
Best hospitals for cardiac treatment Bangalore,Chennai,Hyderabad,Mumbai
Upload
global-hospitalsCategory
view
219download
1
Global Medical DigestISSUE 2. NOVEMBER 2013.
A Clinical Update onCardiac Sciences
Hyderabad | Chennai | Bengaluru | Mumbai
1 GLOBAL MEDICAL DIGEST | NOVEMBER 2013
Primary PTCA in a Young adult male with cardiac arrest (Unusual presentation with an unusually remarkable recovery)
A 21 year old healthy young male was brought to our emergency in unconscious state. He is neither a diabetic nor a hypertensive with a very healthy life style as well as healthy food habits. That day he went for his routine exercise and after finishing his running routine complained of epigastric discomfort a/w burning sensation in the retrosternal area. Initially he was taken to a local hospital where ECG done was s/o Acute AWMI. He had a one episode of VT/VF and was cardioverted. Subsequently as he was being shifted to higher centre, mid way through the journey he sustained a cardiac arrest and was brought to our emergency in that condition. Immediately CPR was initiated and after a prolonged CPR>30mins cardiac activity was restored.
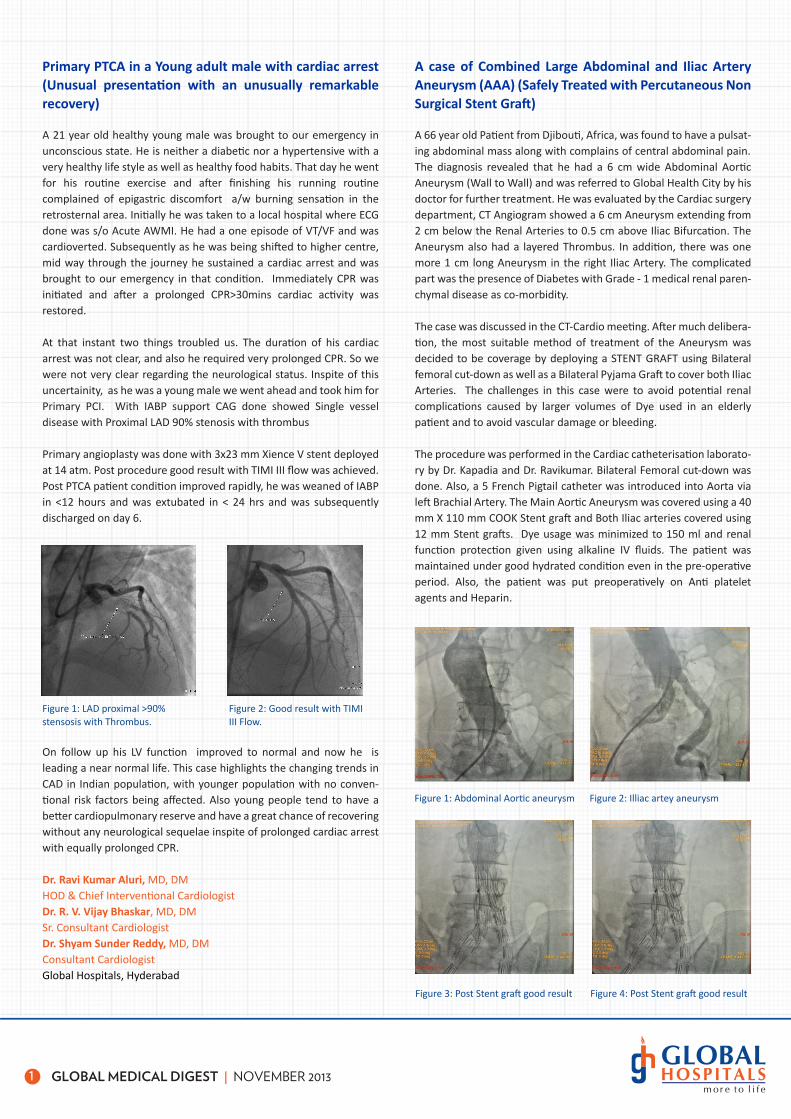
At that instant two things troubled us. The duration of his cardiac arrest was not clear, and also he required very prolonged CPR. So we were not very clear regarding the neurological status. Inspite of this uncertainity, as he was a young male we went ahead and took him for Primary PCI. With IABP support CAG done showed Single vessel disease with Proximal LAD 90% stenosis with thrombus
Primary angioplasty was done with 3x23 mm Xience V stent deployed at 14 atm. Post procedure good result with TIMI III flow was achieved. Post PTCA patient condition improved rapidly, he was weaned of IABP in <12 hours and was extubated in < 24 hrs and was subsequently discharged on day 6.
