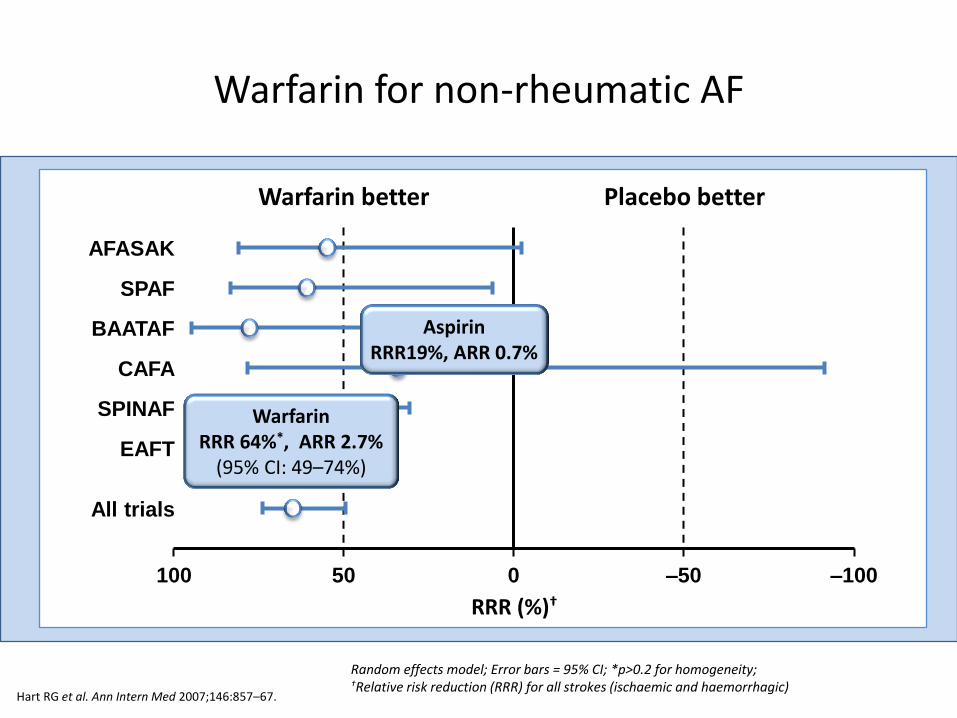
Random effects model; Error bars = 95% CI; *p>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic)
Warfarin for non-rheumatic AF
Hart RG et al. Ann Intern Med 2007;146:857–67.
Warfarin better Placebo better
RRR (%)†
100 –100 50 0 –50
AFASAK
SPAF
BAATAF
CAFA
SPINAF
EAFT
All trials
Warfarin RRR 64%*, ARR 2.7%
(95% CI: 49–74%)
Aspirin RRR19%, ARR 0.7%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0 1 2 3 4 5 6 7 8 9
Risk Score
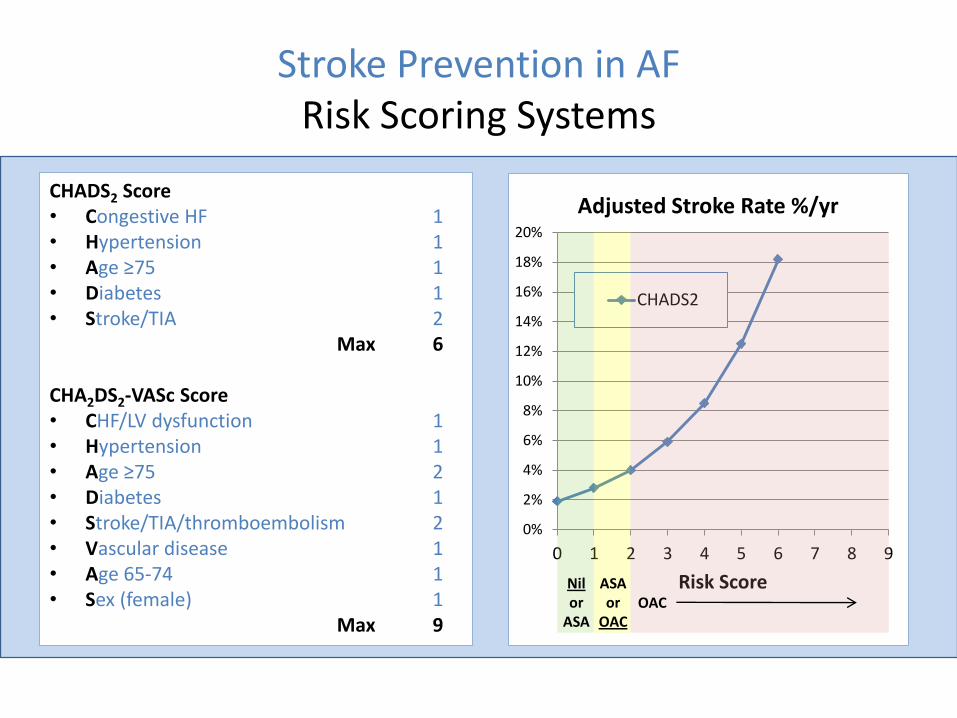
Adjusted Stroke Rate %/yr
CHADS2
Stroke Prevention in AF Risk Scoring Systems
CHADS2 Score • Congestive HF 1 • Hypertension 1 • Age ≥75 1 • Diabetes 1 • Stroke/TIA 2 Max 6
CHA2DS2-VASc Score • CHF/LV dysfunction 1 • Hypertension 1 • Age ≥75 2 • Diabetes 1 • Stroke/TIA/thromboembolism 2 • Vascular disease 1 • Age 65-74 1 • Sex (female) 1 Max 9
ASA or
OAC OAC
Nil or
ASA
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0 1 2 3 4 5 6 7 8 9
Risk Score
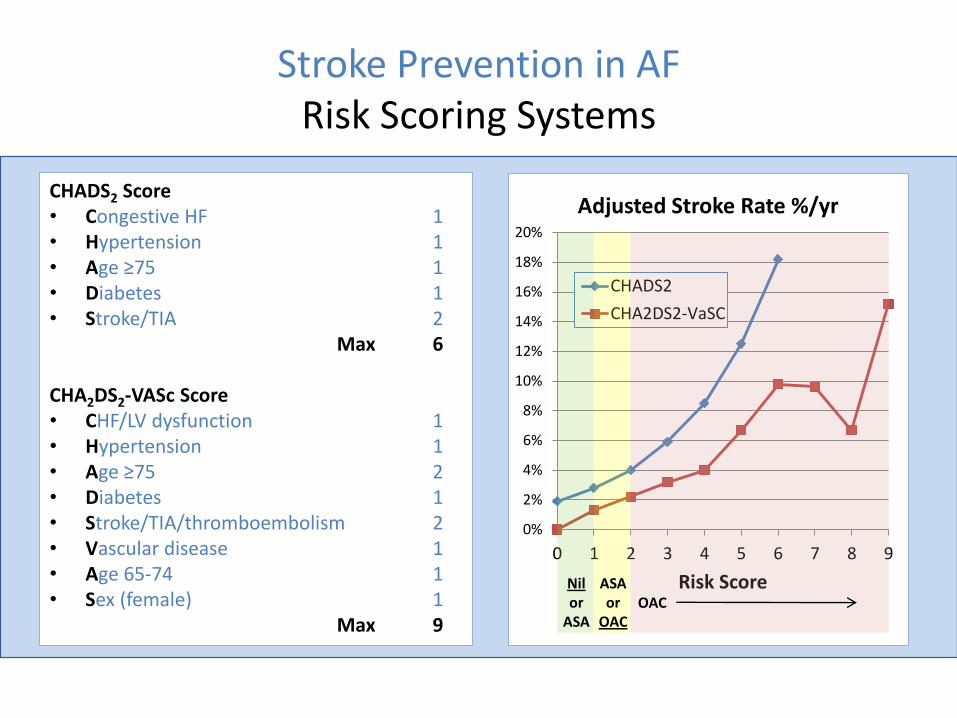
Adjusted Stroke Rate %/yr
CHADS2
CHA2DS2-VaSC
Stroke Prevention in AF Risk Scoring Systems
CHADS2 Score • Congestive HF 1 • Hypertension 1 • Age ≥75 1 • Diabetes 1 • Stroke/TIA 2 Max 6
CHA2DS2-VASc Score • CHF/LV dysfunction 1 • Hypertension 1 • Age ≥75 2 • Diabetes 1 • Stroke/TIA/thromboembolism 2 • Vascular disease 1 • Age 65-74 1 • Sex (female) 1 Max 9 ASA
or OAC
OAC Nil or
ASA
CHADS2 Score • Congestive HF 1 • Hypertension 1 • Age ≥75 1 • Diabetes 1 • Stroke/TIA 2 Max 6
CHA2DS2-VASc Score • CHF/LV dysfunction 1 • Hypertension 1 • Age ≥75 2 • Diabetes 1 • Stroke/TIA/thromboembolism 2 • Vascular disease 1 • Age 65-74 1 • Sex (female) 1 Max 9
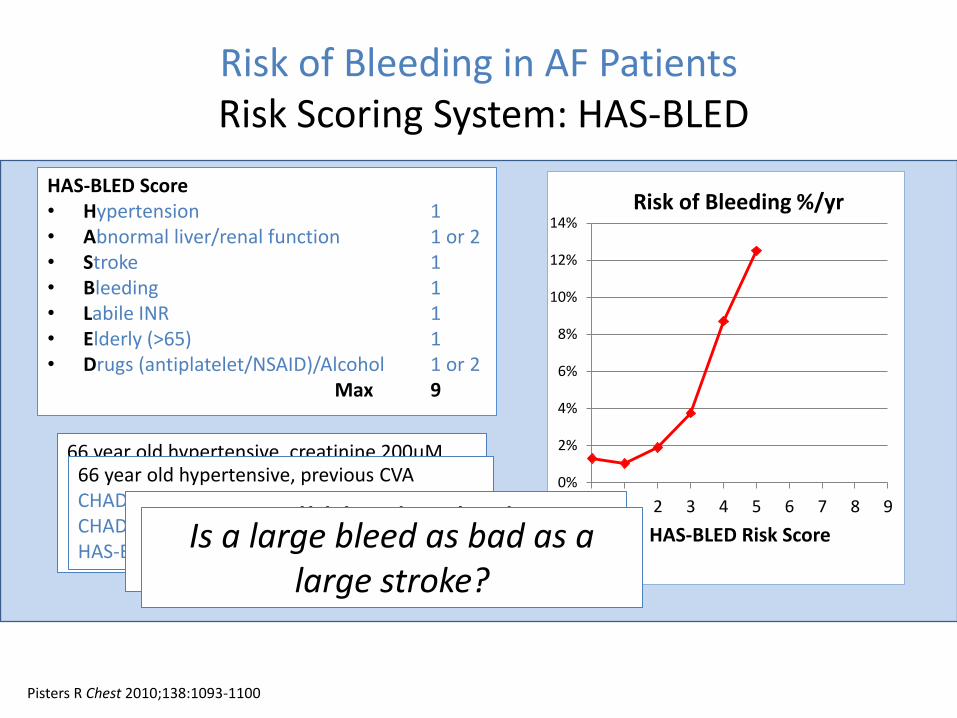
