AES 2014 Practice Management Course December 9, 2014 Gregory L. Barkley, M.D. Comprehensive Epilepsy...
60
AES 2014 Practice Management Course December 9, 2014 Gregory L. Barkley, M.D. Comprehensive Epilepsy Program Henry Ford Hospital Detroit, MI Associate Professor of Neurology Wayne State University
-
Upload
dania-keeler -
Category
Documents
-
view
214 -
download
1
Transcript of AES 2014 Practice Management Course December 9, 2014 Gregory L. Barkley, M.D. Comprehensive Epilepsy...

AES 2014 Practice Management Course
December 9, 2014
Gregory L. Barkley, M.D.Comprehensive Epilepsy Program
Henry Ford HospitalDetroit, MI
Associate Professor of NeurologyWayne State University

Outline
2015 Medicare Conversion Factor and SGR 2015 CPT Code Changes

Noteworthy in 20152% Sequestration cuts remain in place
CMS is required by law to cut the Conversion Factor on April 1, 2015 to maintain budget neutrality.
The Conversion factor until April 1, 2015 will be $35.8013, down from $35.8228
Conversion Factor cut in 2015 is scheduled to be about 21% to $28.2239 unless Congress changes the law as it has done annually since 2002. (Last year, we were facing a 23.7% cut to $27.006 showing that the SGR deficit has narrowed in the past year.)
Unless the fix happens in the next three weeks, the legislation will have to come from a Republican House and a Republican Senate and be acceptable to President Obama in 2015.
– Republican strategy on budget issues is being internally debated
– One group wants to find ways to pass laws & avoid shutdown
– Another group is more confrontational with the President
– One strategy that may be used is to tie funding that one party wants to a bill that the other party wants to hold each side hostage
ICD-10 to begin on October 1, 2015 – REALLY!
CMS drops 10-day global in 2017, 90-global in 2018

The Medicare Fee Schedule
In 2009, the Neurology Member Census showed 37% of Neurology patients are 65 and older and are thus on Medicare
Medicare Fee Schedule is an open process Private payers use a closed process but base payments on Medicare
Codes are defined by the AMA CPT Editorial Panel Codes are given a relative work value (RVU) by the AMA RBRVS
Update Committee (RUC) as a recommendation to CMS CMS reviews RUC values and assigns RVU (~90% unchanged from
RUC) CMS publishes annual Conversion Factor (CF) Medicare payment formula is RVU x CF = Payment Annual Medicare payment determined by Sustainable Growth Rate
Sustainable Growth Rate (SGR) Law passed in 1997, requires Medicare payments to follow a formula linked to the
cost of medical care, MEI
Medicare Economic Index (MEI) is a conservative government estimate of the rate of inflation of medical care
Annual overrides have prevented decreased payments to physicians since 2002, but the law has not been changed so the deficit keeps building
The 2015 CF will be $28.2239 to comply with SGR, a cut of 21% unless Congress overrides the cut.
CBO estimates the total cost of repeal of the SGR has dropped to $144 billion over 10 years, down from $153.2 B/10 years last year, & down from the peak estimate in 2012 of $376.6 B/10 years

Possible Republican Strategy on SGR Fix Heritage Foundation is an influential conservative “Think Tank”
Issue Brief #4303 on 11/20/2014 re: SGR Fix made the following points
http://thf_media.s3.amazonaws.com/2014/pdf/IB4303.pdf
Should be permanent and based upon bipartisan agreement
Principle: “Permanent “Doc Fix” must be financed by permanent Medicare savings”
Must take into account demographics of baby boomers
Possible solutions
– Combine Part A & Part B with single deductible, streamline cost sharing
– Reform Medigap
– Give seniors catastrophic coverage
– Gradually raise age of Medicare eligibility
– Gradually decrease subsidy of wealthy
– Pave way for defined contribution plan (aka Paul Ryan plan)
Making Your Voice Heard is Easy
Why has the cost of the SGR fix gone down? Has the cost curve been bent?
SGR is linked to the Medicare Economic Index.
Health care inflation has decreased primarily due to the recession, or is there something else going on? This is a major question and source of political debate
There is no doubt that recessions temporarily decrease health care spending in every country
In US, major factors have also been bending the health care curve:
– The marked increase in insurance policy deductions and in copayments
– High deductible plans are changing the way people access health care
– Loss of patents on high cost drugs has dropped the cost of medications
• Now generic drug costs are rising
– Hospitals have had decreased reimbursement in ACA and new controls such as increased use of Observation Days, 30-Day Readmission Penalties, POS non-payment policies
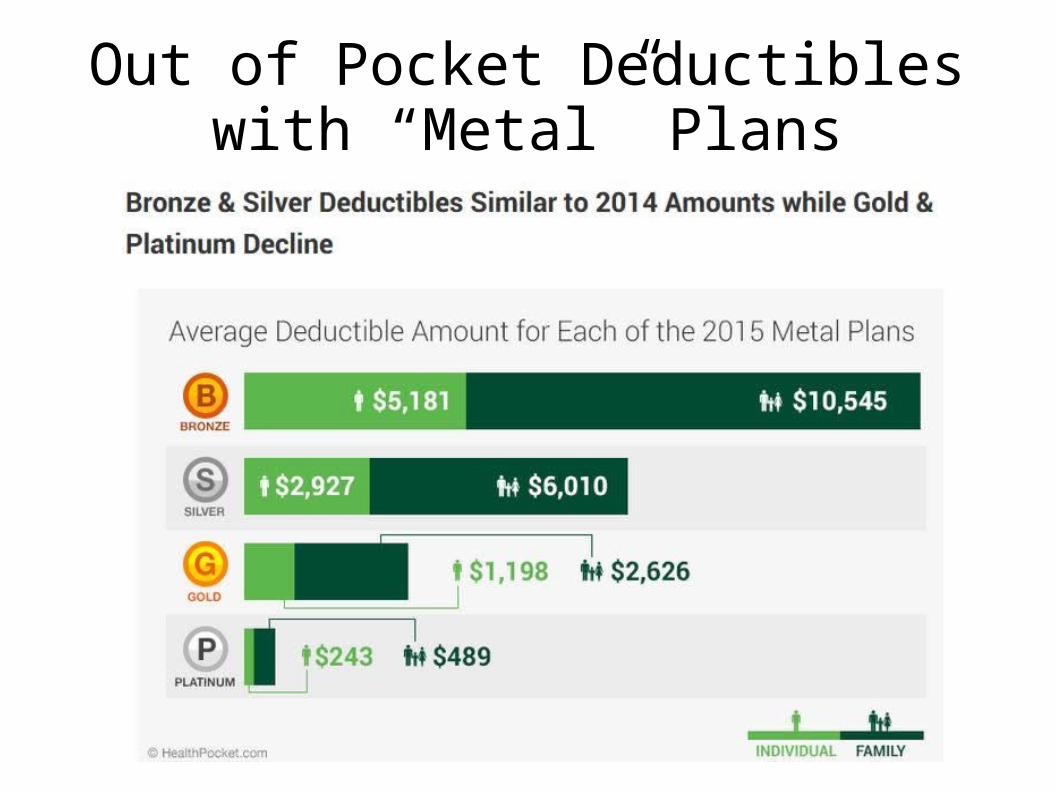
Out of Pocket Deductibles with “Metal” Plans
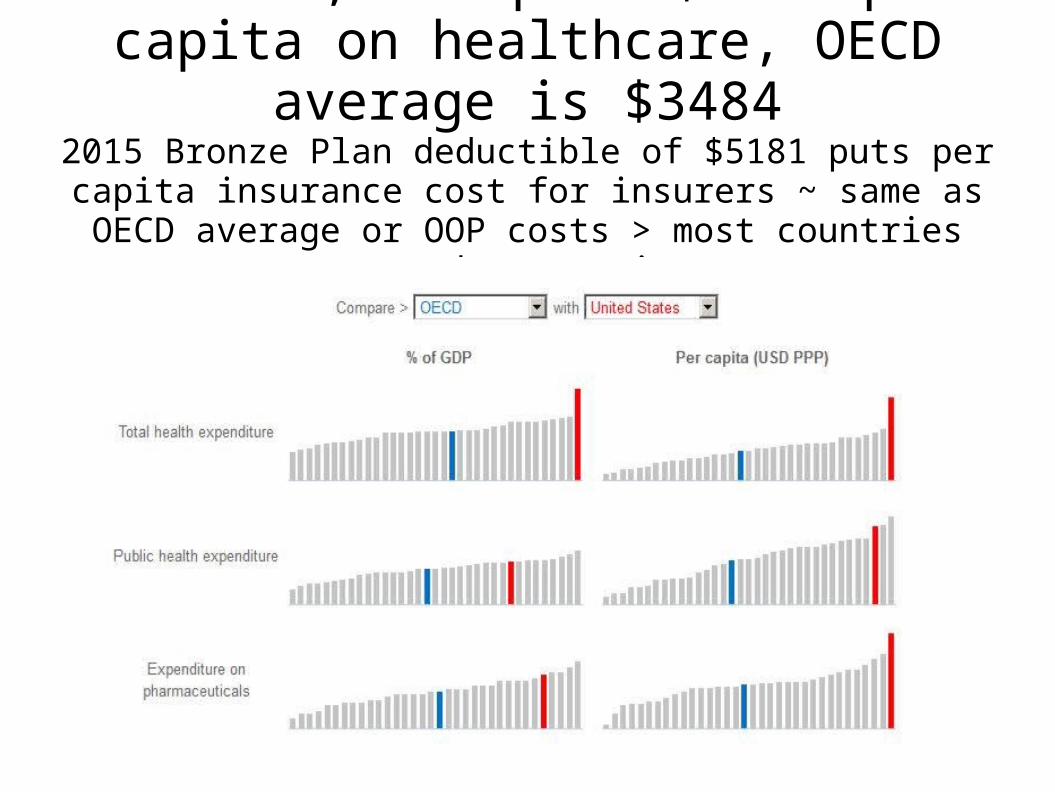
In 2012, US spent $8745 per capita on healthcare, OECD average is $3484
2015 Bronze Plan deductible of $5181 puts per capita insurance cost for insurers ~ same as OECD average or OOP costs > most
countries spend per capita
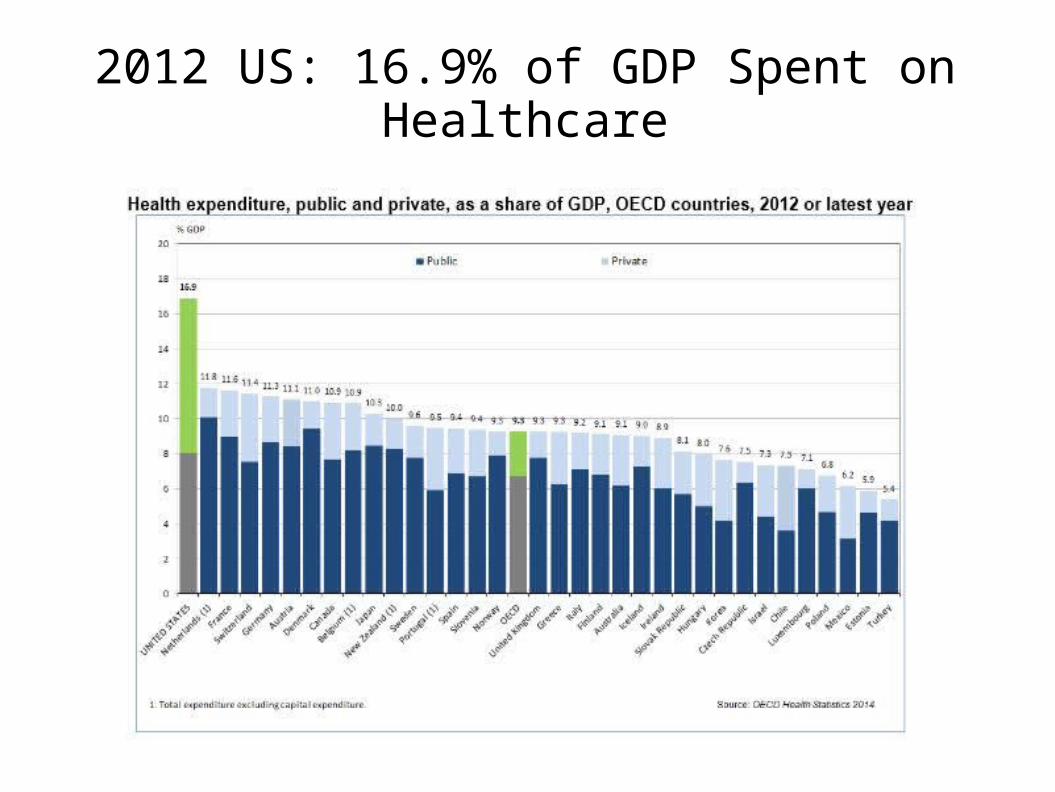
2012 US: 16.9% of GDP Spent on Healthcare