On follow up his LV function improved to normal and now he is leading a near normal life. This case highlights the changing trends in CAD in Indian population, with younger population with no conven-tional risk factors being affected. Also young people tend to have a better cardiopulmonary reserve and have a great chance of recovering without any neurological sequelae inspite of prolonged cardiac arrest with equally prolonged CPR.
Dr. Ravi Kumar Aluri, MD, DMHOD & Chief Interventional CardiologistDr. R. V. Vijay Bhaskar, MD, DMSr. Consultant CardiologistDr. Shyam Sunder Reddy, MD, DMConsultant CardiologistGlobal Hospitals, Hyderabad
A case of Combined Large Abdominal and Iliac Artery Aneurysm (AAA) (Safely Treated with Percutaneous Non Surgical Stent Graft)
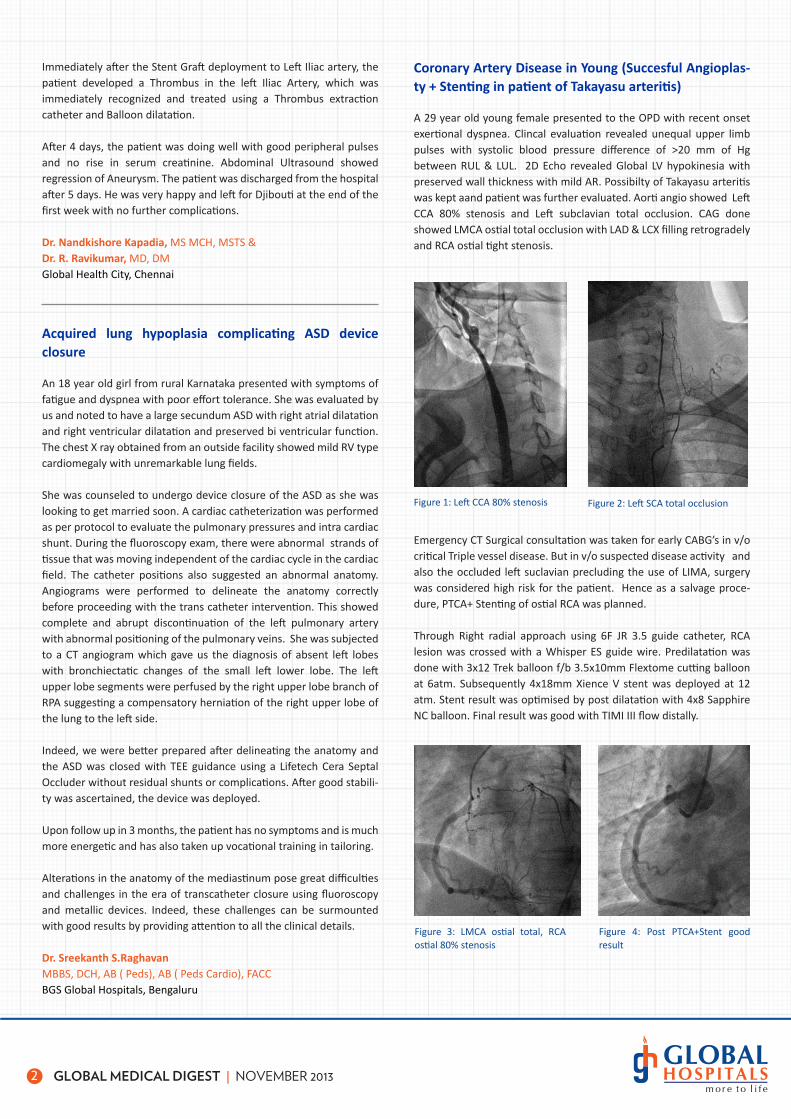
A 66 year old Patient from Djibouti, Africa, was found to have a pulsat-ing abdominal mass along with complains of central abdominal pain. The diagnosis revealed that he had a 6 cm wide Abdominal Aortic Aneurysm (Wall to Wall) and was referred to Global Health City by his doctor for further treatment. He was evaluated by the Cardiac surgery department, CT Angiogram showed a 6 cm Aneurysm extending from 2 cm below the Renal Arteries to 0.5 cm above Iliac Bifurcation. The Aneurysm also had a layered Thrombus. In addition, there was one more 1 cm long Aneurysm in the right Iliac Artery. The complicated part was the presence of Diabetes with Grade - 1 medical renal paren-chymal disease as co-morbidity.
