Advanced Drug Delivery Reviewsdownload.xuebalib.com/xuebalib.com.47562.pdf · Combinatorial drug...
15
Combinatorial drug delivery approaches for immunomodulation ☆ Joshua M. Stewart a , Benjamin G. Keselowsky a,b, ⁎ a J. Crayton Pruitt Family Department of Biomedical Engineering, University of Florida, Gainesville, FL 32611, USA b Department of Pathology, Immunology and Laboratory Medicine, University of Florida, Gainesville, FL 32611, USA abstract article info Article history: Received 14 February 2017 Received in revised form 5 May 2017 Accepted 17 May 2017 Available online 19 May 2017 Immunotherapy has been widely explored for applications to both augment and suppress intrinsic host immuni- ty. Clinical achievements have seen a number of immunotherapeutic drugs displace established strategies like chemotherapy in treating immune-associated diseases. However, single drug approaches modulating an individ- ual arm of the immune system are often incompletely effective. Imperfect mechanistic understanding and het- erogeneity within disease pathology have seen monotherapies inadequately equipped to mediate complete disease remission. Recent success in applications of combinatorial immunotherapy has suggested that targeting multiple biological pathways simultaneously may be critical in treating complex immune pathologies. Drug de- livery approaches through engineered biomaterials offer the potential to augment desired immune responses while mitigating toxic side-effects by localizing immunotherapy. This review discusses recent advances in immunotherapy and highlights newly explored combinatorial drug delivery approaches. Furthermore, prospective future directions for immunomodulatory drug delivery to exploit are provided. © 2017 Elsevier B.V. All rights reserved. Keywords: Immunotherapy Combination therapy Drug delivery Biomaterials Immunomodulation Autoimmunity Cancer Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161 2. Targeted drug delivery to immune cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163 2.1. Targeting antigen-presenting cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163 2.2. Targeting T cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166 2.3. Alternative targeting strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167 3. Controlled-release approaches to recruit immune cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 168 4. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171 4.1. Combinatorial use of monoclonal antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171 4.2. Combinatorial use of immunoablation and cellular reprogramming . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171 4.3. Combinatorial use with antigen-specific therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171 5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172 Acknowledgment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172 1. Introduction The complexity of the immune system affords ample opportunities for pathologies to develop, both from aberrant immune activation and misguided immunosuppression. Recent advances delineating immunobiological mechanisms in infectious disease, cancer, and auto- immunity have helped inform novel therapeutic approaches. Immuno- therapy, an increasingly popular methodology, attempts to modulate specific arms of the immune system by interfacing with host biology to augment or suppress natural immune responses. Since Edward Jen- ner first developed a vaccine for smallpox in the late 18th century, im- munotherapy has played a prominent role in improving human health Advanced Drug Delivery Reviews 114 (2017) 161–174 Abbreviations: CAR, chimeric antigen receptor; Treg, regulatory T cell; PD-1, programmed death-1; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; PD-L1, programmed death ligand 1; APC, antigen-presenting cell; DC, dendritic cell; TLR, toll- like receptor; OVA, ovalbumin; PLGA, poly(lactide-co-glycolide); MPLA, monophosphoryl lipid A; poly(I:C), poly(inosinic:cytidylic acid); SB, SB505124; NK, natural killer; siRNA, small interfering RNA; GM-CSF, granulocyte-macrophage colony-stimulating factor. ☆ This review is part of the Advanced Drug Delivery Reviews theme issue on "Immuno- engineering". ⁎ Corresponding author at: J. Crayton Pruitt Family Department of Biomedical Engineering, PO Box 116131, Gainesville, FL 32611-6131, USA. E-mail address: [email protected]fl.edu (B.G. Keselowsky). http://dx.doi.org/10.1016/j.addr.2017.05.013 0169-409X/© 2017 Elsevier B.V. All rights reserved. Contents lists available at ScienceDirect Advanced Drug Delivery Reviews journal homepage: www.elsevier.com/locate/addr
Transcript of Advanced Drug Delivery Reviewsdownload.xuebalib.com/xuebalib.com.47562.pdf · Combinatorial drug...
-
Advanced Drug Delivery Reviews 114 (2017) 161–174
Contents lists available at ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Combinatorial drug delivery approaches for immunomodulation☆
Joshua M. Stewart a, Benjamin G. Keselowsky a,b,⁎a J. Crayton Pruitt Family Department of Biomedical Engineering, University of Florida, Gainesville, FL 32611, USAb Department of Pathology, Immunology and Laboratory Medicine, University of Florida, Gainesville, FL 32611, USA
Abbreviations: CAR, chimeric antigen receptor; Tprogrammed death-1; CTLA-4, cytotoxic T-lymphocyteprogrammed death ligand 1; APC, antigen-presenting celike receptor; OVA, ovalbumin; PLGA, poly(lactide-co-glyclipid A; poly(I:C), poly(inosinic:cytidylic acid); SB, SB50small interfering RNA; GM-CSF, granulocyte-macrophage☆ This review is part of the Advanced Drug Delivery Rev
engineering".⁎ Corresponding author at: J. Crayton Pruitt Fami
Engineering, PO Box 116131, Gainesville, FL 32611-6131,E-mail address: [email protected] (B.G. Kesel
http://dx.doi.org/10.1016/j.addr.2017.05.0130169-409X/© 2017 Elsevier B.V. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 14 February 2017Received in revised form 5 May 2017Accepted 17 May 2017Available online 19 May 2017
Immunotherapy has beenwidely explored for applications to both augment and suppress intrinsic host immuni-ty. Clinical achievements have seen a number of immunotherapeutic drugs displace established strategies likechemotherapy in treating immune-associated diseases. However, single drug approachesmodulating an individ-ual arm of the immune system are often incompletely effective. Imperfect mechanistic understanding and het-erogeneity within disease pathology have seen monotherapies inadequately equipped to mediate completedisease remission. Recent success in applications of combinatorial immunotherapy has suggested that targetingmultiple biological pathways simultaneously may be critical in treating complex immune pathologies. Drug de-livery approaches through engineered biomaterials offer the potential to augment desired immune responseswhile mitigating toxic side-effects by localizing immunotherapy. This review discusses recent advances inimmunotherapy andhighlights newly explored combinatorial drug delivery approaches. Furthermore, prospectivefuture directions for immunomodulatory drug delivery to exploit are provided.
© 2017 Elsevier B.V. All rights reserved.
Keywords:ImmunotherapyCombination therapyDrug deliveryBiomaterialsImmunomodulationAutoimmunityCancer
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1612. Targeted drug delivery to immune cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
2.1. Targeting antigen-presenting cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1632.2. Targeting T cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1662.3. Alternative targeting strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
3. Controlled-release approaches to recruit immune cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1684. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
4.1. Combinatorial use of monoclonal antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1714.2. Combinatorial use of immunoablation and cellular reprogramming . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1714.3. Combinatorial use with antigen-specific therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Acknowledgment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
reg, regulatory T cell; PD-1,-associated protein 4; PD-L1,ll; DC, dendritic cell; TLR, toll-olide); MPLA, monophosphoryl5124; NK, natural killer; siRNA,colony-stimulating factor.iews theme issue on "Immuno-
ly Department of BiomedicalUSA.owsky).
1. Introduction
The complexity of the immune system affords ample opportunitiesfor pathologies to develop, both from aberrant immune activation andmisguided immunosuppression. Recent advances delineatingimmunobiological mechanisms in infectious disease, cancer, and auto-immunity have helped inform novel therapeutic approaches. Immuno-therapy, an increasingly popular methodology, attempts to modulatespecific arms of the immune system by interfacing with host biologyto augment or suppress natural immune responses. Since Edward Jen-ner first developed a vaccine for smallpox in the late 18th century, im-munotherapy has played a prominent role in improving human health
http://crossmark.crossref.org/dialog/?doi=10.1016/j.addr.2017.05.013&domain=pdfhttp://dx.doi.org/10.1016/j.addr.2017.05.013mailto:[email protected]://dx.doi.org/10.1016/j.addr.2017.05.013http://www.sciencedirect.com/science/journal/0169409Xwww.elsevier.com/locate/addr
-
162 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
and quality of life. Similarly, allergy immunotherapy has been used clin-ically for more than a century, yielding positive outcomes for patientswith asthma, dietary, and seasonal allergies [1]. Today, immunother-apies are supplanting several well-established clinical treatment para-digms. For example, cancer immunotherapy has emerged in recentdecades as an attractive alternative to chemotherapy, as administrationof broadly cytotoxic drugs has dangerous and potentially fatal side ef-fects. By contrast, controlled modulation of innate and adaptive immu-nity can generate robust anti-tumor responses while minimizingsystemic toxicity. Recently, a number of innovative immunotherapeuticstrategies have garnered attention. Enthusiasm for immunotherapiessuch as Sipuleucel-T dendritic cell therapy, chimeric antigen receptor(CAR) T cells, andmonoclonal antibodies is buoyed by success in clinicaltrials. Sipuleucel-T immunotherapy, wherein isolated autologous den-dritic cells are exogenously activated, loaded with tumor-specific anti-gen and are re-administered, was the first FDA-approved therapeuticvaccine for cancer of any kind and showed improved survival in menwith metastatic prostate cancer [2]. Similarly, adoptive transfer ofCD19+ B cell targeting CAR T cells demonstrated sustained remissionof acute lymphoblastic leukemia in children and adults [3]. Overall,immune modulating interventions to harness specific features of theimmune system are becoming widespread and multipurpose.