2012 Drug costs are $885 in US vs $414 OECD average

2004-2012 OECD Health Expenditure Annual Changes
US rise moderated by drop in drug costs & hospital care, started before recession
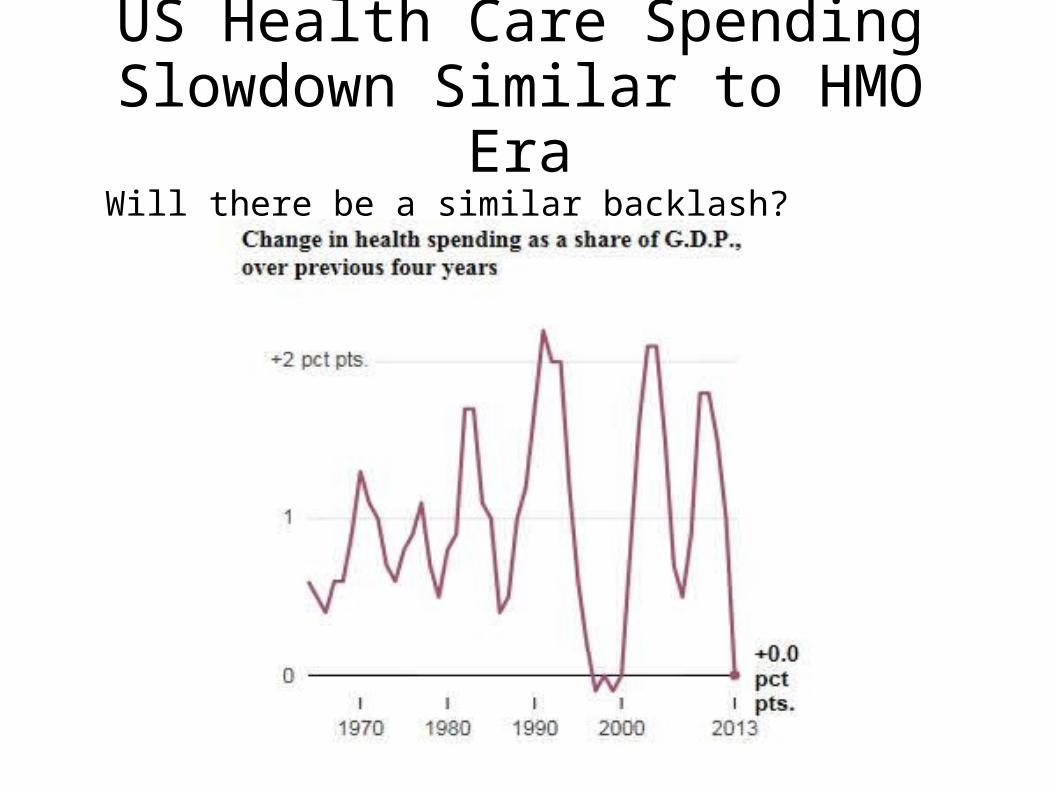
US Health Care Spending Slowdown Similar to HMO Era
Will there be a similar backlash? D Lionhardt, NYTimes 12-6-2014
All Physicians are not Paid the Same, I
GPCI makes adjustments in payment based upon location of service
Since 2011: some providers are paid more by specialty
Primary Care Physician Medicaid parity payments end 12/31/14 unless extended (S. 2694)
ACA's Primary Care Incentive Payments (PCIP) in place, 2011-2015
Primary care providers are paid a 10% bonus for non-hospital E&M visits.
The payments are paid quarterly to primary care physicians.
Does not apply to neurologists despite the attempts of the AAN to include neurologists.
APRN/PA payments are 85% of the rate that physicians are paid, but for a primary care APRN/PA, with the 10% bonus, their payment for the same level of service is 93% of what a specialist would receive for the same service, say for CPT code 99213.
All Physicians are not Paid the Same, II
Your type of practice and the site of service determines how you will be paid
In private offices, payments are global, combining pro fee and tech fee
In medical centers, payments to physicians are for professional fees only
Technical payments by HOPPS as APCs to medical center Same applies to patients seen in emergency rooms and observation
patients who are not admitted and are subject to outpatient copays For inpatients, payments to physicians are for professional fees only
Technical payments are bundled IPPS as DRGs paid to hospital
CPT Medicare Payment Relative to Site of Services
Inpatient care:
– Professional fee paid to physician using -26 modifier
– Technical fee paid by DRG to hospital using IPPS (DRG values based upon hospital cost reporting) Top-down methodology based upon hospital-supplied cost data
Outpatient care: Provider-based billing
– Professional fee paid to physician using -26 modifier
– Technical fee paid to medical center using HOPPS (APC charges based upon hospital cost reporting averaged for all procedures in the APC) Top-down methodology
Outpatient care: private office
– Professional fee bundled with technical payment, so-called global billing using CMS MFS largely following RUC recommended values. Bottom-up methodology by RUC PE

