
Advancements in Cardiac Surgery - Cleveland Clinic · Isolated CABG Aorta 13% 16% 27% 22% N = 4,405...
114
Advancements in Cardiac Surgery
Transcript of Advancements in Cardiac Surgery - Cleveland Clinic · Isolated CABG Aorta 13% 16% 27% 22% N = 4,405...

Advancements in Cardiac Surgery
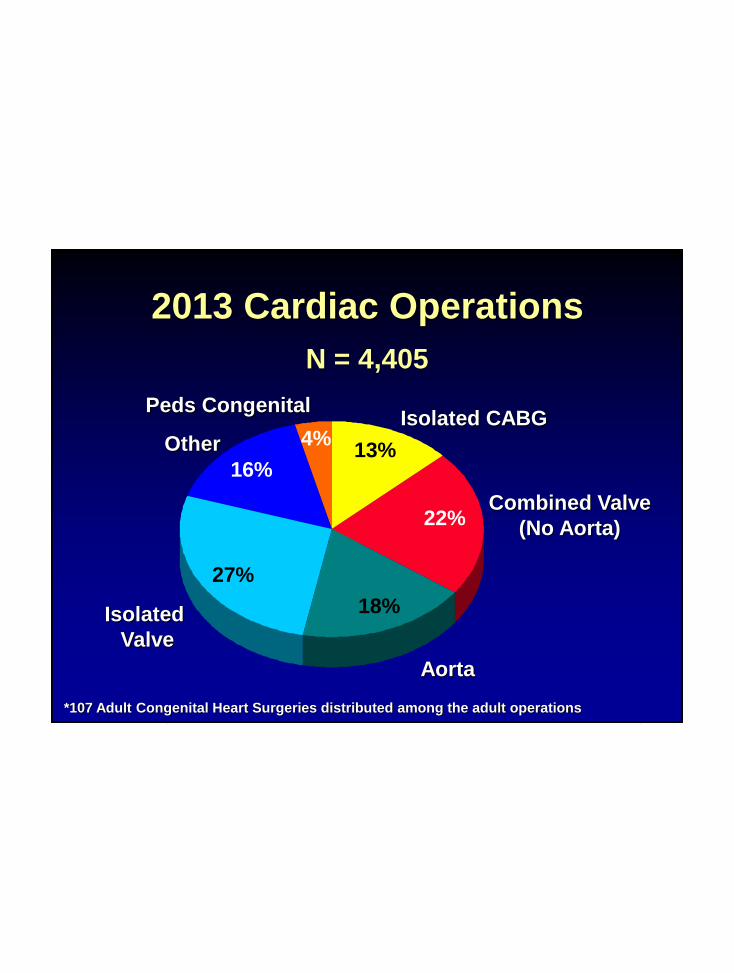
2013 Cardiac Operations
Combined Valve
(No Aorta)
Isolated
Valve
Other
Isolated CABG
Aorta
13%16%
27%
22%
N = 4,405
18%
4%
Peds Congenital
*107 Adult Congenital Heart Surgeries distributed among the adult operations

US Cardiac Surgery

Cuyahoga
County
15%
Cardiothoracic Surgery
National Volume

Cardiothoracic Surgery
National Volume
20 County
30%

Cardiothoracic Surgery
National Volume
Ohio
9%
United States
42%
Cardiothoracic Surgery
National Volume

Patients from 76 Countries Outside the US
came for their Cardiovascular Care
0
1
2
3
4
5
6
7
8
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
0.00%
2.00%
4.00%
6.00%
8.00%
1975 90 93 96 99 2
2005
2008
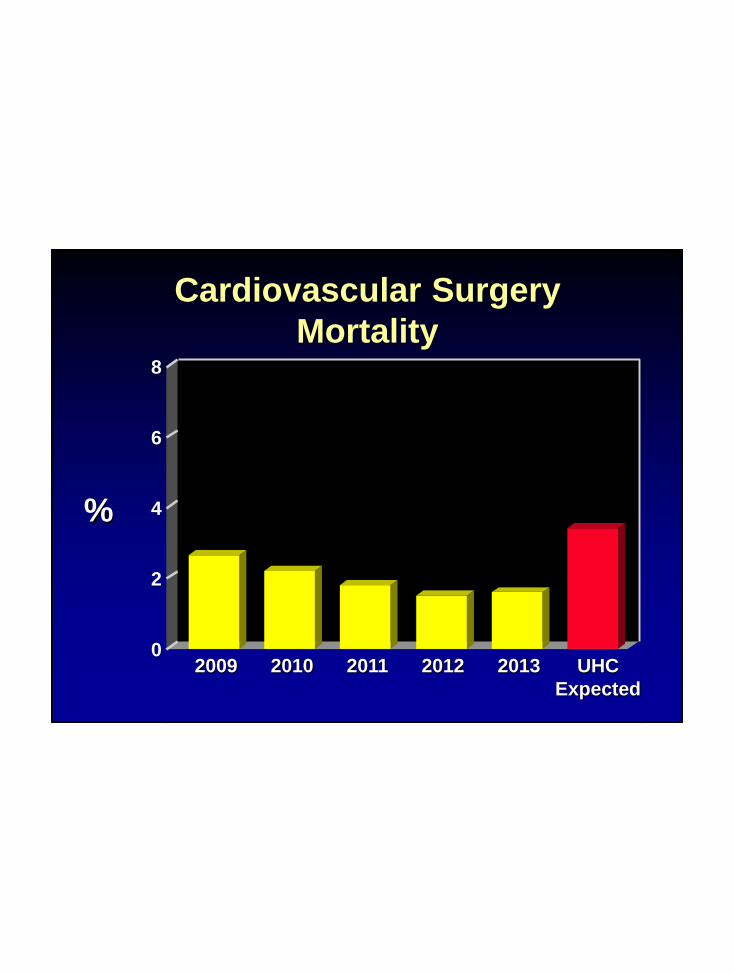
Cardiovascular Surgery
Mortality8
6
4
2
0
%
2010 2011 UHC
Expected
2009 2012 2013

3 Stars in All 3 STS Categories!
Min89.3
10th
93.150th
96.790th
97.9Max98.9
Rating
Overall
CCF
CABG
Min85.2
10th
92.250th
94.890th
96.5Max98.2
Overall
CCF
AVR
Min78.7
10th
87.850th
91.690th
94.4Max97.0
Overall
CCF
AVR + CABG

Quality:
Measure of Excellence
“We are what we repeatedly do.
Excellence, then,
is not an act, but a habit.”
Aristotle, 384-322 BC

Value is driven by provider experience,
scale, and learning at the medical
condition level
“21st century care should
be innovative.”
“Collaborative care is
essential.”
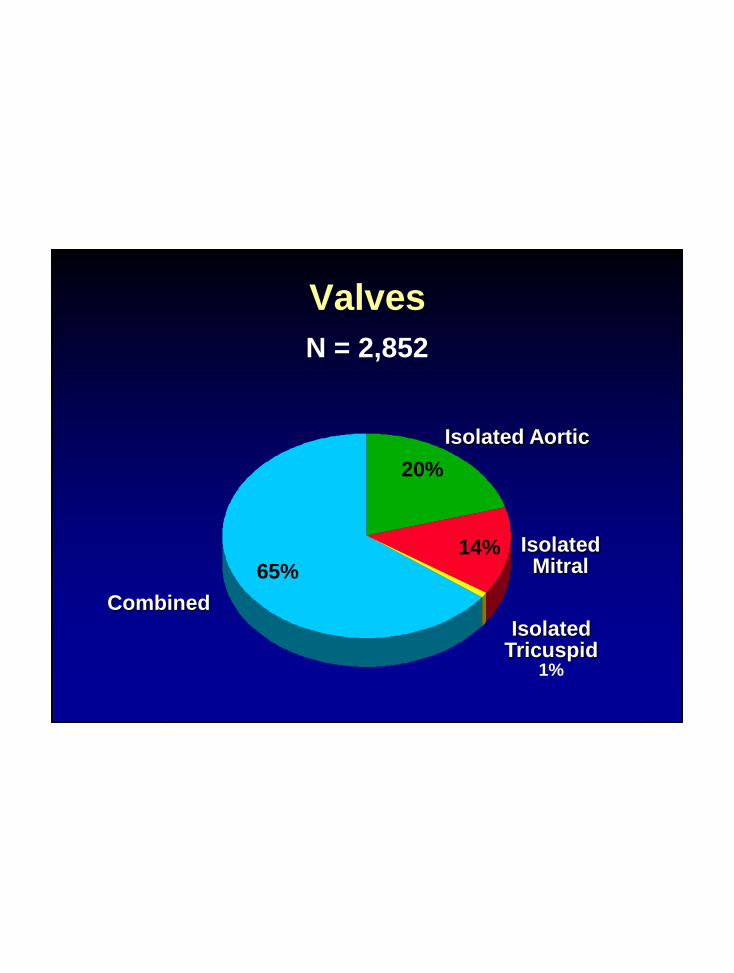
Isolated Aortic
Isolated Tricuspid
1%
IsolatedMitral
14%
20%
Valves
N = 2,852
65%
Combined
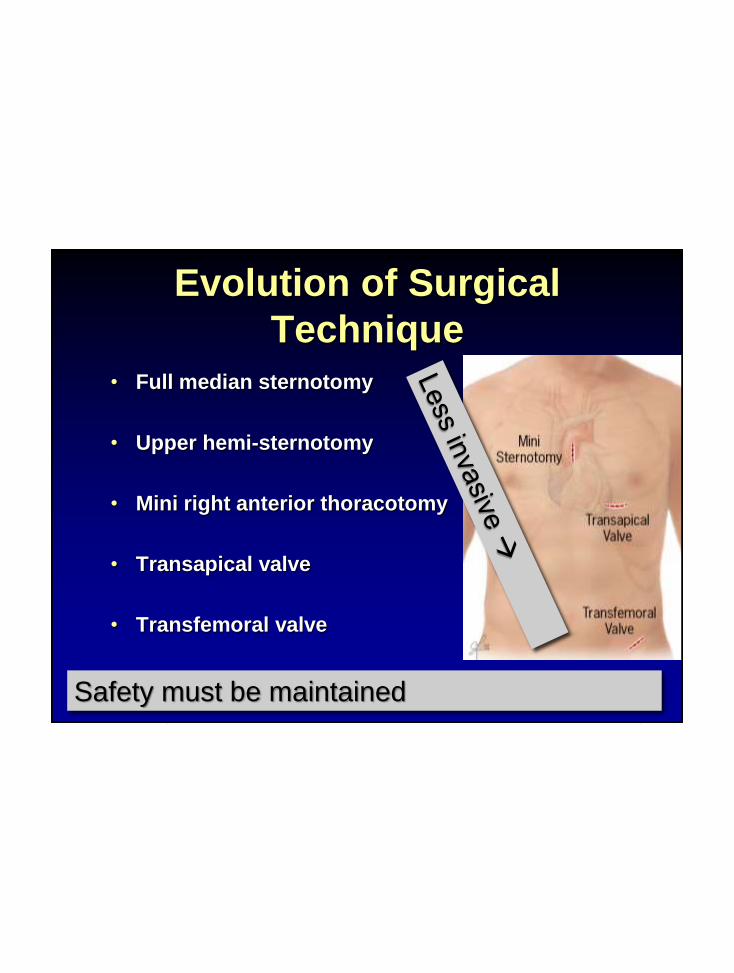
Evolution of Surgical
Technique
• Full median sternotomy
• Upper hemi-sternotomy
• Mini right anterior thoracotomy
• Transapical valve
• Transfemoral valve
Safety must be maintained

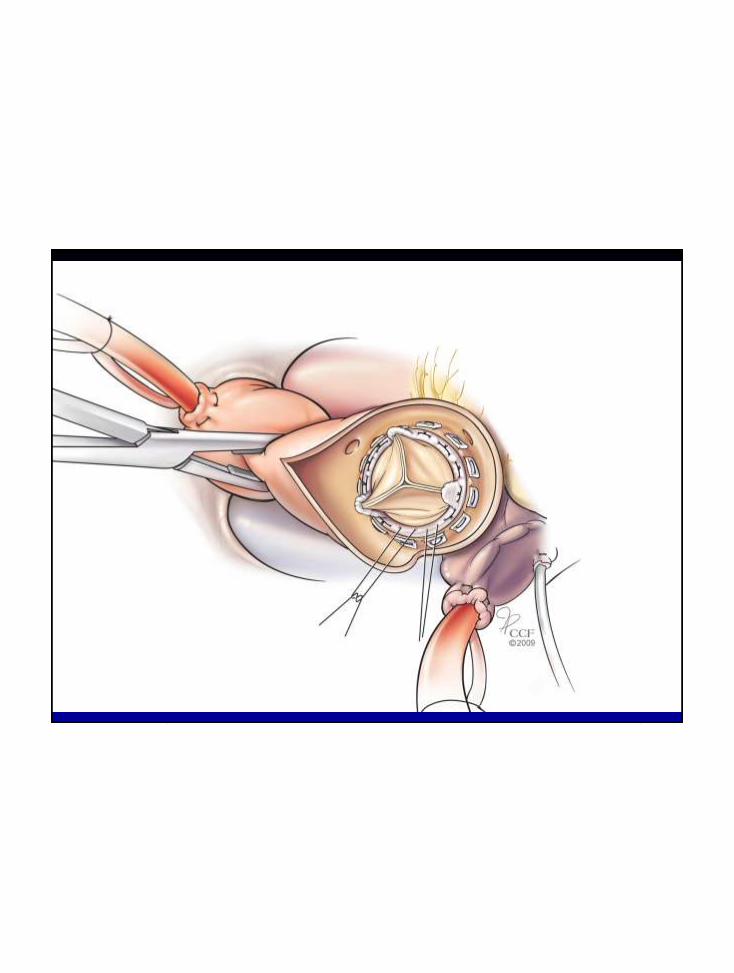
Operative Approach – Isolated Valve
Transcatheter
Placement
Full
Conventional
Sternotomy
N = 960
32%
27% Mini
Sternotomy
10%19%
Mini
Thoracotomy
Robotic12%


Robotically-assisted Cardiac Surgery l November 3, 2014 l 19
Median
SternotomyMini
Thoracotomy
Totally
Endoscopic
Robotic
>450 procedures >150 procedures >150 procedures