The abundance of immunotherapy strategies being explored is inlarge part due to the expanding number of therapeutic tools. The in-creasedmechanistic understanding and availability of immunomodula-tory drugs including recombinant cytokines (e.g., IL-2, TGF-β, IFNγ),small molecule adjuvants (e.g., CpG, MPLA, Pam3CSK4), and monoclo-nal antibodies (e.g., anti-PD1, anti-CTLA-4, anti-IL-10) have facilitateddevelopment of immunotherapy approaches. In cancer immunotherapyalone, there are over 50 immunotherapy agents currently being used inthe clinic or in clinical trials [4]. The targets of these single drug ap-proaches are wide ranging, but similar in that they engage an isolatedimmune pathway. In one clinical trial, for example, immunotherapy
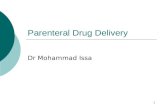
Fig. 1. Various biomaterial platforms have been developed for combinatorial drug delivery to mMicro- and nanoparticle vehicles have been designed for specific targeting/retention tomodulathave been explored to actively recruit immune populations in vivo.
with low-dose administration of IL-2 resulted in a dose-dependent in-crease of FoxP3+ regulatory T cells (Tregs) in patientswith type 1 diabe-tes, a cellular phenotype critically lacking in many autoimmuneconditions [5]. On the other hand, recent work using monoclonal anti-bodies for checkpoint blockade therapy has potentially revolutionizedcancer immunotherapy. Nivolumab, a monoclonal antibody that pre-vents T cell inhibition by impeding programmed death-1 (PD-1) signal-ing, dramatically increased survival in metastatic melanoma patients,outperforming a standard first-line chemotherapy regimen [6]. In otherclinical trials, monoclonal antibody therapy with ipilimumab, a mono-clonal antibody that inhibits cytotoxic T-lymphocyte-associated protein4 (CTLA-4), improved survival in patients with metastatic melanomaby over 10 months and ~20% exhibited long term survival after fiveyears [7,8]. While clinical achievements from single drug immunother-apies cannot be understated, such approaches are limited by a numberof factors. In particular, incomplete understanding of disease pathologyand associated immune pathways hinders identification and applicationof relevant monotherapies. Additionally, heterogeneity within diseasepathogenesis and among patient populations can limit the efficacy ofdrugs that engage individual pathways.
Combinatorial strategies to modulate multiple immune axes in coor-dination are seen as an attractive strategy to overcome these barriers,the growth of which is well documented [4,9–11]. Combinatorial immu-notherapy success is represented by recent clinical trials involvingsimultaneous administration of nivolumab and ipilimumab [12,13]. Thisgroundbreakingwork demonstrated the importance of engagingmultipleimmune pathways, as metastatic melanoma patients with programmeddeath ligand 1 (PD-L1) negative tumors displayed significantly reducedsurvival when administered either agent alone. Conversely, when PD-1and CTLA-4 monoclonal antibodies were delivered in combination, PD-L1-negative tumor patients had improved survival by over 5 months.While the clinical success of combinatorial immunomodulationhas fueleda dramatic increase in such approaches, concerns about toxicity
odulate immunity. A few of the most frequently applied systems are depicted here. (Top)e subpopulations of immune cells (e.g., T cells, DCs). (Bottom) Alternatively, bulkmaterials
-
163J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
associated with systemic administration have restricted their therapeuticpotential. Poorly managed global immunostimulation when using acti-vating adjuvants [14], CAR T cells [15], or monoclonal antibodies [16]can induce life-threatening cytokine storm or autoimmune disease. Simi-larly, chronic global immunosuppression, often employed for organ trans-plant and autoimmunity, leaves patients at risk for opportunisticinfections and tumor development [17]. To address such problems associ-atedwith systemic delivery, controlled-release platforms are increasinglybeing explored for combination therapies.
Biomaterial-based drug delivery systems have been extensively in-vestigated for immunotherapy applications. Controlled-release systemsexhibit a number of advantageous chemical andphysical properties thathave been exploited to augment immunomodulation compared to solu-ble drug administration. One frequently employed characteristic, biode-gradable materials can deliver sustained release of encapsulated drugsto prolong therapeutic levels, reducing high and/or frequent doserequirements. Similarly, drug degradation and clearance, two criticallimitations associated with soluble drug delivery, can be minimized bybiomaterial encapsulation. Drug delivery approaches can also enhancethe mass and frequency of payload delivered to immune populations,which can facilitate and augment immunotherapy. For example, bioma-terial vehicles can be modified to target drug delivery to key cells ortissues. Alternatively, implantable controlled-release platforms havebeen developed to localize drug delivery at the site of administration,adjacent to relevant immune-associated structures. Such biomaterialapproaches are also particularly appealing in order to minimize
Table 1Biomaterial platforms explored in vivo for combination immunotherapy.
Reference Delivery system Delivery target Drug(s) delive
46, 47 PLGA/PROMAXX™ microparticles DCs Antisense oligCD80, and CD8
50 Polypropylene sulfidenanoparticles
Tumor-drainingLNs/DCs
CpG and paclit
54 PLGA nanoparticles DCs/B cells MPLA, imiquim
62 PLGA nanoparticles DCs Surface conjugencapsulated C
68 PLGA nanoparticles covalentlycoupled with α-CD40
DCs Surface conjugPam3CSK4, po
69 PEGylated liposomes covalentlycoupled with CpG and α-CD40
DCs Surface conjug
80 PLGA nanoparticles covalentlycoupled with α-CD4
T cells TGF-β1 and IL
93 PEGylated liposomessurrounding PLA-PEG core
Tumormicroenvironment/Tcells
TGF-β inhibito
94 TLR9-ligand construct Myeloid/B cells Stat3 siRNA an
19 PLGA scaffolds DCs GM-CSF, CpG,
103 Silica micro-rods DCs GM-CSF, CpG,
104 PLGA microparticles DCs GM-CSF, TGF-β105 PuraMatrix™ peptide hydrogel
containing PLGA microparticlesDCs GM-CSF, CpG,
103, 104 Dextran vinyl sulfone andtetra-functionalized PEG thiolhydrogel & PLGA microparticles
DCs CCL20 in hydrIL-10 siRNA, C
114 Alginate scaffold seeded withtumor-specific T cells and silicamicroparticles
Seeded T cells GFOGER, α-CDIL-15 superago
120 Lipoprotein nanodiscs DCs CpG, antigen, aanti-CTLA4
undesirable systemic immunomodulation. While there is a vast arrayof biomaterials that have been developed for drug delivery, distinctplatforms (e.g., hydrogels, micro- or nanoparticles, liposomes) eachoffer unique advantages for immunotherapy (Fig. 1). Particle-based sys-tems have been extensively explored to deliver payloads to antigen-presenting cells [18]. Conversely, biomaterial scaffolds have beenengineered to actively recruit immune populations in vivo [19]. The var-ious tunable parameters of biomaterial platforms have made them aparticularly useful tool for immunotherapy.
This review highlights recent work on combinatorial drug deliverystrategies for immunosuppression and immunostimulation. The prima-ry focus will be on biomaterial platforms (Table 1), although core im-munotherapy principles and background results will be discussed forcontext. Specifically, we emphasize recent experimental work in drugdelivery approaches that rely on cellular targeting modalities and con-trolled-release strategies to recruit immune cells in vivo. While signifi-cant progress has been made toward integrating immunomodulatorytherapies in the clinic, we also discuss the limitations in current ap-proaches and suggest a number of future directions that show promise.
2. Targeted drug delivery to immune cells
2.1. Targeting antigen-presenting cells
Drug delivery approaches using targetingmodalities are seen as par-ticularly appealing for immunotherapy. Targeted drug delivery to
red Outcome
onucleotides against CD40,6
Reversed new-onset diabetes in non-obesediabetic (NOD) mice
axel Skewed CD4+ T cells to a Th1 phenotype andhindered melanoma growth
od, and antigen Produced persistent (N1.5 yr) germinal centerformation and plasma-cell responses
ated MPLA andpG and antigen
Robust antigen-specific T cell response wasdependent on combination delivery
ated α-CD40 and encapsulatedly(I:C), and antigen
α-CD40 coupling improved selective DC uptakeand prolonged survival in a melanoma model
ated α-CD40 and CpG Surface conjugation improved nanoparticleretention at the local tumor site, minimizedsystemic inflammation, and mitigatedmelanoma tumor growth in mice
-2 Increased the percentage of regulatory T cells
r and IL-2 Doubled the number of tumor-infiltrating NK cellsand delayed tumor growth in a melanomamodel
d CpG Minimized tumor burden in melanoma andmetastatic lung cancer models. Only thecovalently linked construct mediated potentanti-tumor effects
and antigen Demonstrated a dose-dependent recruitmentof DCs and diminished tumor burden in amelanoma model
and antigen Generated robust humoral immune responsesand ameliorated tumor burden
1, vitamin D3, and antigen Prevented type 1 diabetes onset in NOD miceand antigen Prevented type 1 diabetes onset in NOD mice
ogel and PLGA MPs encapsulatingpG and antigen
Induced a robust Th1 response. A later iterationwith CpG improved survival in mice immunizedwith B-cell lymphoma
3, α-CD28, α-CD137, and annist
Improved T cell migration, viability, and expansion,resulting in augmented tumor suppression
nd soluble anti-PD-1 and Nanodiscs alone increased the frequency ofantigen-specific T cells. In combination withcheckpoint inhibitor therapy, eliminatedtumor burden in colon carcinoma and melanomamouse models
-
164 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
disease-relevant organs, tissues, or cells can attenuate the dangerousside effects associated with broad, systemic immunotherapy. Addition-ally, selective delivery to specific immune compartments can enhancedownstream immune responses.
There have been broad efforts developing immunotherapeuticstargeting antigen-presenting cells (APCs). Operating at the interface be-tween innate and adaptive immunity, APCs are critical in mediating thebalance between immune tolerance and activation. Dendritic cells(DCs) are the most efficient APC in the body [20]. As multifunctionalregulators of immunity, variousDC subsets existwith differential capac-ities for immunogenicity [21]. Upon exposure to inflammatory signals,such as engagement of toll-like receptors (TLRs) on DCs by pathogenicligands (e.g., LPS, CpG), DCs become functionallymature. DCmaturationresults in phenotypic and functional changes that promote migration tolymphoid organs, secretion of inflammatory cytokines, and T cell activa-tion. However, in a resting state, DCs process and present antigen in animmature fashion, maintaining homeostatic tolerance toward self-antigen [22]. In addition to immature DCs, tolerogenic DC phenotypescan be induced which can promote peripheral tolerance. TolerogenicDCs employ a variety of modalities to preserve tolerance includinginduction of T cell anergy or deletion, release of anti-inflammatorycytokines (e.g., TGF-β, IL-10), and expansion of regulatory T cells [23].Insight into TLRs, DC subpopulations, and the interface between innateand adaptive immunity have driven the continued development oftailored DC-based therapies [24–27]. The robust capacity of APCs toorchestrate immunity, particularly in antigen-specific directions,makes them a frequent target for immunotherapy.
