Adult Problems in Pediatric Patients 2018/Peds1.pdf · Adult Problems in Pediatric Patients ... ACT...
35
2/20/2018 1 Adult Problems in Pediatric Patients February 21, 2018 Lauren Haney, PharmD, BCPS, BCPPS Clinical Pharmacy Specialist Describe barriers and considerations in anticoagulation therapy in pediatric patients. Discuss options for pulmonary hypertension treatment in pediatric patients. Develop understanding of challenges in pain management in pediatric patients during an opioid epidemic.
Transcript of Adult Problems in Pediatric Patients 2018/Peds1.pdf · Adult Problems in Pediatric Patients ... ACT...

2/20/2018
1
Adult Problems in Pediatric Patients
February 21, 2018
Lauren Haney, PharmD, BCPS, BCPPS
Clinical Pharmacy Specialist
Describe barriers and considerations in anticoagulation therapy in pediatric patients.
Discuss options for pulmonary hypertension treatment in pediatric patients.
Develop understanding of challenges in pain management in pediatric patients during an opioid epidemic.
2/20/2018
2
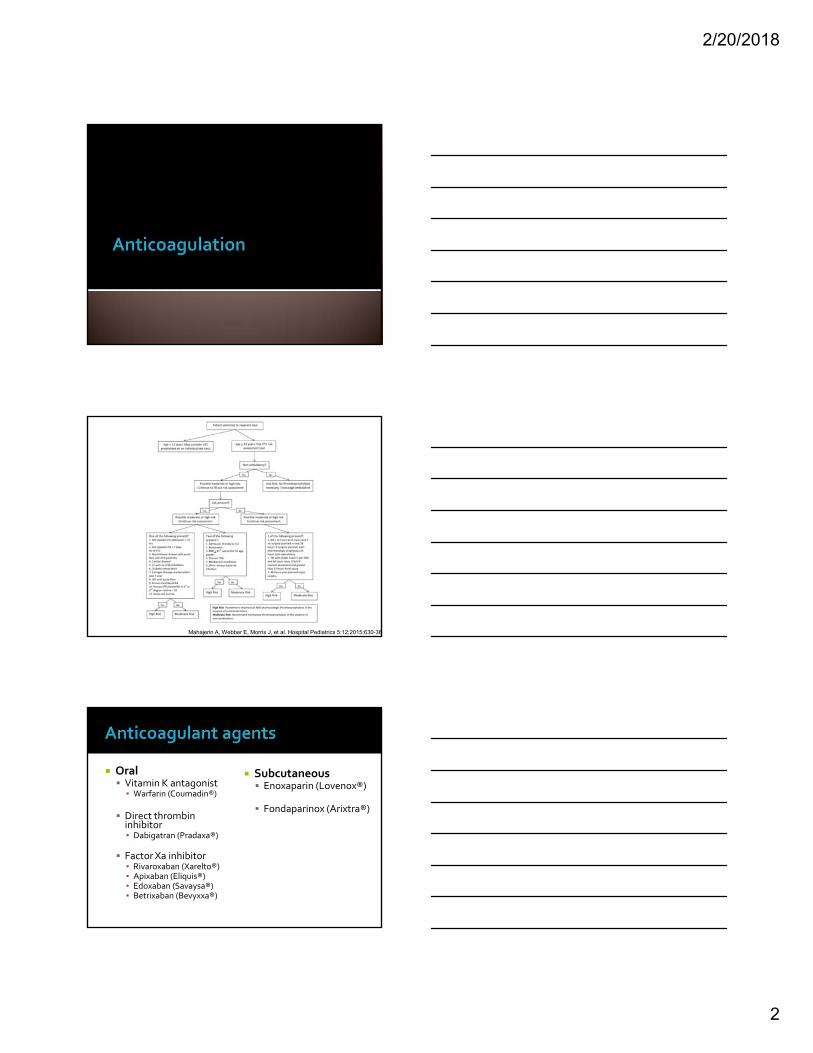
Mahajerin A, Webber E, Morris J, et al. Hospital Pediatrics 5:12;2015:630-36
Subcutaneous Enoxaparin (Lovenox®)
Fondaparinox (Arixtra®)
Oral Vitamin K antagonist▪ Warfarin (Coumadin®)
Direct thrombin inhibitor ▪ Dabigatran (Pradaxa®)
Factor Xa inhibitor ▪ Rivaroxaban (Xarelto®)▪ Apixaban (Eliquis®) ▪ Edoxaban (Savaysa®)▪ Betrixaban (Bevyxxa®)
2/20/2018
3
