Adverse Food Reactions & Inflammation Understanding the Connection and Empowering Patients to Heal...
60
Adverse Food Reactions & Inflammation Understanding the Connection and Empowering Patients to Heal from the Inside Out BY ERIN PEISACH, RDN, CLT OWNER OF
-
Upload
stanley-chandler -
Category
Documents
-
view
213 -
download
0
Transcript of Adverse Food Reactions & Inflammation Understanding the Connection and Empowering Patients to Heal...

Adverse Food Reactions & Inflammation
Understanding the Connection and Empowering Patients to Heal from the Inside Out
BY ERIN PEISACH, RDN, CLTOWNER OF

Objectives
Briefly review the immune system as it relates to inflammation.
Highlight the connection between inflammation, adverse food reactions (AFR), and disease.
Explain various types of AFRs, emphasizing immune-mediated reactions, and review diagnostics, symptoms and treatment options.
Outline the tools RDNs may provide their patients with AFRs to help reduce inflammation, improve symptoms, and promote the healing process.
Review an AFR case study.

The Immune System

Purpose of The Immune System: Immune cells and other components fight
invaders to keep the body healthy and safe
Invaders: bacteria, viruses, parasites, & food
Military Personnel: • White Blood Cells:
• Mast cells, basophils, eosinophils, lymphocytes, neutrophils, monocytes, macrophages, T-cells, NK-cells
• Antibodies:
• IgE, IgG, IgM, IgA, IgD
• Complement System:
• C3, C4
• Platelets
• Chemical Mediators
• Histamine, prostaglandins, serotonin, cytokines, leukotrienes, etc.
My Kindergarten take on the topic

Immune System 101
Innate Involves barriersFirst line of defense
AdaptivePrevents
indiscriminate responses to harmless antigens
Long lasting defense

Gut Immunology
GI tract has two major roles:
Digestion and absorption of nutrients
Immune homeostasis
Constantly exposed to chemicals, proteins, bacteria, & antigens
Separates the external environment from the internal environment
The gut ultimately must decide: friend or foe?

Gut Immunology
Gut associated lymphoid tissue (GALT):
Aka The Gut Immune System
Largest immune organ in the body

Definitions:
Intestinal barrier: is a functional entity separating the gut lumen from the inner host
Intestinal permeability: a functional feature of the intestinal barrier at given sites Normal: stable permeability found in healthy individuals with no
signs of intoxication, inflammation or impaired intestinal functions Impaired: a disturbed permeability being non-transiently
changed compared to the normal permeability leading to a loss of intestinal homeostasis, functional impairments and disease
Bischoff et al. BMC Gastroenterology 2014 14:189

Intestinal Permeability
Impaired intestinal barrier integrity in the colon of patients with irritable bowel syndrome: involvement of soluble mediators. – 2008 study in BMJ
Conclusions: “Our study shows that colonic soluble mediators are able to reproduce functional (permeability) and molecular (ZO-1 mRNA expression) alterations observed in IBS patients.”

Healthy Digestive Pathway
Digestion of food begins in the mouth, then travels to the stomach
Food/proteins interact with gastric acid and enzymes, turning into smaller particles ready for absorption
Once the particles (antigens) pass the epithelium barrier, the immune system typically expresses oral tolerance
The GALT is tightly regulated to prevent excessive immune responses

Oral Tolerance Definition: Active systemic suppression of cellular or humoral
immune responses to an antigen following prior administration of the antigen by the oral route
Impacted by: Antigen specific elements
Age
Genetics
Intestinal microbial environment
Changes throughout the lifetime
Loss of oral tolerance triggers immune reactions that may cause adverse food reactions and pathological conditions

Inflammation

Inflammation- to set on fire (Latin) Acute inflammation
Natural and essential for health
Defend, fight, repair, & heal
Caused by short term injury Tissue injury, infections, immune reactions
Symptoms: heat, redness, swelling, pain, loss of function
Chronic inflammation Long term damaging to health
Related to disease, illness, and reduced quality of life
Caused by on-going injury SAD diet, nutrient deficiencies, obesity, stress
Symptoms: chronic pain, allergies, fatigue, altered blood sugar, cancer