Risk of Bleeding in AF Patients Risk Scoring System: HAS-BLED
HAS-BLED Score • Hypertension 1 • Abnormal liver/renal function 1 or 2 • Stroke 1 • Bleeding 1 • Labile INR 1 • Elderly (>65) 1 • Drugs (antiplatelet/NSAID)/Alcohol 1 or 2 Max 9
0%
2%
4%
6%
8%
10%
12%
14%
0 1 2 3 4 5 6 7 8 9
HAS-BLED Risk Score
Risk of Bleeding %/yr
66 year old hypertensive, creatinine 200μM CHADS2 = 1 risk of stroke = 2.8%/yr CHADS-VaSC = 2 risk of stroke = 2.2%/yr HAS-BLED = 2 risk of bleed = 1.88% / yr HAS-BLED = 3 risk of bleed = 3.74%/yr
66 year old hypertensive, previous CVA CHADS2 = 3 risk of stroke = 5.9%/yr CHADS-VaSC = 4 risk of stroke = 4%/yr HAS-BLED = 3 risk of bleed = 3.74%/yr
Pisters R Chest 2010;138:1093-1100
Is a small bleed as bad as a small stroke?
Is a large bleed as bad as a large stroke?
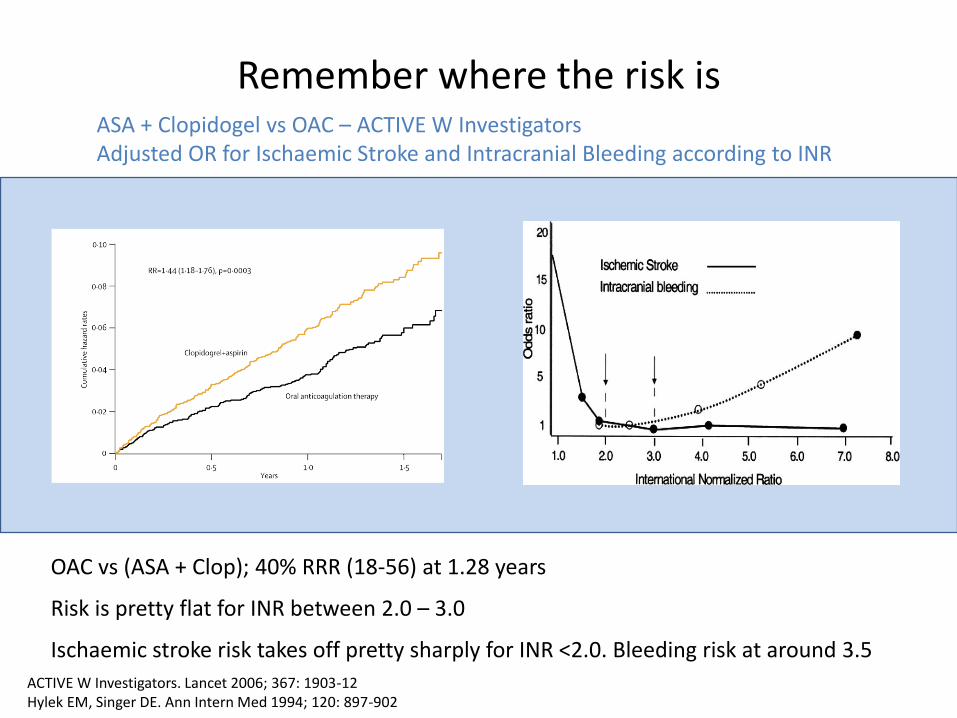
Remember where the risk is
ACTIVE W Investigators. Lancet 2006; 367: 1903-12 Hylek EM, Singer DE. Ann Intern Med 1994; 120: 897-902
OAC vs (ASA + Clop); 40% RRR (18-56) at 1.28 years
Risk is pretty flat for INR between 2.0 – 3.0
Ischaemic stroke risk takes off pretty sharply for INR <2.0. Bleeding risk at around 3.5
ASA + Clopidogel vs OAC – ACTIVE W Investigators Adjusted OR for Ischaemic Stroke and Intracranial Bleeding according to INR
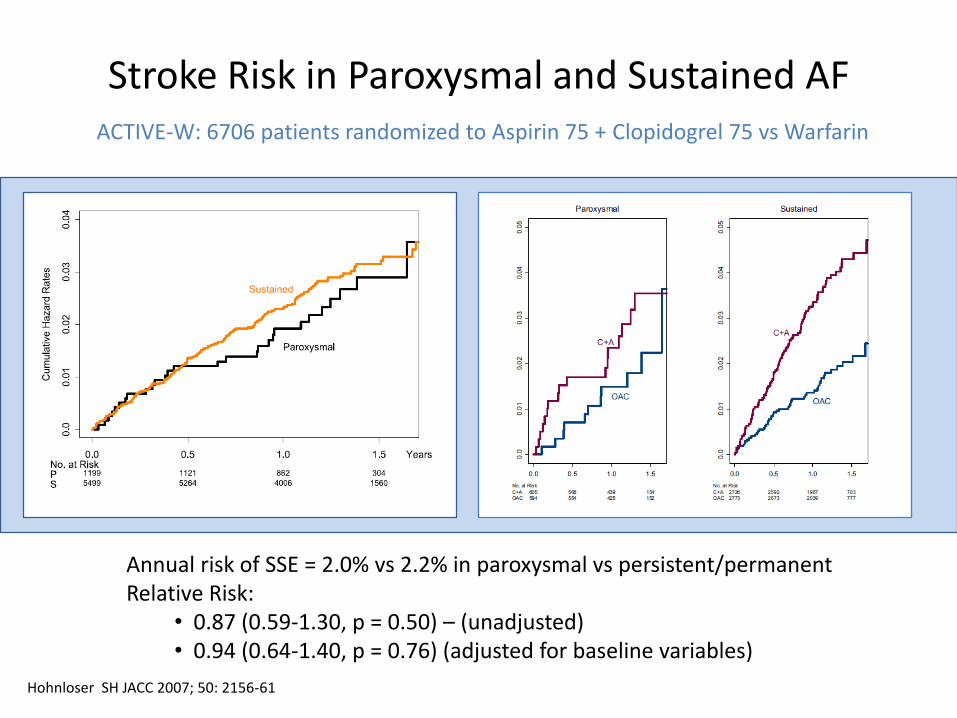
Stroke Risk in Paroxysmal and Sustained AF
Hohnloser SH JACC 2007; 50: 2156-61
Annual risk of SSE = 2.0% vs 2.2% in paroxysmal vs persistent/permanent Relative Risk:
• 0.87 (0.59-1.30, p = 0.50) – (unadjusted) • 0.94 (0.64-1.40, p = 0.76) (adjusted for baseline variables)
ACTIVE-W: 6706 patients randomized to Aspirin 75 + Clopidogrel 75 vs Warfarin
For stroke prevention in AF, which of the following is true?