Vitamin K Antagonist Indications DVT/PE
Nonvalvular atrial fibrillation
Prosthetic heart valves
Mechanism of action: Inhibits coagulation factors II, VII, IX, and X and proteins C and S
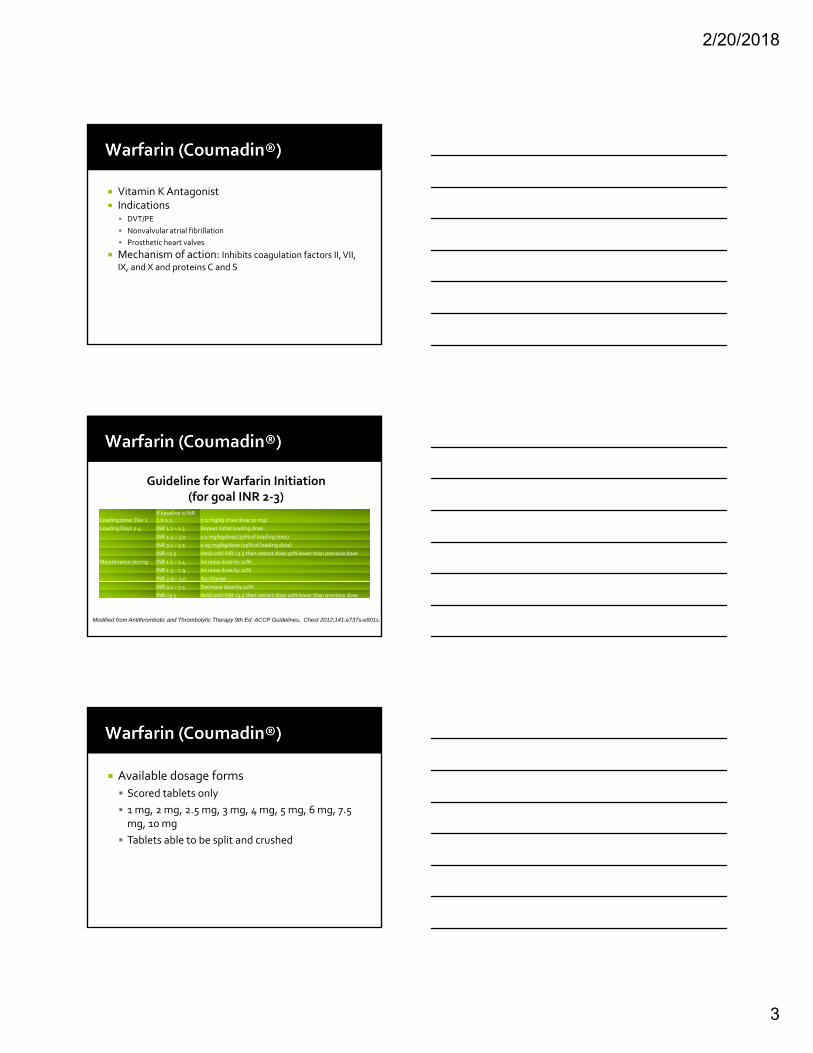
Guideline for Warfarin Initiation (for goal INR 2‐3)
Loading dose: Day 1 If baseline is INR 1.0‐1.3 0.2 mg/kg (max dose 10 mg)
Loading Days 2‐4 INR 1.1 – 1.3 Repeat initial loading dose
INR 1.4 – 3.0 0.1 mg/kg/dose (50% of loading dose)
INR 3.1 – 3.5 0.05 mg/kg/dose (25% of loading dose)
INR >3.5 Hold until INR <3.5 then restart dose 50% lower than previous dose
Maintenance dosing INR 1.1 – 1.4 Increase dose by 20%
INR 1.5 – 1.9 Increase dose by 10%
INR 2.0 – 3.0 No change
INR 3.1 – 3.5 Decrease dose by 10%
INR >3.5 Hold until INR <3.5 then restart dose 20% lower than previous dose
Modified from Antithrombotic and Thrombolytic Therapy 9th Ed: ACCP Guidelines, Chest 2012;141:e737s-e801s.
Available dosage forms
Scored tablets only
1 mg, 2 mg, 2.5 mg, 3 mg, 4 mg, 5 mg, 6 mg, 7.5 mg, 10 mg
Tablets able to be split and crushed
2/20/2018
4
http://www.aboutkidshealth.ca/En/HealthAZ/Drugs/Pages/Warfarin.aspx [accessed 2/14/18]
RISK OF CLOTS
Foods
▪ Vitamin K containing foods
▪ lettuce, spinach, broccoli, cabbage
▪ liver or soybean‐containing food such as mayonnaise, soy milk
RISK OF BLEEDING
Juices
▪ Cranberry, grapefruit and mango can make the medicine too effective and increase risk of bleeding.