How to Improve Your Net Revenue, I
Control costs
Control costs
Control costs
Rent, supplies, staff each need to be scrutinized
How to Improve Your Net Revenue, II
Check to make sure that your staff is not stealing from you
If it involves money, someone will try and take it from you Set up checks & balances for for all processes involving money
Always have two people handling money Nearly 83% of 688 practice managers were affiliated at some point
with medical offices where employee theft occurred (MGMA Survey 11/5/2010)
Nearly 45% of practice managers reported cash stolen before or after it was recorded on the books.
Profile of the embezzler: first one in, last to one to leave, never takes a vacation, stops by on weekends, very friendly and helpful; be suspicious of those who have a gambling habit

2015 Office-base Fee ScheduleFor those billing Global
N.B. For the following slides, the values are estimates. They do not take into account modifiers such as the GPCI (Geographic Practice Cost Indices).
I have done my best to capture this data accurately, but every year, I unfortunately find a few typos in the previous year's slides as I manually update them. Please refer to your state Medicare carrier for the rates for your practice.
2015 MFS for Neurology Services**Assuming conversion factor of $35.80
• 95812, EEG 41-60 minutes– Total RVU: 11.79; -3%, $422.31, -3%
– PE: 10.63 RVU; -3%, $364.06, -3%
– Professional: 1.63 RVU, 1%; $58.35, 0%
– Physician Work (wRVU): 1.08, No change
• 95813, EEG > 1 hour– Total RVU: 14.11, 0%, $505.46, 0%
– PE: 12.25 RVU, -1%; $411.67, -2.8%
– Professional: 2.62 RVU, 1%; $93.79, 1%
– Physician Work (wRVU): 1.73, No change
2015 MFS for Neurology Services**Assuming Conversion Factor of $35.80
• 95816, Awake EEG– Total RVU: 10.11, 2%, $362.27, 2%
– PE: 8.96 RVU, 3%; $303.92, 3%
– Professional: 1.63 RVU, 0%; $58.71, 1%
– Physician Work (wRVU): 1.08, No change
• 95819, Awake and Asleep EEG – Total RVU: 11.53, 2%, $413.11, 2%
– PE: 10.37 RVU, 1%; $354.76, 2%
– Professional: 1.63 RVU, 1%; $58.35, 1%
– Physician Work (wRVU): 1.08, No change
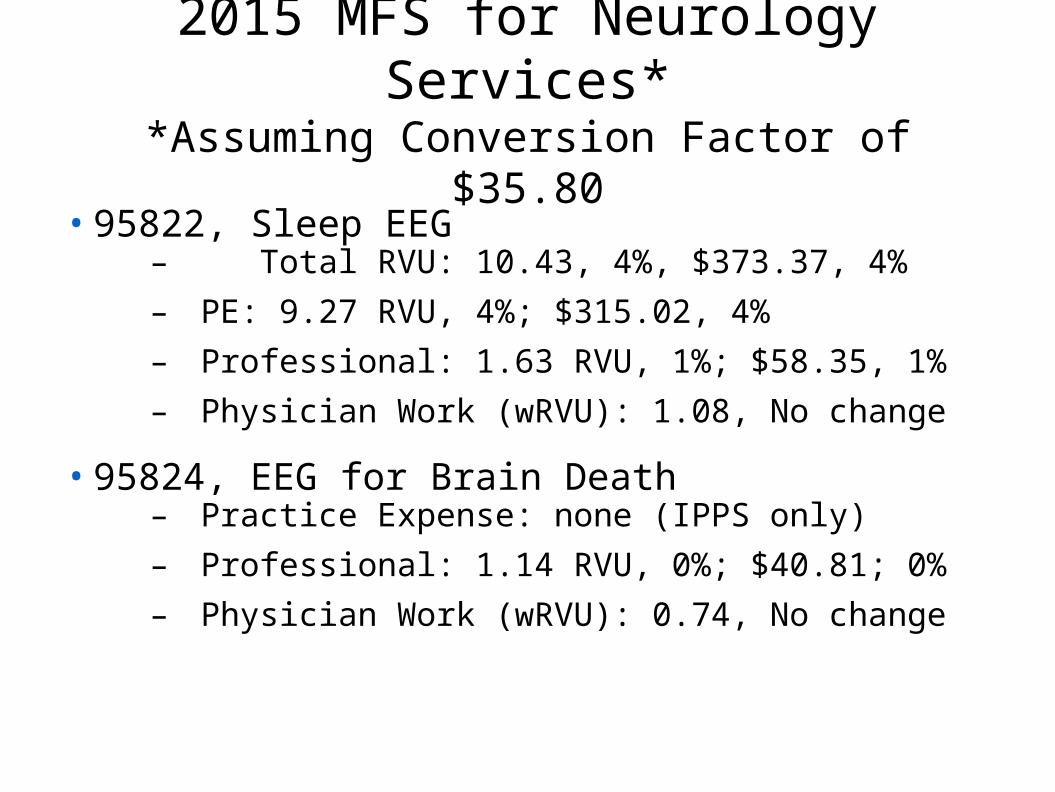
2015 MFS for Neurology Services**Assuming Conversion Factor of $35.80
• 95822, Sleep EEG– Total RVU: 10.43, 4%, $373.37, 4%
– PE: 9.27 RVU, 4%; $315.02, 4%
– Professional: 1.63 RVU, 1%; $58.35, 1%
– Physician Work (wRVU): 1.08, No change
• 95824, EEG for Brain Death– Practice Expense: none (IPPS only)
– Professional: 1.14 RVU, 0%; $40.81; 0%
– Physician Work (wRVU): 0.74, No change
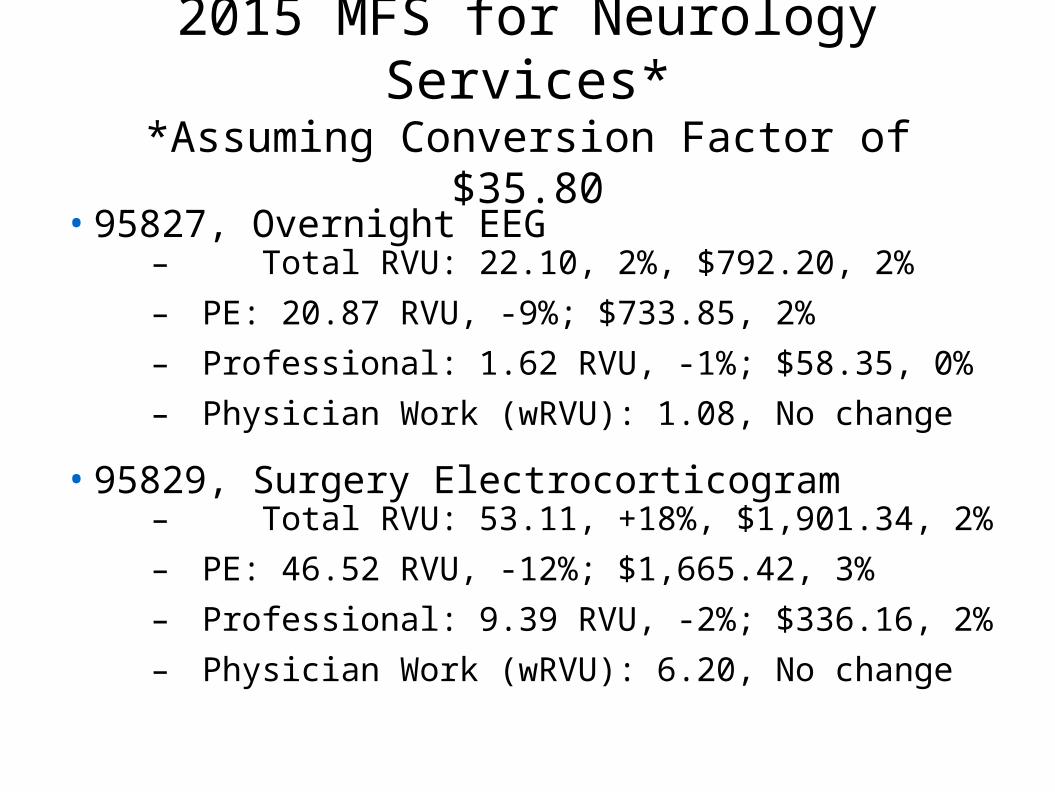
2015 MFS for Neurology Services**Assuming Conversion Factor of $35.80
• 95827, Overnight EEG– Total RVU: 22.10, 2%, $792.20, 2%
– PE: 20.87 RVU, -9%; $733.85, 2%
– Professional: 1.62 RVU, -1%; $58.35, 0%
– Physician Work (wRVU): 1.08, No change
• 95829, Surgery Electrocorticogram– Total RVU: 53.11, +18%, $1,901.34, 2%
– PE: 46.52 RVU, -12%; $1,665.42, 3%
– Professional: 9.39 RVU, -2%; $336.16, 2%
– Physician Work (wRVU): 6.20, No change