Gastrointestinal:• Cyclic Vomiting
Syndrome• Functional Diarrhea• Irritable Bowel
Syndrome• Lymphocytic Colitis• Crohn’s Disease• Ulcerative Colitis• GERD• Celiac Disease• Systemic Lupus
Neurological:• Migraine• ADD/ADHD• Autism Spectrum
Disorder• Epilepsy• Depression• Insomnia• Multiple Sclerosis
Musculoskeletal:• Fibromyalgia• Rheumatoid Arthritis• Reactive Arthritis• Chronic Fatigue
Syndrome
Metabolic:• Metabolic
Syndrome• Obesity• Type 1 Diabetes• Type II Diabetes
Dermatological:• Atopic Dermatitis• Dermatitis
Herpetiformis• Urticaria• Psoriasis
Pulmonology• Asthma• Anaphylaxis
Urology• Interstitial
Cystitis
Endocrinology• Hashimoto’s• Grave’s Disease
Inflammation & Disease

Steps to Consider to Reduce Inflammation:
Identify inflammator
y triggers
Remove triggers
Heal the gut &
boost the immune system
Reduce
inflammation
Support
sustained
improvement in disease,
illness &
symptoms

Inflammatory Triggers Psychological
Stress, depression, anxiety
Environmental Mold, pollution, lack of outdoors/sunlight, allergens, toxin exposure
Lifestyle Choices Sedentary lifestyle, tobacco/drug/alcohol use, lack of sleep
Dietary choices Adverse food reactions, inadequate nutrient intake, excessive intake
of poor quality/processed foods
Other Overweight/obesity, genetic predisposition

How Food Sensitivities Cause Inflammation

There is a strong connection between gastrointestinal health,
immune system function, inflammation, and adverse food
reactions.

Adverse Food Reactions

20
AFR
Toxic
Food Contaminant
Non Toxic
Immune mediated
Allergy
Sensitivity
Celiac
Non-immune mediated
Intolerance
Aversion
Adverse Food Reactions (AFR):

Non-Immunol
ogic Reaction
s
Enzyme Deficien
cies
Toxic Reaction
sMalabsorption
(FODMAPS)
Lectins
Histamine
Irritants

IMMUNE REACTIONS
ALLERGIES
TYPE 1
SENSITIVITIES
TYPE 3 TYPE 4

Food Allergy- Type 1 Hypersensitivity

Food Allergy Impacts ~6% of children and 3.7% of adults
Risk factors: family history
male sex
genetic polymorphisms
early infectious exposure
rural upbringing with exposure to animals and livestock (protective)
pathogenic microorganisms
gut mucosa
antigenic characteristic of food proteins (size, abundance, resistance to acidic and enzymatic denaturation and digestion, immunogenicity)
sanitary living
No prevention strategies known at this time

Food Allergy
Most common allergens (accounts for >90% of cases in children): Hen’s egg
Cow’s milk
Peanuts
Soybean products
Wheat
Tree nuts
Fish
Shellfish

Food Allergy
Symptoms Skin- itching, hives, angioedema, flushing
GI- oral itching, nausea, vomiting, diarrhea
Nasal/respiratory tract- nasal congestion, runny nose, itchy eyes/nose, sneezing, laryngeal edema, wheezing, shortness of breath
Cardiovascular system- light headedness, syncope, hypotension
Oral Allergy Syndrome
Most common food allergy in adults
Examples: birch-fruit/veggie, celery-birch-mugwort, ragweed-melon/banana
Generally more mild symptoms primarily in the oropharynx
Lip/mouth itching, swelling, hoarseness, rhinitis, etc.

Food Allergy- Testing Begin assessment with thorough clinical history and physical exam
Patient will typically report reproducible symptoms occurring after exposure to a food
Oral Food Challenge The definitive, gold standard test
In vivo testing (SPT/Scratch test): skin test
In vitro testing (RAST/ELISA): blood test

Food Allergy- Treatment
Remove food from the diet completely, including cross contamination exposure
Consider oral food challenge (ideally double-blind, placebo-controlled) Weigh the risks (anaphylaxis, other symptoms) and benefits
(nutritional, social, quality of life)
Medical supervision
Protocol: 1-6 weeks (varies based on severity) elimination followed by monitored/controlled food reintroduction
Limitations: concerns about safety, time, reimbursement, lack of space/time