https://www.cincinnatichildrens.org/health/w/warfarin [accessed 2/14/18]
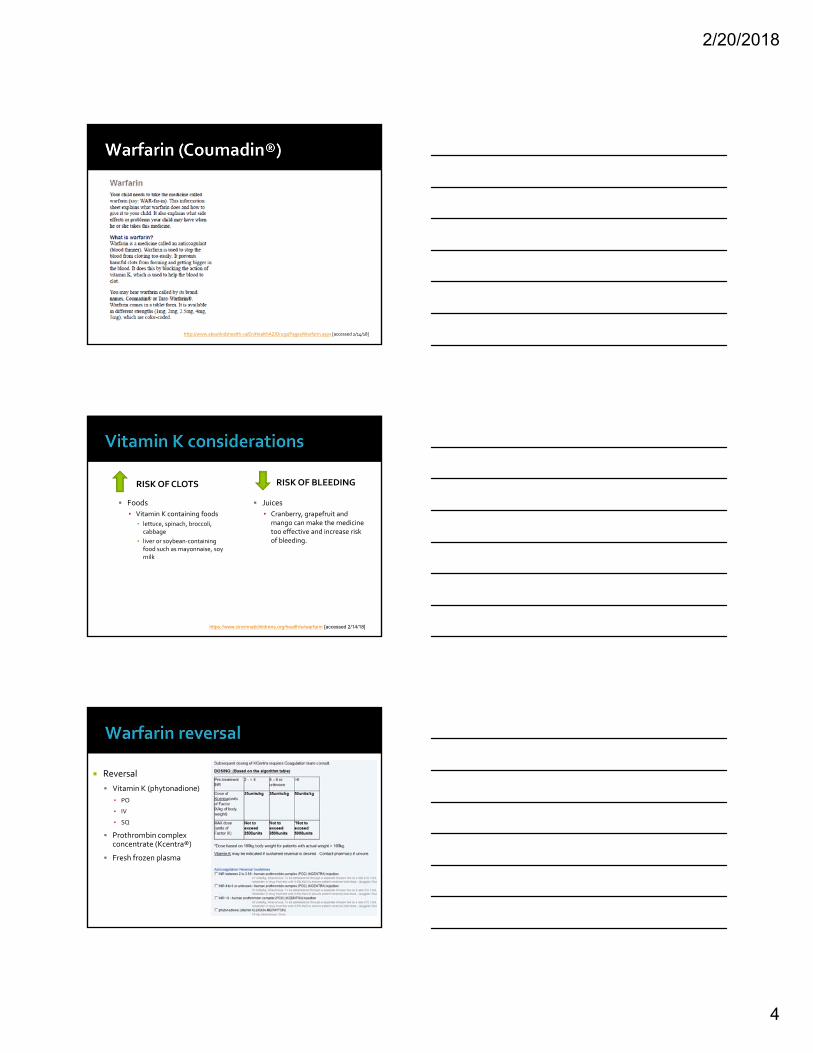
Reversal
Vitamin K (phytonadione)
▪ PO
▪ IV
▪ SQ
Prothrombin complex concentrate (Kcentra®)
Fresh frozen plasma

2/20/2018
5
Oral Factor Xa inhibitor Indications (adult) DVT/PE
Nonvalvular atrial fibrillation
DVT prophylaxis after knee or hip replacement
Mechanism of action: Factor Xa inhibitor causing platelet inactivation and prevents fibrin clot formation
Reversal No specific antidote
Consider Prothrombin complex (FEIBA NF®) or recombinant factor VIIa
NOT dialyzable
Renally eliminated: Avoid use for CrCl < 30 mL/min (PE/DVT and post‐op thrombophrophylaxis) and CrCl < 15 mL/min for atrial fibrillation
Review for drug interactions
Administer with food
Routine monitoring of coagulation tests not required
Monitor for signs & symptoms of bleeding or intolerance to drug
Crushed tablets in water (via NG tube) or applesauce: Stable for ≤4 hours.
Rivaroxaban: Clinical Pearls
Oral Factor Xa inhibitor Indications (Adult) Nonvalvular atrial fibrillation
DVT prophylaxis after knee or hip replacement
Treatment of DVT/PE
Mechanism of action: Factor Xa inhibitor causing platelet inactivation and prevents fibrin clot formation
Reversal
No specific antidote
Consider Prothrombin complex (FEIBA NF®) or recombinant factor VIIa
NOT dialyzable
2/20/2018
6
Oral Factor Xa inhibitor Indications (Adult) Nonvalvular atrial fibrillation
Treatment of DVT/PE
Black Box Warning: reduced efficacy in atrial fibrillation pts with CrCl >95 mL/min
Mechanism of action: Factor Xa inhibitor causing platelet inactivation and prevents fibrin clot formation
Reversal No specific antidote
NOT dialyzable
Dose reduction if weight < 60 kg or CrCl < 50 mL/min
Mechanism of action: small effect on aPTT and strongly inhibit factor Xa
Indications: systemic anticoagulation Monitoring: LMWH heparin AntiXa Special considerations
Contraindications: bleeding
Risks: bleeding
Limitations: bleeding, monitoring, thrombosis, SQ injection
Pharmacokinetics
Half life: 4 to 7 hours
Elimination: 40% urine
Organ dysfunction
▪ Do not use in CrCl <30 mL/min
▪ Hepatic metabolism
▪ Active metabolites Reversal Protamine may be useful but does not completely reverse
effects
2/20/2018
7
Available package sizes
Prefilled syringes
▪ 100 mg/mL concentration: 30 mg, 40 mg, 60 mg, 80 mg, 100 mg
▪ 150 mg/mL concentration: 120 mg and 150 mg
Multidose vial
▪ 100 mg/mL
▪ May need insulin syringes to measure doses ▪ Example: 8 mg = 0.08 mL = 8 units on insulin (100 unit/mL) syringe
▪ Will need prescription for syringes
Subcutaneous injection (not IM) Site of administration
Recommended site
▪ Abdomen: 1‐2 inches away from belly button and scars
Alternative site
▪ Thighs▪ More erratic absorption
Rotate injection sites
To lesson pain and anxiety
Numb injection site with ice
Insuflon catheter
Have patient look away
Self‐administered injections

2/20/2018
8
Counseling points
Great instructional videos on www.lovenox.com
Monitor signs of bleeding and bruising
May experience injection site pain…rotate sites
Best site = abdomen
Store at room temperature (do NOT refrigerate)
Place used syringe in plastic or metal container and place in regular bagged trash for disposal (stickers available from DHEC)
Lexicomp dosing Round dose to nearest commercially‐available syringe when possible.