2015 MFS for Neurology Services**Assuming Conversion Factor of $35.80
• 95950, Ambulatory Cassette EEG, unattended (Old Oxford Medilog)– Total RVU: 9.26, -1%, $332.20, -1%
– PE: 7.66 RVU, -1%; $251.30, -1%
– Professional: 2.26 RVU, -1%; $80.90; -1%
– Physician Work (wRVU): 1.51, No change
• 95951, 24 Hour Video EEG Long Term Monitoring– Practice Expense: *Carrier-defined technical expense
– Professional: 9.27 RVU, 0%; $330.41, 0%
– Physician Work (wRVU): 5.99, No change
– Hospital coders: use 89.19 for inpatient coding
– Do not use this code for ambulatory in home recordings, use 95953

2001-2012 Claims for 95951, RUC database
2001 2002 2003 2004 2005 2006 2008 2009 2010 2011 20120
10000
20000
30000
40000
50000
60000
70000
80000
90000
100000

2015 MFS for Neurology Services**Assuming Conversion Factor of $35.80
• 95953, 24 hour automated ambulatory digital EEG, unattended
• Use this code for all uses of computerized digital EEG +/- video– Total RVU: 11.80, -3%, $422.05, -3%
– Practice Expense: 8.53 RVU, -4%; $256.31, -3%
– Professional: 4.65 RVU, 0%; $165.74, 0%
– Physician Work (wRVU): 3.08, no change
• 95956, 24 Hour attended EEG without video (assuming 1 tech:: 2 patients)
– Total RVU: 47.02, 1%, $1,683.92, 1%
– Practice Expense: 43.04 RVU, 1%; $1,489.90; 1%
– Professional: 5.43 RVU, 0%; $194.02; 0%
– Physician Work (wRVU): 3.61, no change