The case was discussed in the CT-Cardio meeting. After much delibera-tion, the most suitable method of treatment of the Aneurysm was decided to be coverage by deploying a STENT GRAFT using Bilateral femoral cut-down as well as a Bilateral Pyjama Graft to cover both Iliac Arteries. The challenges in this case were to avoid potential renal complications caused by larger volumes of Dye used in an elderly patient and to avoid vascular damage or bleeding.
The procedure was performed in the Cardiac catheterisation laborato-ry by Dr. Kapadia and Dr. Ravikumar. Bilateral Femoral cut-down was done. Also, a 5 French Pigtail catheter was introduced into Aorta via left Brachial Artery. The Main Aortic Aneurysm was covered using a 40 mm X 110 mm COOK Stent graft and Both Iliac arteries covered using 12 mm Stent grafts. Dye usage was minimized to 150 ml and renal function protection given using alkaline IV fluids. The patient was maintained under good hydrated condition even in the pre-operative period. Also, the patient was put preoperatively on Anti platelet agents and Heparin.
Figure 1: LAD proximal >90% stensosis with Thrombus.
Figure 2: Good result with TIMI III Flow.
Figure 1: Abdominal Aortic aneurysm Figure 2: Illiac artey aneurysm
Figure 3: Post Stent graft good result Figure 4: Post Stent graft good result
2 GLOBAL MEDICAL DIGEST | NOVEMBER 2013
Immediately after the Stent Graft deployment to Left Iliac artery, the patient developed a Thrombus in the left Iliac Artery, which was immediately recognized and treated using a Thrombus extraction catheter and Balloon dilatation.
After 4 days, the patient was doing well with good peripheral pulses and no rise in serum creatinine. Abdominal Ultrasound showed regression of Aneurysm. The patient was discharged from the hospital after 5 days. He was very happy and left for Djibouti at the end of the first week with no further complications.
Dr. Nandkishore Kapadia, MS MCH, MSTS & Dr. R. Ravikumar, MD, DMGlobal Health City, Chennai
Acquired lung hypoplasia complicating ASD device closure
An 18 year old girl from rural Karnataka presented with symptoms of fatigue and dyspnea with poor effort tolerance. She was evaluated by us and noted to have a large secundum ASD with right atrial dilatation and right ventricular dilatation and preserved bi ventricular function. The chest X ray obtained from an outside facility showed mild RV type cardiomegaly with unremarkable lung fields.
She was counseled to undergo device closure of the ASD as she was looking to get married soon. A cardiac catheterization was performed as per protocol to evaluate the pulmonary pressures and intra cardiac shunt. During the fluoroscopy exam, there were abnormal strands of tissue that was moving independent of the cardiac cycle in the cardiac field. The catheter positions also suggested an abnormal anatomy. Angiograms were performed to delineate the anatomy correctly before proceeding with the trans catheter intervention. This showed complete and abrupt discontinuation of the left pulmonary artery with abnormal positioning of the pulmonary veins. She was subjected to a CT angiogram which gave us the diagnosis of absent left lobes with bronchiectatic changes of the small left lower lobe. The left upper lobe segments were perfused by the right upper lobe branch of RPA suggesting a compensatory herniation of the right upper lobe of the lung to the left side.
Indeed, we were better prepared after delineating the anatomy and the ASD was closed with TEE guidance using a Lifetech Cera Septal Occluder without residual shunts or complications. After good stabili-ty was ascertained, the device was deployed.
Upon follow up in 3 months, the patient has no symptoms and is much more energetic and has also taken up vocational training in tailoring.
Alterations in the anatomy of the mediastinum pose great difficulties and challenges in the era of transcatheter closure using fluoroscopy and metallic devices. Indeed, these challenges can be surmounted with good results by providing attention to all the clinical details.