MAY NEED HIGHER DOSES
Prophylaxis Dose (mg/kg) q12hr
< 2 months 0.75
≥ 2 months 0.5
Treatment
< 2 months 1.5
≥ 2 months 1
Modified from Antithrombotic and Thrombolytic Therapy 9th Ed: ACCP Guidelines, Chest 2012;141:e737s-e801s.
Monitoring AntiXa
Draw 4 to 6 hours after dose administered
Ensure correct lab is ordered
Ranges
▪ Therapeutic 0.5‐1 units/mL
▪ Prophylaxis 0.1‐0.3 units/mL
Monagle P, Chan A, Goldenberg NA, et al, "Antithrombotic Therapy in Neonates and Children: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (9th Edition)," Chest, 2012, 141(2 Suppl):e737-801.

2/20/2018
9
No established dosing in pediatric patients
Mechanism of action: Inhibits Factor Xa and impairs hemostasis by causing inhibition thrombin formation
Indications DVT prophylaxis in patient with history of HIT DVT/PE treatment
Monitoring� Fondaparinux Anti‐Xa levels – draw 3 hours post‐administration of dose Anti‐Xa goals vary based on indication
Dose adjustments� Give 50% of dose if CrCL < 50 mL/min, contraindicated if CrCl < 30 mL/min� If for acute DVT/PE treatment:
�< 50kg: 5mg daily; 50‐100kg: 7.5mg daily,;> 100kg: 10mg daily
Fondaparinux (Arixtra®)
Pharmacokinetics
Half life: 17 to 21 hours
Elimination: 75% urine
Organ dysfunction: prolonged elimination in renal dysfunction
Effects may persist for 2‐4 days after discontinuation
Reversal: NONE
IV
Bivalirudin (Angiomax®)
Argatroban
Oral
Dabigatran (Pradaxa®)
2/20/2018
10
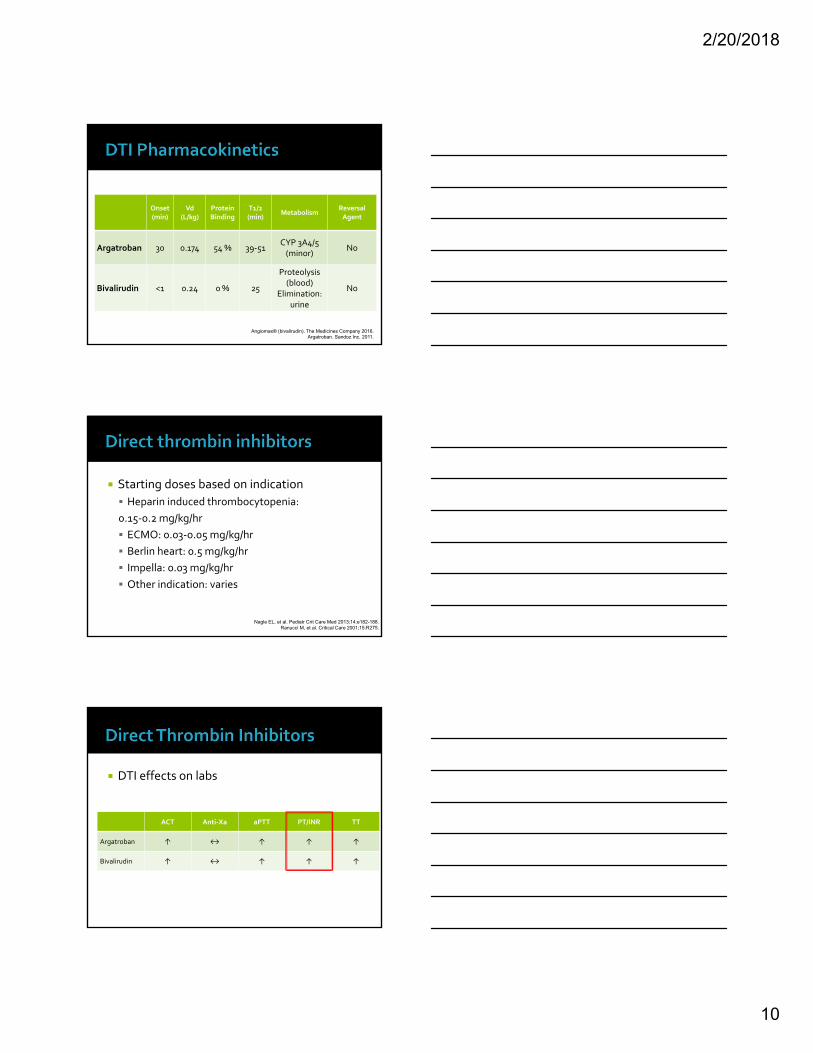
Onset (min)
Vd(L/kg)
Protein Binding
T1/2 (min)
MetabolismReversalAgent
Argatroban 30 0.174 54 % 39‐51CYP 3A4/5 (minor)
No
Bivalirudin <1 0.24 0 % 25
Proteolysis (blood)
Elimination: urine
No
Angiomax® (bivalirudin). The Medicines Company 2016.Argatroban. Sandoz Inc. 2011.
Starting doses based on indication
Heparin induced thrombocytopenia:
0.15‐0.2 mg/kg/hr
ECMO: 0.03‐0.05 mg/kg/hr
Berlin heart: 0.5 mg/kg/hr
Impella: 0.03 mg/kg/hr
Other indication: varies
Nagle EL, et al. Pediatr Crit Care Med 2013;14:e182-188.Ranucci M, et al. Critical Care 2001;15:R275.