2015 MFS for Neurology Services**Assuming a Conversion Factor of $35.80
• 95954, EEG with administration of drugs– Total RVU: 12.94, 5%, $463.58, 4%
– Practice Expense: 10.33 RVU, 7%; $337.21, 7%
– Professional: 3.54 RVU, 2%; $126.37, 2%
– Physician Work (wRVU): 2.45, no change
• 95955, EEG during surgery– Total RVU: 6.02, -2%, $215.50, -6%
– Practice Expense: 4.95 RVU, -7%; $161.09, -8%
– Professional: 1.52 RVU, 0%; $54.41, 0%
– Physician Work (wRVU): 1.01, no change
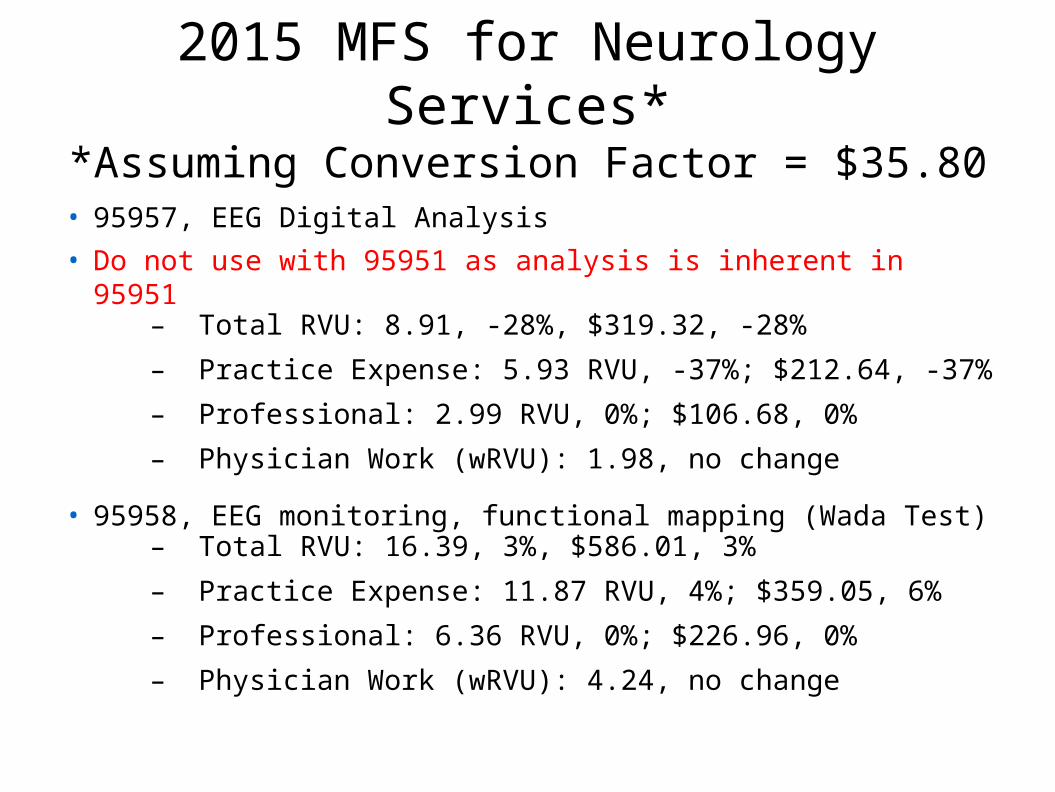
2015 MFS for Neurology Services**Assuming Conversion Factor = $35.80
• 95957, EEG Digital Analysis
• Do not use with 95951 as analysis is inherent in 95951– Total RVU: 8.91, -28%, $319.32, -28%
– Practice Expense: 5.93 RVU, -37%; $212.64, -37%
– Professional: 2.99 RVU, 0%; $106.68, 0%
– Physician Work (wRVU): 1.98, no change
• 95958, EEG monitoring, functional mapping (Wada Test)– Total RVU: 16.39, 3%, $586.01, 3%
– Practice Expense: 11.87 RVU, 4%; $359.05, 6%
– Professional: 6.36 RVU, 0%; $226.96, 0%
– Physician Work (wRVU): 4.24, no change
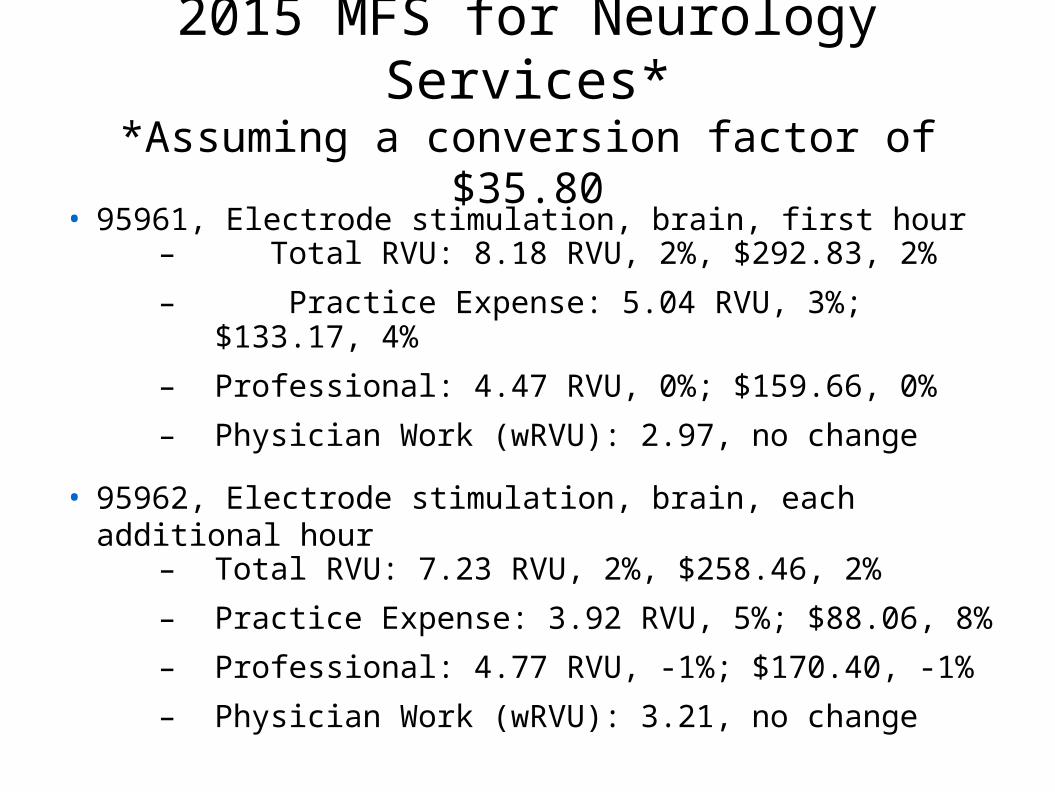
2015 MFS for Neurology Services**Assuming a conversion factor of $35.80
• 95961, Electrode stimulation, brain, first hour– Total RVU: 8.18 RVU, 2%, $292.83, 2%
– Practice Expense: 5.04 RVU, 3%; $133.17, 4%
– Professional: 4.47 RVU, 0%; $159.66, 0%
– Physician Work (wRVU): 2.97, no change
• 95962, Electrode stimulation, brain, each additional hour– Total RVU: 7.23 RVU, 2%, $258.46, 2%
– Practice Expense: 3.92 RVU, 5%; $88.06, 8%
– Professional: 4.77 RVU, -1%; $170.40, -1%
– Physician Work (wRVU): 3.21, no change
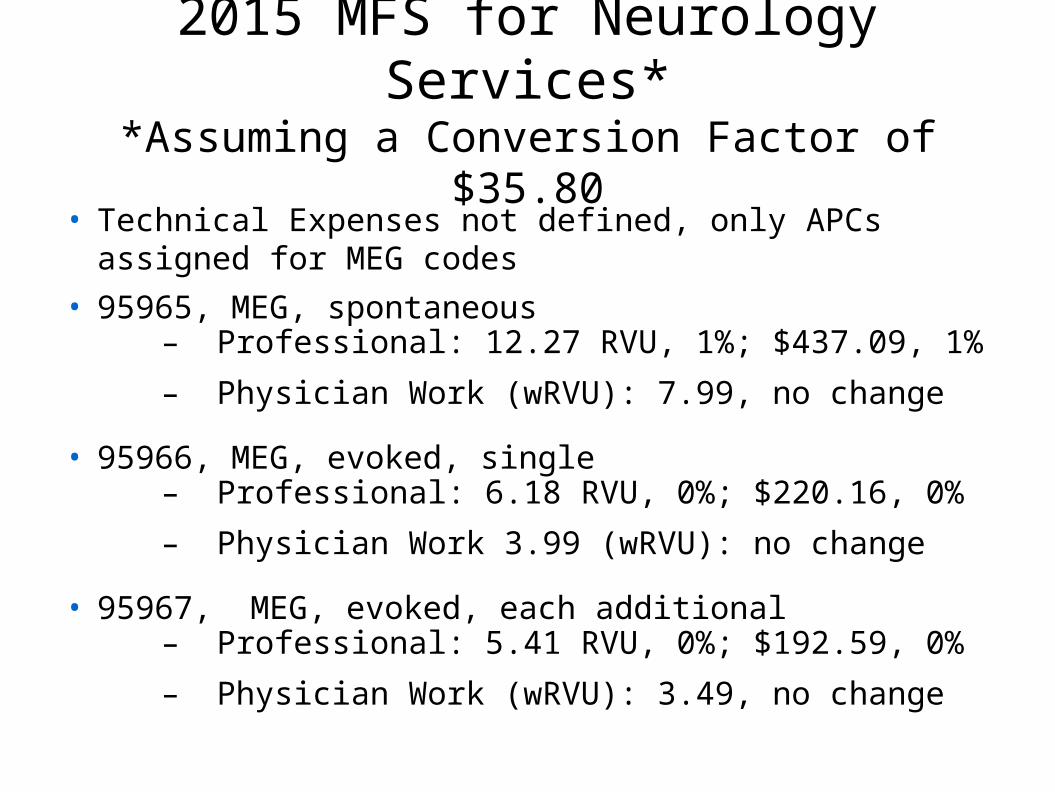
2015 MFS for Neurology Services**Assuming a Conversion Factor of $35.80
• Technical Expenses not defined, only APCs assigned for MEG codes
• 95965, MEG, spontaneous– Professional: 12.27 RVU, 1%; $437.09, 1%
– Physician Work (wRVU): 7.99, no change
• 95966, MEG, evoked, single– Professional: 6.18 RVU, 0%; $220.16, 0%
– Physician Work 3.99 (wRVU): no change
• 95967, MEG, evoked, each additional– Professional: 5.41 RVU, 0%; $192.59, 0%
– Physician Work (wRVU): 3.49, no change

2015 MFS for Neurology Services**Assuming a Conversion Factor of $35.80
• 95970, Analyze neurostimulator, no programming– Total RVU: 1.89, -2%, $67.66, -2%
– Practice Expense: 1.40 RVU, -3%;
– Physician Work (wRVU): 0.45, no change
• 95974, Cranial neurostimulation, complex analysis and programming, first hour (3 or more parameters)
– Total RVU: 5.89, 0%, $209.42, 0%
– Practice Expense: 2.59 RVU, 0%
– Physician Work (wRVU): 3.00, no change
– Use -52 modifier if less than 30 minutes
• 95975 Cranial neurostimulation, complex, each additional 30 minutes
– Total RVU: 3.16 RVU, 1%, $112.76, 1%
– Practice Expense: 1.31 RVU, 0%
– Physician Work (wRVU): 1.70, no change