Robotically-assisted Cardiac Surgery l November 3, 2014 l 20
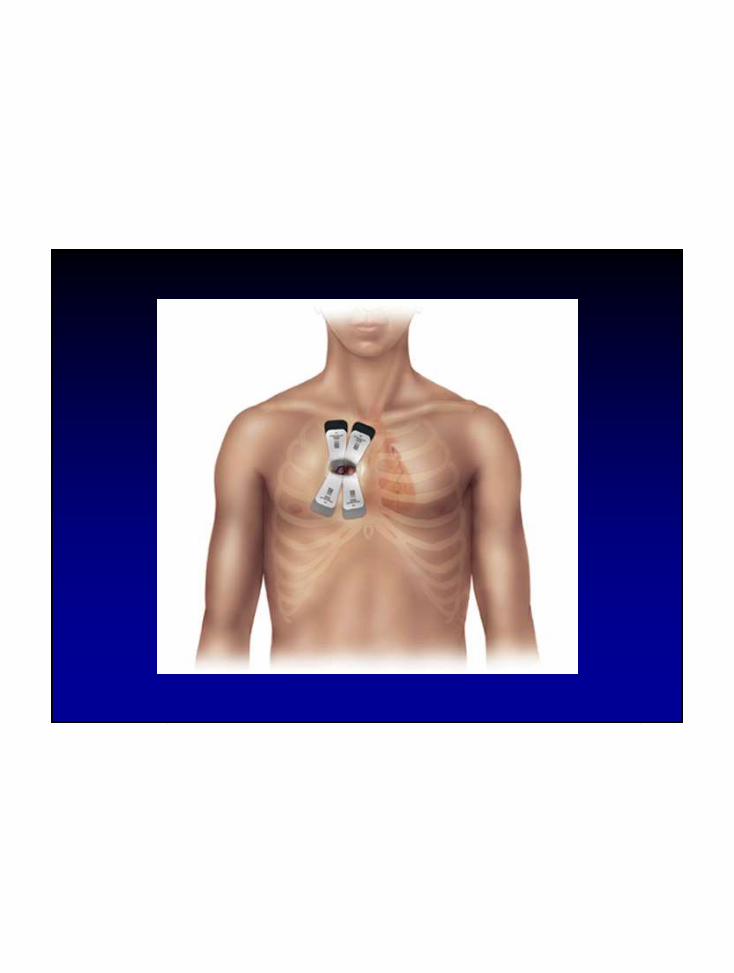
4th intercostal
space is ideal
Camera
Port
Service
Port

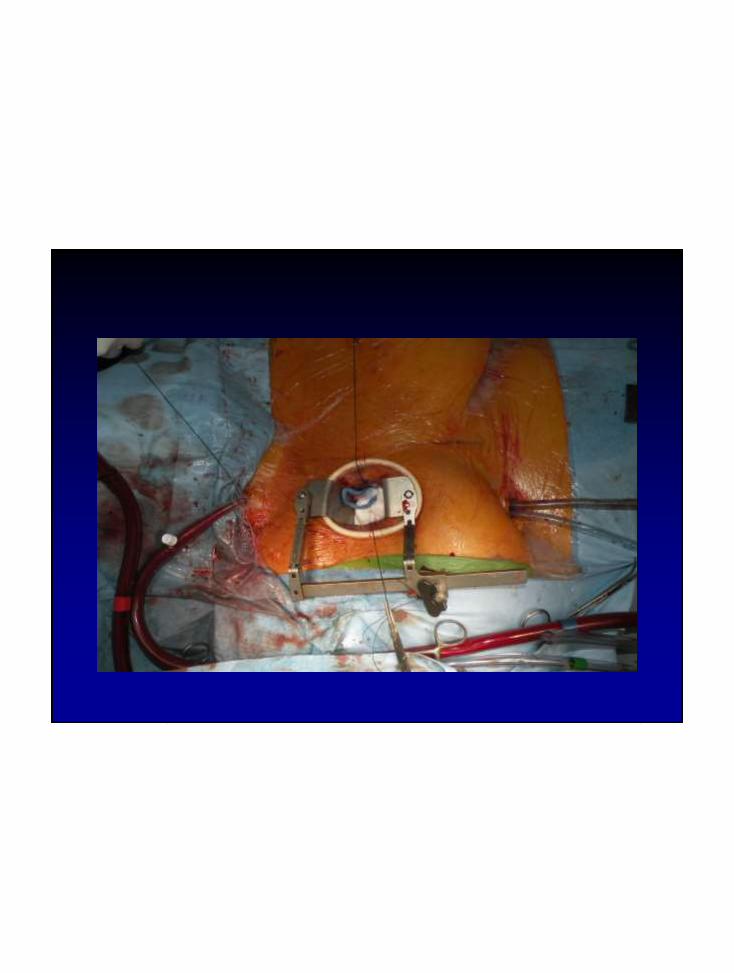
Robotically-assisted Cardiac Surgery l November 3, 2014 l 21
SERVICE
PORT

Robotically-assisted Cardiac Surgery l November 3, 2014 l 22




Isolated Mitral Valve Mortality
%
6
4
2
00%.3%
STS Expected
STS Expected
ReplaceRepair*
*2013 only
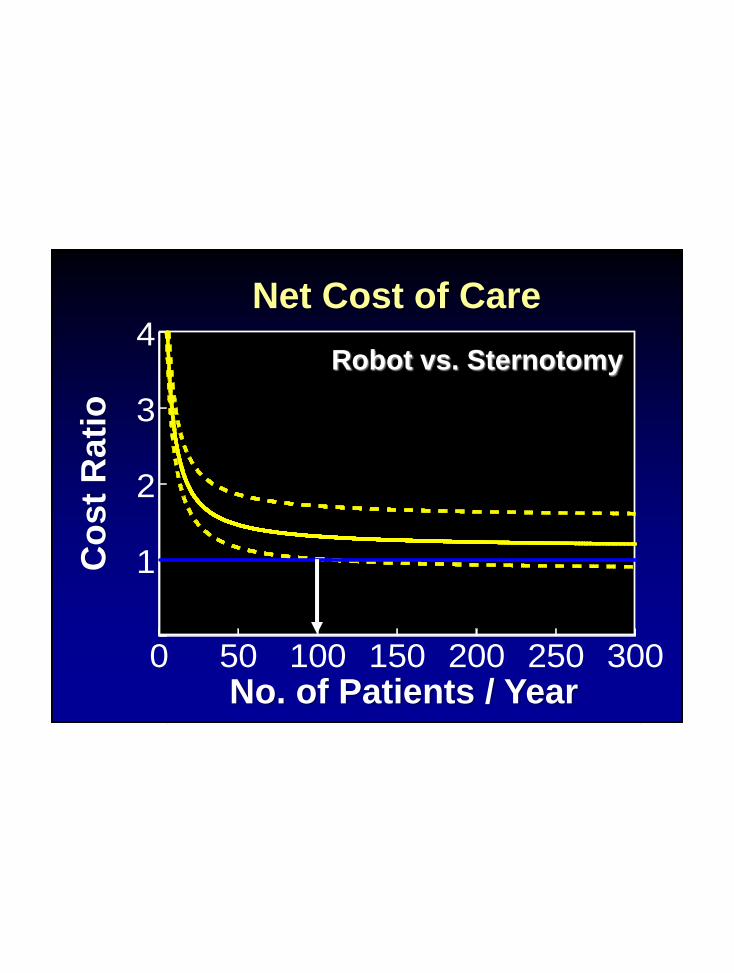
1
2
3
4
0 50 100 150 200 250 300
Net Cost of Care
Co
st
Ra
tio
No. of Patients / Year
Robot vs. Sternotomy

AVR Volume Trend
400
#
300
200
02009 2012 20132010 2011
100
Primary
Reoperation
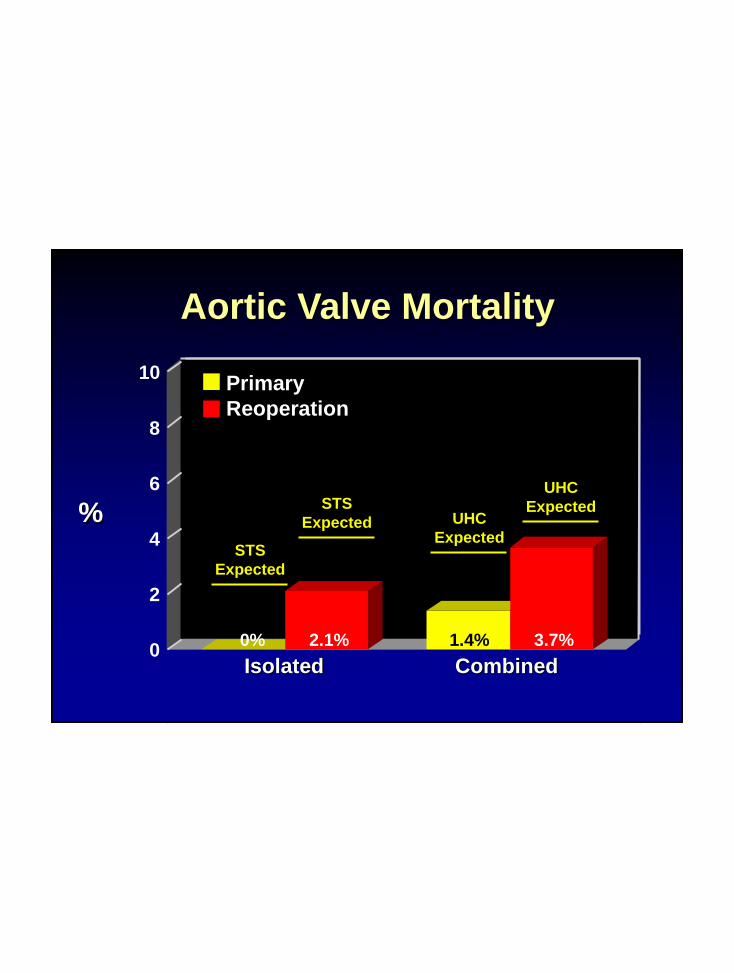
Aortic Valve Mortality
Isolated Combined
Primary
Reoperation
0% 2.1% 1.4% 3.7%
STS
Expected
%
10
6
4
0
2
8
STS
Expected UHC
Expected
UHC
Expected



Works well in larger patients
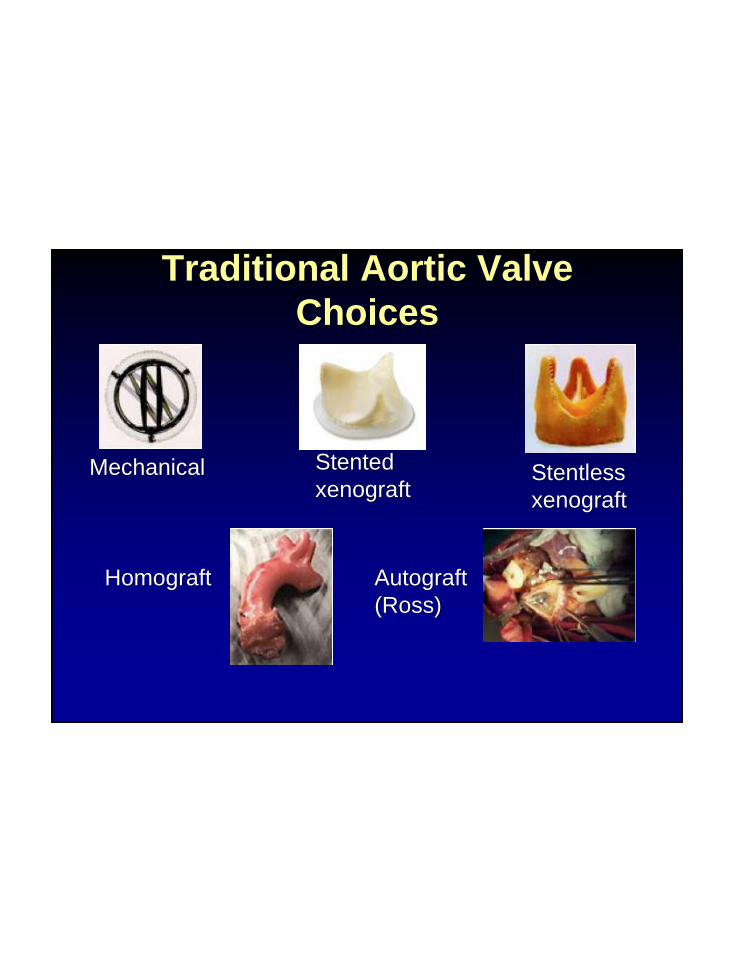
Traditional Aortic Valve
Choices
Mechanical Stented
xenograftStentless
xenograft
Homograft Autograft
(Ross)
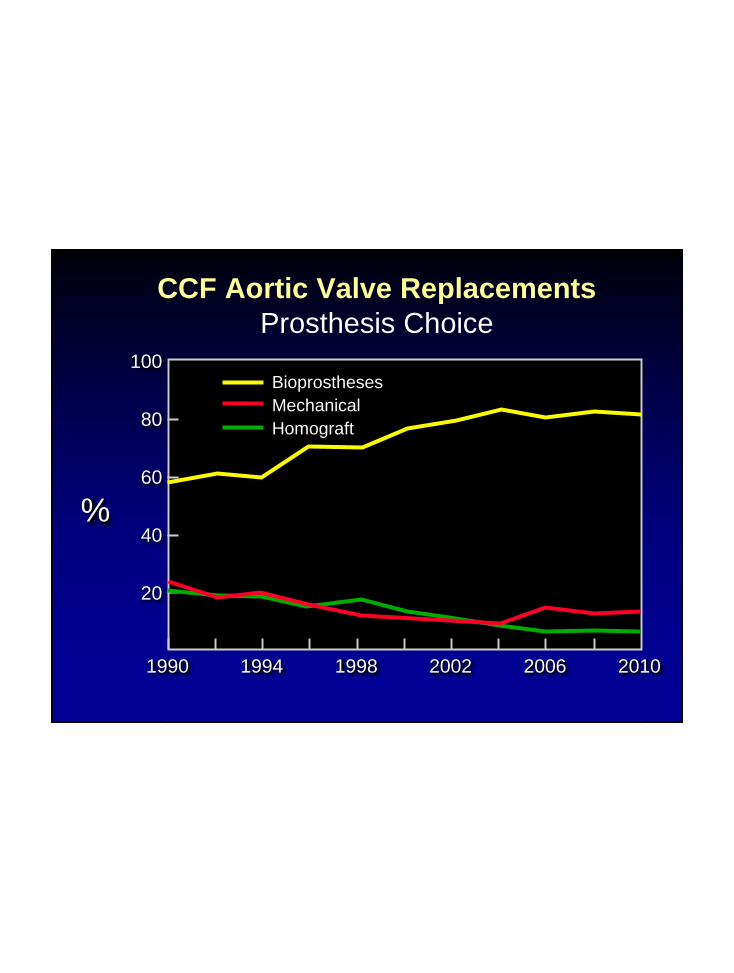
0
20
40
60
80
100
2001 2002 2003 2004 2005 2006
Bioprostheses
Mechanical
Homograft
100
80
60
40
20
CCF Aortic Valve Replacements
Prosthesis Choice
%
1994 1998 20102002 20061990
Long Term Valve Outcomes
12,569 Perimount (CE) implants
1981-2011
30 yrs of data