Immunotherapy with exogenously manipulated DCs has demon-strated positive therapeutic outcomes in both preclinical and clinicalinvestigations [28,29]. Since the first clinical trial using DC-based vacci-nation in 1996 [30], numerous studies have demonstrated induction ofantigen-specific T and B cell responses against malignant cancers usingDCs primed with tumor-associated antigens [31,32]. Not until 2010,however, was the first DC-based vaccine for cancer immunotherapy,Sipuleucel-T, approved by the FDA. Sipuleucel-T immunotherapy
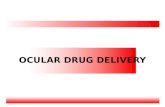
Fig. 2. Ultra-small nanoparticles (25 nm) more efficiently drain to lymph nodes and are takenlabeled nanoparticles are seen draining through lymphatic capillaries (a; scale bar, 1 mm) anwith 25 nm particles trafficking more adeptly. Flow cytometry histograms (c) examined DC ulymph nodes and was quantified (d).Reprinted by permission from Macmillan Publishers Ltd.: Nature Biotechnology [48], copyrigh
demonstrated success in patients with castration-resistant prostatecancer, improving mean survival time by ~4 months and increasingtumor-specific antibody titers and antigen-specific T cell proliferation[2]. While the anti-tumor effects demonstrated were modest, as tumorburdenwas not significantly diminished, the first-of-its-kind regulatoryapproval generated enthusiasm for DC-based immunotherapy. Alterna-tively, “negative vaccination” usingDCs to induce tolerance has been in-vestigated in models of graft survival, multiple sclerosis, and type 1diabetes [33–36]. One approach that employed DC adoptive transferfor type 1 diabetes was recently explored in a phase I clinical trial,attempting to modulate autologously isolated DCs toward an immuno-suppressive state via a combination of antisense oligonucleotidesagainst co-stimulatory molecules CD40, CD80, and CD86 before beingre-administered [37]. While the study was not powered to determinetherapeutic benefits, there was no measurable change in C-peptidelevels or in regulatory T cell frequency. Notably, however, the approachdemonstrated tolerable safety profiles. Similarly, combinatorial drugstrategies to modulate DCs ex-vivo have also been an active area of in-vestigation [38,39]. While DC-based immunotherapy has demonstratedclinical efficacy, administration of exogenously-treated DCs exhibits nu-merous barriers for widespread implementation including high cost,poor yield, and inefficient DC homing to regional lymph nodes [40,41].
A promising strategy to overcome these limitations is the targeteddelivery of immunomodulatory factors to DCs in vivo. Nano- andmicro-particles of various shapes, sizes, and compositions (e.g., lipids,polymers, metals) have been extensively studied as vehicles for in vivodrug delivery [42]. Particle-based approaches are valuable for drug de-livery because they are often highly tunable, provide a sustained releasedepot for encapsulated agents, reduce systemic toxicity and dosing re-quirements, and simplifymanufacturing, storage and shipping concerns[43,44]. Delivery to endosomes is facilitated when targeting APCs, asparticles less than ~5 μm in diameter are endocytosed by APCs withoutthe need for specific receptor-targeting strategies [45]. This strategy of“passive targeting”, relying on the intrinsic phagocytic activity of APCsfor particle-based drug delivery, has drawn significant interest for
up by DCs than large nanoparticles (100 nm) upon intradermal injection. Fluorescently-d from isolated lymph nodes (b; scale bar, 200 μm; blue:cell nuclei, red:nanoparticles),ptake of nanoparticles (black) or phosphate-buffered saline (grey) isolated from draining
t 2007.
-
165J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
immunomodulation. Recent work by the Giannoukakis laboratoryestablished microparticles containing antisense oligonucleotidesagainst CD40, CD80, and CD86 co-stimulatory molecule transcripts cancombinatorially downregulate DC maturation and ameliorate diseasein a type 1 diabetes mouse model, laying the foundation for the DC-based clinical trial mentioned above. Upon subcutaneous injection,microparticles were shown to be taken up by DCs, traffic to draininglymph nodes, augment antigen-specific regulatory T cell proliferation,and reverse new-onset diabetes [46,47].
In contrast to micron-sized particles, which exclusively rely on up-take by APCs in order to traffic to secondary lymphoid organs, nanopar-ticles can be fabricated small enough to migrate to draining lymphnodes through lymphatic vessels [45]. Reddy et al. demonstrated thiseffect in a passive targeting strategy to activate lymph node-residingDCs using ultra-small polypropylene sulfide nanoparticles (Fig. 2) [48].Initially, the authors established the importance of nanoparticle size inlymphatic drainage, as 100 nm nanoparticles were only 10% as efficientin trafficking to draining lymph nodes compared to 25 nm particles.When 25 nm particles were surface-coated with pluronic, previouslyshown to activate the complement cascade [49], intradermal injectionresulted in upregulation of co-stimulatory molecules CD80, CD86, andCD40 on lymph node DCs similar to levels seen by LPS activation.Furthermore, nanoparticles conjugated with ovalbumin (OVA) antigengenerated significant antigen-specific humoral and cellular responses.In a follow-up manuscript, Thomas and colleagues took advantage ofthis lymphatic transport phenomenon using a combinatorial drug cock-tail to activate DCs in tumor-draining lymph nodes [50]. Building ontheir original work, they hypothesized that delivery of adjuvants totumor-draining lymph nodes, which contain high concentrations oftumor-associated antigens, would induce activated DC phenotypesand generate a potent anti-tumor response. They confirmed their hy-pothesis in a murine model of melanoma. Intradermal injection of30 nm nanoparticles encapsulating CpG oligodeoxynucleotide (CpG), aTLR9 agonist, and paclitaxel, a well-established anti-proliferative drugand TLR4 ligand [51], hindered tumor growth and skewed the CD4+ Tcell distribution toward a Th1 phenotype. Results also demonstratedthe requirement of drainage to tumor-draining lymph nodes for effec-tive therapy, as contralateral injections did not generate as robust anti-gen-specific CD8+ T cell responses compared to ipsilateral injections
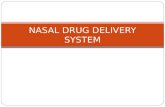
Fig. 3. Immunizationwith combinatorial TLR agonists (MPLA:TLR4 and R837:TLR7) encapsulatelymph nodes were isolated four weeks post-immunization and stained for germinal center mabar, 200 μm). (b) The number of germinal centers in draining lymph nodes over time was stratiantibody-secreting cells compared to single TLR agonists as determined by an ELISPOT assay. R
upstream of tumor-draining lymph nodes. This work also highlights arecurring theme of controlled-release drug delivery platforms: encap-sulation of the combinatorial drug cocktail produced a more efficaciousimmune response than soluble administration of adjuvants.
As important intermediaries between innate and adaptive immunity,DCs express high concentrations and heterogeneity of TLRs to directdiverse immune responses. Improved immunogenicity through combi-natorial TLR agonist delivery is being explored. For example, mice immu-nized with bone marrow-derived DCs activated with TLR7 and TLR3agonists improved cytotoxic lymphocyte responses in vivo compared toindividual agonists [52]. Similarly, engagement of distinct stimulatorypathways through TLR4 and TLR8 on human DCs in vitro inducedcytokine IL-12 and IL-23 levels 50–100 fold higher than those inducedby single TLR agonists [53]. Biomaterial drug delivery systems havesought to take advantage of combinatorial TLR approaches. A break-through study in 2011 demonstrated the benefits of controlled-releasevehicles to deliver two TLR agonists in vivo [54]. Mice subcutaneouslyinjected with poly(lactide-co-glycolide) (PLGA) nanoparticles bearingmonophosphoryl lipid A (MPLA; TLR4 agonist), imiquimod (TLR7 ago-nist), and OVA antigen generated persistent germinal center formationand plasma-cell responses, which were present in lymph nodes forN1.5 years following immunization (Fig. 3). Notably, they found immuni-zation with the combinatorial formulation increased the antigen-specifichumoral response compared to nanoparticles with individual TLR ago-nists. Results also demonstrated that TLR engagement on B cells, in addi-tion to DCs, was critical in producing antibody responses. As cellsdifferentially express TLRs [55], this work suggests that TLR-based vac-cines can be optimally designed by rational inclusion of TLR agonists togenerate tailored immune responses. Higher order TLR combinationsare also being investigated. Recent work described high-throughputmethods for combinatorial loading of factors in microparticles [56], aswell as a high-throughput microarray to assess DC activation in responseto combinations of three TLR-encapsulating microparticles [57,58].The adjuvant-screening microarray demonstrated microparticle combi-nations delivering poly(inosinic:cytidylic acid) (poly(I:C)), MPLA, orCpG elicited differential expression of DC activation biomarkers CD86,MHC-II, CCR7, IL-12, and IL-10.
Classically, antigen that is endocytosed by DCs is presented by MHCclass II molecules and restricted to CD4+ T cell presentation [59]. Cross-
d in polymeric PLGA nanoparticles induces robust germinal center formation. (a) Drainingrkers, with combinatorial agonist delivery producing the most persistent formation (scalefied by treatment group. (c) Combinatorial TLR agonists promote longevity (~1.5 years) ofeprinted by permission from Macmillan Publishers Ltd.: Nature [54], copyright 2011.
-
166 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
presentation is the process by which antigen is released from the endo-some into the cytosol and, through alternative pathways, presented onMHC class Imolecules to CD8+ cytotoxic T cells [60]. Cross-presentationis vital to vaccines dependent on cytotoxic T cell responses. Controlled-release particles have been shown to be advantageous in generatingCD8+ T cell responses. In addition to promoting prolonged antigen pre-sentation, sustained release of antigen from biodegradable microparti-cles has demonstrated a roughly 1000-fold increase in cross-presentation compared to soluble protein [61]. In a similar vein, a recentnanoparticle-based approach pioneered by the Fahmy laboratoryemployed combinatorial TLR activation to generate robust CD8+ T cellimmunity [62]. The platform utilized PLGA nanoparticles surface-conju-gatedwithMPLA and encapsulated CpG and OVA. An important findingfrom their research demonstrated the significance of the mode ofpresentation when designing TLR-based vaccines. CpG efficacy as animmunostimulant, characterized by cytokine profiles, antibody titers,and antigen-specific T cell responses, wasmaximizedwhen encapsulat-ed in nanoparticles compared to when surface bound. As the receptorfor CpG, TLR9, is localized endosomally [63], the authors suggest thatphysiologically relevant presentation of CpG is important in generatinga robust immune response. This work additionally showed the impor-tance of co-delivery, as single TLR agonists failed to replicate the potentCD8+ T cell response generated with the combinatorial formulation.