Dr. Sreekanth S.RaghavanMBBS, DCH, AB ( Peds), AB ( Peds Cardio), FACCBGS Global Hospitals, Bengaluru
Coronary Artery Disease in Young (Succesful Angioplas-ty + Stenting in patient of Takayasu arteritis)
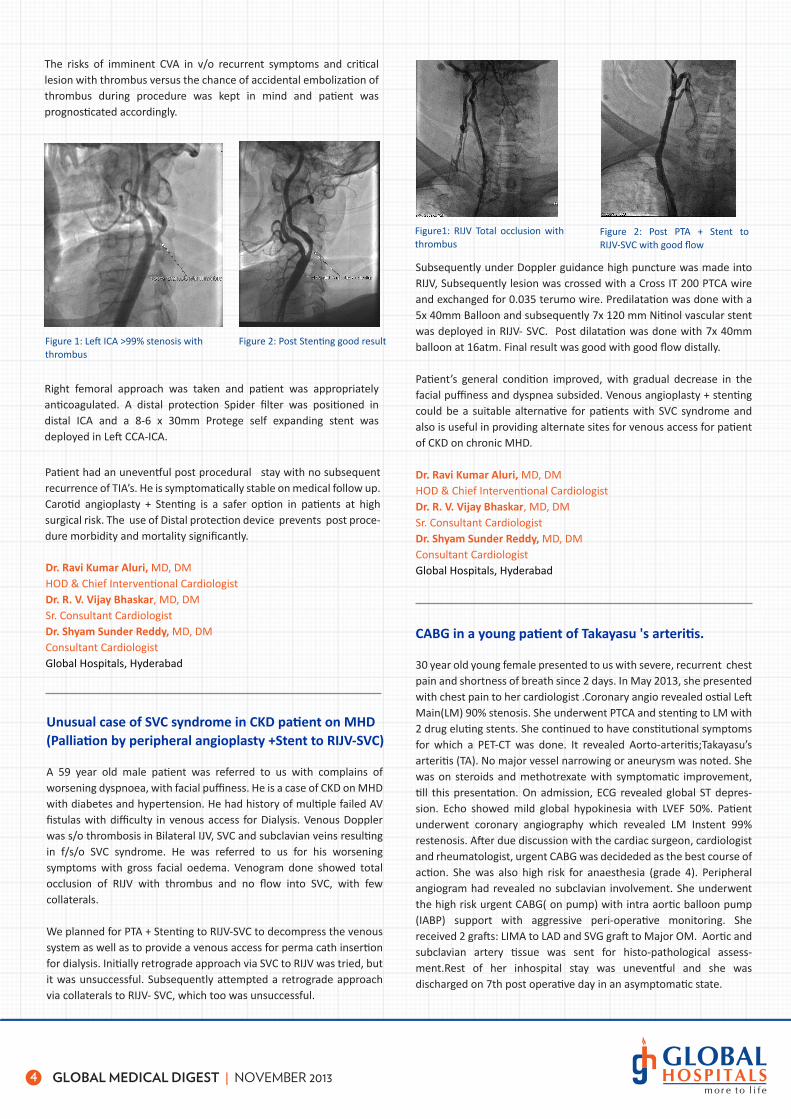
A 29 year old young female presented to the OPD with recent onset exertional dyspnea. Clincal evaluation revealed unequal upper limb pulses with systolic blood pressure difference of >20 mm of Hg between RUL & LUL. 2D Echo revealed Global LV hypokinesia with preserved wall thickness with mild AR. Possibilty of Takayasu arteritis was kept aand patient was further evaluated. Aorti angio showed Left CCA 80% stenosis and Left subclavian total occlusion. CAG done showed LMCA ostial total occlusion with LAD & LCX filling retrogradely and RCA ostial tight stenosis.
Emergency CT Surgical consultation was taken for early CABG’s in v/o critical Triple vessel disease. But in v/o suspected disease activity and also the occluded left suclavian precluding the use of LIMA, surgery was considered high risk for the patient. Hence as a salvage proce-dure, PTCA+ Stenting of ostial RCA was planned.
Through Right radial approach using 6F JR 3.5 guide catheter, RCA lesion was crossed with a Whisper ES guide wire. Predilatation was done with 3x12 Trek balloon f/b 3.5x10mm Flextome cutting balloon at 6atm. Subsequently 4x18mm Xience V stent was deployed at 12 atm. Stent result was optimised by post dilatation with 4x8 Sapphire NC balloon. Final result was good with TIMI III flow distally.
Figure 1: Left CCA 80% stenosis
Figure 3: LMCA ostial total, RCA ostial 80% stenosis
Figure 4: Post PTCA+Stent good result
Figure 2: Left SCA total occlusion

3
Take home message from the case was that Graft renal artery stenting, even though difficult but is the only useful therapeutic modality in such situations. Abnormal graft renal artery anatomy might make things difficult; approach has to be planned accordingly. Opposite femoral artery access could be useful in difficult situations. Proper catheter support as well as techniques such as floating wire could be useful in difficult situations.
Dr. Ravi Kumar Aluri, MD, DMHOD & Chief Interventional CardiologistDr. R. V. Vijay Bhaskar, MD, DMSr. Consultant CardiologistDr. Shyam Sunder Reddy, MD, DMConsultant CardiologistGlobal Hospitals, Hyderabad
GLOBAL MEDICAL DIGEST | NOVEMBER 2013
Patient had an uneventful post procedural stay. Her symptoms as well as her LV function improved gradually. Patients with aortoarteritis have an unpredictable course and are usually at high risk for CABG’s in v/o diffuse involvement of aorta. Also coexistent involvement of Subclavian arteries, precludes the usage of LIMA/RIMA. In such situations PTCA+ Stent with DES is a better alternative.