DTI effects on labs
Direct thrombin inhibitorsACT Anti‐Xa aPTT PT/INR TT
Argatroban ↑ ↔ ↑ ↑ ↑
Bivalirudin ↑ ↔ ↑ ↑ ↑

2/20/2018
11
INR 2‐3
INR >4
On warfarin for minimum 4‐5 days
INR 4‐5 at time of stopping DTI
Repeat INR 4‐6 hours after stopping infusion
New Oral Anticoagulants/Direct Oral Anticoagulants
(NOAC/DOAC) Dabigatran (Pradaxa®)
Rivaroxaban (Xarelto®)
Apixaban (Eliquis®)
Edoxaban (Savaysa®)
Oral Anticoagulant Agents
NEW
Oral direct thrombin inhibitor (DTI)
Indications (adult)
▪ Anticoagulation therapy in patients with non‐valvular atrial fibrillation
▪ DVT/PE
▪ Mechanism of action: Inhibits free and bound thrombin causing activation of factors V, VIII, XI, and XIII and inhibiting platelet aggregation
Reversal▪ Idarucizumab (Praxbind ®)
▪ Consider Prothrombin complex (FEIBA NF®) or recombinant factor VIIa
▪ Partially dialyzable
Dabigatran (Pradaxa®)
2/20/2018
12
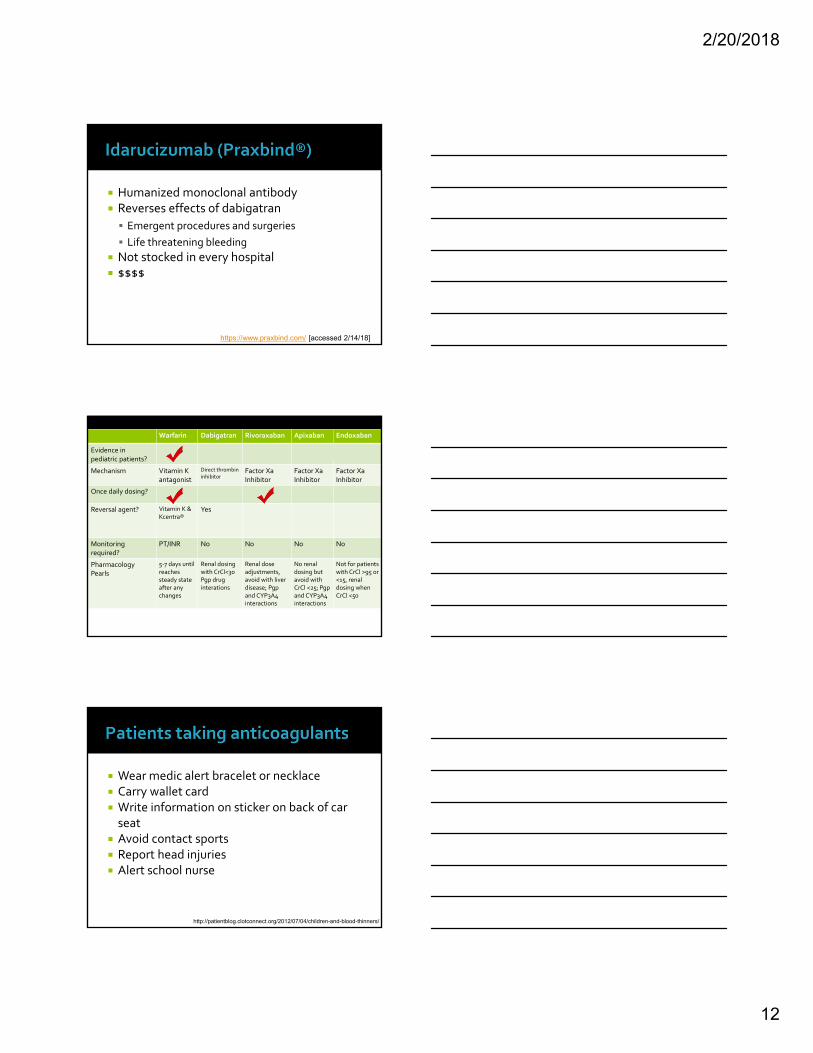
Humanized monoclonal antibody Reverses effects of dabigatran
Emergent procedures and surgeries
Life threatening bleeding
Not stocked in every hospital $$$$
https://www.praxbind.com/ [accessed 2/14/18]
Warfarin Dabigatran Rivoraxaban Apixaban Endoxaban
Evidence in pediatric patients?
Mechanism Vitamin K antagonist
Direct thrombin inhibitor
Factor XaInhibitor
Factor XaInhibitor
Factor XaInhibitor
Once daily dosing?
Reversal agent? Vitamin K & Kcentra®
Yes
Monitoring required?