Strategies for APC targeting have also been developed that bind sur-face moieties to increase retention and uptake. This approach seeks tominimize off-target drug interactions and can producemore potent im-mune responses due to the efficiencywithwhich drug cargo is more se-lectively taken up by APCs. Particulate formulations functionalized withsurfacemoieties includingα-CD40,α-DEC205, andα-CD11c antibodieshave been explored for DC targeting [64]. As noted earlier, in contrast tomicroparticles, nano-sized particulates injected intradermally orsubcutaneously can migrate and drain through lymphatic vessels.While advantageous in certain applications, nanoparticles are proneto non-specific cellular uptake and this competition for uptake iscompounded by hepatic filtration and renal clearance [65]. Thus,targeting strategies to improve DC uptake of nanoparticles is particular-ly valuable. Recent work characterized the impact of targeting moietiesbased on particulate size, demonstrating that particles surface conjugat-ed with the human C-type lectin receptor DC-SIGN dramatically im-proved DC uptake for polymeric nanoparticles, but only produced amodest increase in uptake for micron-sized particles [66]. The choiceof targeting moiety is often dictated by the therapeutic intention. DCmaturation is undesirable when delivering immunomodulatory drugsfor tolerance-inducing purposes. Along these lines, microparticlesmod-ified with antibodies against CD11c or DEC-205, an integrin and C-typelectin respectively that are highly expressed on DCs, or functionalizedwith peptides P-D2 or RGD, targeting intercellular adhesion molecule-4 and surface integrins respectively, were found to efficiently targetDCs, both in vitro and in vivo, in a non-activating manner [67].
Conversely, targeting ligands have been studied to improve uptakeby DCs and simultaneously augment immunogenicity. Rosalia and col-leagues demonstrated that covalent coupling of α-CD40 to PLGA nano-particles containing antigen, Pam3CSK4 and poly(I:C), a TLR2 and TLR3agonist respectively, improved selective DC uptake and activated DCs invivo [68]. In a tumor model of melanoma, subcutaneous administrationofα-CD40-functionalized adjuvant-bearing nanoparticles improved theantigen-specific CD8+ T cell response and prolonged survival comparedto mice treated with nanoparticles conjugated with an isotype control.While the authors confirm that conjugation of α-CD40 to nanoparticlesaugmented nanoparticle uptake and delivery of TLR agonists to DCs, itwas not investigated whether DCmaturation was improved by engage-ment of CD40 inflammatory signaling pathways. In another approach,Kwong and colleagues used a combinatorial drug approach deliveredintratumorally to generate an anti-tumor response [69]. Intratumoralinjection of PEGylated liposomes surface conjugatedwith CpG and anti-body against CD40 significantly mitigated tumor growth in a mouse
model of melanoma. Importantly, retention at the local tumor site wasconfirmed. Surface conjugation of α-CD40 and CpG, the receptors forwhich are highly expressed on APCs, aided tumor retention. Liposomeuptake by CD11c+ DCs and F4/80+ macrophages was observed at ex-tended time periods, 24 and 48 h post injection. Similarly, their drug de-livery approach curtailed systemic inflammation, as intratumoraladministration of soluble immunomodulators increased serum levelsof TNF-alpha and IL-6 and resulted in weight loss compared to the lipo-some formulation.
2.2. Targeting T cells
While APC-targeting therapies attempt to modulate immunitythrough critical cellular mediators, drug delivery strategies have alsobeen developed to target other immune compartments more directly.Like DC-based therapies, various strategies to modulate T cell numbersand activity ex-vivo for adoptive transfer therapyhave been investigated(reviewed in [70]). However, limitations with adoptive cellular transfersimilarly plague T cell approaches. T cell targeting strategies have beenconducted to work around these limitations. In one approach, re-searchers developed a targeting strategy to minimize T cell loss uponadoptive transfer. Three days after adoptive transfer of allogeneic Tcells bearing the distinct congenic marker Thy1.1, intravenous injectionof PEGylated liposomes conjugated with targeting ligands againstThy1.1 effectively marked N95% of transferred cells [71]. As the authorssuggest, this targeting approach could be universally applied for adop-tive cellular transfer through introduction of distinct surface markersby genetic engineering of cells pre-transfer. In another approach fortargeted drug delivery to discrete T cell populations, Vincent et al. devel-oped aMHC-I tetramer construct to deliver payloads to antigen-specificT cells [72]. Conjugation of MHC-I tetramers loaded with islet-specificpeptide antigen to saporin, a ribosomal toxin, enriched ablation ofantigen-specific, autoreactive CD8+ T cells in a mouse model of type 1diabetes. Three intravenous injections of the construct reduced diabetesincidence in 8 week old non-obese diabetic mice by 30% afterN50 weeks compared to controls. This approach, employing selectivedelivery to distinct T cell compartments, is desirable in order to mini-mize global immunotoxicity.
Regulatory T cells (Tregs) are critical for themaintenance of immunetolerance. Impaired Treg function and reduced numbers have beenidentified as important factors in cases of autoimmunity, organ trans-plant rejection, and allergy (reviewed in [73]). Immunotherapy strate-gies to augment Treg activation, proliferation, and function remainhighly desirable, and have been explored through a number of diversedrug delivery platforms. In one example, microparticles deliveringsustained release of the Treg chemokine CCL22 were shown to recruitTregs locally and delay organ rejection in a murine allotransplantmodel [74]. In another unique strategy, the Hubbell laboratory devel-oped an erythrocyte-targeting platform for induction of antigen-specifictolerance [75]. This system was composed of erythrocyte-binding con-structs that were coupled with antigen, built around the premise thatapoptotic cells, and erythrocytes are frequently recycled, are clearedthrough self-tolerance promoting pathways (reviewed in [76]). In a fol-low-up study by the Hubbell group, researchers explored the mecha-nisms by which the erythrocyte-targeting platform induced tolerance[77]. Results using antigen-specific T-cell-transgenic OT mouse modelsdemonstrated that blockade of PD-1/PD-L1 signaling, but not CTLA-4/CD28, impaired antigen-specific T cell deletion, anergy, and expressionof regulatory biomarkers. Additionally, the platform significantly in-creased the frequency of Tregs compared to administration of solubleantigen. Depletion of Tregs through α-CD25 demonstrated the criticalrole Tregs played in mediating CD4+ and CD8+ T cell suppression. Theconcept of antigen coupled to apoptotic cells recently demonstratedpromise in a phase I clinical trial for multiple sclerosis [78]. In the trial,patients that received apoptotic leukocytes covalently coupled withvarious multiple sclerosis-specific peptide antigens demonstrated
-
167J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
favorable safety profiles. Furthermore, patients receiving higher dosesof apoptotic coupled cells displayed decreases in antigen-specific T cellresponses.
As numerous factors have been identified as important modulatorsfor Treg induction, a combinatorial approach engaging multiple path-ways has been suggested as an ideal strategy for robust Treg responses.In one such approach, PLGA microparticles were loaded with threeknown Treg inducing agents: rapamycin, TGF-β1, and IL-2 [79]. Micro-particles were separately loaded with individual factors and demon-strated sustained release of encapsulated agents over 3–4 weeks.Notably, the system was most effective in skewing murine CD4+ Tcells to express FoxP3 in vitrowhen all threemicroparticleswere includ-ed. This work also showed the combinatorial microparticle formulationwas also effective for induction of human Tregs in vitro, suggesting thetranslatability of their approach. Using an in vivo targeting scheme,McHugh and colleagues developed a similar approach by targeting de-livery of TGF-β and IL-2 to T cells using PLGA nanoparticles surface-con-jugated with α-CD4 antibodies [80]. Their results demonstrated thatnanoparticles surface modified with α-CD4 dramatically increasedbinding of T cells by ~18-fold in vitro. Furthermore, the increased bio-availability of these pro-tolerogenic factors was shown to skew theCD4+ T cell populations in vivo toward a regulatory phenotype,increasing the percentage of CD4+ T cells expressing FoxP3. The authorssuggest this approach can also minimize the pleiotropic effects of thesecytokines when delivered solubly, as TGF-β is well known to cause se-vere adverse responses when administered systemically [81]. However,as they note, a potential shared drawback of particle-based systems isnon-specific uptake of nanoparticles byAPCs through passive phagocyt-ic activity. As such, it may be advantageous to minimize undesirablephagocytosis when designing vehicles for drug delivery to non-APCcellular compartments. Strategies such as functionalizing peptidesfrom membrane proteins CD47 or CD200, reported ubiquitous self-identifiers, have been employed for drug delivery applications to miti-gate macrophage-mediated phagocytic clearance [82,83]. Additionally,surface charge has been explored tomodulate phagocytic uptake of par-ticulate delivery systems, albeit with varying results. It has been report-ed that particles exhibiting high negative or positive charges are morereadily taken up by DCs and macrophages compared those displayinga neutral surface charge [84,85]. However, concerns about toxicitymay limit drug delivery applications for such approaches. In 2014, forexample, Getts et al. described how anionic microparticles were takenup by monocytes via the scavenger receptor, MARCO, which resultedin sequestration of monocytes in the spleen and subsequent apoptoticclearance [86]. Similarly, it has been demonstrated that cationic parti-cles can result in the generation of reactive oxygen species ormitochon-drial injury pathways [87,88]. Lastly, particle shape has been describedas an influential design consideration to avoid phagocytosis. Unlikespherical particles which are phagocytosed within minutes, rat alveolarmacrophages had greatly diminished uptake capacity when incubatedwith ellipsoid polystyrene particles [89]. The initial point of contact be-tween macrophages and particles was shown to be pivotal in internali-zation kinetics. Macrophages that attached to the spheroid end of anellipsoid particle internalized it withinminutes, however, those that en-countered the flat portion of the ellipsoid did not internalize the particlefor over 12 h. These approaches have been suggested to increase pay-load delivery to non-APC targets. Understanding the parameters that ef-fect phagocytosis are critical in designing particle-based drug deliverysystems and need to be further explored.
2.3. Alternative targeting strategies
Alternative immunotherapy targeting strategies have also beenpursued. A recent innovative targeting approach modulates immunityby “hitchhiking” onto albumin protein draining to peripheral lymphoidorgans [90]. Instead of targeting cell surface receptors, Liu et al. soughtto localize an immunostimulatory vaccine intranodally by conjugating
a lipophilic albumin-binding moiety to CpG. Subcutaneous administra-tion of the albumin-binding construct resulted in an 8-fold increase inaccumulation to peripheral lymph nodes compared to soluble CpG.Localization was further amplified as the albumin-binding vaccineshowed sustained retention in lymph nodes after seven days. Notably,their approach dramatically increased anti-tumor effects in a murinemodel, while reducing systemic inflammation by attenuating serumIL-6 and IL-12 levels.