Dr. Ravi Kumar Aluri, MD, DMHOD & Chief Interventional CardiologistDr. R. V. Vijay Bhaskar, MD, DMSr. Consultant CardiologistDr. Shyam Sunder Reddy, MD, DMConsultant CardiologistGlobal Hospitals, Hyderabad
Post renal transplant - Graft renal artery stenting in a complex anatomy
A 51 year old male patient was referred to us with poorly controlled hypertension. He is a K/c/o Chronic Kidney Disease, S/P Renal transplant done in 2011. He is a diabetic and hypertensive on regular follow up. Now he presented with poorly controlled hypertension a/w worsening of creatinine. ECG, 2D ECHO done were normal and there was no evidence of graft rejection. Renal Doppler done was suggestive of Graft renal artery tight Stenosis. In v/o worsening renal dysfunction and uncontrolled hypertension, Nephrology team referred the patient to us for Graft renal artery stenting.
Recurrent TIA’S with near total occlusion of ICA with thrombus (Successful Carotid Stenting with distal protection)
A 66 year old male patient was referred to us with complains of recurrent TIA’S. He is a case of old CVA with Right hemi paresis in 2009 with total recovery. Now he presented with recurrent episodes of Transient ischemic attacks. This time he presented with TIA in the form of right upper limb weakness which improved spontaneously. 2D echo done was normal and Carotid Doppler done showed Left ICA critical stenosis. In v/o recurrent TIA’S neurologist referred the patient for further management.
Carotid angio done showed Left ICA near total occlusion with large thrombus. CAG done showed two vessel disease with >80% stenosis in LAD & RCA. As the patient was a high risk candidate for surgery in v/o coexistent cardiac and carotid disease, he was planned for PTA + stent to Left ICA with distal protection f/b elective PTCA + Stents at a later date.
Angiogram showed two tandem lesions with tight stenosis. It was a Long segment lesion with Complex anatomy due to the abnormal angle with the iliac artery. Initially we tried through RFA approach, but there was difficulty in tracking the stent even with buddy wire.
Subsequently we tried through the contra-lateral route, but there was an acute angulation at aortic bifurcation. It was causing kinking of the catheter as we try to hook the graft renal artery.
Figure 1: Graft renal artery tight stenosis
Figure 2: Unable to track even with Buddy wire
Figure 3: Acute angulation at bifurcation
Figure 4: Floating wire technique.
Figure 5: Post Dilatation Figure 6: Good result with TIMI III flow.
Hence using Floating wire technique, lesion was crossed and was successfully stented with 7x24mm (Cordis Genesis )Stent deployed at 10 atm. Post procedure good result with good flow was noted. On follow up his renal parameters improved and also the antihyperten-sive requirement decreased.
4 GLOBAL MEDICAL DIGEST | NOVEMBER 2013
Unusual case of SVC syndrome in CKD patient on MHD(Palliation by peripheral angioplasty +Stent to RIJV-SVC)
A 59 year old male patient was referred to us with complains of worsening dyspnoea, with facial puffiness. He is a case of CKD on MHD with diabetes and hypertension. He had history of multiple failed AV fistulas with difficulty in venous access for Dialysis. Venous Doppler was s/o thrombosis in Bilateral IJV, SVC and subclavian veins resulting in f/s/o SVC syndrome. He was referred to us for his worsening symptoms with gross facial oedema. Venogram done showed total occlusion of RIJV with thrombus and no flow into SVC, with few collaterals.
We planned for PTA + Stenting to RIJV-SVC to decompress the venous system as well as to provide a venous access for perma cath insertion for dialysis. Initially retrograde approach via SVC to RIJV was tried, but it was unsuccessful. Subsequently attempted a retrograde approach via collaterals to RIJV- SVC, which too was unsuccessful.
Subsequently under Doppler guidance high puncture was made into RIJV, Subsequently lesion was crossed with a Cross IT 200 PTCA wire and exchanged for 0.035 terumo wire. Predilatation was done with a 5x 40mm Balloon and subsequently 7x 120 mm Nitinol vascular stent was deployed in RIJV- SVC. Post dilatation was done with 7x 40mm balloon at 16atm. Final result was good with good flow distally.
Patient’s general condition improved, with gradual decrease in the facial puffiness and dyspnea subsided. Venous angioplasty + stenting could be a suitable alternative for patients with SVC syndrome and also is useful in providing alternate sites for venous access for patient of CKD on chronic MHD.