PT/INR No No No No
PharmacologyPearls
5‐7 days until reaches steady state after any changes
Renal dosing with CrCl<30Pgp drug interations
Renal dose adjustments, avoid with liver disease; Pgpand CYP3A4 interactions
No renal dosing but avoid with CrCl <25; Pgpand CYP3A4 interactions
Not for patients with CrCl >95 or <15, renal dosing when CrCl <50
Wear medic alert bracelet or necklace Carry wallet card Write information on sticker on back of car seat
Avoid contact sports Report head injuries Alert school nurse
http://patientblog.clotconnect.org/2012/07/04/children-and-blood-thinners/
2/20/2018
13
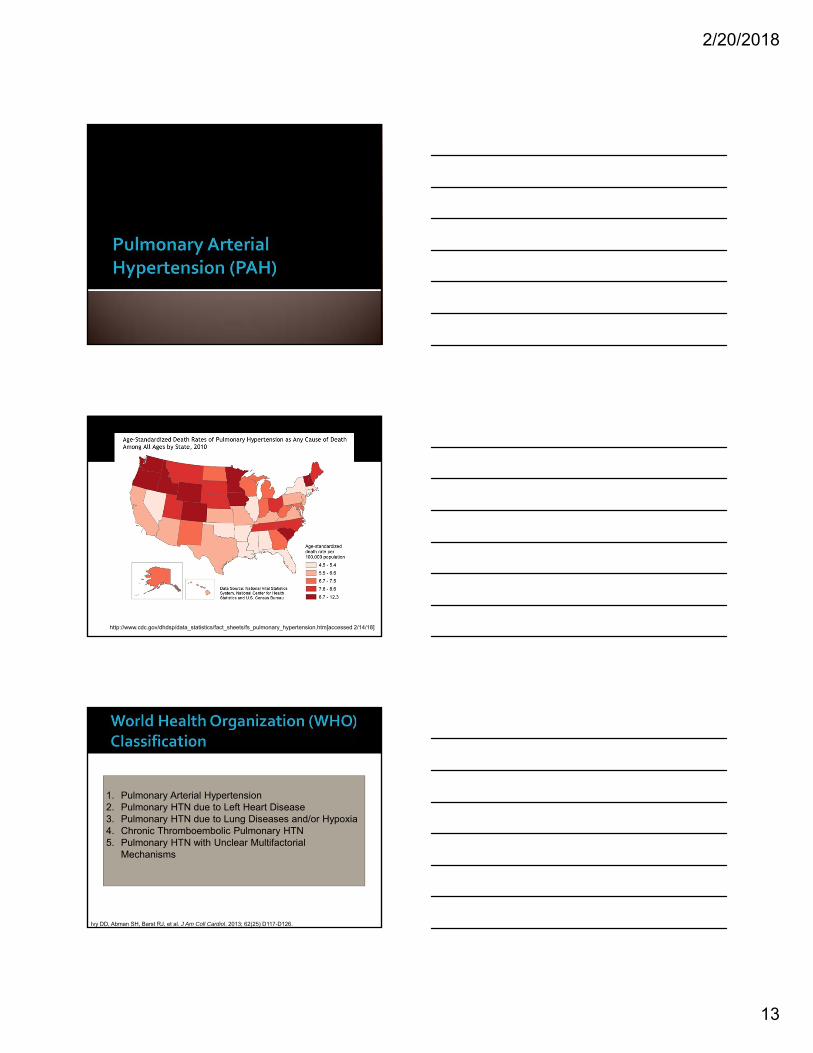
http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_pulmonary_hypertension.htm[accessed 2/14/18]
1. Pulmonary Arterial Hypertension2. Pulmonary HTN due to Left Heart Disease3. Pulmonary HTN due to Lung Diseases and/or Hypoxia4. Chronic Thromboembolic Pulmonary HTN5. Pulmonary HTN with Unclear Multifactorial
Mechanisms
Ivy DD, Abman SH, Barst RJ, et al. J Am Coll Cardiol. 2013; 62(25) D117-D126.
2/20/2018
14
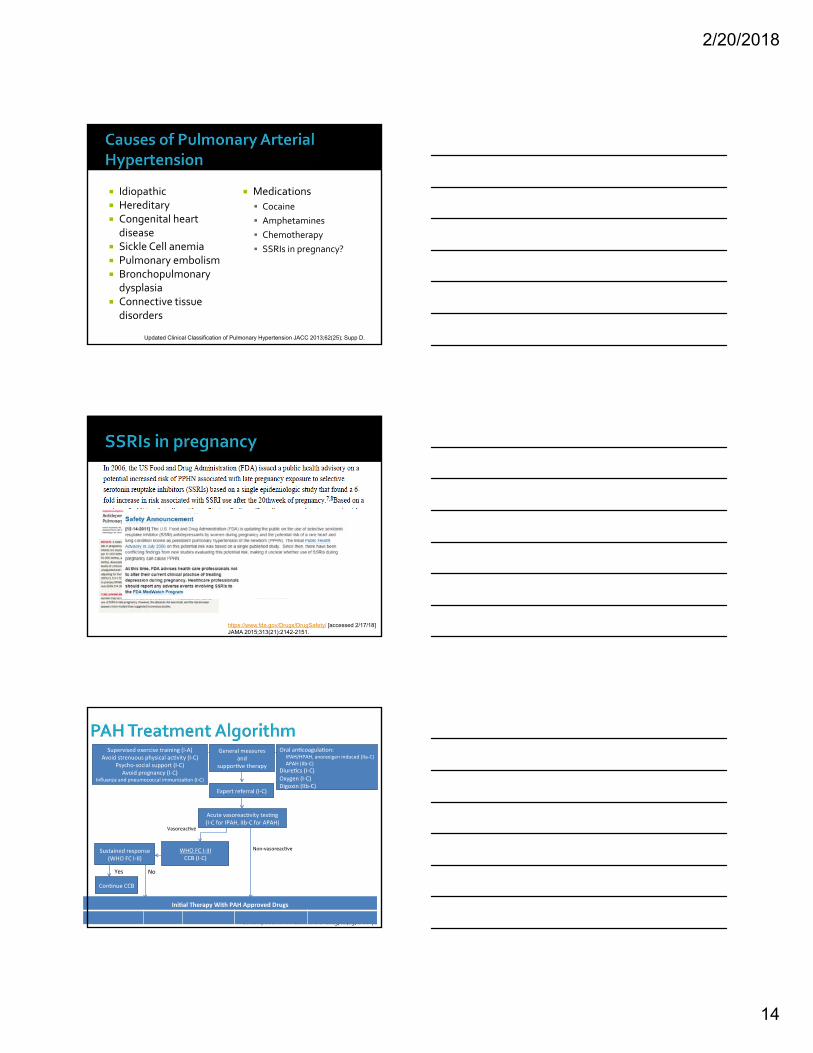
Idiopathic Hereditary Congenital heart disease
Sickle Cell anemia Pulmonary embolism Bronchopulmonary dysplasia
Connective tissue disorders
Medications
Cocaine
Amphetamines
Chemotherapy
SSRIs in pregnancy?