1. Aspirin is adequate for atrial flutter with normal heart
2. Aspirin only reduces the stroke risk by 40%
3. Paroxysmal and persistent AF should generally be treated the same
4. Aspirin should generally be given if CHADS2 = 1
5. Patients with CHADS-VASC = 2 should definitely be anticoagulated
Q1 (Indications for anticoagulation)
Which of these is false?
Compared to warfarin, stroke prevention in AF using dabigatran, rivaroxaban, apixaban or edoxiban ...
1. ...is at least as effective
2. ...risk of GI bleeding is equal or greater
3. ...risk of major bleeding is equal or lower
4. ...all cause mortality is equal or (very slightly) higher
5. ...risk of intracerebral haemorrhage is lower
Q2: New Oral Anticoagulant Drugs (NOACs)
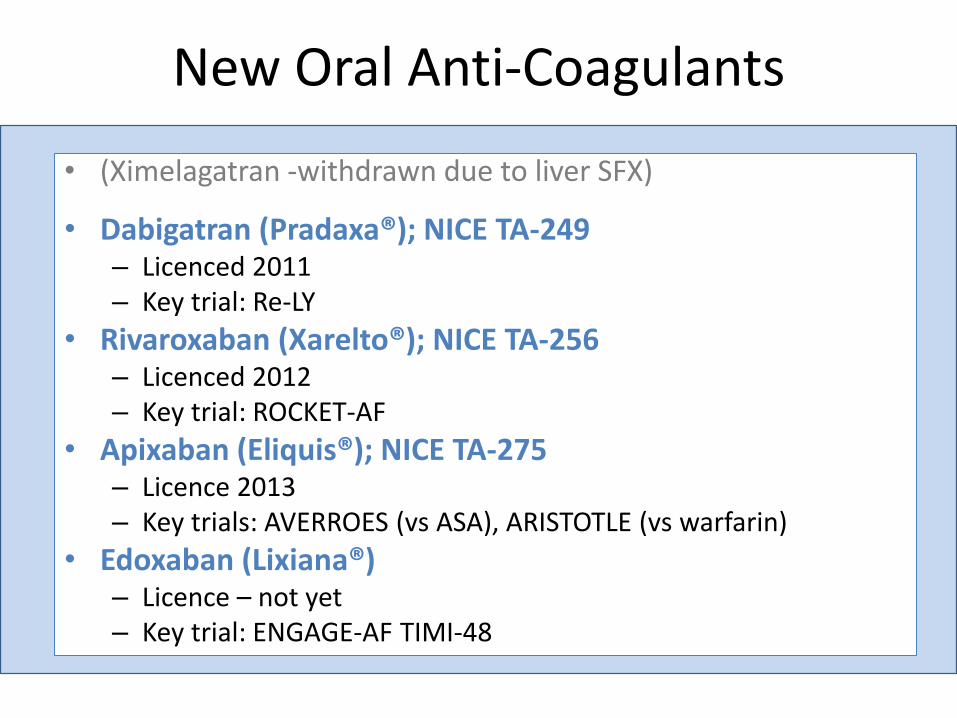
New Oral Anti-Coagulants
• (Ximelagatran -withdrawn due to liver SFX)
• Dabigatran (Pradaxa®); NICE TA-249 – Licenced 2011 – Key trial: Re-LY
• Rivaroxaban (Xarelto®); NICE TA-256 – Licenced 2012 – Key trial: ROCKET-AF
• Apixaban (Eliquis®); NICE TA-275 – Licence 2013 – Key trials: AVERROES (vs ASA), ARISTOTLE (vs warfarin)
• Edoxaban (Lixiana®) – Licence – not yet – Key trial: ENGAGE-AF TIMI-48
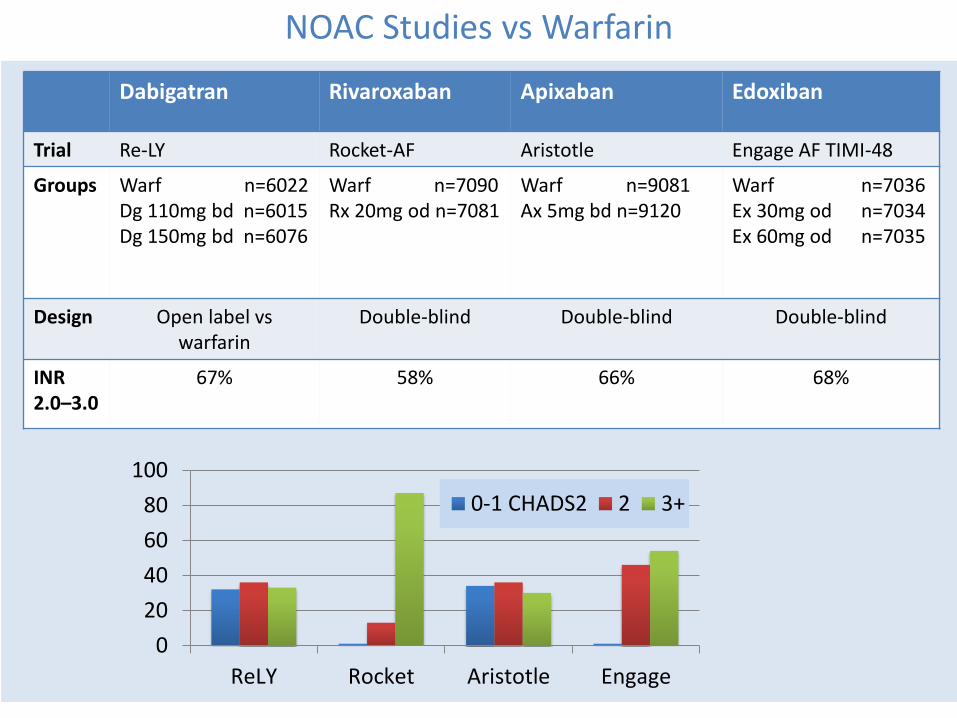
NOAC Studies vs Warfarin
Dabigatran Rivaroxaban Apixaban Edoxiban
Trial Re-LY Rocket-AF Aristotle Engage AF TIMI-48
Groups Warf n=6022 Dg 110mg bd n=6015 Dg 150mg bd n=6076
Warf n=7090 Rx 20mg od n=7081
Warf n=9081 Ax 5mg bd n=9120