Localization of immunomodulatory agents to sites of concentratedimmune activity has also been explored by more direct deliveryapproaches. In one strategy, researchers highlighted the efficacy ofcontrolled-release particles to elicit robust immunity via intranodal de-livery. By mapping the lymphatic system of mice using the tracer dyeEvans blue, Jewell et al. intranodally injected PLGA microparticles con-taining poly(I:C) andOVA asmodel antigen to generate antigen-specificimmunity [91]. Results demonstrated a single intranodal injection ofthe microparticle vaccine expanded the frequency of OVA-specificCD8+ T cells by over 8-fold compared to intramuscular immunization.Additionally, encapsulation of vaccine components in controlled-release microparticles augmented poly(I:C) intranodal persistence.Fluorescently-conjugated poly(I:C) levels released from microparticleswere ~2.5-fold higher measured after four days compared to an equiv-alent soluble intranodal dose. This work also displayed a core paradigmof controlled-release drug delivery approaches by reducing the adju-vant dose necessary to achieve similar immunogenicity. Microparticlesloaded with a poly(I:C) and antigen generated a stronger OVA-specificCD8+ T cell response than soluble poly(I:C) given at a 10-fold greaterdose. Analogous intranodal microparticle immunotherapy has alsodemonstrated antigen-specific suppression in amousemodel of multiplesclerosis by delivering myelin self-antigen and the immunoregulatorydrug rapamycin [92].
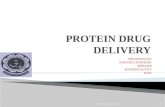
Drugdelivery approacheshave also beenexplored to localize immuno-therapy agents to the tumormicroenvironment. In a strategy to promote Tcell proliferation and simultaneously attenuate the immunosuppressivetumor microenvironment, Park and colleagues designed PEGylatedliposomes to deliver IL-2 and a TGF-β inhibitor (Fig. 4) [93]. The nanoscalevehicles were composed of a lipid bilayer surrounding a degradable, poly-meric core encapsulating the hydrophilic cytokine, IL-2, and the small hy-drophobic TGF- β inhibitor, SB505124 (SB). To deliver sustained release ofboth drugs upon hydrolysis of the internal polylactide-PEG core, SB wassolubilized with β-cyclodextrans to enable encapsulation of the small hy-drophobic molecule. Solubilization minimized the burst release observedcompared to when SB was loaded in the absence of β-cyclodextransand improved sustained release to over 7 days in vitro. The authorsdemonstrated the efficacy of this combination therapy as weeklyintratumoral injections of nanoscale liposomes significantly improved sur-vival and delayed tumor growth in amousemodel of melanoma, more sothan liposomes bearing individual drugs. Strikingly, intratumoral numbersof activated CD8+ T cells and natural killer (NK) cells more than doubledupon liposome administration. Lastly, using NK-depleted mice, theyshowed liposomal-mediated tumor suppression required NK cells.
Targeting of multiple immune compartments for coordinated activa-tion can also be desirable. In one example, researchers covalently linkedCpG to small interfering RNA (siRNA) to preferentially target myeloidand B cells rich in TLR9 [94]. Their combinatorial approach sought to acti-vate the TLR9 immunostimulatory pathway and silence Stat3, an impor-tant oncogenic transcription factor that mediates immunosuppressiveactivity. By covalently linking CpG to Stat3 siRNA, the researchers hypoth-esized that TLR9 ligation, located endosomally, would facilitate cytosolicescape of the construct and improve siRNA gene silencing. The efficacyof their engineered platformwas demonstrated in murine tumor modelsof melanoma and metastatic lung cancer. Administration of non-conjugated CpG and Stat3 siRNA produced only minor anti-tumoreffects compared to the covalently linked combination. Additionally, thefrequency of FoxP3+ Tregs within the CD4+ T cell compartmentintratumorally diminished from ~60% to 25% post CpG-Stat3 siRNA
-
Fig. 4. Synthesis scheme of PEGylated liposomes with polymeric cores to deliver the T cell proliferative factor, IL-2, and a TGF-β inhibitor, SB505124. Methacrylated cyclodextrans (CD)were used to solubilize the small, hydrophobic inhibitor (SB505). (Top) CD-SB505 complexes and IL-2 were loaded into a biodegradable polymer core (red) with a PEGylatedliposomal exterior (grey). Photoinduced polymerization of the polymer core and the acrylated-CD induces nanoscale liposome gel (nLG) formation, capable of delivering sustainedrelease of both drugs upon hydrolysis of the internal polymeric core. (a–c) B16 melanomas were tracked over time in response to various treatments, with combinatorial nLGsdelaying tumor growth most effectively. Red arrows indicate intratumoral treatment administration.Reprinted by permission from Macmillan Publishers Ltd.: Nature Materials [93], copyright 2012.
168 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
peritumoral injections. The authors found that CpG-siRNA gene silencingwas dependent on TLR9 expression, though it was unclear whether en-gagement of TLR9 promoted endosomal release or altered intracellularprocessing.
3. Controlled-release approaches to recruit immune cells
While targeting systems have been investigated for in vivo drugdelivery, controlled-release materials to promote cellular recruitmentand localized conditioning have also gained traction for immunotherapy.Traditionally, synthetic biomaterial scaffolds have primarily been investi-gated in applications for tissue engineering (reviewed in [95]). Scaffoldswith high porosity are compatible carriers for cellular engraftment or re-cruitment and also allow encapsulation of biologics to direct cell function.Many of the same attributes that makes biomaterial structures desirablefor tissue engineering can be applied for immunomodulation. Biomate-rials can be engrafted with immune cells in adoptive cell therapies toimprove leukocyte viability and subsequent immune responses [96]. Sim-ilarly, biological signals incorporated into biomaterial scaffolds have beenbroadly explored for immunomodulation (reviewed in [97]). This sectionof the review discusses the controlled-release material approaches thathave been developed to recruit and modulate immune cells in situ.
Inflammatory responses following biomaterial implantation coin-cide with recruitment of innate immune cells to the site of injection.This is advantageous for combinatorial therapies that seek to deliver im-munomodulatory drugs to APCs. However, the significance of DCs as themost effective APC can be diminished by its low frequency [21]. In re-sponse, some drug delivery approaches intend to maximize DC recruit-ment, differentiation, and proliferation. Granulocyte-macrophagecolony-stimulating factor (GM-CSF) is a pleiotropic cytokine producedby a number of myeloid and supporting cells that features prominentlyin the pursuit of a number of DC-recruiting biologics. GM-CSF has dem-onstrated capacity for promoting DC proliferation, recruitment of DCs,antigen cross-presentation, and differentiation of monocytes into DCs[98–101]. Incorporation of GM-CSF has been explored both in emergingimmunotherapy technologies and clinically. As has been discussed ear-lier, Sipuleucel-T immunotherapy utilizes GM-CSF to mature and ex-pand DCs upon autologous isolation. GM-CSF has also been used as asupplementary therapeutic for cancer treatment to improvemyeloid re-covery following chemotherapy (reviewed in [102]).
Recently, a number of groups have combined GM-CSF with immu-nomodulatory agents in controlled-release materials to activate or sup-press DCs. In 2009, researchers in the Mooney laboratory created asynthetic biomaterial scaffold to program DCs in a protective, anti-
-
Fig. 5.Mesoporous silica rods (MSRs) aggregate upon injection, forming macroporous spaces where host cells can be recruited and educated by encapsulated immunomodulatory drugs,GM-CSF and CpG. (a) In vitro cumulative release of GM-CSF fromMSRs (b) CD11c+ CD11b+ (left) and CD11c+ MHC II+ (right) DCs were recruited to MSR scaffolds in a dose-dependentmanner. (c) In vitro cumulative release of CpG from MSRs. (d) CpG inclusion in MSRs augmented DC activation, increasing surface expression of CD86 and MHC class II molecules. (e)Fluorescent in vivo imaging demonstrated MSRs loaded with OVA antigen deliver sustained release of protein over an extended period compared to bolus OVA injection.Reprinted by permission from Macmillan Publishers Ltd.: Nature Biotechnology [103], copyright 2014.
169J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
tumor fashion [19]. The authors fabricated biodegradable PLGA scaffoldsthat were made macroporous in order to create space for DC recruit-ment and antigen-presentation. Initial investigations demonstratedscaffolds loaded with GM-CSF were shown to mediate DC recruitmentin a dose-dependent manner, improving DC recruitment by up to 12times that of unloaded scaffolds. Upon the addition of the TLR9 agonistCpG, DC recruitment to the biomaterial was further improved as ~1.5million DCs were isolated 7 days following in vivo implantation. Conse-quently, the highlight of thisworkwas the combinatorial effect CpG andGM-CSF had inmitigating tumor burden in themousemodel ofmelano-ma. PLGA matrices loaded with tumor lysate as antigen, CpG, and GM-CSF increased antigen-specific CD8+ T cell recruitment, DC traffickingto lymph nodes, and resulted in a 90% survival rate by day 90 comparedto 0% survival for unloaded scaffolds.
This combinatorial approach of using GM-CSF and CpG to modulateDCmaturation has been explored in the same laboratory through otherdrug delivery vehicles as well. One strategy implemented an injectablematerial that agglomerated in vivo to form a macroporous scaffold, im-proving the safety profile by removing the need the surgical implanta-tion [103]. Results from this work show mesoporous silica rodssubcutaneously injected can deliver sustained release of GM-CSF, CpG,and OVA as a model antigen to generate a potent OVA-specific cellular
and humoral response (Fig. 5). By altering the size of the microrods,they demonstrated that larger aspect-ratio material augmented cellularrecruitment, which they attributed to the larger interparticle poresallowing robust cellular infiltration. Notably, they found that three re-peated booster injections of the unencapsulated soluble factorswere re-quired to produce an OVA IgG2a antibody response comparable to thatof the single injection of the microrod technology encapsulating thesame factors. This combinatorial drug delivery strategy also significantlyminimized tumor growth and survival using an EG.7-OVA tumormousemodel.