Food Sensitivity- Type III & IV Hypersensitivity

Food Sensitivity
Type 3 & 4 immune-mediated reaction
Develops after loss of oral tolerance
No set list of common reactive foods
Dose-dependent reaction
Delayed reaction time (4-72 hours post-ingestion)
Patient is likely to have more than one reactive food (typically 10-20)
Symptoms vary- impact the body anywhere blood flows
Difficult to identify/diagnose- more research is needed

Food Sensitivity (FS)
May be associated with: Intestinal dysbiosis Increased gut permeability Stress Anxiety/depression Immunological and local factors

FS Symptoms
Systemic symptoms
Patients typically report multiple symptoms

Food Sensitivity- Testing No test is currently supported by strong evidence
ELISA IgG or IgG4 Antibodies
Quantifies the level of IgG response to specific foods
Tests foods only, not food chemicals
Elevated IgG may be harmful or protective
Antigen Leukocyte Cellular Antibody Test (ALCAT)
End-point blood test that quantifies mediator release (i.e. histamine, cytokines, prostaglandins, etc.)
Tests both foods and food chemicals
Poor split sample reproducibility, low accuracy, outdated technology
Mediator Release Test (MRT)
Similar, but updated ALCAT technology
Tests both foods and food chemicals
94.5%sensitivity, 91.7% specificity (high accuracy) and >90% split sample reproducibility (high reliability)

“ Food specific IgG antibodies in serum are not of clinical importance but merely indicate a previous exposure to the food.”
-Krause’s Food Nutrition and Diet Therapy 2008
IgG “is a marker of exposure and tolerance to food…”
-Canadian Society of Allergy and Clinical Immunology
“…the direct clinical meaning of food IgG testing is not known. The industry needs more extensive clinical research in this area.”
-Aristo Vojdani, PhD, MSc, CLS, Alternative Therapies 2015

How MRT Works


Food Sensitivity- Treatment
Elimination Diet (at least two weeks)
Specific Foods
Low FODMAPS, gluten, dairy, nightshades, soy, etc.
Oligoantigenic/Selected Foods
LEAP protocol
Elemental
Oral Food Challenge
Heal/repair the gut
Rotation Diets?

Examples of Elimination Diets Rowe Elimination Diet:
5-10 foods only
Institute of Functional Medicine Diet: avoid gluten, corn, soy, dairy, shellfish, beef, pork, peanuts, eggs,
oranges, refined sugar
Lifestyle Eating And Performance Diet (LEAP) 6 Phase-diet based on results of MRT testing and clinical history
SWAG Diet:

Commonly Eliminated FoodsFatty meats: beef, pork, veal Eggs
Dairy and products made from dairy Gluten and products made from gluten
Corn and products made from corn Alcohol/Caffeine
Foods containing yeast or promoting yeast overgrowth: processed foods, refined sugar, cheese, peanuts, vinegar
Simple carbohydrates: sugar, “white” flour, processed foods, soda
Unhealthy fats: margarine, shortening, butter
Peanuts
Strawberries and citrus fruit Foods with high FODMAPs: apples, onions, dairy, legumes, etc.
Additives and preservatives Soy and products made from soy

Summary of Immune-Mediated AFRs
Food Allergy Food Sensitivity
What Is It? Generally Quick Immune Reaction That Results in Hives, Asthma, Swelling of Airways, Vomiting
Often Delayed Immune Reaction That Results In Chronic Health Problems Like IBS & Migraine Headaches
Unique Characteristics: Quick ReactionAnaphylactic ShockSingle Mechanism (IgE)
Delayed ReactionCan Be Dosage RelatedMultiple MechanismsDifficult to Identify Culprits
Cells Involved in Reaction:
Mast CellsPossibly Basophils
T-CellsNK CellsNeutrophilsMonocytesEosinophilsBasophilsPlatelets
Mechanisms Which Trigger Mediator Release:
IgE IgG, IgM, IgAC3, C4Immune CellsLectinsToxins

Dietitian Toolbox

Toolbox:
1. Help the patient identify inflammatory triggers/problematic foods
2. Design a systematic and effective elimination diet
3. Assess patient progress over time
4. Continue to help the patient heal, repair, and relieve inflammation through nutrition and lifestyle interventions