CPT Medicare Payment Relative to Site of Services
Inpatient care:
– Professional fee paid to physician using -26 modifier
– Technical fee paid by DRG to hospital using IPPS (DRG values based upon hospital cost reporting) Top-down methodology based upon hospital-supplied cost data
Outpatient care: Provider-based billing
– Professional fee paid to physician using -26 modifier
– Technical fee paid to medical center using HOPPS (APC charges based upon hospital cost reporting averaged for all procedures in the APC) Top-down methodology
Outpatient care: private office
– Professional fee bundled with technical payment, so-called global billing using CMS MFS largely following RUC recommended values. Bottom-up methodology by RUC PE
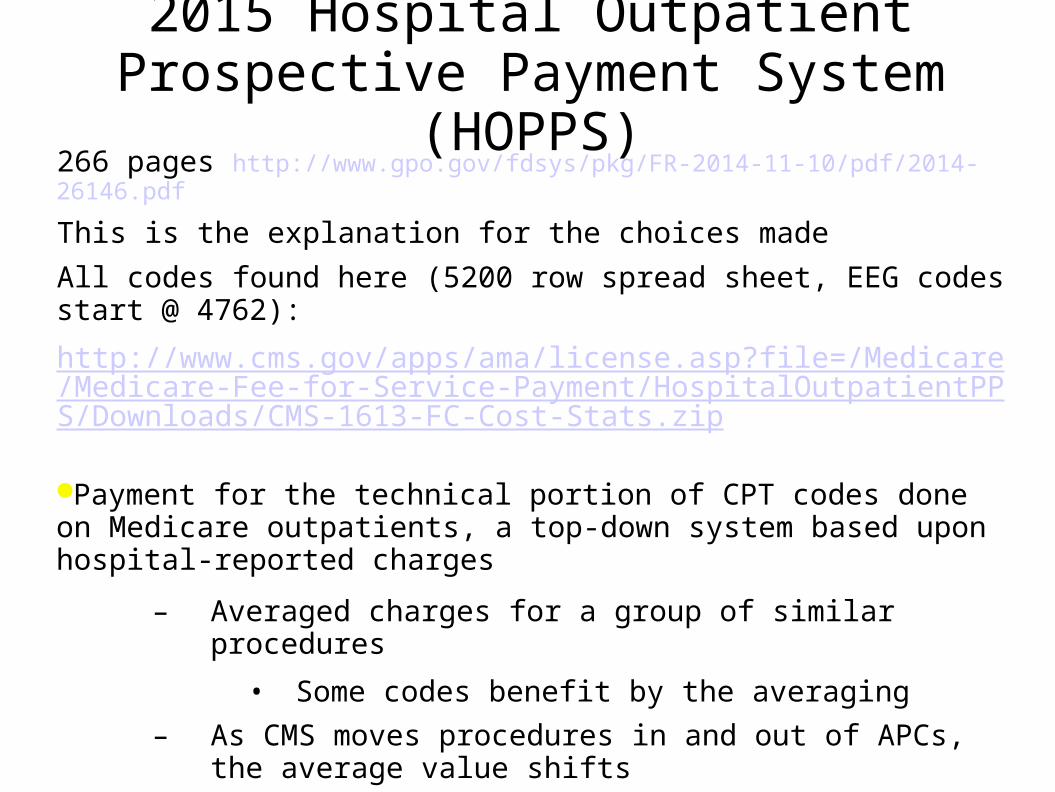
2015 Hospital Outpatient Prospective Payment System (HOPPS)
266 pages http://www.gpo.gov/fdsys/pkg/FR-2014-11-10/pdf/2014-26146.pdf
This is the explanation for the choices made
All codes found here (5200 row spread sheet, EEG codes start @ 4762):
http://www.cms.gov/apps/ama/license.asp?file=/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Downloads/CMS-1613-FC-Cost-Stats.zip
Payment for the technical portion of CPT codes done on Medicare outpatients, a top-down system based upon hospital-reported charges
– Averaged charges for a group of similar procedures
• Some codes benefit by the averaging
– As CMS moves procedures in and out of APCs, the average value shifts
– Major rearrangement in EEG APCs in 2015
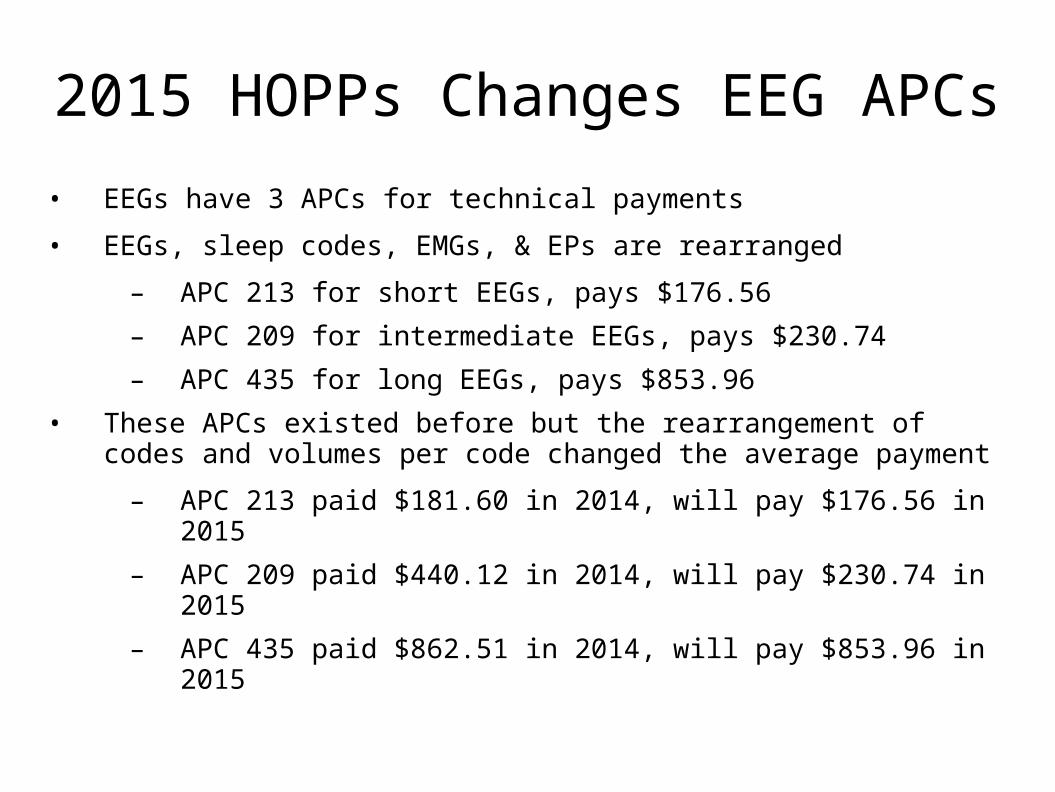
2015 HOPPs Changes EEG APCs
• EEGs have 3 APCs for technical payments
• EEGs, sleep codes, EMGs, & EPs are rearranged
– APC 213 for short EEGs, pays $176.56
– APC 209 for intermediate EEGs, pays $230.74
– APC 435 for long EEGs, pays $853.96
• These APCs existed before but the rearrangement of codes and volumes per code changed the average payment
– APC 213 paid $181.60 in 2014, will pay $176.56 in 2015
– APC 209 paid $440.12 in 2014, will pay $230.74 in 2015
– APC 435 paid $862.51 in 2014, will pay $853.96 in 2015
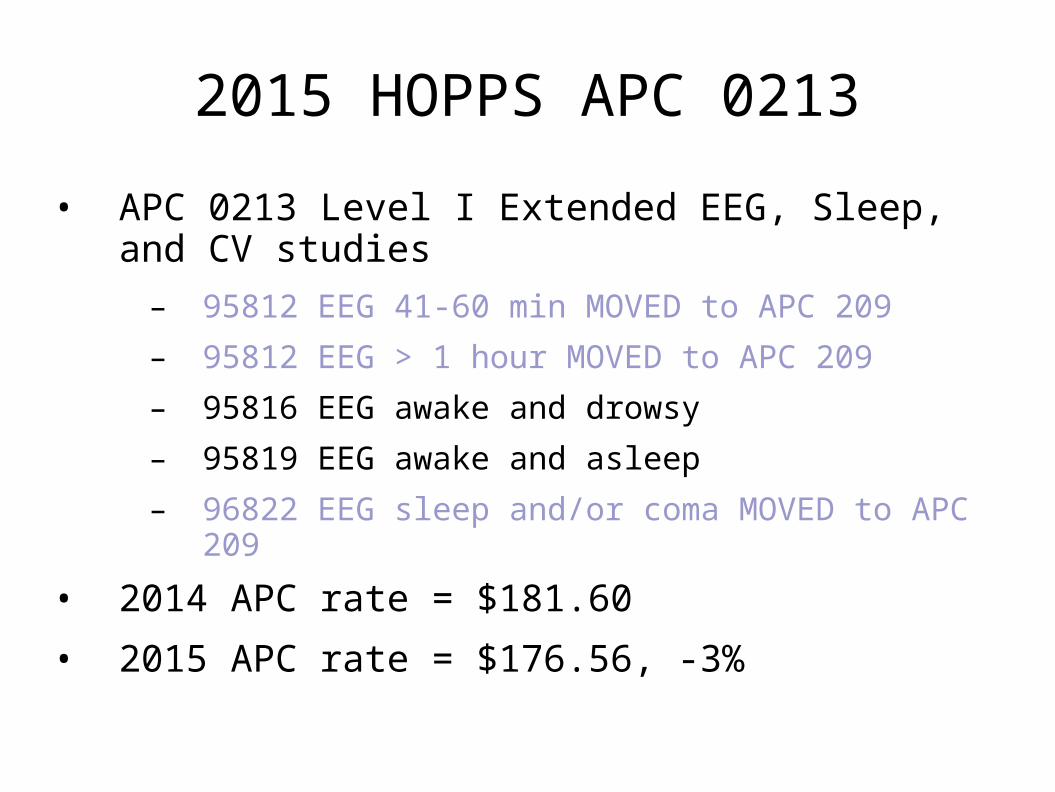
2015 HOPPS APC 0213
• APC 0213 Level I Extended EEG, Sleep, and CV studies
– 95812 EEG 41-60 min MOVED to APC 209
– 95812 EEG > 1 hour MOVED to APC 209
– 95816 EEG awake and drowsy
– 95819 EEG awake and asleep
– 96822 EEG sleep and/or coma MOVED to APC 209
• 2014 APC rate = $181.60
• 2015 APC rate = $176.56, -3%