3
6
9
12
15
40 50 60 70 80 90
Risk of Explant for SVD
Age (years)
%
Actual Risk within 20 years

New Valves

TAVR
Edwards - S3
Direct Flow - Salus
St Jude’s - Portico
Boston Scientific
- Sadra
Medtronic - CoreValve
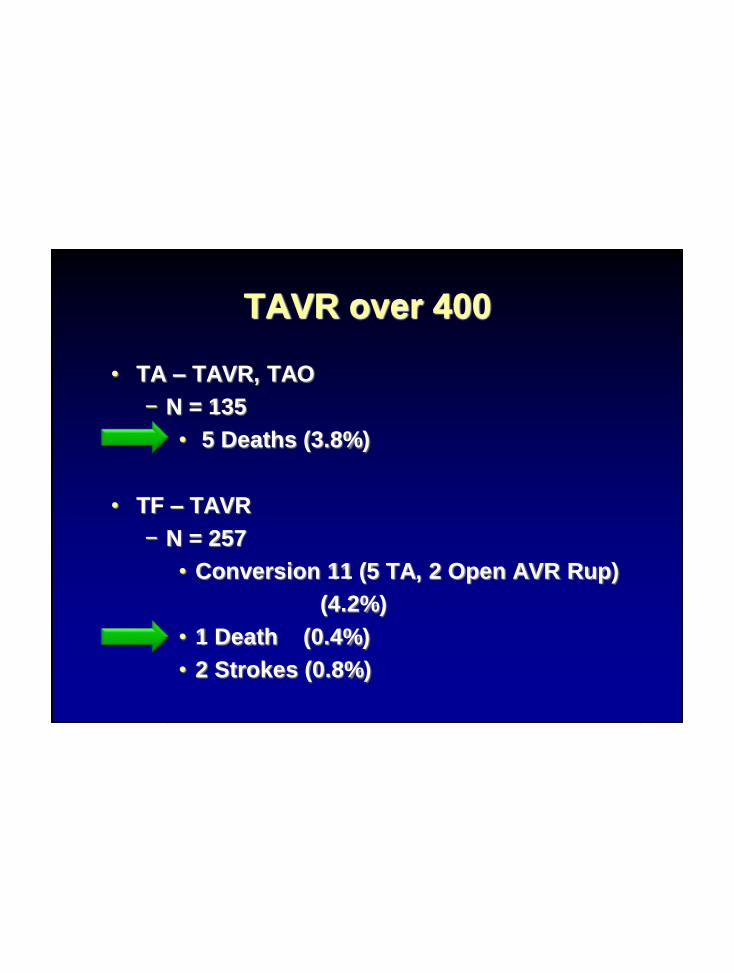
TAVR over 400
• TA – TAVR, TAO
− N = 135
• 5 Deaths (3.8%)
• TF – TAVR
− N = 257
• Conversion 11 (5 TA, 2 Open AVR Rup)
(4.2%)
• 1 Death (0.4%)
• 2 Strokes (0.8%)


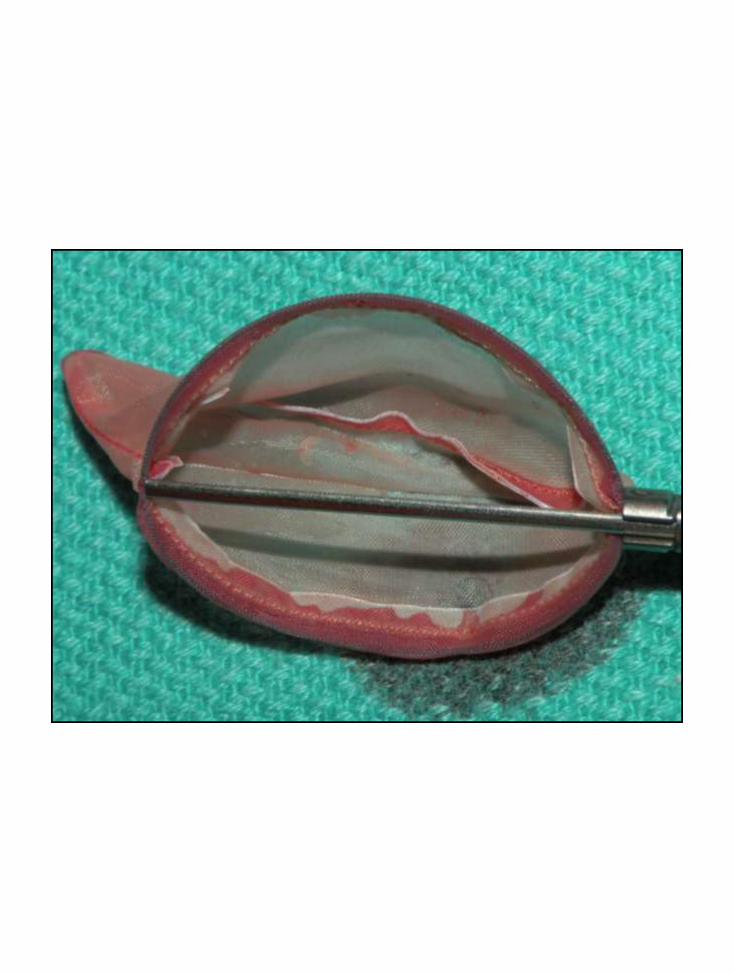
TAO Insertion

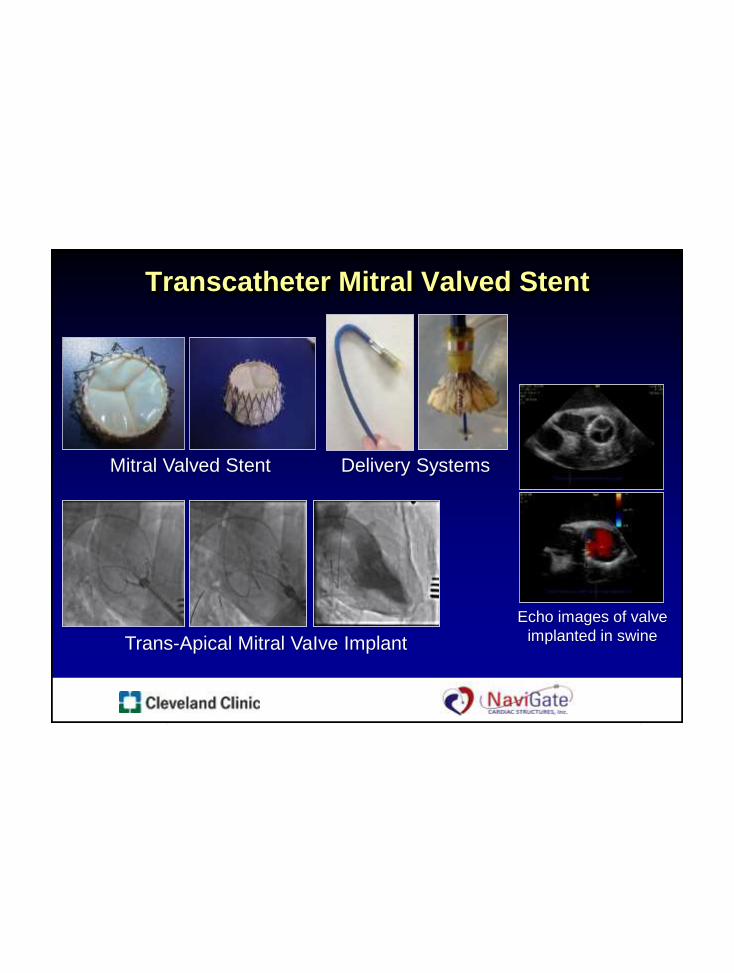
Transcatheter Mitral Valved Stent
Trans-Apical Mitral VaIve Implant
Delivery Systems
Echo images of valve
implanted in swine
Mitral Valved Stent

New Cleveland Clinic Valve Treatment
(GLX)
GLX Valve
Commence Trial

Univ of Maryland
St. Vincent’s Hosp – Indiana
Univ of Florida at Shands
Columbia University
Cleveland Clinic
Spectrum Health
Baylor St. Luke’s Houston
Univ of S. California
Emory Univ Hospital
Mt Sinai Medical Center
Univ of Kansas Med Ctr
0 5 10 15 20 25 30 35 40
CCF Valve Exchange Vitality45 Patients, European CE Label
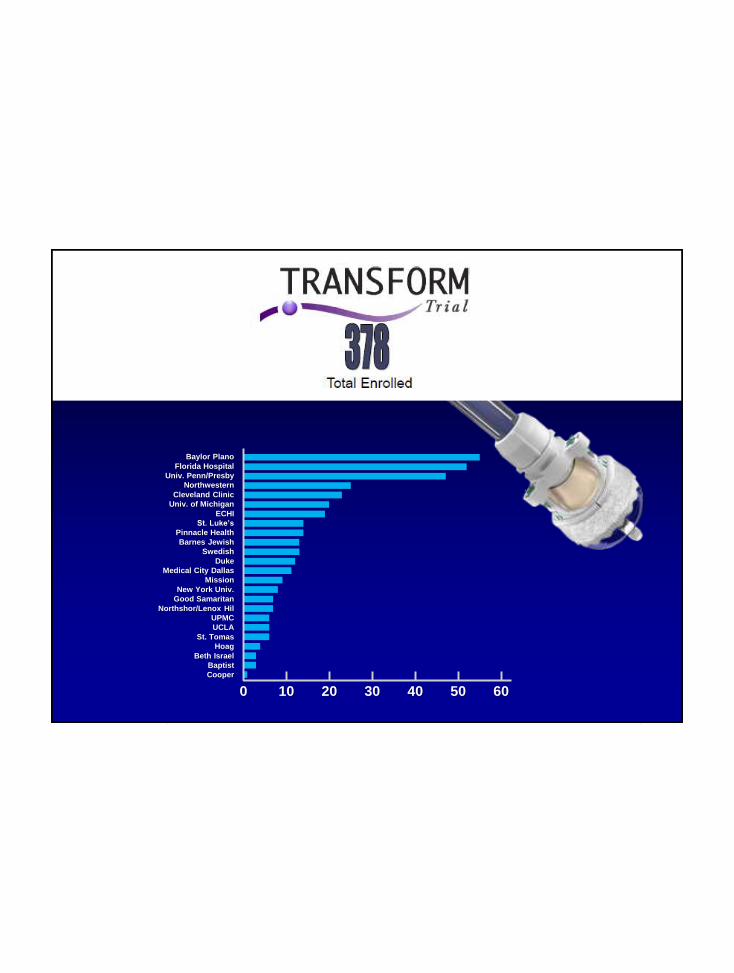
Baylor Plano
Florida Hospital
Univ. Penn/Presby
Northwestern
Cleveland Clinic
Univ. of Michigan
ECHI
St. Luke’s
Pinnacle Health
Barnes Jewish
Swedish
Duke
Medical City Dallas
Mission
New York Univ.
Good Samaritan
Northshor/Lenox Hil
UPMC
UCLA
St. Tomas
Hoag
Beth Israel
Baptist
Cooper
0 10 20 30 40 50 60
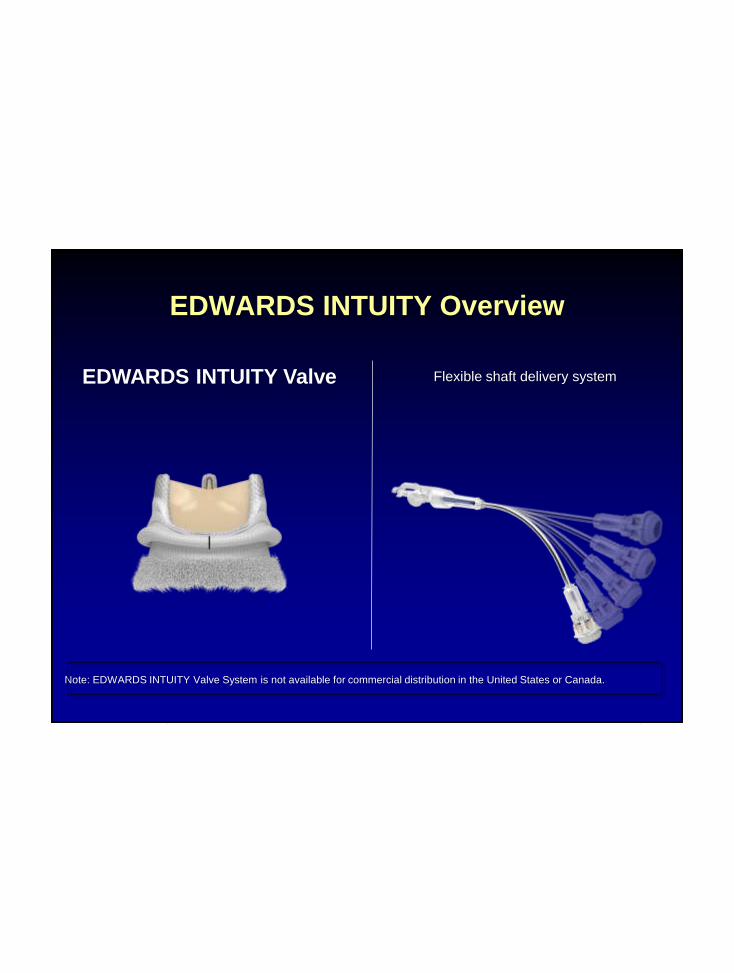
EDWARDS INTUITY Overview
EDWARDS INTUITY Valve Flexible shaft delivery system
Note: EDWARDS INTUITY Valve System is not available for commercial distribution in the United States or Canada.