Warf n=7036 Ex 30mg od n=7034 Ex 60mg od n=7035
Design Open label vs warfarin
Double-blind Double-blind Double-blind
INR 2.0–3.0
67% 58% 66% 68%
0
20
40
60
80
100
ReLY Rocket Aristotle Engage
0-1 CHADS2 2 3+
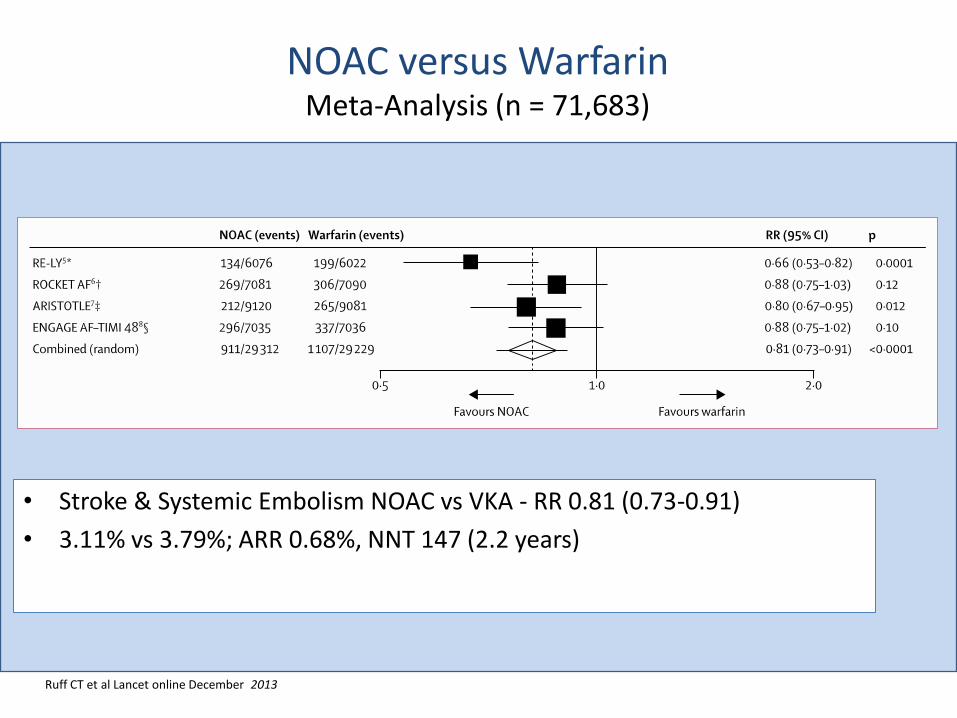
NOAC versus Warfarin Meta-Analysis (n = 71,683)
• Stroke & Systemic Embolism NOAC vs VKA - RR 0.81 (0.73-0.91)
• 3.11% vs 3.79%; ARR 0.68%, NNT 147 (2.2 years)
Ruff CT et al Lancet online December 2013

NOAC Meta-Analysis Secondary End-Points
• Reduced haemorrhagic stroke RR 0.49 (0.38-0.64) – NNT 219
• Ischaemic stroke RR 0.92 (0.83-1.02)
• All cause mortality RR 0.9 (0.85-0.95) – NNT 128
• Increase in GI bleed RR 1.25 (1.01-1.55) – NNH 185
Ruff CT et al Lancet online December 2013
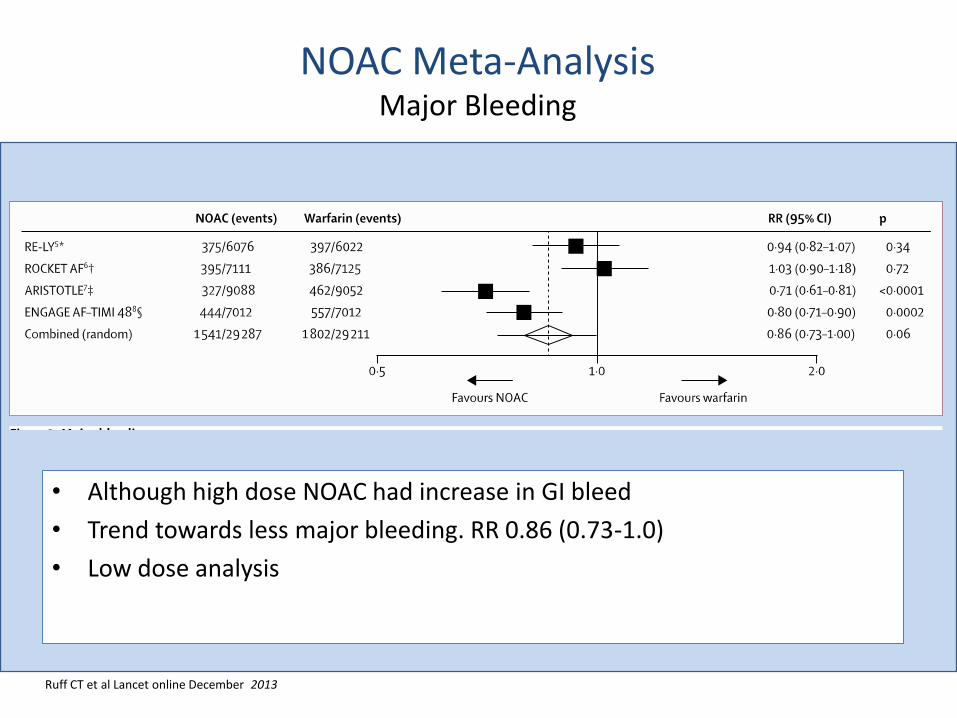
NOAC Meta-Analysis Major Bleeding
• Although high dose NOAC had increase in GI bleed
• Trend towards less major bleeding. RR 0.86 (0.73-1.0)
• Low dose analysis
Ruff CT et al Lancet online December 2013
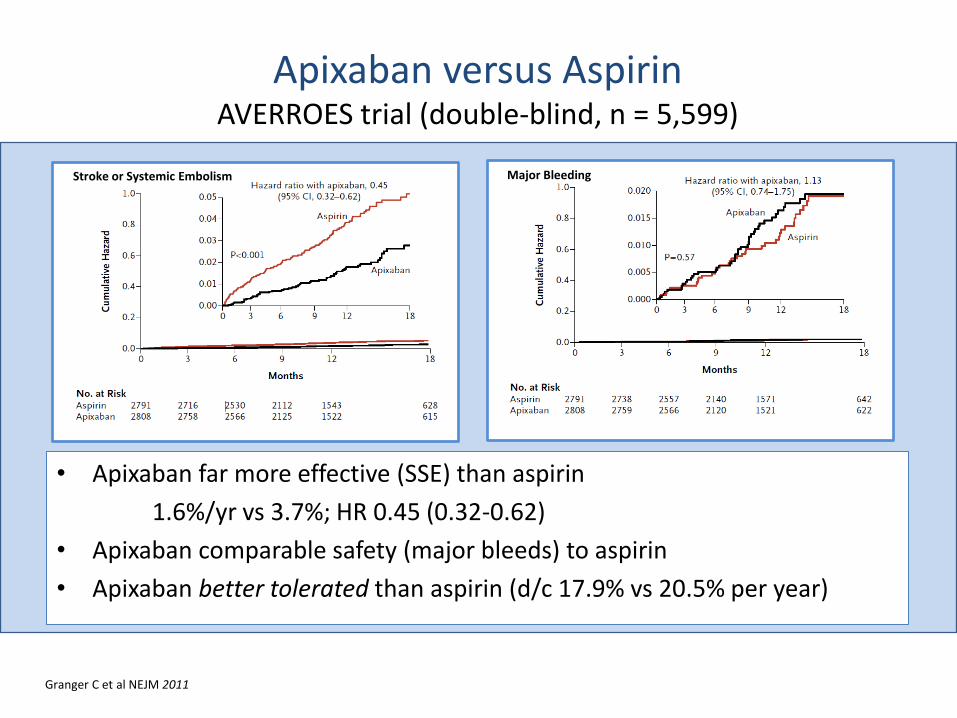
Apixaban versus Aspirin AVERROES trial (double-blind, n = 5,599)
• Apixaban far more effective (SSE) than aspirin
1.6%/yr vs 3.7%; HR 0.45 (0.32-0.62)
• Apixaban comparable safety (major bleeds) to aspirin
• Apixaban better tolerated than aspirin (d/c 17.9% vs 20.5% per year)
Stroke or Systemic Embolism Major Bleeding
Granger C et al NEJM 2011
Which of these is false?
Compared to warfarin, stroke prevention in AF using dabigatran, rivaroxaban, apixaban or edoxiban ...