Applications of GM-CSF as a DC chemokine has also been explored intandemwith other immunomodulatory drugs tomoderate immune tol-erance. Lewis et al. describe a dual-microparticle approach consisting ofsmall (~1 μm), phagocytosable microparticles and large (~30 μm), non-phagocytosablemicroparticles designed to recruit DCs and induce toler-ance in type 1 diabetes upon subcutaneous injection [104]. Briefly, largeparticles encapsulatingGM-CSF and the tolerogenic drug TGF-β1 servedto create a microparticle depot to recruit and condition DCs, respective-ly, via extracellular pathways. Simultaneous delivery of small,phagocytosable particles containing insulin B:9–23 peptide, a primaryautoantigen for type 1 diabetes, and an additional immunomodulatoryfactor, vitamin D3, targeted the intracellular delivery of factors to
-
170 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
recruited DCs. The premise behind the system was to promote presen-tation of autoantigen in a tolerogenic context to reeducate aberrantautoreactivity. In vitro characterization demonstrated the efficacy ofthis system, inducing tolerogenic DC phenotypes with downregulatedexpression of CD86 and MHC-II molecules, suppression of allogeneic Tcell proliferation, and induction of FoxP3+ Tregs. Cumulatively, its effectin vivo resulted in a 40% prevention rate of type 1 diabetes in 4-week oldnon-obese diabetic mice.
In a similar approach to induce antigen-specific tolerance in a type 1diabetes model, researchers fabricated a peptide hydrogel that deliveredsustained release of GM-CSF to recruit DCs to an immunomodulatorymicroenvironment [105]. The hydrogel contained PLGA microparticlesencapsulating denatured insulin to promote self-tolerance to recruitedDCs and, notably, CpG. While CpG is more classically used as a vaccineadjuvant in an inflammatory capacity, the authors note it can elicit anti-inflammatory effects such as inducing IL-10 production [106]. Thisapproach protected disease incidence in 40% of pre-diabetic mice.Additionally, results demonstrated that hydrogel implantation generateda resolvable granulomatous tissue at the site of administration that re-cruited an array of leukocyte populations and with some characteristicsof a tertiary lymphoid organ.
In another DC recruiting strategy pioneered by the Roy group, the DCchemokine MIP3α, also known as CCL20, was loaded into a crosslinkabledextran vinyl sulfone and tetra-functional PEG thiol hydrogel along withPLGA microparticles encapsulating IL-10 targeting siRNA and plasmidDNA antigen [107]. The authors built off their original research whichdemonstratedmicroparticles bearing IL-10 siRNAboostedDCmaturation,T cell proliferation, and skewed the in vivo T cell response to a Th1
Fig. 6. (Top) Illustration of the biomaterial system. Collagen-mimetic peptides conjugated to thetumor beds. Additionally, microparticles in the scaffold encapsulating an IL-15 superagonist andproliferation.(a) Bioluminescent imaging of 4T1 breast tumors demonstrates the potency oftechnology compared to other treatments. (b) Kaplan-Meier survival curves for treated and cocells, showing the scaffold technology encourages robust T cell proliferation and migration.Reprinted by permission from Macmillan Publishers Ltd.: Nature Biotechnology [114], copyrig
phenotype [108]. By incorporating a DC chemokine into biodegradablehydrogels, Singh et al. hypothesized that more DCs would encountersiRNA and plasmid antigen and the hydrogel might serve as an artificialDC priming center. The results demonstrated that a sustained chemokinegradient exuded in a controlled-release manner from the hydrogel waspivotal to its success, as the combinatorial system recruited ~5-foldmore DCs over an extended period of time compared to an equivalentbolus dose in vitro. The recruited DCs efficiently infiltrated hydrogelsand displayed notably diminished gene expression of IL-10. In vivo resultsdemonstrated that intramuscular injection of the combinatorial DC-recruiting platform induced T-cell class switching toward a Th1 response,inducing CD8+ CTL responses ~3-foldmore robust compared to adminis-tration of soluble components alone [109]. An iteration of this work wasfurther explored, when in 2014 Pradhan et al. incorporated the adjuvantCpG into the IL-10 siRNAandplasmidDNAantigen bearingmicroparticles[110]. Hydrogels formulated with the full combinatorial payload (MIP3αand microparticles containing IL-10 siRNA, CpG, and plasmid DNA)significantly improved prophylactic survival in mice immunized withA20 B-lymphoma cells compared to controls without all four agents.
Incorporation of biological factors into scaffolds can also be accom-plished by surface ligation. This may be advantageous when designingsystems that benefit from localized effects and to limit systemic toxicityfrom soluble factors. This approach has been suggested as a potential so-lution for allograft tolerance, wherein researchers conjugated TGF-β1 toglass beads to generate Tregs [111]. Combinatorial approaches of liga-tion of biologics has also been explored. Hume and colleagues function-alized IL-10 and TGF-β1 to PEG hydrogels in an effort to minimize DCmaturation in vitro [112]. Immature DCs seeded in hydrogels with
polymeric scaffold encourage trafficking of loaded tumor-specific T cells into surroundingwith surface-bound anti-CD3, anti-CD28, and anti-137 stimulate lymphocyte survival andthe biomaterial system, as minimal tumor presence is observed with the combinatorialntrol mice (ms:median survival). (c) Bioluminescent imaging of adoptively transferred T
ht 2014.
-
171J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
immobilized pro-tolerogenic cytokines maintained their immaturephenotypes following incubation with LPS, displaying reducedexpression of MHC-II molecules and IL-12 production. In another exam-ple, researchers demonstrated that incorporation of cell-adhesion moi-eties improved subsequent interaction between recruited T cells andimmunomodulatory microenvironment in a hydrogel platform [113].Specifically, the Anseth laboratory developed a PEG hydrogel function-alized with intercellular adhesion molecule-1 and α-Fas antibodies,where Fas is a well-established death receptor, to modulate localized Tcell apoptosis. This platform could be valuable as a complementaryimmunotherapy on the surface of cell encapsulationmaterials to reduceallograft rejection. Results show that hydrogels coatedwith both ligandsimprove T cell apoptosis by 50% in vitro compared to hydrogel onlycontaining α-Fas antibodies.
Macroporous biomaterial scaffolds contain large surface area whichencourages complex biomaterial design and conveys higher order spa-tiotemporal control of the surroundingmicroenvironment. In a particu-larly innovative combinatorial approach, Stephan et al. developed analginate scaffold implant to improve adoptive transfer of tumor-specificT cells [114]. In the approach, tumor-specific T cells were loaded into thealginate scaffold which was conjugated with the collagen-mimeticpeptide (GFOGER) to stimulate T cell migration (Fig. 6). Additionally,the scaffold contained silica microparticles with surface-bound α-CD3,α-CD28, andα-CD137 antibodies to stimulate lymphocyte proliferationand encapsulated an IL-15 superagonist as a T cell survival signal. Thismultipronged approach minimized numerous steps normally requiredfor adoptive cellular transfer (e.g., T cell expansion and viability,intratumoral delivery), as biological factors included in the alginatescaffold account support these functions in vivo. Notably, uponperitumoral administration of the biopolymer in a murine tumormodel, adoptively transferred tumor-specific T cells were isolatedfrom tumor beds and found to suppress tumor growth. The inclusionmicroparticles bearing survival and proliferative factors was shownto generate robust T cell expansion and improve the viability of encap-sulated cells released from the scaffold. Additionally, GFOGER linkageonto the polymer matrix augmented T cell migration and resulted in asignificantly higher number of T cells released from the scaffold.
4. Future directions
There is mounting evidence that combinatorial immunotherapy canoffer significant advantages in treating complex immune-associateddiseases. While we have described a number of approaches that havedemonstrated potential as therapeutic strategies, the future of combina-torial drug delivery is not limited to the approaches discussed. The contin-ually expanding body of immunotherapy research provides a strongfoundation from which scientists can draw upon. Certain drug deliveryopportunities may prove particularly important in establishing successfulimmunotherapies in the future.
4.1. Combinatorial use of monoclonal antibodies
Checkpoint blockade therapy has buoyed the enthusiasm for mono-clonal antibody immunotherapy, as it has produced some of the mostsuccessful human clinical trials for cancer in recent years (reviewed in[115]). Drug delivery strategies to exploit the expanding field of mono-clonal antibody immunotherapy could be immensely beneficial. For ex-ample, controlled-release approaches can aid in mitigating antibodyclearance that limits their therapeutic effects [116]. Additionally, local-ized release adjacent to specific immune-associated structures (e.g.,peritumorally, perinodally) could augment immunotherapy and ad-dress renewed concerns of systemic toxicity. However, limitationswith biomaterial incorporation to deliver sensitive biologics are wellestablished. Functional activity can be lostwhen attempting to encapsu-late or conjugate large proteins to drug delivery vehicles [117]. Noveldrug delivery strategies to circumvent these challenges are actively
being explored. Recent work, for example, developed a method toreduce antibody oxidation encapsulated in silk biomaterials viamethionine functionalization [118]. Strategies that utilize monoclonalantibodies in combination with other immunotherapeutics have alsodemonstrated promise in pre-clinical investigations. One approach ex-plored this past year saw a vaccine composed of four components(anti-PD-1, tumor-specific antibodies, recombinant IL-2, and albumin-binding CpG-peptide antigen constructs) build upon checkpoint inhibi-tor blockade therapy to mediate improved, antigen-specific survival intumor-bearingmice [119]. Another recent approach utilized lipoproteinnanodiscs to deliver multiple tumor-associated epitopes and the adju-vant CpG while intraperitoneally administering checkpoint blockadetherapy [120]. The combinatorial technology,when applied in coordina-tion with anti-PD-1 and anti-CTLA4 antibodies, dramatically improvedanti-tumoral immunity compared to nanodiscs alone. These results sug-gest that applications involving monoclonal antibody therapy couldbenefit from combinatorial and controlled-release approaches.
4.2. Combinatorial use of immunoablation and cellular reprogramming
Often accomplished through monoclonal antibodies, selective deple-tion of immune compartments has been investigated as an alternativetherapy for systemic, cytotoxic chemotherapy. Monoclonal antibodiesagainst CD20+B cells are frequently employed forNon-Hodgkin Lympho-ma [121,122]. Similarly, depletion of CD25+ Tregs has been investigatedin a clinical setting for augmenting anti-tumor vaccines [123]. Approachesutilizing immunoablating techniques have also generated interest in au-toimmune disease to deplete autoreactive cells in order to reprogram ho-meostatic immunity. Combination therapy with anti-thymocyte globulinand GM-CSF has been shown to increase Treg frequency, alter DC pheno-types, and improve survival inmousemodels of type 1diabetes [124,125].This combinatorial approach was validated when explored in clinicaltrials of type 1 diabetics, improving Treg frequency and preserving β-cell function compared to placebo controls [126,127]. While careful con-sideration should be given to therapies that completely ablate leukocytesubpopulations for fear of promoting systemic immunosuppression,there is growing evidence that suggests immunoablation in combinationwith immunomodulation can be a useful approach.