Note: EDWARDS INTUITY Valve System is not available for commercial distribution in the United States or Canada.
Procedure Overview
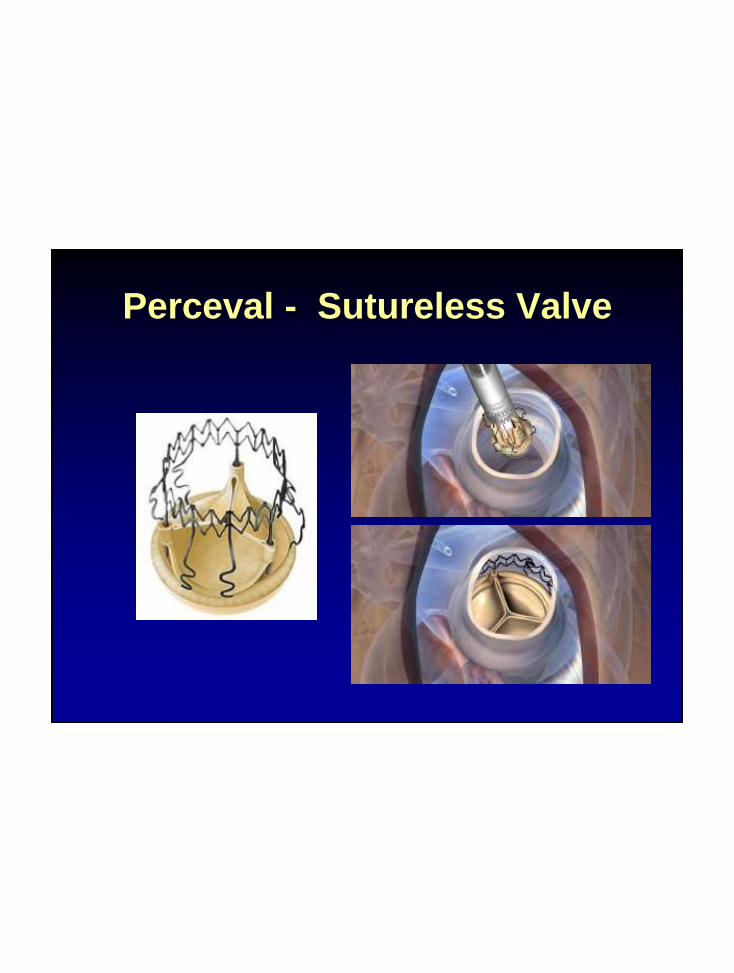
Perceval - Sutureless Valve
Prediction: In 10 Years:
• Percutaneous Valves, ASDs, Aortas,
PCI
− Outpatients
− Echo
− Local Anesthetic
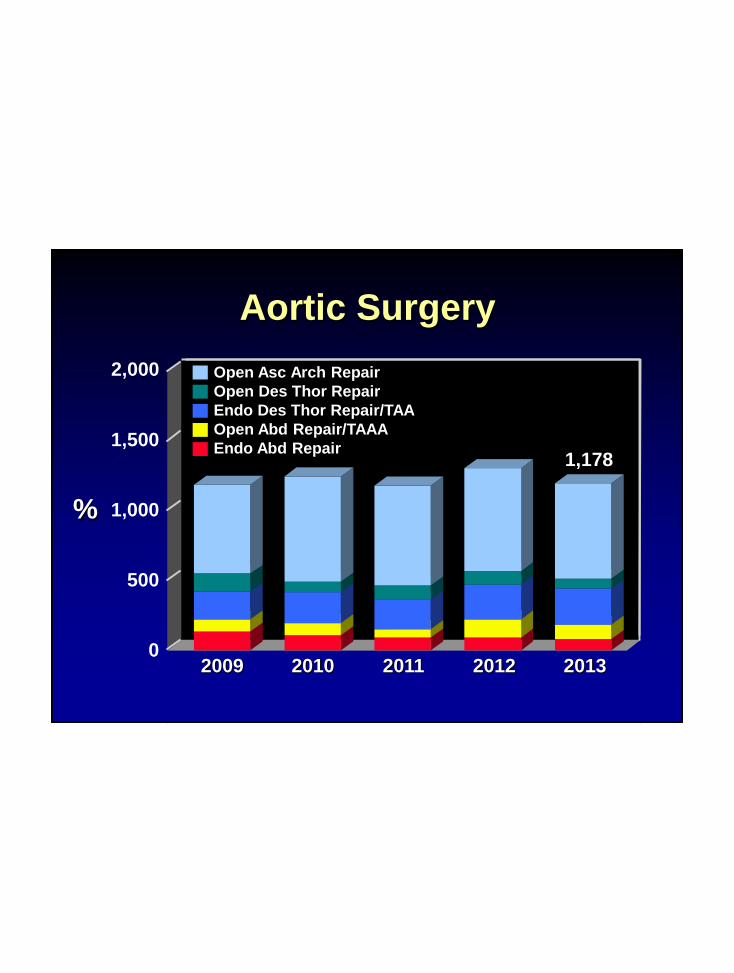
Aortic Surgery
%
2,000
1,000
500
0
Open Asc Arch Repair
Open Des Thor Repair
Endo Des Thor Repair/TAA
Open Abd Repair/TAAA
Endo Abd Repair
2010 2011 20122009 2013
1,5001,178
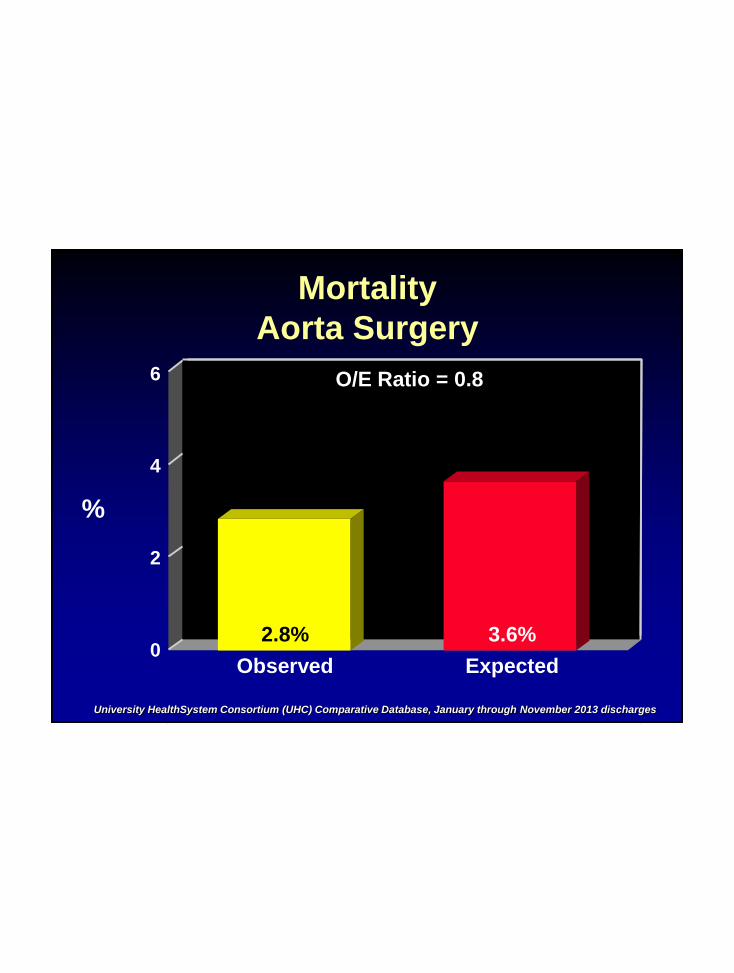
6
Mortality
Aorta Surgery
%
Observed
4
2
0Expected
University HealthSystem Consortium (UHC) Comparative Database, January through November 2013 discharges
O/E Ratio = 0.8
2.8% 3.6%


Descending Thoracic Endovascular
Repairs: Proven Technology

Current Device Choices
Gore
Cook
Medtronic
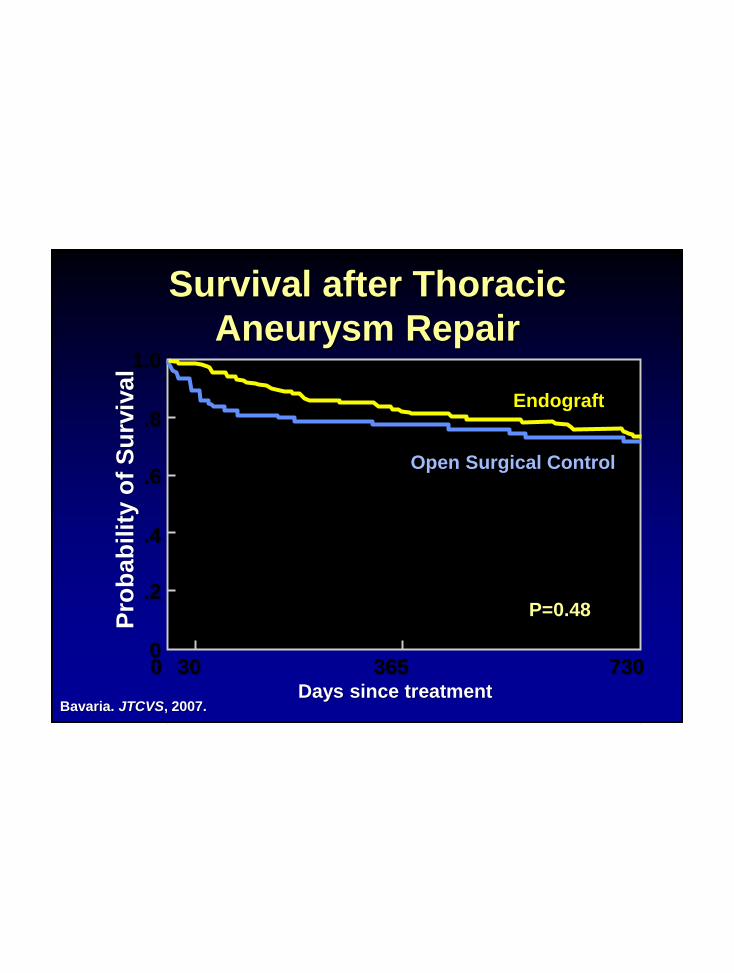
Survival after Thoracic
Aneurysm Repair
365 730300
1.0
.8
.6
.4
.2
0
Open Surgical Control
Endograft
P=0.48
Days since treatment
Pro
ba
bilit
y o
f S
urv
ival
Bavaria. JTCVS, 2007.
The New Frontier:
Thoracoabdominal Aortic
Aneurysms
Acute Mortality: 7.4 –17%
• Older Age
• Co-morbid conditions
− COPD
− CRI
− CAD
− Frail
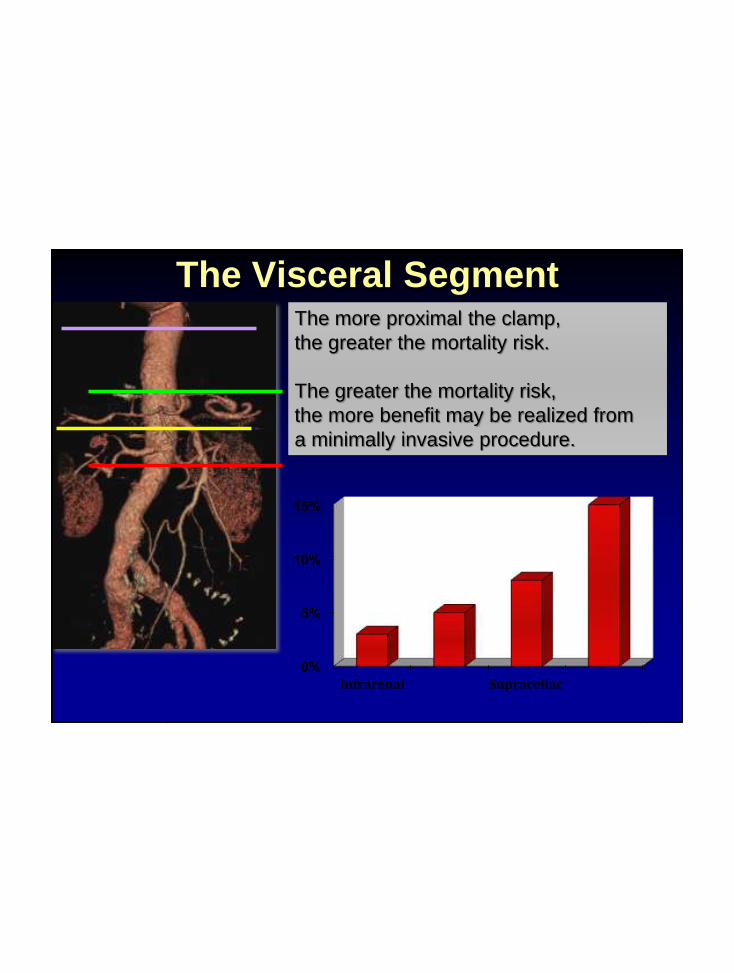
The Visceral Segment
0%
5%
10%
15%
Infrarenal Supraceliac
The more proximal the clamp,
the greater the mortality risk.
The greater the mortality risk,
the more benefit may be realized from
a minimally invasive procedure.