1. ...is at least as effective
2. ...risk of GI bleeding is equal or greater
3. ...risk of major bleeding is equal or lower
4. ...all cause mortality is equal or (very slightly) higher
5. ...risk of intracerebral haemorrhage is lower
A2: New Oral Anticoagulant Drugs (NOACs)
Q3: Cardioversion
When cardioverting a patient with AF of unknown duration and no stroke risk factors (CHADS2 = 0), which one is true:
1. Anticoagulation should be continued for six months following cardioversion
2. If the heart is structurally normal on transthoracic echo (LA = 3.5cm), anticoagulation is not required
3. If TOE shows no LA thrombus, anticoagulation is unnecessary
4. Dabigatran can be used instead of warfarin
5. Anticoagulation is unnecessary if it is certain that the only arrhythmia is atrial flutter
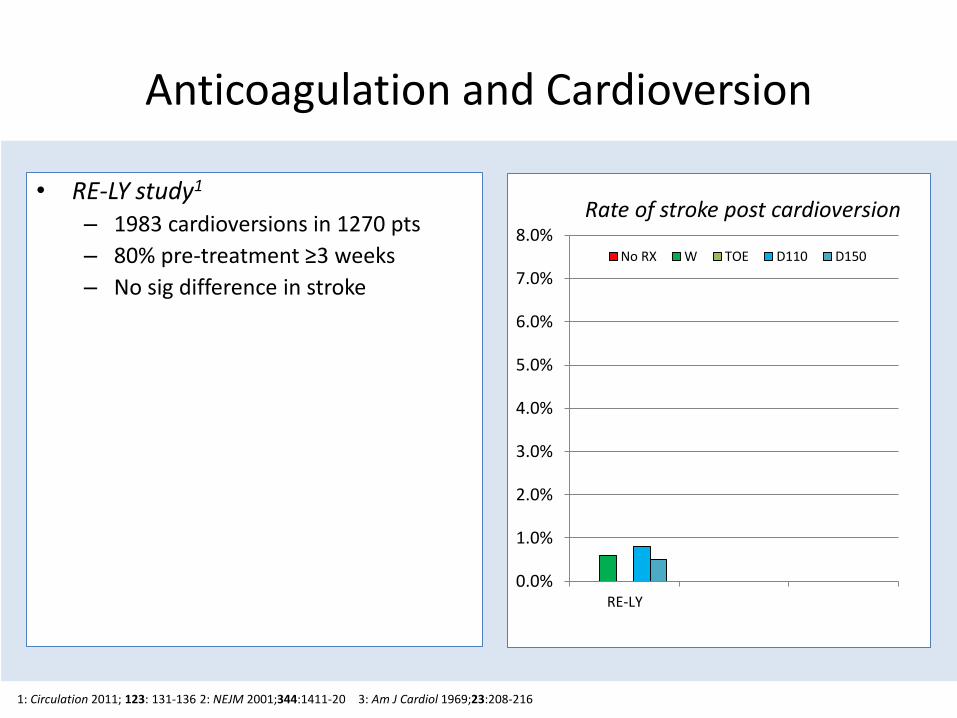
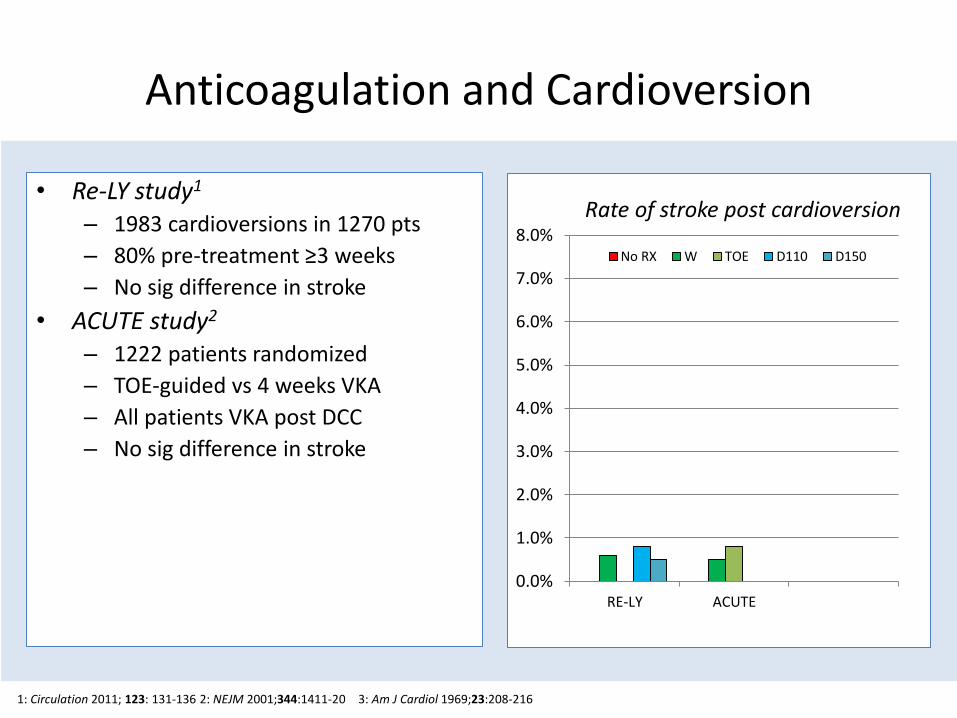
Anticoagulation and Cardioversion
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
RE-LY
Rate of stroke post cardioversion
No RX W TOE D110 D150
• RE-LY study1
– 1983 cardioversions in 1270 pts
– 80% pre-treatment ≥3 weeks
– No sig difference in stroke
• ACUTE study2
– 1222 patients randomized
– TOE-guided vs 4 weeks VKA
– All patients VKA post DCC
– No sig difference in stroke
• Bjerkelund et al3
– N = 537
– 6-fold increase in stroke if no VKA
– Retrospective so probable bias (high risk on VKA)
1: Circulation 2011; 123: 131-136 2: NEJM 2001;344:1411-20 3: Am J Cardiol 1969;23:208-216
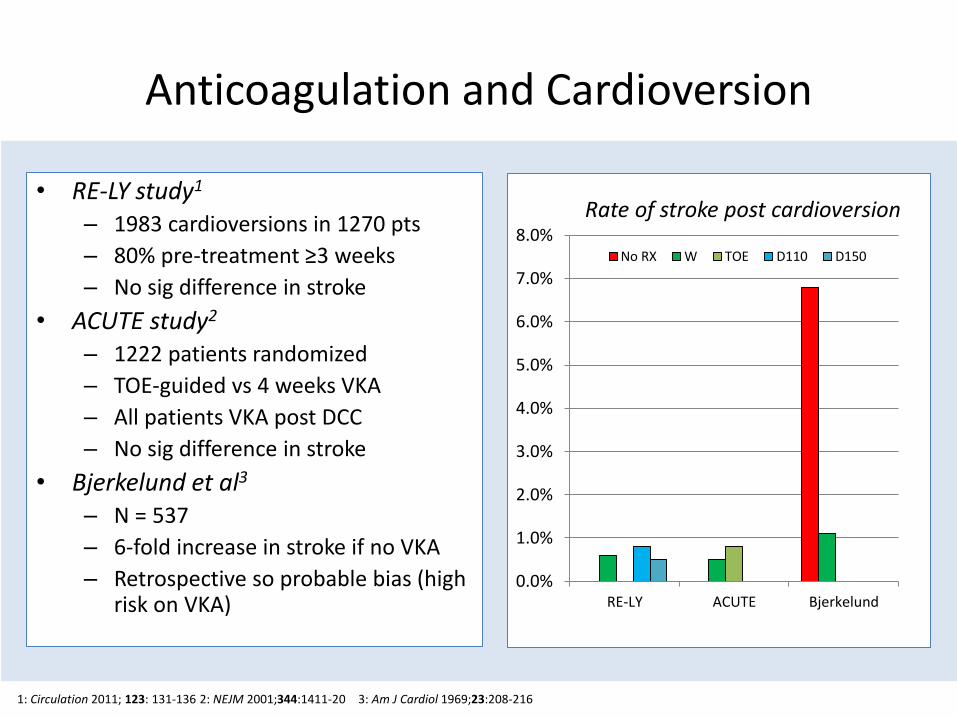
Anticoagulation and Cardioversion
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
RE-LY ACUTE
Rate of stroke post cardioversion
No RX W TOE D110 D150
• Re-LY study1
– 1983 cardioversions in 1270 pts
– 80% pre-treatment ≥3 weeks
– No sig difference in stroke
• ACUTE study2
– 1222 patients randomized
– TOE-guided vs 4 weeks VKA
– All patients VKA post DCC
– No sig difference in stroke
• Bjerkelund et al3
– N = 537
– 6-fold increase in stroke if no VKA
– Retrospective so probable bias (high risk on VKA)
1: Circulation 2011; 123: 131-136 2: NEJM 2001;344:1411-20 3: Am J Cardiol 1969;23:208-216
Anticoagulation and Cardioversion
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
RE-LY ACUTE Bjerkelund
Rate of stroke post cardioversion
No RX W TOE D110 D150
• RE-LY study1
– 1983 cardioversions in 1270 pts
– 80% pre-treatment ≥3 weeks
– No sig difference in stroke
• ACUTE study2
– 1222 patients randomized
– TOE-guided vs 4 weeks VKA
– All patients VKA post DCC
– No sig difference in stroke
• Bjerkelund et al3
– N = 537
– 6-fold increase in stroke if no VKA
– Retrospective so probable bias (high risk on VKA)
1: Circulation 2011; 123: 131-136 2: NEJM 2001;344:1411-20 3: Am J Cardiol 1969;23:208-216
A3: Cardioversion
When cardioverting a patient with AF of unknown duration and no stroke risk factors (CHADS2 = 0), which one is true:
1. Anticoagulation should be continued for six months following cardioversion
2. If the heart is structurally normal on transthoracic echo (LA = 3.5cm), anticoagulation is not required
3. If TOE shows no LA thrombus, anticoagulation is unnecessary
4. Dabigatran can be used instead of warfarin
5. Anticoagulation is unnecessary if it is certain that the only arrhythmia is atrial flutter
Q4: New oral anticoagulants
Which of the following is true regarding new oral anticoagulants?