Dr. Ravi Kumar Aluri, MD, DMHOD & Chief Interventional CardiologistDr. R. V. Vijay Bhaskar, MD, DMSr. Consultant CardiologistDr. Shyam Sunder Reddy, MD, DMConsultant CardiologistGlobal Hospitals, HyderabadDr. Ravi Kumar Aluri, MD, DM
HOD & Chief Interventional CardiologistDr. R. V. Vijay Bhaskar, MD, DMSr. Consultant CardiologistDr. Shyam Sunder Reddy, MD, DMConsultant CardiologistGlobal Hospitals, Hyderabad
Patient had an uneventful post procedural stay with no subsequent recurrence of TIA’s. He is symptomatically stable on medical follow up. Carotid angioplasty + Stenting is a safer option in patients at high surgical risk. The use of Distal protection device prevents post proce-dure morbidity and mortality significantly.
Figure 1: Left ICA >99% stenosis with thrombus
Figure 2: Post Stenting good result
Figure1: RIJV Total occlusion with thrombus
Figure 2: Post PTA + Stent to RIJV-SVC with good flow
Right femoral approach was taken and patient was appropriately anticoagulated. A distal protection Spider filter was positioned in distal ICA and a 8-6 x 30mm Protege self expanding stent was deployed in Left CCA-ICA.
The risks of imminent CVA in v/o recurrent symptoms and critical lesion with thrombus versus the chance of accidental embolization of thrombus during procedure was kept in mind and patient was prognosticated accordingly.
CABG in a young patient of Takayasu 's arteritis.
30 year old young female presented to us with severe, recurrent chest pain and shortness of breath since 2 days. In May 2013, she presented with chest pain to her cardiologist .Coronary angio revealed ostial Left Main(LM) 90% stenosis. She underwent PTCA and stenting to LM with 2 drug eluting stents. She continued to have constitutional symptoms for which a PET-CT was done. It revealed Aorto-arteritis;Takayasu’s arteritis (TA). No major vessel narrowing or aneurysm was noted. She was on steroids and methotrexate with symptomatic improvement, till this presentation. On admission, ECG revealed global ST depres-sion. Echo showed mild global hypokinesia with LVEF 50%. Patient underwent coronary angiography which revealed LM Instent 99% restenosis. After due discussion with the cardiac surgeon, cardiologist and rheumatologist, urgent CABG was decideded as the best course of action. She was also high risk for anaesthesia (grade 4). Peripheral angiogram had revealed no subclavian involvement. She underwent the high risk urgent CABG( on pump) with intra aortic balloon pump (IABP) support with aggressive peri-operative monitoring. She received 2 grafts: LIMA to LAD and SVG graft to Major OM. Aortic and subclavian artery tissue was sent for histo-pathological assess-ment.Rest of her inhospital stay was uneventful and she was discharged on 7th post operative day in an asymptomatic state.

5 GLOBAL MEDICAL DIGEST | NOVEMBER 2013
A Novel approach for an Exceptional Condition
“PUMPLESS” KEYHOLE ASD HYBRID DEVICE CLOSURE IN A PREGNANT LADY (First of its kind in India) Unusual circumstances call for innova-tive ideas and more so, when it comes to save lives. This is such a case where the doctors at Global Health City, Chennai were confronted with a rare medical condition that tested their ultimate expertise and gave them an unspeakable pleasure of achievement.
31 yrs old Kareem Naser from Iraq had an episode of minor Cardiac stroke along with seizures and transient weakness of left hand. The diagnosis revealed that she was having a 25mm Atrial Septal Defect (ASD) with transient Ischemic attack and Paradoxical embolism. She was advised to undergo the ASD closure procedure in Iraq. But, the challenging part was that she was into her third month of pregnancy and the operation could prove fatal for the unborn baby.
Angiography image 1
Angiography image 3 Intra Operation shot during CABG
Angiography image 2
TAKAYASU'S ARTERITISIt is a rare type of large vessel vasculitis ( a group of disorders that cause inflammation of blood vessels).In TA ,aorta and its major branches are affected by this inflammation resulting in narrowing or aneurysmal dilatation and is usually associated with hypertension. Left main disease is rare in TA, affecting ~5% of all cases. This case had a unique presentation in the form of acute coronary syndrome due to severe LM instent restenosis. She will require long term immuno suppresants and close follow up to ensure disease remission and prevent recurrence of symptoms.