Thoracoabdominal Aneurysms

Standard Repair
Circa 1999
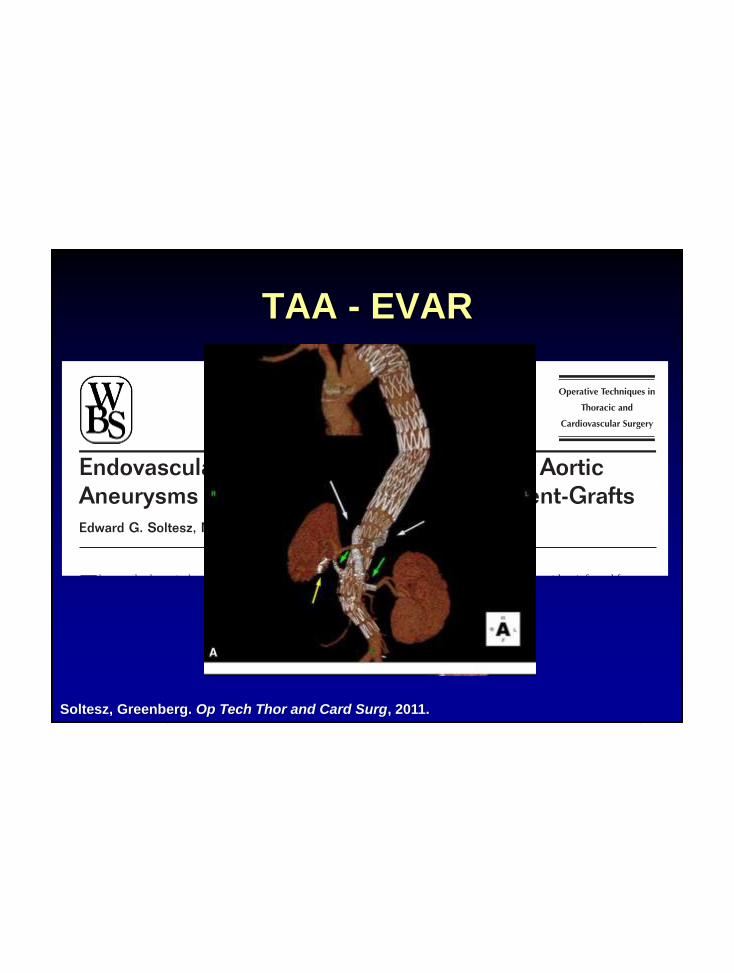
TAA - EVAR
Soltesz, Greenberg. Op Tech Thor and Card Surg, 2011.
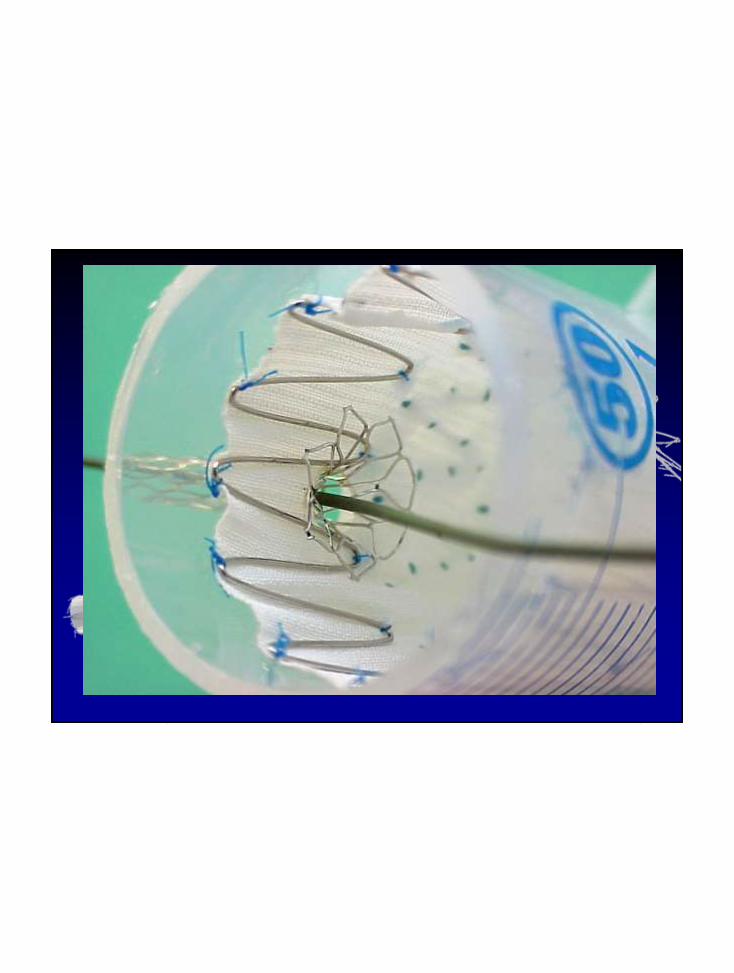

Device Construct
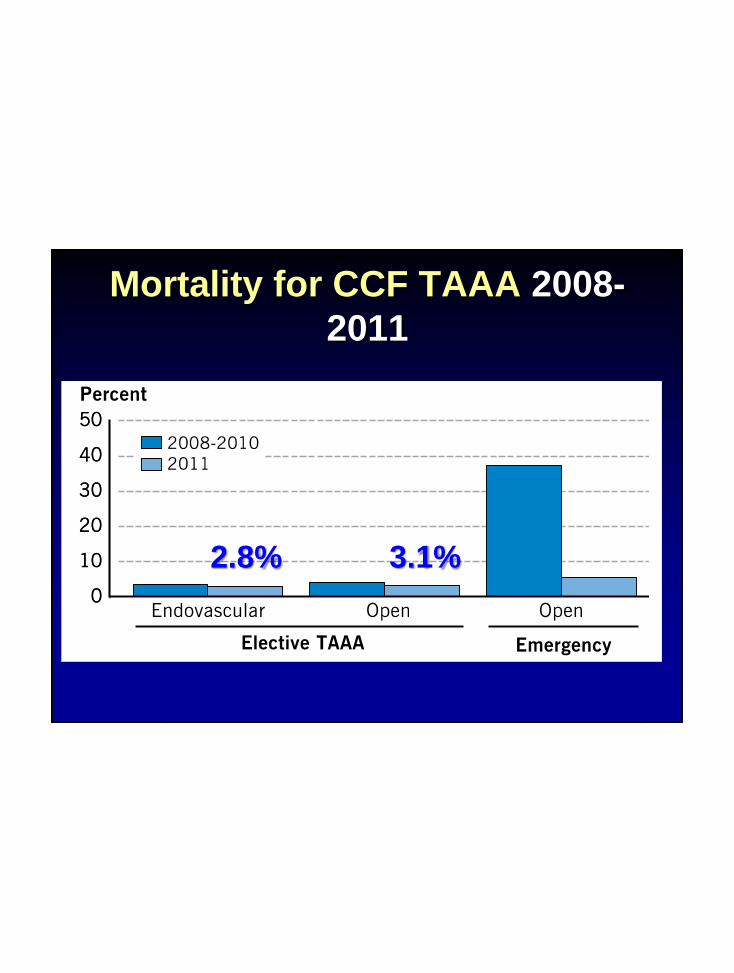
Mortality for CCF TAAA 2008-
2011
2.8% 3.1%

Disasters occur when Hazards
meet Vulnerability
Cardiogenic shock

Progress
1980
Now
Left to die
Survival improving
with prompt therapy and
newer devices

Emergency Circulatory Support
ECMO
Tandem HeartImpella

Emergency Circulatory Support
ECMO
Tandem HeartImpella
ECMO

• Blood pump
• Rotaflow centrifugal pump
• Low cost, small size
• 0-10 L/min
• Oxygenator
• Quadrox D
• Minimal plasma leak
• Long-lasting
ECMOCleveland Clinic Experience
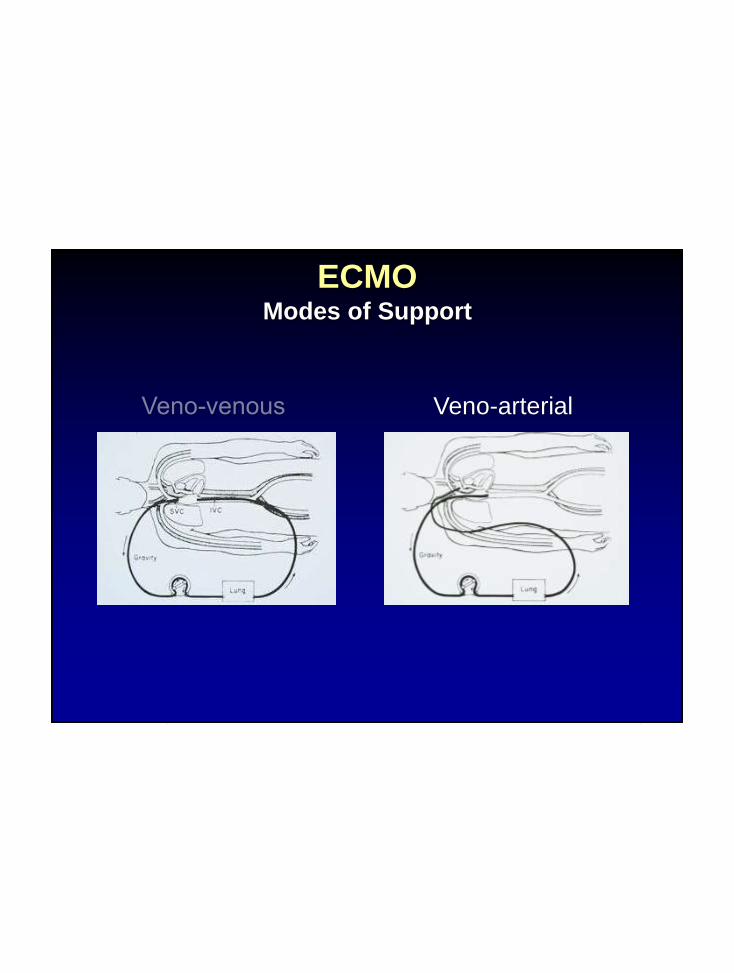
ECMOModes of Support
Veno-arterial
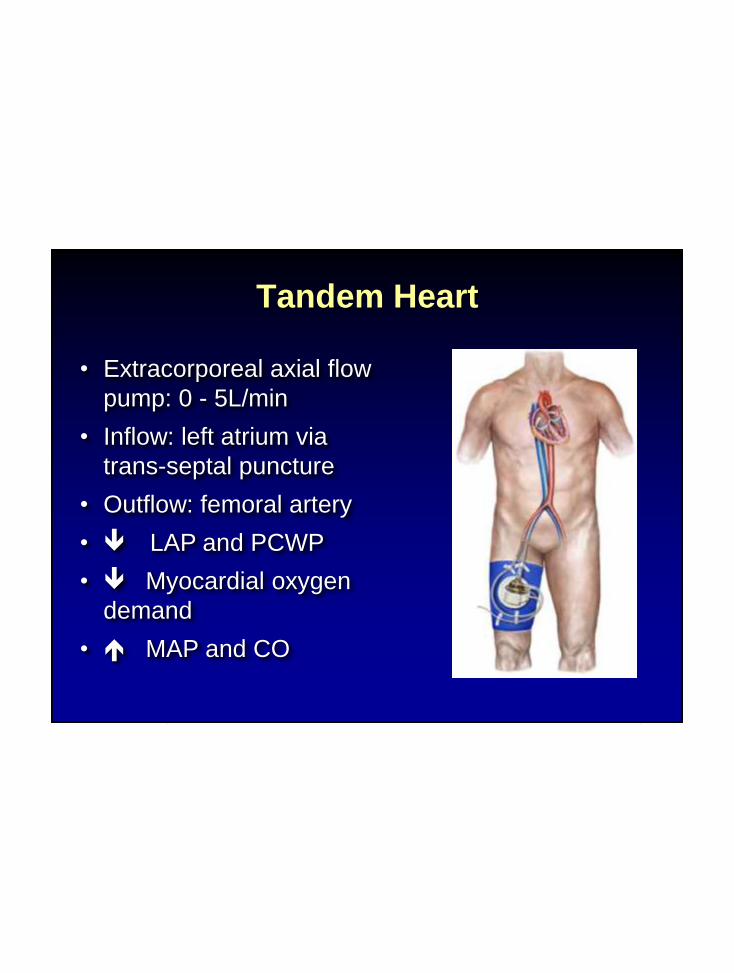
• Extracorporeal axial flow
pump: 0 - 5L/min
• Inflow: left atrium via
trans-septal puncture
• Outflow: femoral artery
• LAP and PCWP
• Myocardial oxygen
demand
• MAP and CO
Tandem Heart

Tandem Heart
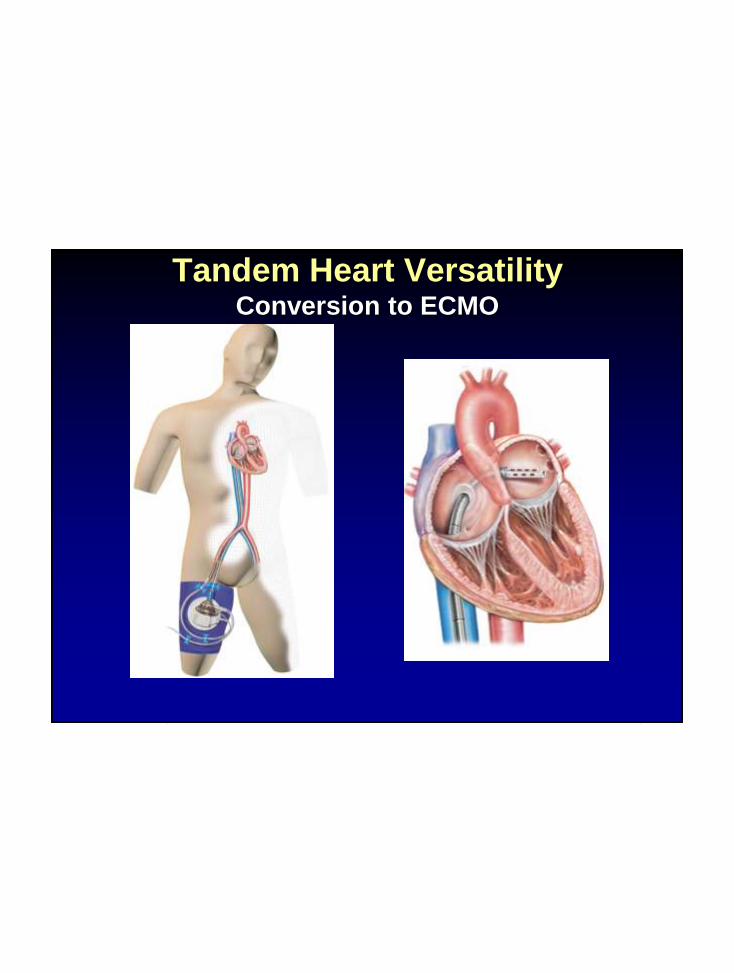
Tandem Heart VersatilityConversion to ECMO