1. They are all factor Xa inhibitors
2. Peak concentration is reached in 4-6h
3. Plasma half-life is of the order of 10-15h
4. They are ~50% renally excreted and ~50% metabolized
5. In case of bleeding, FFP will normalize the INR
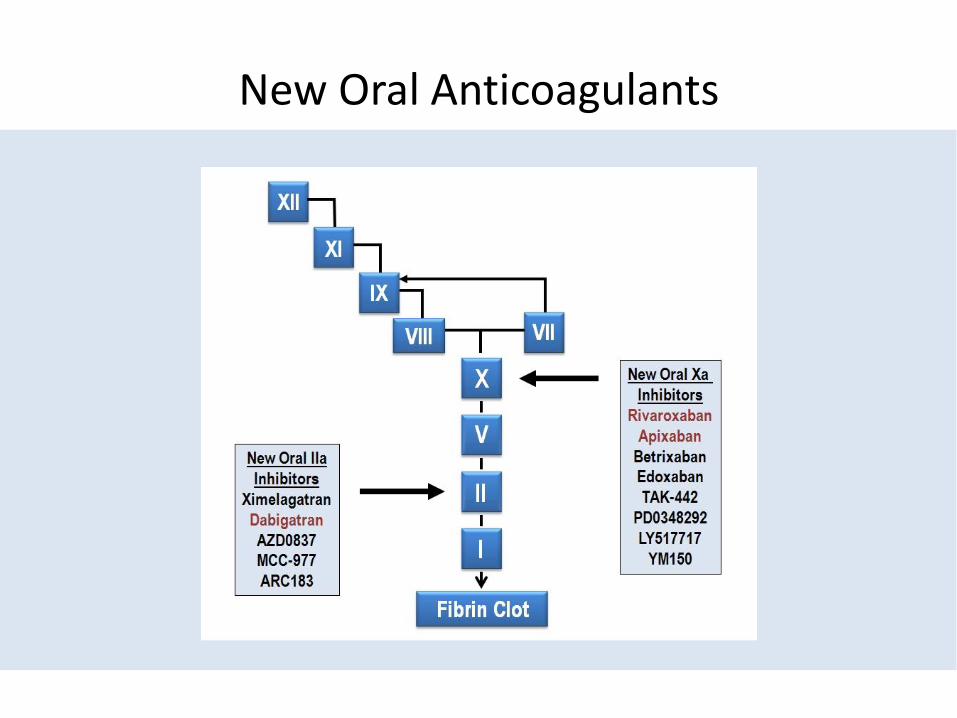
New Oral Anticoagulants
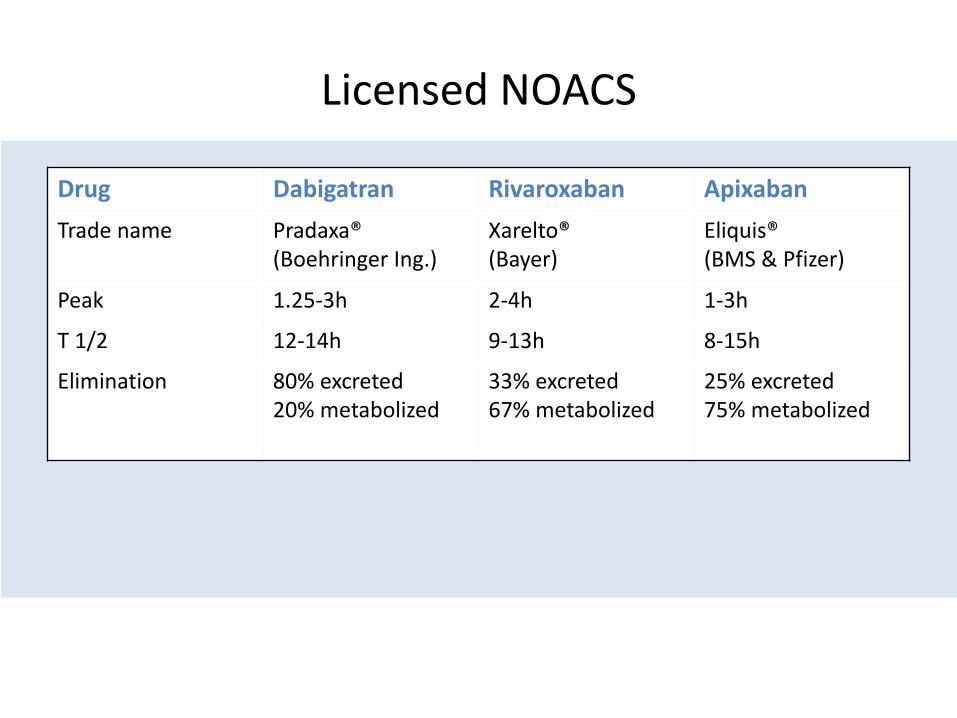
Licensed NOACS
Drug Dabigatran Rivaroxaban Apixaban
Trade name Pradaxa® (Boehringer Ing.)
Xarelto® (Bayer)
Eliquis® (BMS & Pfizer)
Peak 1.25-3h 2-4h 1-3h
T 1/2 12-14h 9-13h 8-15h
Elimination 80% excreted 20% metabolized
33% excreted 67% metabolized
25% excreted 75% metabolized
A4: New oral anticoagulants
Which of the following is true regarding new oral anticoagulants?
1. They are all factor Xa inhibitors
2. Peak concentration is reached in 4-6h
3. Plasma half-life is of the order of 10-15h
4. They are ~50% renally excreted and ~50% metabolized
5. In case of bleeding, FFP will normalize the INR
Q5: Antiarrhythmic Drugs for Paroxysmal AF
• In patients with symptomatic paroxysmal AF, which of the following is false?
1. Flecainide is a first-line antiarrhythmic therapy (in the absence of structural heart disease)
2. Flecainide should usually be given with a rate controlling drug
3. Dronedarone can be given in the presence of coronary disease and good LV function
4. QT interval should be checked 4-6 weeks after initiating or increasing the dose of sotalol
5. Amiodarone can be used for chemical cardioversion in the presence of structural heart disease
A5: Antiarrhythmic Drugs for Paroxysmal AF
• In patients with symptomatic paroxysmal AF, which of the following is false?
1. Flecainide is a first-line antiarrhythmic therapy (in the absence of structural heart disease)
2. Flecainide should usually be given with a rate controlling drug
3. Dronedarone can be given in the presence of coronary disease and good LV function
4. QT interval should be checked 4-6 weeks after initiating or increasing the dose of sotalol
5. Amiodarone can be used for chemical cardioversion in the presence of structural heart disease
www.azcert.org
Q6: Catheter Ablation for AF
A 50 year old woman has symptomatic paroxysmal AF despite flecainide 100mg b.d. She has a structurally normal heart and a history of TIA. Which of the following is true?