4.3. Combinatorial use with antigen-specific therapy
A recurring theme throughout the research discussed in this reviewhas been the incorporation of disease-specific antigen in combinatorialdrug delivery platforms. Antigen-specific immunotherapy is highlydesirable to elicit controlled, directional immune responses. Viable anti-gen-specific therapies are advantageous compared to broadly cytotoxicor immunosuppressive drugs that can result in systemic toxicities.There is a wealth of research on immunotherapy systems that utilize dis-ease-relevant antigen in coordination with immunomodulatory drugs,which indicates the value of this combination (reviewed in [9]). Con-trolled-release biomaterials have been extensively studied to deliver an-tigen, as their tunable properties can be beneficial in shaping immuneresponses. As discussed, sustained release of antigen from biodegradablePLGA nanoparticles has improved both prolonged antigen-presentationand the capacity for cross-presentation in bone-marrow derived DCs[61]. Mimicking long-standing clinical approaches for allergy immuno-therapy, biomaterials have also been studied to deliver self-protein toinduce antigen-specific tolerance. In one approach, intravenous adminis-tration of polystyrene nanoparticles conjugated to myelin sheath epi-topes ameliorated multiple sclerosis in a mouse model [128]. Vaccinesthat rely on immunomodulatory drugsmay be improved upon by the in-clusion of antigen. For example, nanoparticles containing the immuno-suppressive drug rapamycin were most effective in generatingsustained humoral and cellular responses when antigen was includedin the formulation [129,130]. Modulating immunity in antigen-specific
-
172 J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
immune directions will likely continue to be an important feature offorthcoming combinatorial immunotherapy strategies.
5. Conclusions
There is growing interest in combinatorial drug delivery strategiesfor immunomodulation. The breadth of new research highlightingthe efficacy of multi-drug immunotherapy schemes is perenniallyexpanding. Biomaterial platforms offer numerous advantages tooptimize drug delivery for immunotherapy.While there are many chal-lenges associated with successful immunotherapy, we are optimisticthat combinatorial drug delivery platforms can help overcome thelimitations associated with previous therapeutic interventions.
Acknowledgment
This work was supported by the National Institute of Diabetes andDigestive and Kidney Diseases R01DK091658 and R01DK098589.
References
[1] M. Larche, C.A. Akdis, R. Valenta, Immunological mechanisms of allergen-specificimmunotherapy, Nat. Rev. Immunol. 6 (2006) 761–771.
[2] P.W. Kantoff, C.S. Higano, N.D. Shore, E.R. Berger, E.J. Small, D.F. Penson, C.H. Redfern,A.C. Ferrari, R. Dreicer, R.B. Sims, Y. Xu, M.W. Frohlich, P.F. Schellhammer, I.S.Investigators, Sipuleucel-T immunotherapy for castration-resistant prostate cancer,N. Engl. J. Med. 363 (2010) 411–422.
[3] S.L. Maude, N. Frey, P.A. Shaw, R. Aplenc, D.M. Barrett, N.J. Bunin, A. Chew, V.E.Gonzalez, Z. Zheng, S.F. Lacey, Y.D. Mahnke, J.J. Melenhorst, S.R. Rheingold, A.Shen, D.T. Teachey, B.L. Levine, C.H. June, D.L. Porter, S.A. Grupp, Chimeric antigenreceptor T cells for sustained remissions in leukemia, N. Engl. J. Med. 371 (2014)1507–1517.
[4] M.J. Smyth, S.F. Ngiow, A. Ribas, M.W. Teng, Combination cancer immunotherapiestailored to the tumour microenvironment, Nat. Rev. Clin. Oncol. 13 (2016)143–158.
[5] M. Rosenzwajg, G. Churlaud, R. Mallone, A. Six, N. Derian, W. Chaara, R. Lorenzon,S.A. Long, J.H. Buckner, G. Afonso, H.P. Pham, A. Hartemann, A. Yu, A. Pugliese, T.R.Malek, D. Klatzmann, Low-dose interleukin-2 fosters a dose-dependent regulatoryT cell tuned milieu in T1D patients, J. Autoimmun. 58 (2015) 48–58.
[6] C. Robert, G.V. Long, B. Brady, C. Dutriaux, M. Maio, L. Mortier, J.C. Hassel, P.Rutkowski, C. McNeil, E. Kalinka-Warzocha, K.J. Savage, M.M. Hernberg, C. Lebbe,J. Charles, C. Mihalcioiu, V. Chiarion-Sileni, C. Mauch, F. Cognetti, A. Arance, H.Schmidt, D. Schadendorf, H. Gogas, L. Lundgren-Eriksson, C. Horak, B. Sharkey,I.M. Waxman, V. Atkinson, P.A. Ascierto, Nivolumab in previously untreated mela-noma without BRAF mutation, N. Engl. J. Med. 372 (2015) 320–330.
[7] F.S. Hodi, S.J. O'Day, D.F. McDermott, R.W. Weber, J.A. Sosman, J.B. Haanen, R.Gonzalez, C. Robert, D. Schadendorf, J.C. Hassel, W. Akerley, A.J. van denEertwegh, J. Lutzky, P. Lorigan, J.M. Vaubel, G.P. Linette, D. Hogg, C.H.Ottensmeier, C. Lebbe, C. Peschel, I. Quirt, J.I. Clark, J.D. Wolchok, J.S. Weber, J.Tian, M.J. Yellin, G.M. Nichol, A. Hoos, W.J. Urba, Improved survival withipilimumab in patients with metastatic melanoma, N. Engl. J. Med. 363 (2010)711–723.
[8] M. Maio, J.J. Grob, S. Aamdal, I. Bondarenko, C. Robert, L. Thomas, C. Garbe, V.Chiarion-Sileni, A. Testori, T.T. Chen, M. Tschaika, J.D. Wolchok, Five-year survivalrates for treatment-naive patients with advanced melanoma who receivedipilimumab plus dacarbazine in a phase III trial, J. Clin. Oncol. 33 (2015)1191–1196.
[9] L. Northrup, M.A. Christopher, B.P. Sullivan, C. Berkland, Combining antigen andimmunomodulators: Emerging trends in antigen-specific immunotherapy for au-toimmunity, Adv. Drug Deliv. Rev. 98 (2015) 86–98.
[10] P. Pozzilli, E. Maddaloni, R. Buzzetti, Combination immunotherapies for type 1 di-abetes mellitus, Nat. Rev. Endocrinol. 11 (2015) 289–297.
[11] M.R. Carstens, R.C. Fisher, A.P. Acharya, E.A. Butterworth, E. Scott, E.H. Huang, B.G.Keselowsky, Drug-elutingmicroarrays to identify effective chemotherapeutic com-binations targeting patient-derived cancer stem cells, Proc. Natl. Acad. Sci. U. S. A.112 (2015) 8732–8737.
[12] J. Larkin, V. Chiarion-Sileni, R. Gonzalez, J.J. Grob, C.L. Cowey, C.D. Lao, D.Schadendorf, R. Dummer, M. Smylie, P. Rutkowski, P.F. Ferrucci, A. Hill, J.Wagstaff, M.S. Carlino, J.B. Haanen, M. Maio, I. Marquez-Rodas, G.A. McArthur,P.A. Ascierto, G.V. Long, M.K. Callahan, M.A. Postow, K. Grossmann, M. Sznol, B.Dreno, L. Bastholt, A. Yang, L.M. Rollin, C. Horak, F.S. Hodi, J.D. Wolchok, Combinednivolumab and ipilimumab or monotherapy in untreated melanoma, N. Engl. J.Med. 373 (2015) 23–34.
[13] J.D. Wolchok, H. Kluger, M.K. Callahan, M.A. Postow, N.A. Rizvi, A.M. Lesokhin, N.H.Segal, C.E. Ariyan, R.A. Gordon, K. Reed, M.M. Burke, A. Caldwell, S.A. Kronenberg,B.U. Agunwamba, X. Zhang, I. Lowy, H.D. Inzunza, W. Feely, C.E. Horak, Q. Hong,A.J. Korman, J.M. Wigginton, A. Gupta, M. Sznol, Nivolumab plus ipilimumab in ad-vanced melanoma, N. Engl. J. Med. 369 (2013) 122–133.
[14] S.G. Reed, M.T. Orr, C.B. Fox, Key roles of adjuvants in modern vaccines, Nat. Med.19 (2013) 1597–1608.
[15] R.A. Morgan, J.C. Yang, M. Kitano, M.E. Dudley, C.M. Laurencot, S.A. Rosenberg, Casereport of a serious adverse event following the administration of T cells transducedwith a chimeric antigen receptor recognizing ERBB2, Mol. Ther. 18 (2010)843–851.
[16] C.J. Voskens, S.M. Goldinger, C. Loquai, C. Robert, K.C. Kaehler, C. Berking, T.Bergmann, C.L. Bockmeyer, T. Eigentler, M. Fluck, C. Garbe, R. Gutzmer, S.Grabbe, A. Hauschild, R. Hein, G. Hundorfean, A. Justich, U. Keller, C. Klein, C.Mateus, P. Mohr, S. Paetzold, I. Satzger, D. Schadendorf, M. Schlaeppi, G. Schuler,B. Schuler-Thurner, U. Trefzer, J. Ulrich, J. Vaubel, R. von Moos, P. Weder, T.Wilhelm, D. Goppner, R. Dummer, L.M. Heinzerling, The price of tumor control:an analysis of rare side effects of anti-CTLA-4 therapy in metastatic melanomafrom the ipilimumab network, PLoS One 8 (2013), e53745.
[17] M.D. Denton, C.C.Magee,M.H. Sayegh, Immunosuppressive strategies in transplan-tation, Lancet 353 (1999) 1083–1091.
[18] S.T. Reddy, M.A. Swartz, J.A. Hubbell, Targeting dendritic cells with biomate-rials: developing the next generation of vaccines, Trends Immunol. 27(2006) 573–579.
[19] O.A. Ali, N. Huebsch, L. Cao, G. Dranoff, D.J. Mooney, Infection-mimicking materialsto program dendritic cells in situ, Nat. Mater. 8 (2009) 151–158.
[20] J. Banchereau, R.M. Steinman, Dendritic cells and the control of immunity, Nature392 (1998) 245–252.
[21] K.P. MacDonald, D.J. Munster, G.J. Clark, A. Dzionek, J. Schmitz, D.N. Hart, Character-ization of human blood dendritic cell subsets, Blood 100 (2002) 4512–4520.