1. Help the patient identify inflammatory triggers
Complete a thorough clinical and family history Review the patient’s food and symptom diary Request appropriate testing as needed
Food Sensitivity? MRT Food Intolerance? Breathe Test Food Allergy? IgE skin prick or blood test

2. Design a systematic and effective elimination diet
Decide on the optimal dietary plan Will the patient comply? How severe are their symptoms? What previous diets have they tried?
Create a systematic approach Stay organized Avoid conflicting advice (i.e. FODMAP lists,
elimination protocols, celebrity diet-gurus, etc.) Be direct, yet flexible

LEAP Elimination Diet
20-25 of the best and “safest” foods for ~14 days (Phase 1) Patient agrees to consume the food and has consumed the food previously
No intolerances to the food
Food must be accessible and nutritionally valuable
Progress the diet systematically after significant symptom improvement is reported/documented. Foods to progress the diet can be based on: Specific food preferences/accessibility
Nutritional value
Likelihood of tolerance
Slowly- one new food every day or even every week
Document the “oral food challenge” in a food/symptom diary

Example:
Input TESTED foods into each of the 5 phases
Each food listed can be consumed in any “form” (i.e. apples, applesauce, apple juice, apple cider vinegar, etc.)
Each phase, beyond phase 1 lasts at minimum 5 days
Untested foods will be reintroduced after phase 5
The entire process may take >2 months

Food & Symptom Diary
Date/Time
Meds/
supplements taken
Food Eaten, Amounts and
Description: brand preparation, etc.
Symptoms?What and how severe (1-10)
Monitor adherence to the diet
Keep the patient engaged and accountable
Track even minute changes over time
Detective Work!

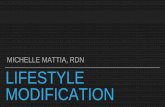
IBS-D PATIENT PLASMA CYTOKINES DURING D-EPISODE v BETWEEN EPISODES
0
50
100
150
200
250
300
350
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
See Specific Cytokine Key
pg
/ml Series1
Series2
Series3
1 IL-2
2 IL-4
3 IL-6
4 IL-8
5 IL-10
6 GM-CSF
7 IFN-g
8 TNF-a
9 IL-1b
10 IL-5
11 IL-7
12 IL-12
13 IL-13
14 IL-17
15 G-CSF
16 MCP-1(MCAF)
Patient on LEAP diet
Patient off LEAP diet
Cytokine Profile of Individual D-IBS Patient

3. Assess patient progress over time
Baseline- report symptoms over the previous month (0-4 rating)
Follow up- after 2 weeks on the program, monthly basis thereafter
Record progress
*Patients tend to “forget how they felt” so you must remind them!

4. Help the patient heal, repair, and relieve inflammation
AFRs are just ONE piece of the complex inflammation puzzle
Address other underlying inflammatory triggers
Develop a sustainable, healthy, anti-inflammatory maintenance plan Varied, balanced diet
Modify food preparation techniques, food quantity, and intake frequency
Weight management as needed
Nutritional supplements as needed

Anti-Inflammatory Recommendations:
Fats Omega 3s, monounsaturated fats Avoid fried foods and hydrogenated fats
Whole foods Antioxidant/colorful foods, herbs, spices High fiber Reduce intake of processed foods
Physical activity Avoid a sedentary lifestyle 10,000 steps per day Flexibility, strength, aerobic exercise
Sleep 7-9 hours of good quality sleep Nap as needed
Reduce toxin exposure Limit caffeine and alcohol Live a “natural” life
Stress management Practice mindfulness each day
Drink plenty of purified water Achieve a healthy weight

Case Study- MC
53 year old female, works as a librarian
Medical History: allergies, menopause, chronic low back pain, joint pain, IBS
Medications: albuterol, bupropion, Allegra, Flonase, D3 1000
BMI= 25.26, overweight
Generally appears healthy, exercises regularly, sleeps well, manages stress
MC’s Health Goals: improve pain, reduce allergic-type symptoms, improve digestive health

Case Study- MC
Diet description: low carb, high protein (fish, chicken, eggs), limits dairy, frequent consumption of fresh greens, 3 glasses of wine 2-3x per week, 1-2c coffee daily
No known food allergies, but avoids wheat, hot peppers and cucumbers related to digestive concerns
Symptoms: sinus congestion/cough/itchy eyes despite year round use of Allegra, daily gas and bloating, heartburn, fatigue, headache, others… Initial Symptom Survey= 69
Intervention: Start with specific food elimination diet: gluten, dairy, sugar, soy
Assess progress. If limited improvement, try olio-antigenic diet (LEAP) based on MRT results