Tandem Heart VersatilityConversion to ECMO
EZ Tandem EZ Tandem with Transseptal
TH-021
1
2
3
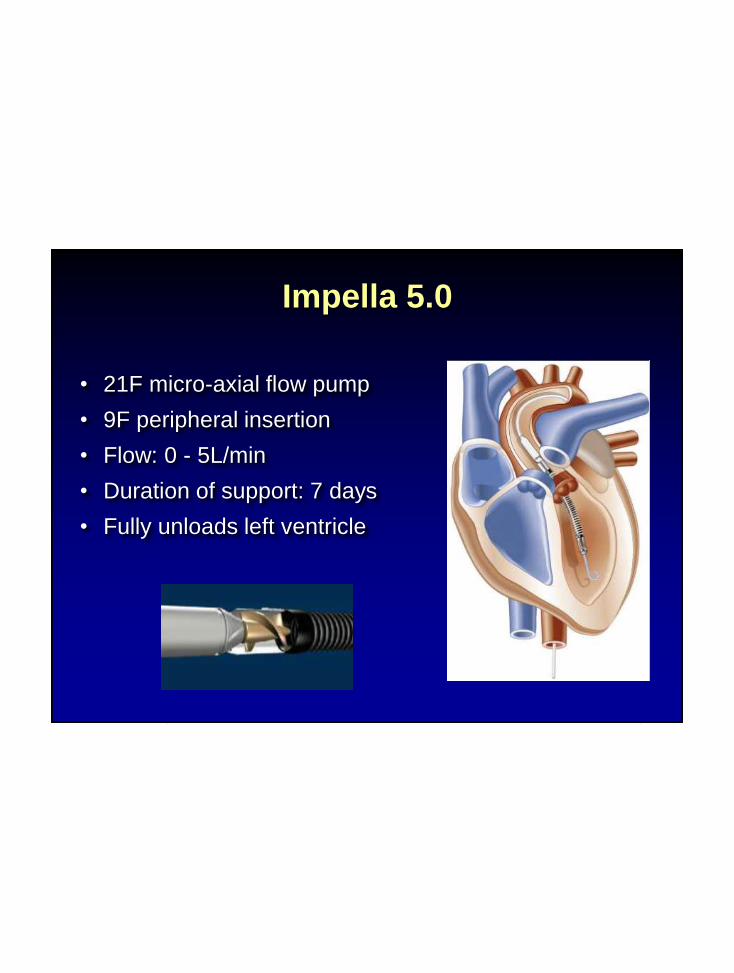
• 21F micro-axial flow pump
• 9F peripheral insertion
• Flow: 0 - 5L/min
• Duration of support: 7 days
• Fully unloads left ventricle
Impella 5.0
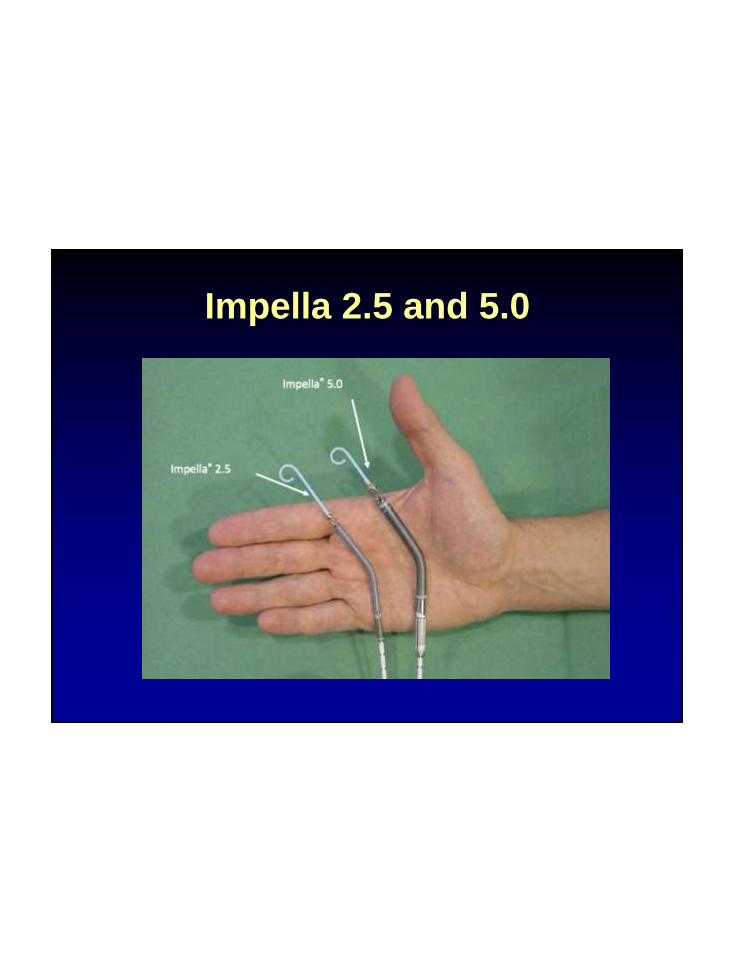
Impella 2.5 and 5.0

Impella Positioning
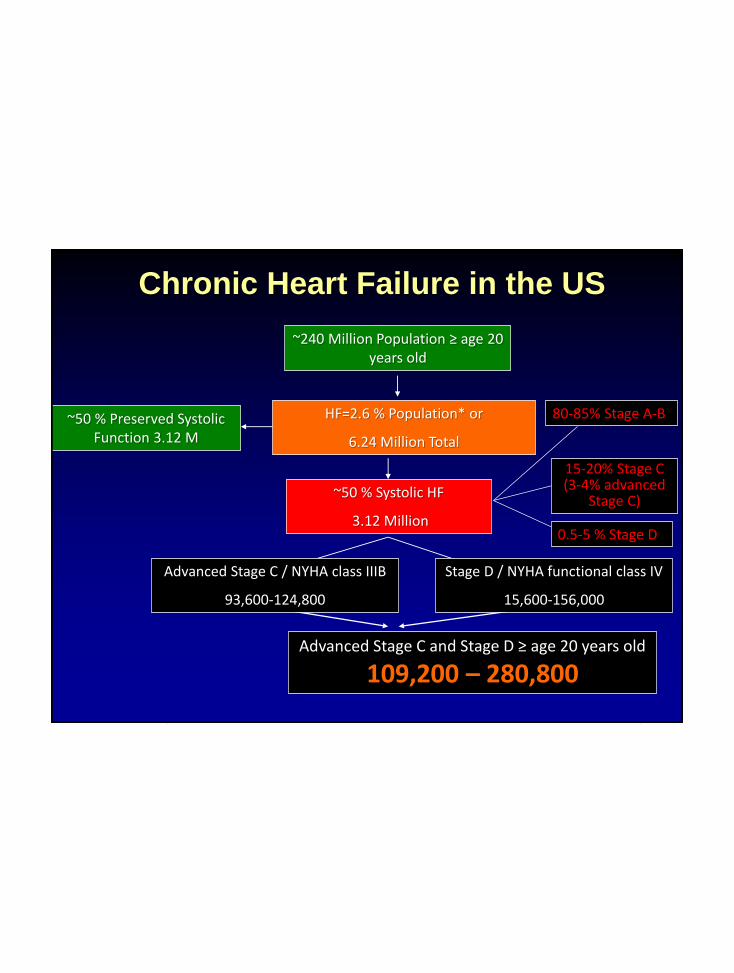
~240 Million Population ≥ age 20 years old
HF=2.6 % Population* or
6.24 Million Total
~50 % Preserved Systolic Function 3.12 M
~50 % Systolic HF
3.12 Million
Advanced Stage C and Stage D ≥ age 20 years old
109,200 – 280,800
Advanced Stage C / NYHA class IIIB
93,600-124,800
80-85% Stage A-B
0.5-5 % Stage D
Stage D / NYHA functional class IV
15,600-156,000
15-20% Stage C (3-4% advanced
Stage C)
Chronic Heart Failure in the US
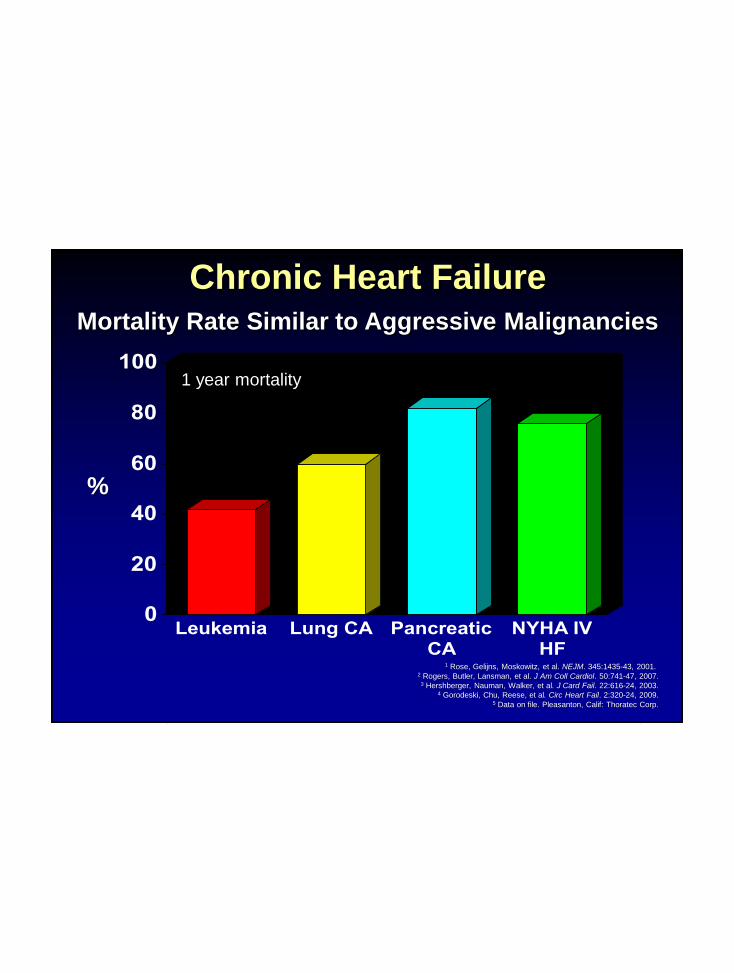
0
20
40
60
80
100
Leukemia Lung CA PancreaticCA
NYHA IVHF
%
1 year mortality
Chronic Heart FailureMortality Rate Similar to Aggressive Malignancies
1 Rose, Gelijns, Moskowitz, et al. NEJM. 345:1435-43, 2001. 2 Rogers, Butler, Lansman, et al. J Am Coll Cardiol. 50:741-47, 2007.
3 Hershberger, Nauman, Walker, et al. J Card Fail. 22:616-24, 2003.4 Gorodeski, Chu, Reese, et al. Circ Heart Fail. 2:320-24, 2009.
5 Data on file. Pleasanton, Calif: Thoratec Corp.
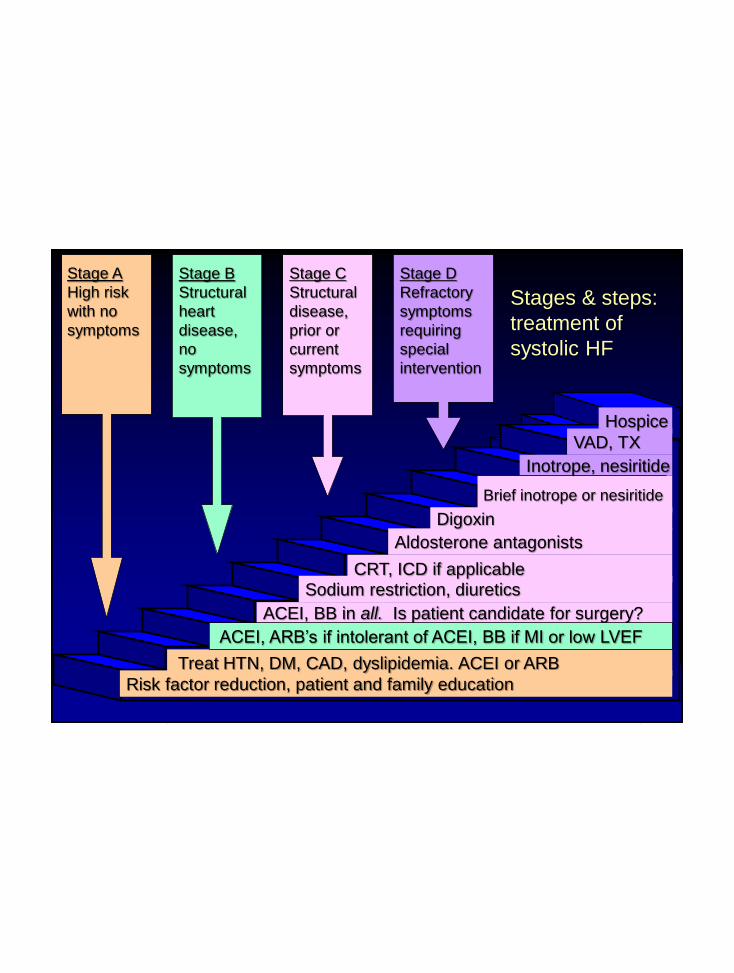
Risk factor reduction, patient and family education
Treat HTN, DM, CAD, dyslipidemia. ACEI or ARB
ACEI, BB in all. Is patient candidate for surgery?
Sodium restriction, diuretics
Aldosterone antagonists
Digoxin
Inotrope, nesiritide
VAD, TX
Stage A
High risk
with no
symptoms
CRT, ICD if applicable
Stage B
Structural
heart
disease,
no
symptoms
Stage C
Structural
disease,
prior or
current
symptoms
Stage D
Refractory
symptoms
requiring
special
intervention
Stages & steps:
treatment of
systolic HF
Hospice
Brief inotrope or nesiritide
ACEI, ARB’s if intolerant of ACEI, BB if MI or low LVEF
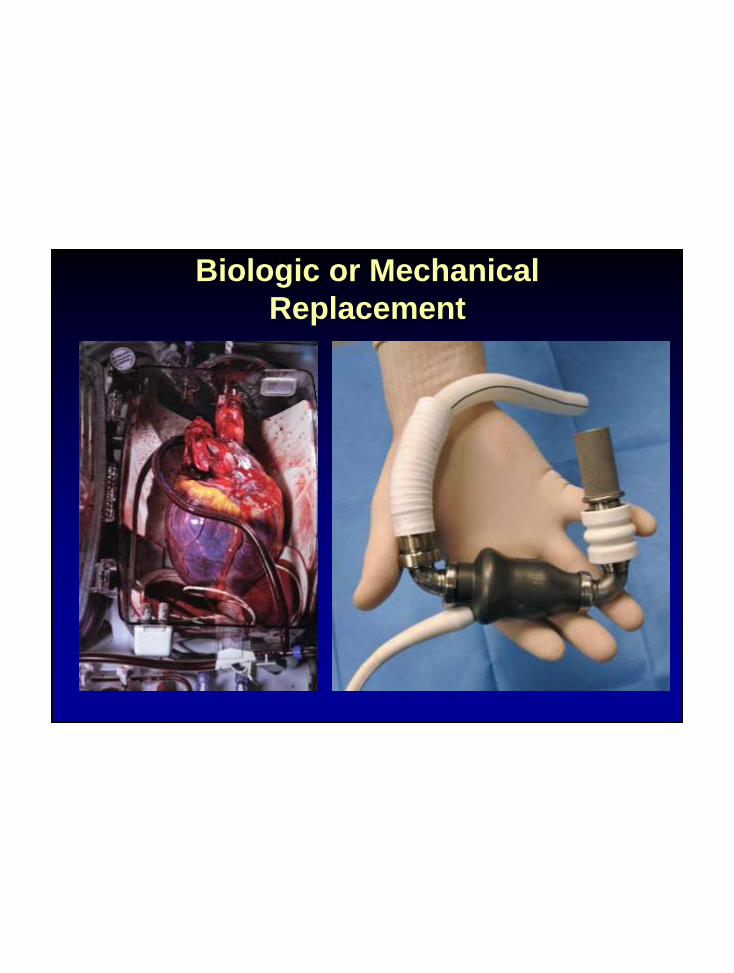
Biologic or Mechanical
Replacement