In an emotional despair Ms. Intisar & her husband Mr. Akran approached Global Heal City, where their case was reviewed by Dr. Nandkishore Kapadia (Senior Consultant & Cardiac Surgeon) and Dr. R. Ravikumar (Senior Consultant & Interventional Cardiologist). There was a brainstorming on the treatment approach with a sole objective to save both the lives i.e. the mother and the child. The traditional Open Heart surgery on Cardiopulmonary Pump was ruled out because of high risk of blood loss, which might lead to abortion. Closure of ASD in Catheterization laboratory was also considered to be risky; since, it could bring about radiation induced anomalies in the unborn child.
After much deliberation, the experts decided upon a unique approach; Hybrid Device Closure of the ASD through a small incision in the right chest (4th ICS) and deployment of a 28 mm ASD Device, which is a Double disc mesh made of NITINOL.
The patient was put under anaesthesia and a 4 cm incision was made in the right chest for passing the device. First, the ASD device was loaded into a 14F sheath and the sheath was used to move the device across the ASD through a small pin sized incision made in the Right Atrium. The device was opened on both sides of the septum and released under Echo Guidance. Bleeding was controlled using a Purse string suture. The passage of the Sheath and Device was monitored using a NOVEL ECHO probe attached to patient’s chest during opera-tion.
The operation lasted for 45 minutes. After deployment of the device, anaesthesia was reversed and the patient was extubated in the Operation Theatre itself. The child was safe. There was no need for blood transfusion during the whole operation and also, because of the cosmetic incision, the visibility of the scar was also minimized. Ms. Naser was under observation in the ICU for a day and then she was shifted to the ward. The recovery from such a major operation was very fast and she was on her feet the third day.
Fast Tracking in Cardiac Surgery
Economics is the main driving force in changing health care delivery in the 90s. The motto is to "do more with less." Cost containment and efficient resource utilization swing the pendulum back to the debate of early tracheal extubation in cardiac surgical patients. Recently, it has been confirmed that fast-track cardiac anesthesia is both safe and cost-effective.
Dr. Ajay ChaughuleM.S., M.Ch. - Cardiovascular SurgeonGlobal Hospitals, Mumbai
Dr. Nandkishore Kapadia, MS MCH, MSTS & Dr. R. Ravikumar, MD, DMGlobal Health City, Chennai
6 GLOBAL MEDICAL DIGEST | NOVEMBER 2013
The advantages of early extubation after cardiac surgery have been well established. Many investigators tried to find a clinical fast-track pathway for an efficient and safe approach to the postoperative management of cardiac surgery patients. The main aim of most studies was to achieve a rapid uncomplicated recovery with minimal load on the intensive care unit (ICU). Different end-points have been used to define the success of these different pathways. Most investi-gators focused on ventilation time, length of ICU and hospital stay and postoperative complications as the main end-points to evaluate the outcome of fast-track management. Fast Tracking also has improved the Patient’s Confidence and hence helping in a fast recovery from the post operative problems viz., Neuropsychiatric, renal and bedsore related ones. Fast Tracking is defined as the Extubation with in Six Hours from the end of Surgery and Shift to CTICU and early shift of the patient from the Intensive Care area with in 24 Hrs after removing the Chest tubes and all the invasive lines followed by early ambulation.
Inclusion criteria for the CTICU protocol:(i) Patients scheduled for isolated coronary artery bypass grafting (CABG), off-pump coronary artery bypass (OPCAB), isolated aortic valve replacement (AVR) or Isolated Mitral Valve Replacement without associated sequelae viz., Grossly dilated LA, Severe PAH.(ii) Non-complex isolated cardiac surgical procedures (closure of atrial septal defect Ventricular Septal Defect)
Exclusion criteria for the CTICU protocol:(i) Physical status class of >3 (according to the American Society of Anesthesiologists classification)(ii) Patients undergoing reoperation.(iii) Chronic obstructive pulmonary disease (COPD) GOLD class 2.(iv) Left ventricular dysfunction.(v) Serum creatinine of 1.50 mg/dL.(vi) Body mass index (BMI) of 35 kg m−2.(vii) Emergency operations.(viii) Surgical complications necessitating prolonged cardiopulmonary bypass time (CPB) (>150 min).
Anesthetic technique and Post operative Analgesia were practiced according to approved international protocols, which can be availed on the Anesthesia Websites.
Operative techniques are as per STS/Protocols for all Cardiac Surgical Cases on CPB or Off Pump CABG. These protocols may be referred to on any of the international Cardiac Surgical websites.