2015 HOPPS APC 0209
• APC 0209 Level II Extended EEG, Sleep & CV
– 95812 EEG 41-60 min, MOVED from APC 213
– 95813 EEG > 1 hour, MOVED from APC 213
– 95822 Sleep/Coma EEG, MOVED from APC 213
– 95950 amb. cassette EEG, MOVED to 435
– 95953 ambulatory digital EEG, MOVED to 435
– 95956 24 hour EEG w/o video, MOVED to 435
– 95827 All night EEG
• 2015 APC Rate = $230.74, -47%
• 2014 APC Rate = $440.12
• 2013 APC Rate = $806.13

2015 HOPPS APC 0435 (new in 2014)
• APC 0435 Level III Extended EEG, Sleep & CV
– 95050 Amb Cassette EEG, MOVED from 209
– 95951 24 Hr Video EEG
– 95953 Amb Digital EEG, MOVED from 209
– 95956 24 Hr EEG w/o Video, MOVED from 209
– 95958 WADA test
• 2014 APC Rate = $862.51
• 2015 APC Rate = $853.93, -1%
2015 HOPPS APC 0215
• APC 215 Level I Nerve and Muscle Tests
– 95970 Neurostimulation, analysis with no programming
• 2014 payment = $50.30
• 2015 payment = $94.93, 89%

2015 HOPPS APC 216
• APC 216 Level III Nerve and Muscle Tests
– 95961 Cortical Stimulation, 1st hour
– 95824, EEG cerebral death only
• 2015 APC Rate = $272.60, 26%
• 2014 APC rate = $216.79
N.B., 95962 Cortical Stimulation, each additional hour, now has no technical payment
This APC also contains NCVs 5-6, 7-8, 9-10, 11-12, 13 />

2015 HOPPS APC 0692• APC 0692 Level II Electronic Analysis of Devices
– 95971 Analyze neurostim, simple
– 95972 Analyze neurostim, complex
– 95974 Cranial neurostim, complex
• 2014 payment = $115.86
• 2015 payment = $128.18, 11%
• NB, For 95973 and 95975, there are no longer technical payments (applies to all add-on codes)
2015 MEG HOPPsA.Technical payments for MEG studies in hospital-based outpatient care facilities
Does not apply to free standing MEG sites
• Carrier priced
Does not apply to MEG studies done on inpatients
• Technical fees bundled to DRG
In 2013, MEG was listed in APC 0066 Level II Stereotactic Radiosurgery, MRgFUS, and MEGAPC 0065 Level I Stereotactic radiosurgery, MRgFUS, and MEGIn 2014, MEG switched to APC 0065 IORT, MRgFUS, and MEGIn 2015, 95965 and 95966 now in APC 0446
2015 HOPPS MEG payment
• In 2013, APC 0066, MEG = $2,520.30 for 95965
• For 2014, MEG 95965 moved to APC 0065 (with 95966)
– APC 0065 Rate = $1,248.28, -50% for MEG 95965
– 2013 APC Rate for 0065 was $978.25, +28% for 95966
– 95967, no technical payment since it is an add-on code
• For 2015, MEG 95965 and 95966 moves to APC 0446
– 2015 APC 0446 Rate = $1,300.45, a 4% increase
– No technical payment for 95967 since it is an add-on code

ICD-10-CM
• The CDC has released the 2015 version of ICD-10-CM
• These codes will be mandatory to file claims starting 10/1/2015
• The following slides will display just the essential epilepsy and seizure codes
– You will need additional learning to code properly
• Complete instructions and all of the codes can be found here:
http://www.cdc.gov/nchs/icd/icd10cm.htm#icd2015
G40-G47 Episodic and Paroxysmal Disorders
G40 Epilepsy and recurrent seizures
Note: the following terms are to be considered equivalent to intractable: pharmacoresistant (pharmacologically resistant), treatment resistant, refractory (medically) and poorly controlled
Excludes1: [An Excludes1 note indicates that the code excluded should never be reported with the code above the Excludes1 note.]
conversion disorder with seizures (F44.5)
convulsions NOS (R56.9)
hippocampal sclerosis (G93.81)
mesial temporal sclerosis (G93.81)
post traumatic seizures (R56.1)
seizure (convulsive) NOS (R56.9)
seizure of newborn (P90)
temporal sclerosis (G93.81)
Todd's paralysis (G83.8)

G40 General Code Convention
G40.XYZ
Where
X = Generalized, Localized, or Special Syndrome
Y = Not Intractable (0) or Intractable (1)
Z = With Status Epilepticus (1) or Without Status Epilepticus (9)

G40.0 Localization-related Idiopathic Epilepsy
G40.0 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset
Benign childhood epilepsy with centrotemporal EEG spikes
Childhood epilepsy with occipital EEG paroxysms
Excludes1:
adult onset localization-related epilepsy (G40.1-, G40.2-)
G40.00 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, not intractable
Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset without intractability
G40.001 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, not intractable, with status epilepticus
G40.009 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, not intractable, without status epilepticus
Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset NOS
G40.01 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, intractable
G40.011 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, intractable, with status epilepticus
G40.019 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset, intractable, without status epilepticus
.
G40.1 Localization-related Symptomatic Epilepsy with SPS
G40.1 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures
Attacks without alteration of consciousness
Epilepsia partialis continua [Kozhevnikof]
Simple partial seizures developing into secondarily generalized seizures
G40.10 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, not intractable
Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures without intractability
G40.101 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, not intractable, with status epilepticus
G40.109 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, not intractable, without status epilepticus
Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures NOS
G40.11 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, intractable
G40.111 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, intractable, with status epilepticus
G40.119 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures, intractable, without status epilepticus
.
G40.2 Localization-related Symptomatic Epilepsy with CPS
G40.2 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures
Attacks with alteration of consciousness, often with automatisms
Complex partial seizures developing into secondarily generalized seizures
G40.20 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, not intractable
Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures without intractability
G40.201 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, not intractable, with status epilepticus
G40.209 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, not intractable, without status epilepticus
Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures NOS
G40.21 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, intractable
G40.211 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, intractable, with status epilepticus
G40.219 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures, intractable, without status epilepticus
.