Updated Clinical Classification of Pulmonary Hypertension JACC 2013;62(25); Supp D.
https://www.fda.gov/Drugs/DrugSafety/ [accessed 2/17/18]JAMA 2015;313(21):2142-2151.
Galiè N, et al. J Am Coll Cardiol 2013;62(25):D60‐72
2/20/2018
15
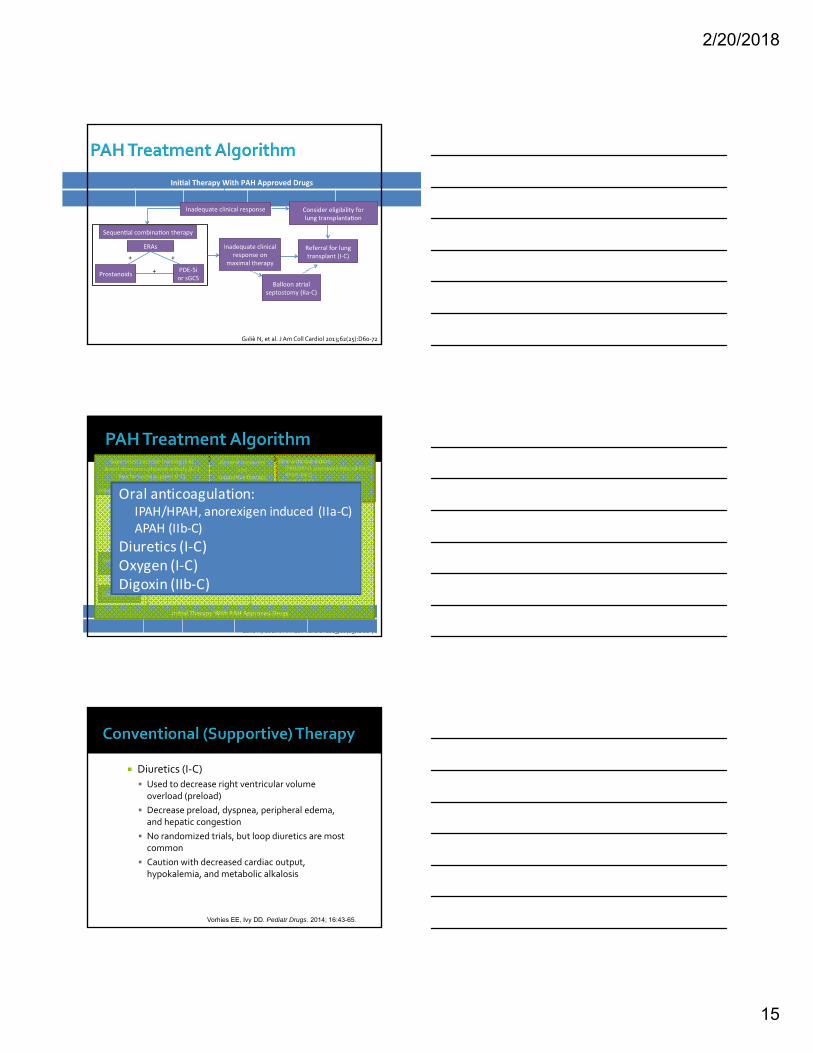
Galiè N, et al. J Am Coll Cardiol 2013;62(25):D60‐72
Galiè N, et al. J Am Coll Cardiol 2013;62(25):D60‐72
Oral anticoagulation: IPAH/HPAH, anorexigen induced (IIa‐C)APAH (IIb‐C)
Diuretics (I‐C)Oxygen (I‐C)Digoxin (IIb‐C)
Diuretics (I‐C)
Used to decrease right ventricular volume overload (preload)
Decrease preload, dyspnea, peripheral edema, and hepatic congestion
No randomized trials, but loop diuretics are most common
Caution with decreased cardiac output, hypokalemia, and metabolic alkalosis
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.

2/20/2018
16
Anticoagulation (IIa‐C or IIb‐C)
High risk for intrapulmonary thrombosis and thromboembolism (sluggish blood flow, dilated chambers, venous stasis, and sedentary lifestyle)
Should be considered in:
▪ WHO Groups 1 (PAH) and 4 (CTEPH)
▪ Advanced disease (continuous IV therapy)
▪ High risk of VTE (HF, sedentary lifestyle, thrombophilic predisposition)
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.