[22] H.C. Probst, K. McCoy, T. Okazaki, T. Honjo, M. van den Broek, Resting dendriticcells induce peripheral CD8+ T cell tolerance through PD-1 and CTLA-4, Nat.Immunol. 6 (2005) 280–286.
[23] R.M. Steinman, D. Hawiger, M.C. Nussenzweig, Tolerogenic dendritic cells, Annu.Rev. Immunol. 21 (2003) 685–711.
[24] D. van Duin, R. Medzhitov, A.C. Shaw, Triggering TLR signaling in vaccination,Trends Immunol. 27 (2006) 49–55.
[25] B. Pulendran, J.L. Smith, G. Caspary, K. Brasel, D. Pettit, E. Maraskovsky, C.R.Maliszewski, Distinct dendritic cell subsets differentially regulate the class of immuneresponse in vivo, Proc. Natl. Acad. Sci. U. S. A. 96 (1999) 1036–1041.
[26] R.A. Maldonado, U.H. von Andrian, How tolerogenic dendritic cells induce regula-tory T cells, Adv. Immunol. 108 (2010) 111–165.
[27] M. Merad, P. Sathe, J. Helft, J. Miller, A. Mortha, The dendritic cell lineage: ontogenyand function of dendritic cells and their subsets in the steady state and the in-flamed setting, Annu. Rev. Immunol. 31 (2013) 563–604.
[28] L.E. Kandalaft, D.J. Powell Jr., C.L. Chiang, J. Tanyi, S. Kim,M. Bosch, K.Montone, R.Mick,B.L. Levine, D.A. Torigian, C.H. June, G. Coukos, Autologous lysate-pulsed dendritic cellvaccination followed by adoptive transfer of vaccine-primed ex vivo co-stimulated Tcells in recurrent ovarian cancer, Oncoimmunology 2 (2013), e22664.
[29] M.J. Clare-Salzler, J. Brooks, A. Chai, K. Van Herle, C. Anderson, Prevention of diabe-tes in nonobese diabetic mice by dendritic cell transfer, J. Clin. Invest. 90 (1992)741–748.
[30] F.J. Hsu, C. Benike, F. Fagnoni, T.M. Liles, D. Czerwinski, B. Taidi, E.G. Engleman, R.Levy, Vaccination of patients with B-cell lymphoma using autologous antigen-pulsed dendritic cells, Nat. Med. 2 (1996) 52–58.
[31] L. Holtl, C. Zelle-Rieser, H. Gander, C. Papesh, R. Ramoner, G. Bartsch, H. Rogatsch,A.L. Barsoum, J.H. Coggin Jr., M. Thurnher, Immunotherapy of metastatic renalcell carcinoma with tumor lysate-pulsed autologous dendritic cells, Clin. CancerRes. 8 (2002) 3369–3376.
[32] J.S. Yu, C.J. Wheeler, P.M. Zeltzer, H. Ying, D.N. Finger, P.K. Lee, W.H. Yong, F.Incardona, R.C. Thompson, M.S. Riedinger, W. Zhang, R.M. Prins, K.L. Black, Vacci-nation of malignant glioma patients with peptide-pulsed dendritic cells elicits sys-temic cytotoxicity and intracranial T-cell infiltration, Cancer Res. 61 (2001)842–847.
[33] T. Taner, H. Hackstein, Z.Wang, A.E. Morelli, A.W. Thomson, Rapamycin-treated, al-loantigen-pulsed host dendritic cells induce ag-specific T cell regulation and pro-long graft survival, Am. J. Transplant. 5 (2005) 228–236.
[34] M.J. Mansilla, C. Selles-Moreno, S. Fabregas-Puig, J. Amoedo, J. Navarro-Barriuso, A.Teniente-Serra, L. Grau-Lopez, C. Ramo-Tello, E.M. Martinez-Caceres, Beneficial ef-fect of tolerogenic dendritic cells pulsed with MOG autoantigen in experimentalautoimmune encephalomyelitis, CNS Neurosci. Ther. 21 (2015) 222–230.
[35] L.C. Harrison, Vaccination against self to prevent autoimmune disease: the type 1diabetes model, Immunol. Cell Biol. 86 (2008) 139–145.
[36] B.G. Keselowsky, C.Q. Xia, M. Clare-Salzler, Multifunctional dendritic cell-targetingpolymeric microparticles: engineering new vaccines for type 1 diabetes, Hum.Vaccin. 7 (2011) 37–44.
[37] N. Giannoukakis, B. Phillips, D. Finegold, J. Harnaha, M. Trucco, Phase I (safety)study of autologous tolerogenic dendritic cells in type 1 diabetic patients, DiabetesCare 34 (2011) 2026–2032.
[38] A.E. Anderson, D.J. Swan, O.Y. Wong, M. Buck, O. Eltherington, R.A. Harry, A.M.Patterson, A.G. Pratt, G. Reynolds, J.P. Doran, J.A. Kirby, J.D. Isaacs, C.M. Hilkens,Tolerogenic dendritic cells generated with dexamethasone and vitamin D3regulate rheumatoid arthritis CD4+ T cells partly via transforming growth factor-beta1, Clin. Exp. Immunol. 187 (2017) 113–123.
[39] J.S. Lewis, C. Roche, Y. Zhang, T.M. Brusko, C.H. Wasserfall, M. Atkinson, M.J. Clare-Salzler, B.G. Keselowsky, Combinatorial delivery of immunosuppressive factors todendritic cells using dual-sized microspheres, J. Mater. Chem. B Mater. Biol. Med.2 (2014) 2562–2574.
[40] A.MartIn-Fontecha, S. Sebastiani, U.E. Hopken,M. Uguccioni, M. Lipp, A. Lanzavecchia,F. Sallusto, Regulation of dendritic cell migration to the draining lymph node: impacton T lymphocyte traffic and priming, J. Exp. Med. 198 (2003) 615–621.
http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0005http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0005http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0010http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0010http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0010http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0010http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0015http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0015http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0015http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0015http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0015http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0020http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0020http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0020http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0025http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0025http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0025http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0025http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0030http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0035http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0040http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0040http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0040http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0040http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0040http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0045http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0045http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0045http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0050http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0050http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0055http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0055http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0055http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0055http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0060http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0065http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0065http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0065http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0065http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0065http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0070http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0070http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0075http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0075http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0075http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0075http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0080http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0085http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0085http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0090http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0090http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0090http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0095http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0095http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0100http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0100http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0105http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0105http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0110http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0110http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0110http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0110http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0115http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0115http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0120http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0120http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0125http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0125http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0125http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0130http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0130http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0135http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0135http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0135http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0140http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0140http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0140http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0140http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0145http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0145http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0145http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0150http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0150http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0150http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0155http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0155http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0155http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0155http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0160http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0160http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0160http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0160http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0160http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0165http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0165http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0165http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0170http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0170http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0170http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0170http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0175http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0175http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0180http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0180http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0180http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0185http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0185http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0185http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0190http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0190http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0190http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0190http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0190http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0195http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0195http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0195http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0195http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0200http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0200http://refhub.elsevier.com/S0169-409X(17)30069-8/rf0200
-
173J.M. Stewart, B.G. Keselowsky / Advanced Drug Delivery Reviews 114 (2017) 161–174
[41] P.J. Tacken, I.J. de Vries, R. Torensma, C.G. Figdor, Dendritic-cell immunotherapy:from ex vivo loading to in vivo targeting, Nat. Rev. Immunol. 7 (2007) 790–802.
[42] J.J. Moon, B. Huang, D.J. Irvine, Engineering nano- and microparticles to tune im-munity, Adv. Mater. 24 (2012) 3724–3746.
[43] K.E. Uhrich, S.M. Cannizzaro, R.S. Langer, K.M. Shakesheff, Polymeric systems forcontrolled drug release, Chem. Rev. 99 (1999) 3181–3198.
[44] F. Danhier, E. Ansorena, J.M. Silva, R. Coco, A. Le Breton, V. Preat, PLGA-based nano-particles: an overview of biomedical applications, J. Control. Release 161 (2012)505–522.
[45] J.A. Champion, A.Walker, S. Mitragotri, Role of particle size in phagocytosis of poly-meric microspheres, Pharm. Res. 25 (2008) 1815–1821.
[46] C. Engman, Y. Wen, W.S. Meng, R. Bottino, M. Trucco, N. Giannoukakis, Generationof antigen-specific Foxp3+ regulatory T-cells in vivo following administration ofdiabetes-reversing tolerogenic microspheres does not require provision of antigenin the formulation, Clin. Immunol. 160 (2015) 103–123.
[47] B. Phillips, K. Nylander, J. Harnaha, J. Machen, R. Lakomy, A. Styche, K. Gillis, L.Brown, D. Lafreniere, M. Gallo, J. Knox, K. Hogeland, M. Trucco, N. Giannoukakis,A microsphere-based vaccine prevents and reverses new-onset autoimmune dia-betes, Diabetes 57 (2008) 1544–1555.
[48] S.T. Reddy, A.J. van der Vlies, E. Simeoni, V. Angeli, G.J. Randolph, C.P. O'Neil, L.K.Lee, M.A. Swartz, J.A. Hubbell, Exploiting lymphatic transport and complement ac-tivation in nanoparticle vaccines, Nat. Biotechnol. 25 (2007) 1159–1164.
[49] S.M. Moghimi, A.C. Hunter, C.M. Dadswell, S. Savay, C.R. Alving, J. Szebeni, Causa-tive factors behind poloxamer 188 (Pluronic F68, Flocor)-induced complement ac-tivation in human sera. A protective role against poloxamer-mediatedcomplement activation by elevated serum lipoprotein levels, Biochim. Biophys.Acta 2004 (1689) 103–113.
[50] S.N. Thomas, E. Vokali, A.W. Lund, J.A. Hubbell, M.A. Swartz, Targeting the tumor-draining lymph node with adjuvanted nanoparticles reshapes the anti-tumor im-mune response, Biomaterials 35 (2014) 814–824.
[51] M. Szajnik, M.J. Szczepanski, M. Czystowska, E. Elishaev, M. Mandapathil, E.Nowak-Markwitz, M. Spaczynski, T.L. Whiteside, TLR4 signaling induced by lipo-polysaccharide or paclitaxel regulates tumor survival and chemoresistance inovarian cancer, Oncogene 28 (2009) 4353–4363.
[52] T. Warger, P. Osterloh, G. Rechtsteiner, M. Fassbender,