1. AF ablation should be considered at this stage
2. Symptomatic success is expected in 50-70%
3. If AF recurs >3 months following pulmonary vein isolation, repeat ablation has a low success rate
4. Anticoagulation can be stopped if the patient is asymptomatic after 1 year
5. Cryoablation has been demonstrated to have fewer complicastions than RF
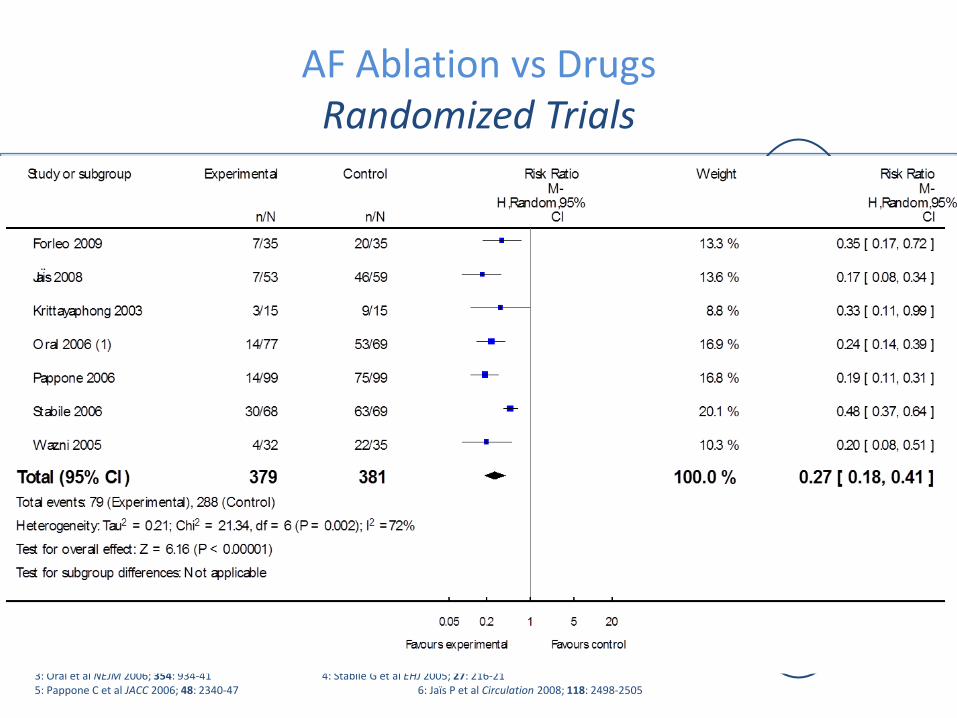
AF Ablation vs Drugs Randomized Trials
Study Pats/
Centres
Age
(mean)
LVEF
(mean)
AF yrs
(mean)
Parox/
Persist
Entry Design Success
@ 1 year
Comp
.
Thai1 30 / 1 52 63 5 (Both) “Chronic,
refract.”
PVI + CTI
vs Amio
80% v 20%
(sympt.)
1 CVA
RAAFT
pilot2
70 / 3 54 54 5 67 +3 No prior
treatment
PVI x1
vs AAD
87% vs 37% 1PVst
Oral3 146 / 2 56 56 5 0 +146 Fail 2+
AADs
CPVA vs nil
(both 3m amio)
ITT 74% vs 58%
(77% x-over)
(PP 94/130 vs 3/16)
Nil
CACAF4 137 / 4 62 58 6 92 +45 Fail 2+
AADs
CPVA + AAD
vs AAD
56% vs 8% 1CVA,
1φ,
1tamp
APAF5 198/1 56 61 6 198 +0 Fail 2+
AADs
CPVA + lines
vs new AAD
86% vs 22%
(5% vs 42% x-over)
1 TIA,
1tamp
A46 112/4 51 64 6 112 +0 Fail 1+
AAD
CPVA + lines
vs new AAD
89% vs 23%
(9% vs 63% x-over)
2 tamp,
2 groin
1 PVst
1: Krittayaphong R et al J Med Assoc Thai 2003; 86: S8-16 2: Wazni OM et al JAMA 2005; 293: 2634-40 3: Oral et al NEJM 2006; 354: 934-41 4: Stabile G et al EHJ 2005; 27: 216-21 5: Pappone C et al JACC 2006; 48: 2340-47 6: Jaïs P et al Circulation 2008; 118: 2498-2505
1 – Year Re-do ORAL 26% CCAF 0% APAF 6% A4 43%
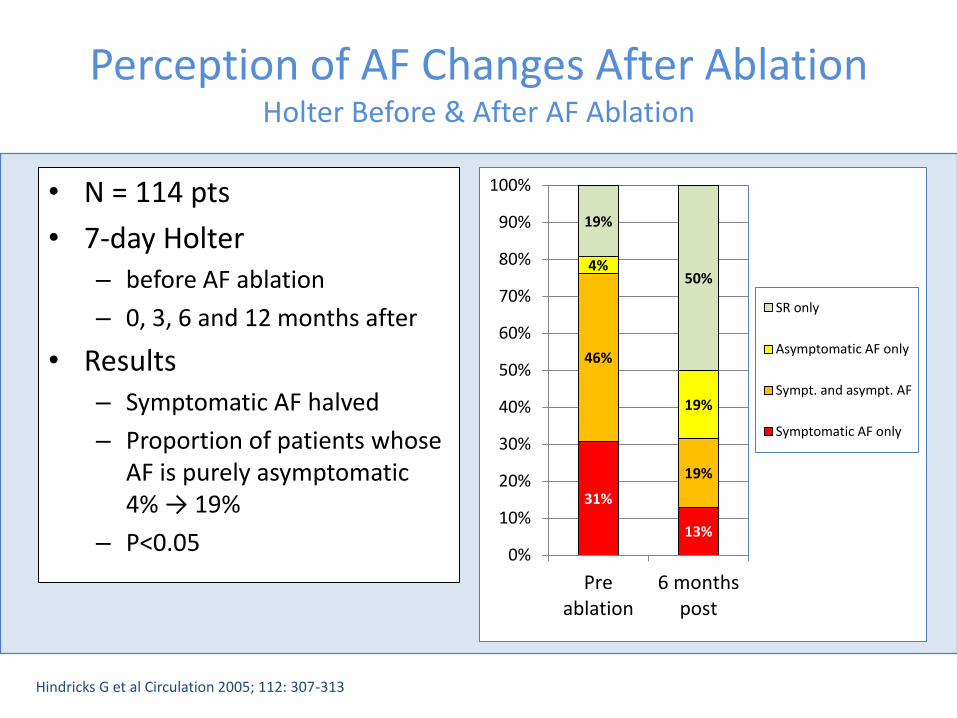
Perception of AF Changes After Ablation Holter Before & After AF Ablation
• N = 114 pts
• 7-day Holter – before AF ablation
– 0, 3, 6 and 12 months after
• Results – Symptomatic AF halved
– Proportion of patients whose AF is purely asymptomatic 4% → 19%
– P<0.05
Hindricks G et al Circulation 2005; 112: 307-313
31%
13%
46%
19%
4%
19%
19%
50%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Preablation
6 monthspost
SR only
Asymptomatic AF only
Sympt. and asympt. AF
Symptomatic AF only

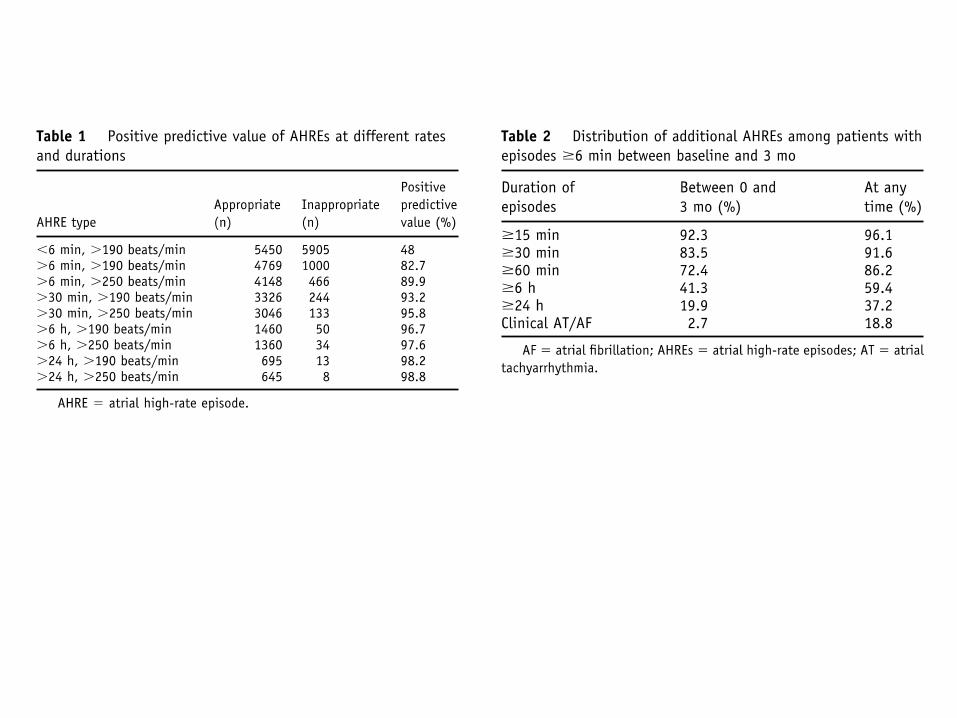
ASSERT • N = 2580 age ≥65 with hypertension & PPM or ICD
• CHADS2 of 2.2
• ATF episodes >6 min
• 10% of patients at 3 months
• 36% at 2.8 yr FU
• Similar result when adjusted for baseline risks
• Annual risk of SSE in CHADS ≥2 patients 0.7% vs 2.1%
Endpoint No AT AT RR (95%CI) p
Isch stroke/TE 40 (0.7%/yr) 11 (1.7%/yr) 2.5 (1.3-4.9) 0.007
Vasc. Death 153 (2.6%/yr) 19 (2.9%/yr) 1.1 (0.7-1.8) 0.67
Stroke/MI/Vasc Death 206 (3.5%/yr) 29 (4.5%/yr) 1.3 (0.9-1.8) 0.27
Clinical AF/FL 71 (1.2/yr) 41(6.3%/yr) 5.6 (3.8-8.2) 0.001
1. Healey J presented at AHA 2010
Catheter ablation of Paroxysmal AF
• Ablation for paroxysmal AF in a patient with minimal/no structural heart disease should eliminate symptoms at 1 year in >70%
• PV reconnection is common, repeat isolation usually effective when recurrence after first ablation
• All patients should be anticoagulated post procedure
• Longterm anticoagulation depends on risk factors not apparent success
A6: Catheter Ablation for AF
A 50 year old woman has symptomatic paroxysmal AF despite flecainide 100mg b.d. She has a structurally normal heart and a history of TIA. Which of the following is true?