“Proposing heart transplantation to cure heart
failure is analogous to proposing the lottery to
cure poverty.” LW Stevenson, MD
“Cardiac transplantation is ‘epidemiologically trivial’ solution.”
Eric Rose, MD
5/4/2014 – 3,972 awaiting heart transplantation
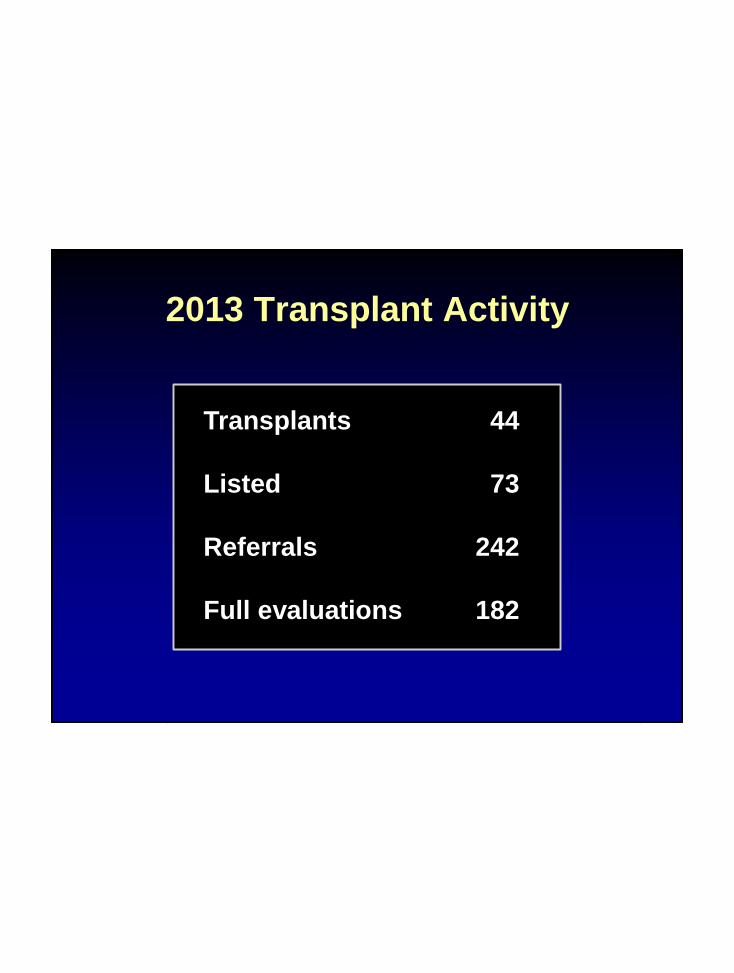
2013 Transplant Activity
Transplants 44
Listed 73
Referrals 242
Full evaluations 182
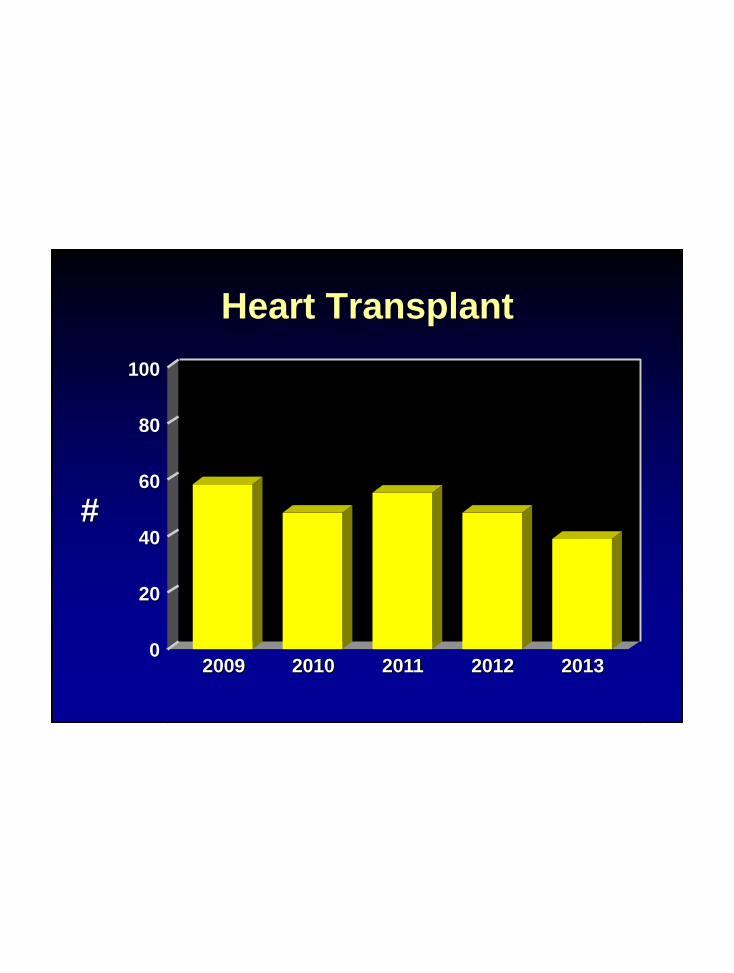
Heart Transplant
#
100
80
60
40
0
20
2009 2010 2011 2012 2013
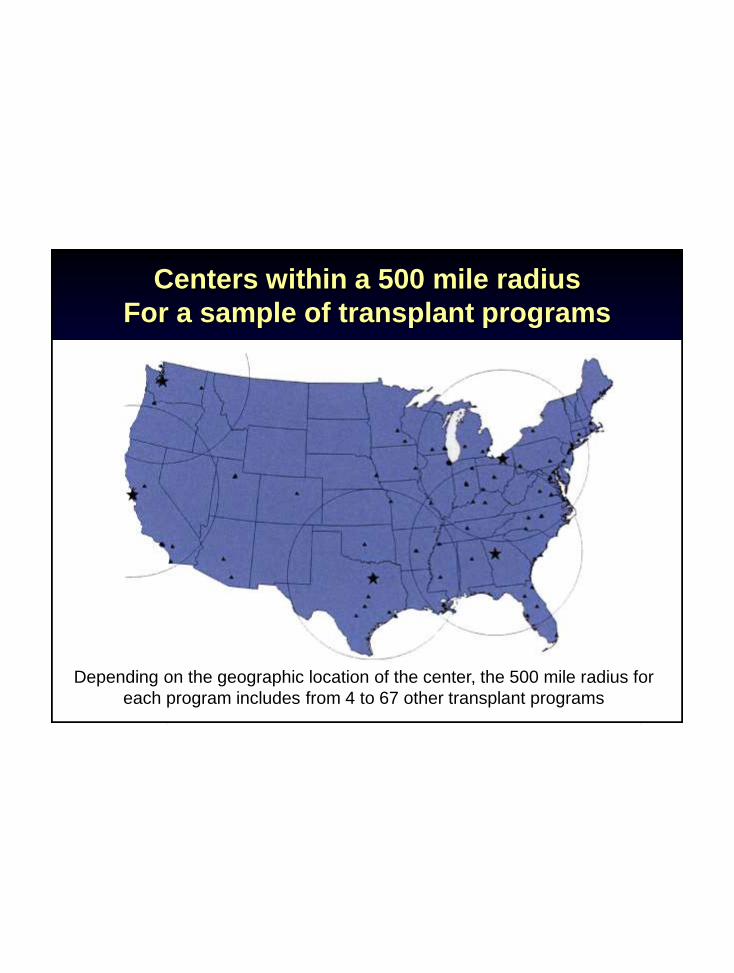
Centers within a 500 mile radius
For a sample of transplant programs
Depending on the geographic location of the center, the 500 mile radius for
each program includes from 4 to 67 other transplant programs

Number of Candidates Ever Actively
Waiting (2010-2012)
Each symbol represents one transplant center, with the size of the
symbol proportional to the number of centers within 500 miles
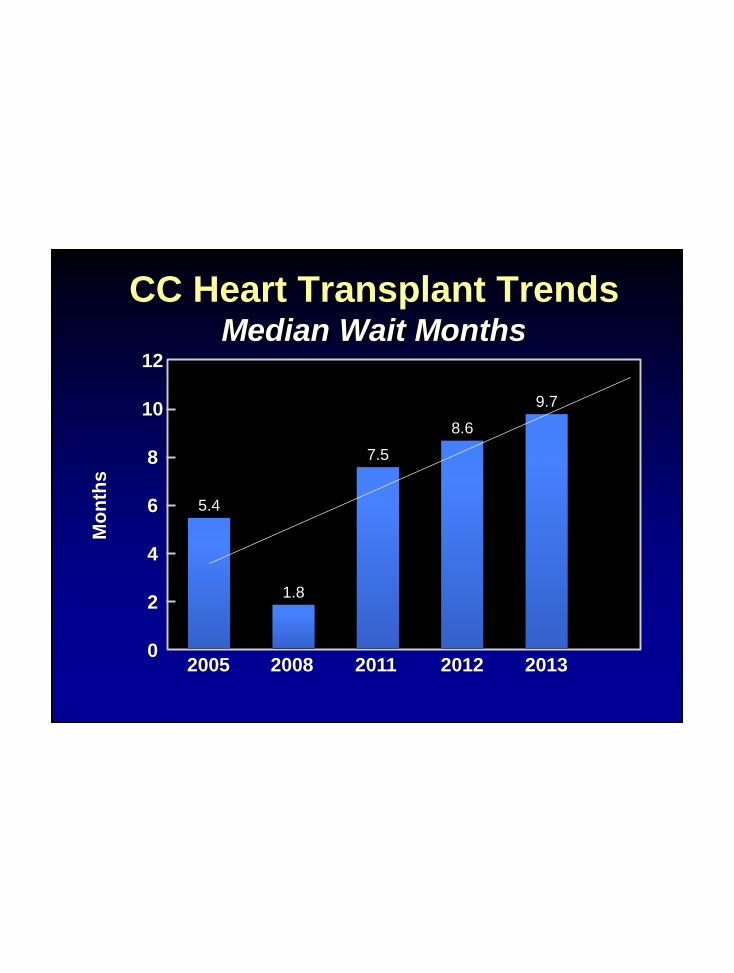
CC Heart Transplant TrendsMedian Wait Months
5.4
1.8
7.5
8.6
9.7
2005 2008 2011 2012 2013
12
10
8
6
4
2
0
Mo
nth
s
Slide Courtesy of Dr. Randall Starling

13.8
22.8
44.6 44.2
57.9
2005 2008 2011 2012 2013
12
10
8
6
4
2
0
CC Heart Transplant TrendsBridge to Transplant
Devic
es %

VAD Implants
2001 2003 2005 2007 2009 2011
80
60
40
20
0
#
Bridge to Decision
Destination Therapy
Bridge to Transplantation
2013
2000
3000
4000
5000
1975 78 81 84 87 90 93
1996
1999
2002
2005
2008
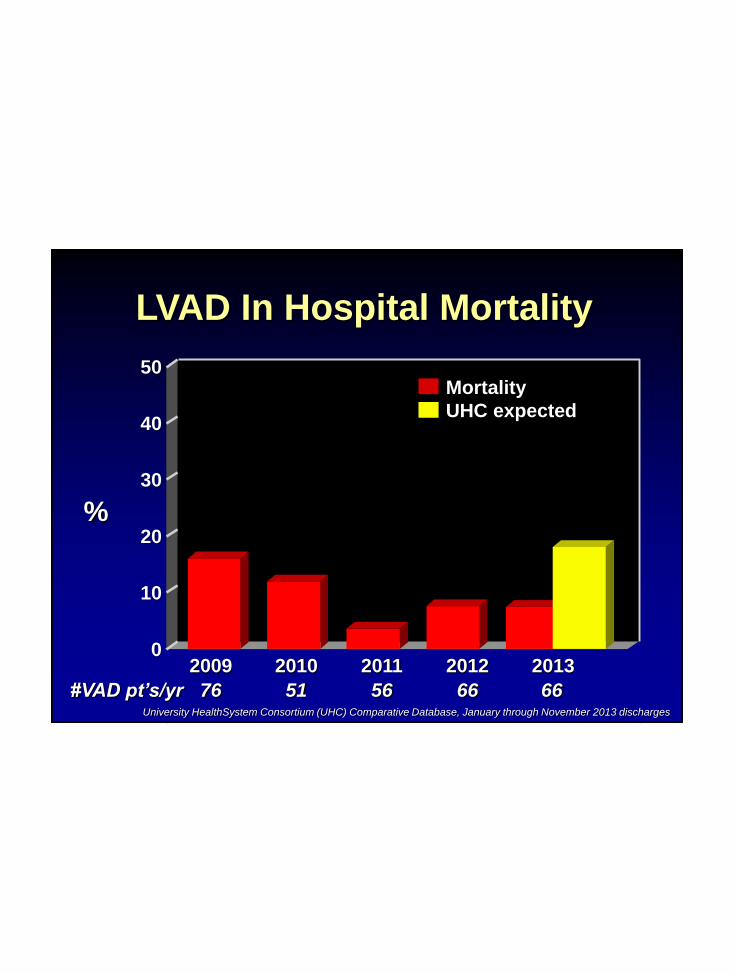
LVAD In Hospital Mortality
50
40
10
0
30
20
76 51#VAD pt’s/yr 56
Mortality
UHC expected
2010 2011 20122009 2013
66
%
66University HealthSystem Consortium (UHC) Comparative Database, January through November 2013 discharges