Case Study- MC
INPUT results

Case Study- MC Phases 1-5
Phase 1: 2 weeks, baseline diet
Phases 2-5: minimum of 5 days each
Add 1 new food each day (or slower!)
Use the food plan to develop a menu plan: B: Hot quinoa flakes in soy milk, add maple syrup,
chopped walnuts, and sliced strawberries. Seltzer water with a few raspberries.
S: Hard-boiled egg
L: Steamed shrimp over cooked quinoa or amaranth, with a side of blanched string beans, toss in sesame oil and toasted sesame seeds.
S: Dry roasted or steamed edamame
D: Baked tofu (marinade in tamari, turmeric, tahini paste, oil). Side of roasted yellow squash.
S: Hot chocolate- heat up hazelnut or soy milk add carob powder & maple syrup

Case Study- MC
Follow up #1: Avoided all yellow and red MRT foods for 1 week, followed by…
LEAP phase 1 for 2 weeks Lost 6.6lb without limiting food quantity or exercising
Follow up SS total= 33 (Initial SS= 69, improved by 36 points in 3 weeks)
Follow up #2: Started probiotic (boost immune health) and curcumin (anti-inflammatory for
joint pain)
LEAP phases 2-5 for 1 month Lost 1 additional pound
Follow up #2 SS= 21 (improved by 12 additional points in 4 weeks, 48 total points)
Added in additional anti-inflammatory compounds: omega 3 fish oil, OPC-Sorb (antioxidant blend for pain)

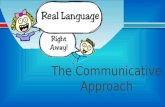
My Own Testimonial
R-arm, eczema flare up R-arm, after following LEAP elimination for 1 month

Conclusion
Inflammation, adverse food reactions, and chronic disease are interrelated and may be present in your patients.
By understanding various types of AFRs you will be able to better identify problematic foods and provide the appropriate dietary intervention.
Primum non nocere- first do no harm. Short-term elimination diets are typically not
harmful and may potentially change someone’s life! Help your patients to heal from the inside out,
supporting them through every step of the process.

References1. Food Allergy: Adverse Reactions to Foods and Food Additives, Fifth Edition. Edited by Dean
D Metcalfe, Hugh A Sampson, Ronald A Simon and Gideon Lack. 2014 John Wiley & Sons, Ltd. Published 2014 by John Wiley & Sons, Ltd.
2. Castro-Sanchez, P. & Martin-Villa, J.M. (2013). Gut immune system and oral tolerance. British Journal of Nutrition, 109, pp. S3-S11.
3. MacDonald T.T. & Monteleone G. (2005). Immunity, Inflammation, and Allergy in the Gut. Science, 307(5717), pp. 1920-1925.
4. Lied, GA. Indication of immune activation in patients with perceived food hypersensitivity. (2014). Dig Dis Sci, 59(2), 259-266.
5. LILLESTØL K, HELGELAND L, BERSTAD A, et al. Indications of ‘atopic bowel’ in patients with self-reported food hypersensitivity. Alimentary Pharmacology & Therapeutics [serial online]. May 15, 2010;31(10):1112-1122. Available from: Academic Search Premier, Ipswich, MA. Accessed March 18, 2015.
6. Thierry Piche, Giovanni Barbara, Philippe Aubert, Stanislas Bruley Des Varannes, Raffaella Dainese, et al. Impaired intestinal barrier integrity in the colon of patients with irritable bowel syndrome: involvement of soluble mediators.. Gut, BMJ Publishing Group, 2009, 58 (2), pp.196-201.
7. Pasula, Mark J.; The Patented Mediator Release Test (MRT); A Comprehensive Blood Test for Inflammation Caused by Food and Food-Chemical Sensitivities. Townsend Letter, January 2014

Thank you!
Erin Peisach, RDN, CLT
Nutrition by Erin, LLC
1777 Reisterstown Road, suite 118A
Pikesville, MD 21208
410-635-4210
www.nutritionbyerin.com
Follow me on facebook!