1. AF ablation should be considered at this stage
2. Symptomatic success is expected in 50-70%
3. If AF recurs >3 months following pulmonary vein isolation, repeat ablation has a low success rate
4. Anticoagulation can be stopped if the patient is asymptomatic after 1 year
5. Cryoablation has been demonstrated to have fewer complicastions than RF
Q7: Catheter Ablation for Persistent AF
Which of the following is true regarding catheter ablation for persistent AF?
1. The risk of symptomatic pulmonary vein stenosis is 2-4%
2. The risk of tamponade is 2-4%
3. The risk of atrio-oesophageal fistula (the most dangerous complication) is 0.5-1%
4. To achieve medium term (1-3 years) success, repeat ablation is required in 5-15% of patients
5. Best technique is PVI plus additional lines
Catheter Ablation of AF Complications
• Tamponade – Worldwide survey 1.2%1, highest report 6% – Large single centre series 10/348 (2.9%)2; 15/632 (2.4%)3
• PV Stenosis – Worldwide survey 0.32% acute, 1.3% persistent – Severe stenosis 21/608 (3.4%)4, symptomatic only if severe and multiple – Probably less frequent with WACA than SOA
• Phrenic nerve palsy – Occurs with all modalities, incidence 0%-0.25%5
• Atrio-oesophageal fistula – Most dangerous complication (usu. fatal), incidence <0.25%5
• Stroke, MI – Should be <1%5
• Death – Rare, (<0.25%) 5
1: Cappato R et al Circulation 2005; 111:1100-05 2: Hsu LF et al PACE 2005;28:S106-9 3: Bunch J et al JCE 2005;16:1172-9 4: Saad et al Circulation 2003;108:3102–3107 5: Calkins Het al Heart Rhythm 2007; 4:816-861
Catheter Ablation of Persistent AF
• 395 patients with persistent AF – mean duration 16 months
• De novo AF ablation – Stepwise approach
• Follow-up 27 ± 7 months
• Single procedure success: 27%
• Multiple (2.3 ± 0.6) procedure success 79% – 23% on BB, 15% other AAD
Rostock T Heart Rhythm 2011; 8 1391-7
A7: Catheter Ablation for Persistent AF
Which of the following is true regarding catheter ablation for persistent AF?
1. The risk of symptomatic pulmonary vein stenosis is 2-4%
2. The risk of tamponade is 2-4%
3. The risk of atrio-oesophageal fistula (the most dangerous complication) is 0.5-1%
4. To achieve medium term (1-3 years) success, repeat ablation is required in 5-15% of patients
5. Best technique is PVI plus additional lines
Q8: Rate control in AF
Regarding rate control in permanent AF, which of the following is false?
1. AV nodal ablation is usually necessary to maximize benefit from CRT necessary in patients with permanent AF
2. A resting ventricular rate of 100bpm is acceptable in asymptomatic patients with permanent AF
3. Digoxin is not first-line therapy for rate control in active elderly patients
4. Amiodarone can be used for rate control
5. When ablating the AV-node, CRT is preferable for patients with a reduced ejection fraction
A8: Rate control in AF
Regarding rate control in permanent AF, which of the following is false?
1. AV nodal ablation is usually necessary to maximize benefit from CRT necessary in patients with permanent AF
2. A resting ventricular rate of 100bpm is acceptable in asymptomatic patients with permanent AF
3. Digoxin is not first-line therapy for rate control in active elderly patients
4. Amiodarone can be used for rate control
5. When ablating the AV-node, CRT is preferable for patients with a reduced ejection fraction
Any Questions
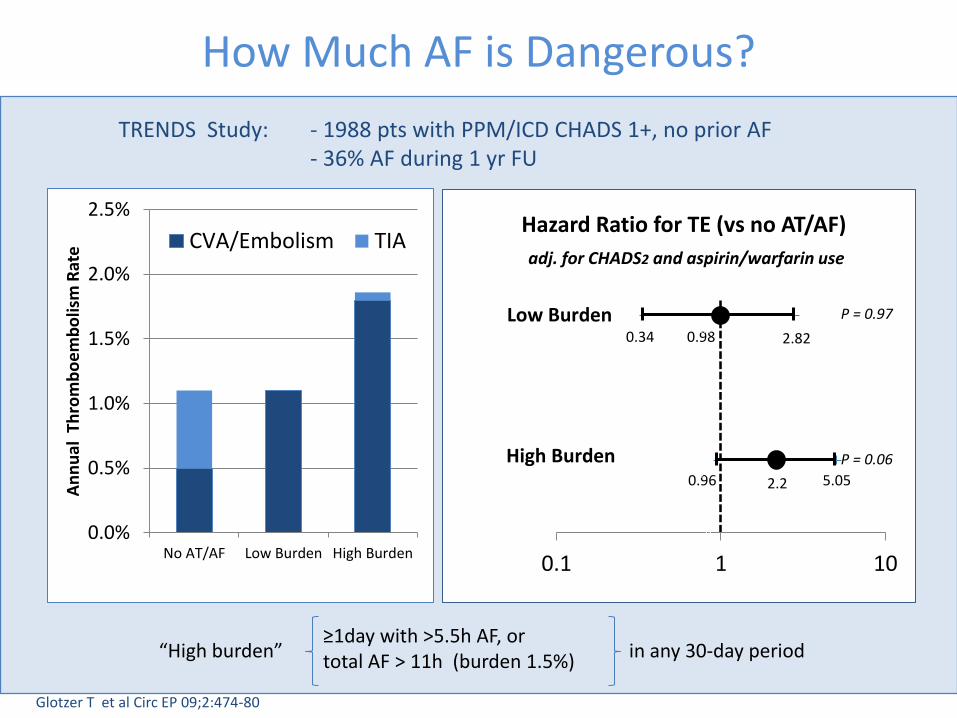
How Much AF is Dangerous?
0.34 0.98 2.82
0.96 2.2 5.05
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
0.1 1 10
Hazard Ratio for TE (vs no AT/AF)
Low Burden
High Burden
adj. for CHADS2 and aspirin/warfarin use
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
No AT/AF Low Burden High Burden
An
nu
al T
hro
mb
oe
mb
olis
m R
ate
CVA/Embolism TIA
Glotzer T et al Circ EP 09;2:474-80
P = 0.97
P = 0.06
≥1day with >5.5h AF, or total AF > 11h (burden 1.5%)
“High burden” in any 30-day period
TRENDS Study: - 1988 pts with PPM/ICD CHADS 1+, no prior AF - 36% AF during 1 yr FU