The CTICU protocol:The aims of the CTICU protocol was to Extubate the patient with in Six Hours from the time of admission to the ICU and transfer the patient postoperatively to the ward on the same day or the First post opera-tive day of the operation. Inj. Naloxone 20-40 μg was given intrave-nously to counter the deep Narcosis in about 5-10% of the cases. Sodium Bicarbonate was given to correct the metabolic acidosis prior to extubation. The first scheduled patients of the day were admitted to the CTICU directly after the operation. Patients were extubated on the CTICU after normalization of the body temperature >37°C, and adequate stabilization of their haemodynamic and respiratory conditions. Strictly, measurement of the haemodynamic parameters such as blood pressure, heart rate, diuresis and peripheral tempera-ture was performed during the whole postoperative day.
If any of these parameters did not meet the determined ‘protocol values’ for diuresis, haemodynamics, respiratory condition and blood loss, the patient was excluded for Fast Tracking. If these conditions remained stable, the patients were transferred to the ordinary ward. Blood loss via the chest tubes was carefully checked during the first 24h. Transfer to the ward was done the same day evening or the next day before noon, when the following conditions were fulfilled:
(i) Stable haemodynamic parameters without pharmacological or mechanical cardiac supports. Systolic blood pressure of >100 mmHg, diastolic blood pressure <70 mmHg.(ii) Awake and alert patients. Patients answer questions and follow orders.(iii) A stable sinus rhythm on the electrocardiogram without signs of ischaemia. Heart rate of <100/min. No atrial fibrillation.(iv) Normal respiratory function with O2 saturation of >90% with maximum 3-5L supplementary oxygen through a nasal catheter, and arterial pCO2 level of <45 mmHg on arterial blood gas analysis.(v) Blood loss of <10-50 ml over the last six Hrs via the chest tubes.(vi) Urine output of >0.5 ml kg−1/ h
Cases on CPB or Off Pump CABG. These protocols may be referred to on any of the international Cardiac Surgical websites.
In the Cardiothoracic Surgery Department, Global Hospitals, Lakdika pul, Hyderabad the Fast Tracking is being practiced from the inception of the department with 60 - 65% cardiac Surgical cases were extubat-ed with in Six Hrs Post-Op (Three of the MICAS cases were Extubated on OT Table itself) and were discharged from the CTICU the same evening or with in 24 Hrs. The readmission to CTICU has been < 0.5 to 1% of the cases where the problems like Atrial Fibrillation, Geriatric related inadequate daily intake of food and fluids are the commonest problems.
Dr. Dharma Rakshak Ayapati, MS, MCh.Director, CTVS, Global Hospitals, HyderabadDr. Amarendra Singh, MS, MCh.Sr. Consultant - Cardiothoracic & Vascular SurgeonDr. M. Rajendra Prasad, MS, MCh.Consultant - Cardiothoracic & Vascular SurgeonDr. Ravi Sankar Venuturumilli, MDChief Cardiac AnesthesiologistGlobal Hospitals, Hyderabad
Global Medical Digest Editorial DeskDr. K. V. KameshDr. Shyam Sunder Reddy
Send in your feedback & contribution to [email protected]

Global Hospitals, MumbaiT: 022 6767 0101
Global Hospitals, Lakdi-ka-pul, HyderabadT: 040 2324 4444
Global Health City, ChennaiT: 044 4477 7000
Global Hospitals,L.B. Nagar, HyderabadT: 040 2411 1111
BGS Global Hospitals,BengaluruT: 080 2625 5555
Global Hospitals Group
www.globalhospitalsindia.com
CABG in a young patient of Takayasu 's arteritis.
30 year old young female presented to us with severe, recurrent chest pain and shortness of breath since 2 days. In May 2013, she presented with chest pain to her cardiologist .Coronary angio revealed ostial Left Main(LM) 90% stenosis. She underwent PTCA and stenting to LM with 2 drug eluting stents. She continued to have constitutional symptoms for which a PET-CT was done. It revealed Aorto-arteritis;Takayasu’s arteritis (TA). No major vessel narrowing or aneurysm was noted. She was on steroids and methotrexate with symptomatic improvement, till this presentation. On admission, ECG revealed global ST depres-sion. Echo showed mild global hypokinesia with LVEF 50%. Patient underwent coronary angiography which revealed LM Instent 99% restenosis. After due discussion with the cardiac surgeon, cardiologist and rheumatologist, urgent CABG was decideded as the best course of action. She was also high risk for anaesthesia (grade 4). Peripheral angiogram had revealed no subclavian involvement. She underwent the high risk urgent CABG( on pump) with intra aortic balloon pump (IABP) support with aggressive peri-operative monitoring. She received 2 grafts: LIMA to LAD and SVG graft to Major OM. Aortic and subclavian artery tissue was sent for histo-pathological assess-ment.Rest of her inhospital stay was uneventful and she was discharged on 7th post operative day in an asymptomatic state.


