G40.3 Generalized Idiopathic Epilepsy
G40.3 Generalized idiopathic epilepsy and epileptic syndromes
Code also MERRF syndrome, if applicable (E88.42)
G40.30 Generalized idiopathic epilepsy and epileptic syndromes, not intractable
Generalized idiopathic epilepsy and epileptic syndromes without intractability
G40.301 Generalized idiopathic epilepsy and epileptic syndromes, not intractable, with status epilepticus
G40.309 Generalized idiopathic epilepsy and epileptic syndromes, not intractable, without status epilepticus
Generalized idiopathic epilepsy and epileptic syndromes NOS
G40.31 Generalized idiopathic epilepsy and epileptic syndromes, intractable
G40.311 Generalized idiopathic epilepsy and epileptic syndromes, intractable, with status epilepticus
G40.319 Generalized idiopathic epilepsy and epileptic syndromes, intractable, without status epilepticus
.
G40.A Absence Epileptic Syndromes
G40.A Absence epileptic syndrome
Childhood absence epilepsy [pyknolepsy]
Juvenile absence epilepsy
Absence epileptic syndrome, NOS
G40.A0 Absence epileptic syndrome, not intractable
G40.A01 Absence epileptic syndrome, not intractable, with status epilepticus
G40.A09 Absence epileptic syndrome, not intractable, without status epilepticus
G40.A1 Absence epileptic syndrome, intractable
G40.A11 Absence epileptic syndrome, intractable, with status epilepticus
G40.A19 Absence epileptic syndrome, intractable, without status epilepticus
.
G40.B Juvenile Myoclonic Epilepsy
G40.B Juvenile myoclonic epilepsy [impulsive petit mal]
G40.B0 Juvenile myoclonic epilepsy, not intractable
G40.B01 Juvenile myoclonic epilepsy, not intractable, with status epilepticus
G40.B09 Juvenile myoclonic epilepsy, not intractable, without status epilepticus
G40.B1 Juvenile myoclonic epilepsy, intractable
G40.B11 Juvenile myoclonic epilepsy, intractable, with status epilepticus
G40.B19 Juvenile myoclonic epilepsy, intractable, without status epilepticus
.

G40.4 Other Generalized Epilepsy and Epileptic SyndromesG40.4 Other generalized epilepsy and epileptic syndromes
Epilepsy with grand mal seizures on awakening
Epilepsy with myoclonic absences
Epilepsy with myoclonic-astatic seizures
Grand mal seizure NOS
Nonspecific atonic epileptic seizures
Nonspecific clonic epileptic seizures
Nonspecific myoclonic epileptic seizures
Nonspecific tonic epileptic seizures
Nonspecific tonic-clonic epileptic seizures
Symptomatic early myoclonic encephalopathy
G40.40 Other generalized epilepsy and epileptic syndromes, not intractable
Other generalized epilepsy and epileptic syndromes without intractability
Other generalized epilepsy and epileptic syndromes NOS
G40.401 Other generalized epilepsy and epileptic syndromes, not intractable, with status epilepticus
G40.409 Other generalized epilepsy and epileptic syndromes, not intractable, without status epilepticus
G40.41 Other generalized epilepsy and epileptic syndromes, intractable
G40.411 Other generalized epilepsy and epileptic syndromes, intractable, with status epilepticus
G40.419 Other generalized epilepsy and epileptic syndromes, intractable, without status epilepticus
.
G40.5 Epileptic Seizures Related to External Causes
G40.5 Epileptic seizures related to external causes
Epileptic seizures related to alcohol
Epileptic seizures related to drugs
Epileptic seizures related to hormonal changes
Epileptic seizures related to sleep deprivation
Epileptic seizures related to stress
Use additional code for adverse effect, if applicable, to identify drug (T36-T50 with fifth or sixth character 5)
Code also, if applicable, associated epilepsy and recurrent seizures (G40.-)
G40.50 Epileptic seizures related to external causes, not intractable
G40.501 Epileptic seizures related to external causes, not intractable, with status epilepticus
G40.509 Epileptic seizures related to external causes, not intractable, without status epilepticus
Epileptic seizures related to external causes, NOS
.

G40.8 Other Epilepsy and Recurrent Seizures, part I
G40.8 Other epilepsy and recurrent seizures
Epilepsies and epileptic syndromes undetermined as to whether they are focal or generalized
Landau-Kleffner syndrome
G40.80 Other epilepsy
G40.801 Other epilepsy, not intractable, with status epilepticus
Other epilepsy without intractability with status epilepticus
G40.802 Other epilepsy, not intractable, without status epilepticus
Other epilepsy NOS
Other epilepsy without intractability without status epilepticus
G40.803 Other epilepsy, intractable, with status epilepticus
G40.804 Other epilepsy, intractable, without status epilepticus
G40.81 Lennox-Gastaut syndrome
G40.811 Lennox-Gastaut syndrome, not intractable, with status epilepticus
G40.812 Lennox-Gastaut syndrome, not intractable, without status epilepticus
G40.813 Lennox-Gastaut syndrome, intractable, with status epilepticus
G40.814 Lennox-Gastaut syndrome, intractable, without status epilepticus
.
G40.8 Other Epilepsy and Recurrent Seizures, part II
G40.82 Epileptic spasms
Infantile spasms
Salaam attacks
West's syndrome
G40.821 Epileptic spasms, not intractable, with status epilepticus
G40.822 Epileptic spasms, not intractable, without status epilepticus
G40.823 Epileptic spasms, intractable, with status epilepticus
G40.824 Epileptic spasms, intractable, without status epilepticus
G40.89 Other seizures
Excludes1: post traumatic seizures (R56.1)
recurrent seizures NOS (G40.909)
seizure NOS (R56.9)
.

G40.9 Epilepsy, Unspecified
G40.9 Epilepsy, unspecified
G40.90 Epilepsy, unspecified, not intractable
Epilepsy, unspecified, without intractability
G40.901 Epilepsy, unspecified, not intractable, with status epilepticus
G40.909 Epilepsy, unspecified, not intractable, without status epilepticus
Epilepsy NOS
Epileptic convulsions NOS
Epileptic fits NOS
Epileptic seizures NOS
Recurrent seizures NOS
Seizure disorder NOS
G40.91 Epilepsy, unspecified, intractable
Intractable seizure disorder NOS
G40.911 Epilepsy, unspecified, intractable, with status epilepticus
G40.919 Epilepsy, unspecified, intractable, without status epilepticus
.
R56 Convulsions not elsewhere classified
CR56 Convulsions, not elsewhere classified
Excludes1:
dissociative convulsions and seizures (F44.5)
epileptic convulsions and seizures (G40.-)
newborn convulsions and seizures (P90)
R56.0 Febrile convulsions
R56.00 Simple febrile convulsions
Febrile convulsion NOS
Febrile seizure NOS
R56.01 Complex febrile convulsions
Atypical febrile seizure
Complex febrile seizure
Complicated febrile seizure
Excludes1:
status epilepticus (G40.901)
R56.1 Post traumatic seizures
Excludes1:
post traumatic epilepsy (G40.-)
R56.9 Unspecified convulsions
Convulsion disorder
Fit NOS
Recurrent convulsions
Seizure(s) (convulsive) NOS

Support Your Patients – Buy their products and services. The job you save may be your own.
Unless you do funded research, you are in the service industry and your job depends upon having primary producers to pay for your services
You should shop locally, particularly if you practice in a small town www.buymichiganproducts.com/

Professionalism
This has been a business talk, but do not forget why you became a physician in the first place. Those blessed with extraordinary gifts have extraordinary obligations.
You are expected to give back to the community by donating your talent, your time, and your money to support worthy causes
These include: your hospital, nonprofit disease organizations such as the Epilepsy Foundation, the American Academy of Neurology, etc.