%
VAD Complications
40
30
20
10
0Re-op for Bleeding
RenalFailure
Stroke DeepWound
Infection
201120122013
AnyRe-op
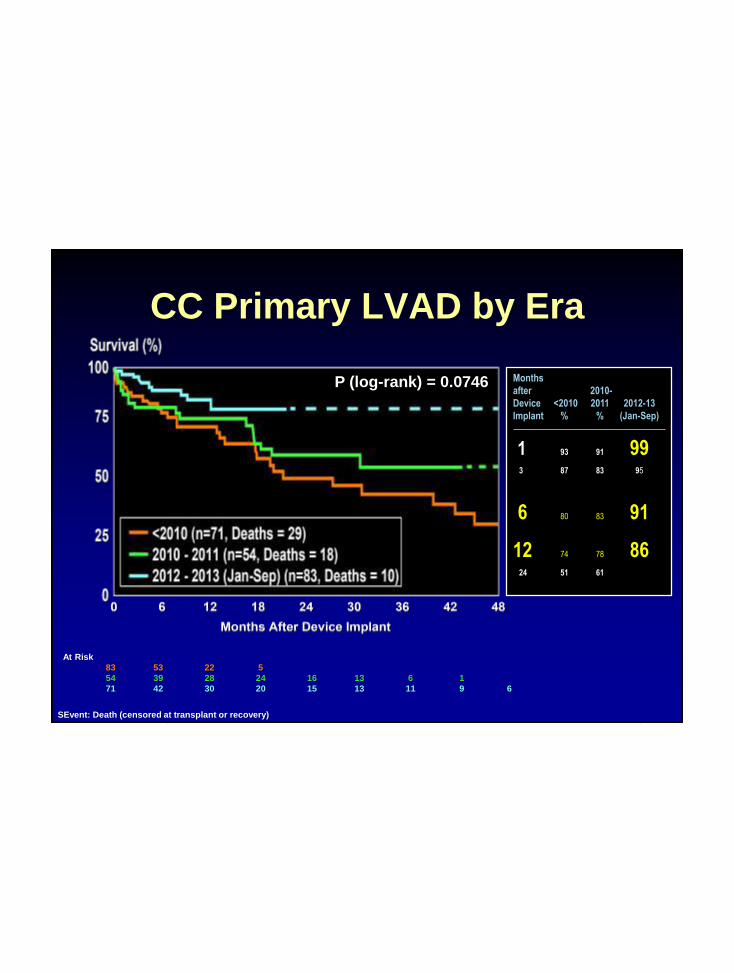
CC Primary LVAD by Era
Months
after 2010-
Device <2010 2011 2012-13
Implant % % (Jan-Sep)
1 93 91 993 87 83 95
6 80 83 91
12 74 78 8624 51 61
SEvent: Death (censored at transplant or recovery)
At Risk
83 53 22 5
54 39 28 24 16 13 6 1
71 42 30 20 15 13 11 9 6
P (log-rank) = 0.0746

HeartMate II HeartWare HVAD
CE Mark, FDA Approved
BTT
DT
CE Mark, FDA approved
BTT
DT clinical trial
LVAD Technology
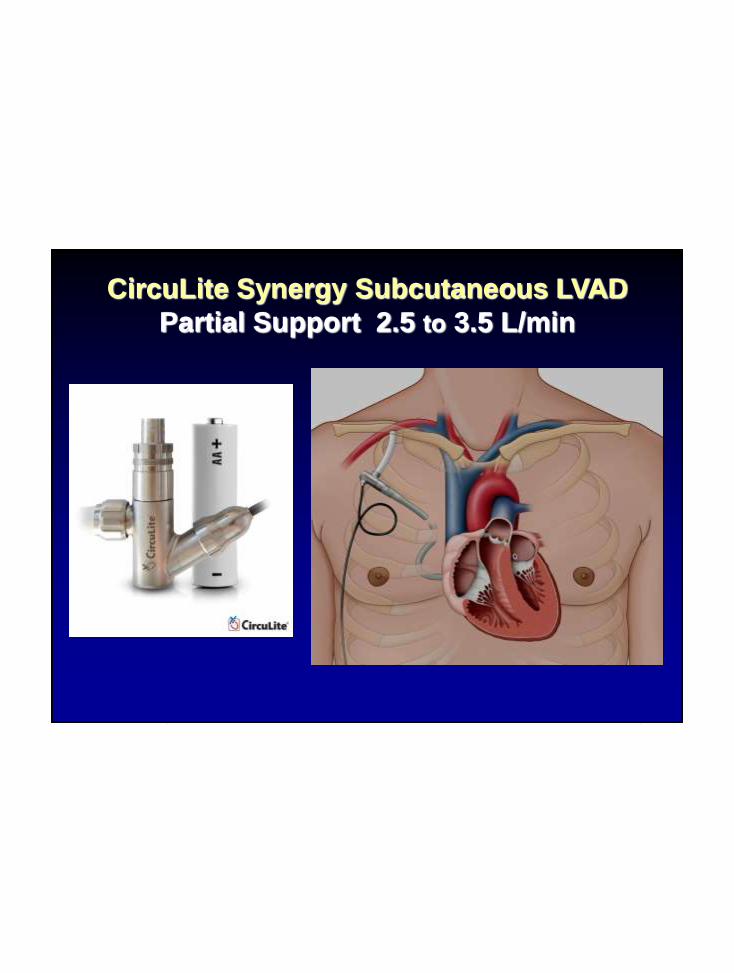
CircuLite Synergy Subcutaneous LVAD
Partial Support 2.5 to 3.5 L/min

CCF Total
Artificial Heart
Heart Transplantation2014
• Most patients who get a transplant will
be Status 1
• Majority will be on an LVAD
• Status 2 patients are unlikely to receive
a transplant but are unlikely to die
waiting
• LVAD survival very close to transplant
survival


www.heartware.com
54 gm
EU late 2013
US 2014
Trial design:
all comers
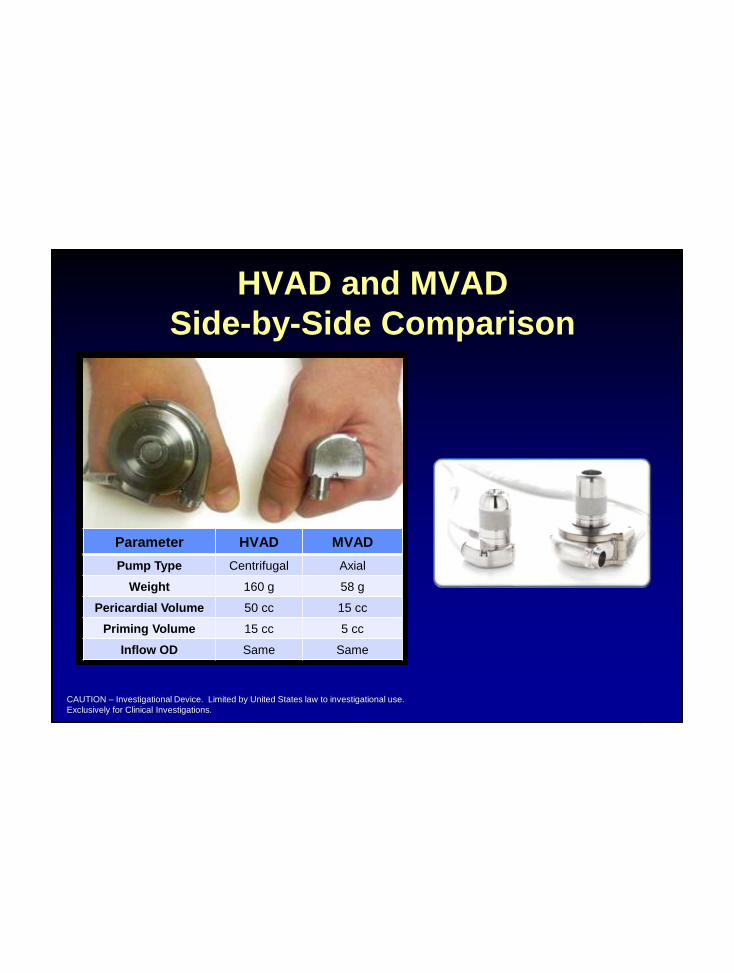
HVAD and MVAD
Side-by-Side Comparison
CAUTION – Investigational Device. Limited by United States law to investigational use.
Exclusively for Clinical Investigations.
Parameter HVAD MVAD
Pump Type Centrifugal Axial
Weight 160 g 58 g
Pericardial Volume 50 cc 15 cc
Priming Volume 15 cc 5 cc
Inflow OD Same Same

HeartMate III*
Hematologically Friendly, Proven Full
Magnetically Levitated VAD
“Artificial pulse”
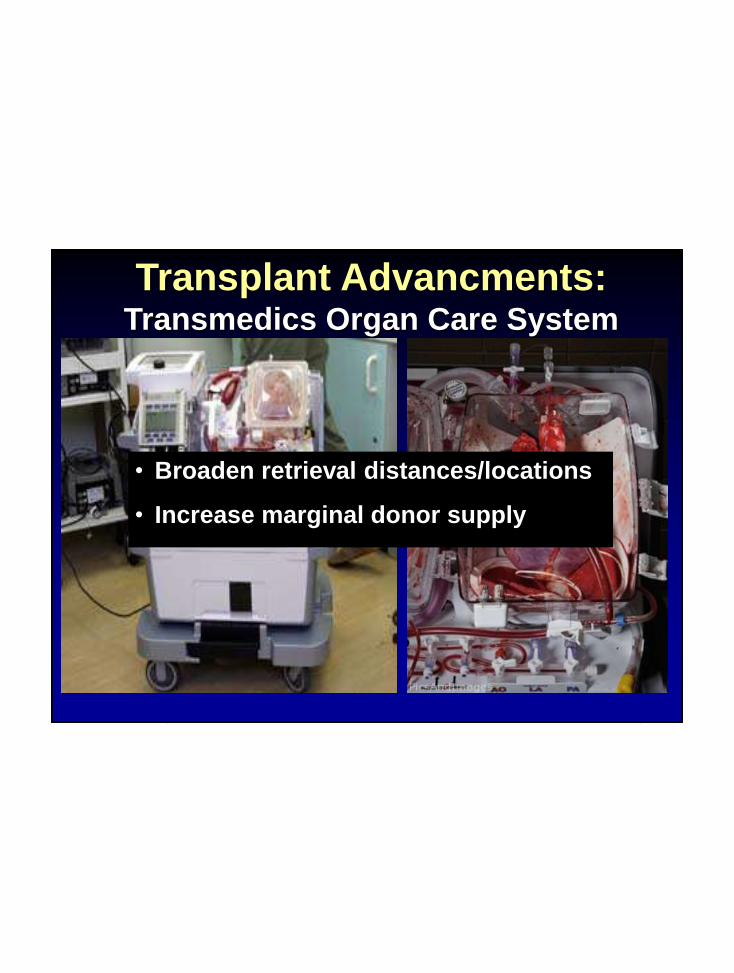
Transplant Advancments:Transmedics Organ Care System
• Broaden retrieval distances/locations
• Increase marginal donor supply
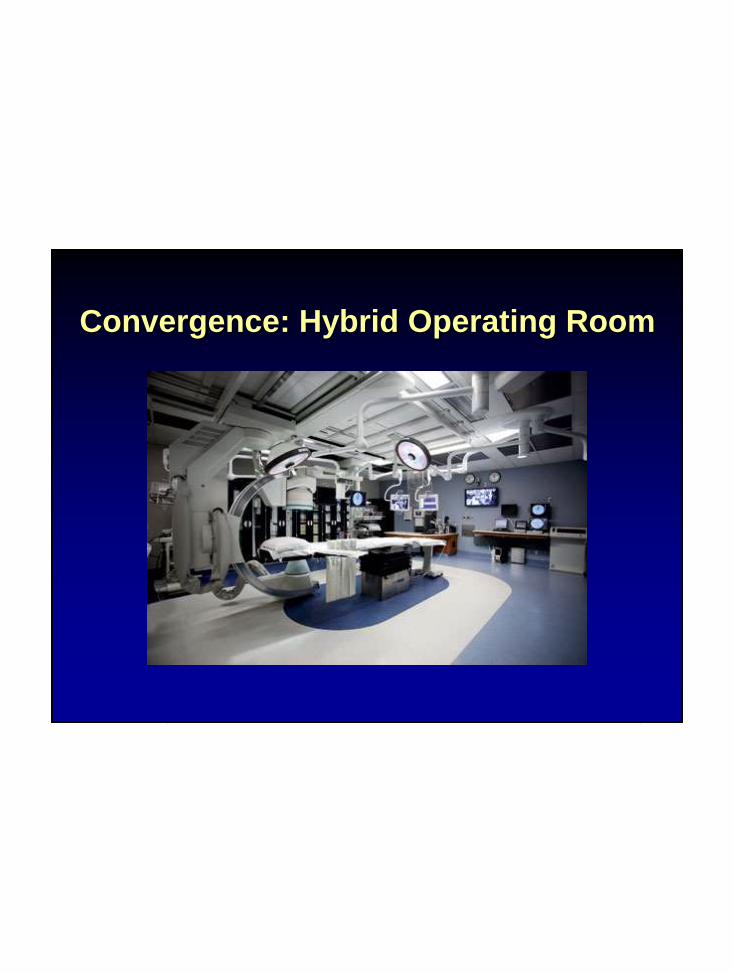
Convergence: Hybrid Operating Room

Value
Best Quality
+
Highest capabilities
+
Competitive costs




