Anticoagulation (IIa‐C or IIb‐C)
Warfarin
▪ Retrospectively shown to improve survival
▪ Goal INR 1.5 – 2.5 based on 2 small studies (retrospective and prospective)
▪ Bleeding risk may be higher in certain subsets (e.g., connective tissue disease APAH)
Limited data with DOACs
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.
Digoxin (IIb‐C)
Controversial use as an adjunct for right heart failure or atrial arrhythmias
▪ Improves RVEF in Group 3 PH due to COPD
▪ No data in Group 1 PAH
▪ Possibly more sensitive to toxicity
Goal level unknown, but probably should be 0.5 –0.8 ng/mL
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.

2/20/2018
17
Phosphodiesterase-5 Inhibitors
Endothelin Receptor
Antagonists
Prostacyclin and
Analogues
• Sildenafil (Revatio®)• Tadalafil (Adcirca®)
• Bosentan (Tracleer®)• Ambrisentan (Letairis®)
• Epoprostenol (Flolan®, Veletri®)• Treprostinil (Remodulin®, Tyvaso®)• Iloprost (Ventavis®)
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.
Inhibit PDE5 in vascular smooth muscle
Inhibits cGMP breakdown → increasing local NO
Vasodilation and inhibition of smooth muscle cell growth
Improves hemodynamics, functional class, and quality of life
Easier to administer
Vorhies EE, Ivy DD. Pediatr Drugs. 2014; 16:43-65.
Sildenafil (Revatio®)
Dosage forms
▪ 20 mg tablets ($900 for 45 tablets)
▪ 10 mg/mL suspension commerically available ($9000/bottle)
Likely requires prior authorization
Tadalafil (Adcirca®)
Available as tablets only ($2100 for 30 tablets)
Compounded suspension recipe
Lexicomp

2/20/2018
18
Sildenafil
Pediatrics: 0.5‐1 mg/kg PO q6‐8hr (max 20 mg)
Adults: Sildenafil started at 20 mg PO TID
Give doses 4 – 6 hrs apart
Tadalafil
Pediatrics: 15‐40 mg PO daily
Adults: 40 mg PO daily
Decrease to 20 mg PO daily if CrCl <80 mL/min
Avoid if CrCl <30 mL/min or on hemodialysis
LexiComp Sabri RM, et al. Pediatr Cardiol (2014) 35:699–704
Sildenafil Tadalafil
Headache ✔� ✔�
Flushing ✔� ✔�
Nasal congestion ✔� ✔�
Dyspepsia ✔� ✔�
Dizziness ✔�
Epistaxis ✔�
Visual disturbance(blue‐tint, sudden loss)
✔�
Rash ✔�
Sudden decrease or loss of hearing
✔�
Myalgia ✔�
Nausea ✔�
Contraindicated with nitrates or riociguat due to potential severe hypotension
PDE‐5 degrades cGMP
Additive vasodilatory effects of nitric oxide

2/20/2018
19
www.fda.gov [accessed 2/17/18Revatio package insert Jan 2014
Sildenafil Citrate in Treatment‐Naïve Children with Pulmonary Arterial Hypertension
Primary objective: Assess sildenafil effectiveness on exercise capacity
• Measured peak oxygen consumption (PVO2) at week 16
• Assessed 106 of 235 patients using Cardiopulmonary Exercise Test (CPET)
• Limited due to developmental functionality of patients
• Patients on monotherapy
Secondary objectives: Change from baseline to week 16• Pulmonary artery pressure (PAP)
• Pulmonary vascular resistance index
• WHO functional class
• Cardiac index
• Right atrial (RA) pressure
• Exercise duration
• Child Health Questionnaire
Barst RJ, Ivy D, Gaitan G, et al. Circ 2012;125:324-334.
o Patient heterogeneityo Differences in ageo Etiology of disease (IPAH and HPAH compared to secondary
PAH)o Infant population: PAH secondary disease processo Variable WHO functional class
o Primary outcomeo Difficult to accurately measure in majority of patients
o Overall survival o 3 year survival is higher than without treatment o Natural disease progression: Median survival is 10 months o No deaths were thought to be treatment relatedo No explanation in pharmacokinetic differences
Barst RJ, Ivy D, Gaitan G, et al. Circ 2012;125:324-334.

2/20/2018
20
• After 2 years of treatment
• Increased risk of death in high dose group
Barst RJ, Ivy D, Gaitan G, et al. Circ 2012;125:324-334.
If sildenafil is not safe….
Block vasoconstriction and cellular proliferation caused by endothelin‐1 (ET‐1)
Improve exercise capacity, functional class, hemodynamics and delay clinical worsening
Efficacy of dual ETA and ETB and selective ETAreceptor antagonists appear comparable
Dual (or nonselective): bosentan, macitentan
Selective ETA: ambrisentan

2/20/2018
21
To initiate
Discuss indication, dosing, and length of treatment with primary patient care team
Contact and assist case manager about insurance and acquisition for home (usually takes 7‐10 business days)
Verify approval for home supply BEFORE initiating therapy inpatient
Discuss implications with family for home use (ie, cutting tablets, teratogen)
Refer to website for Patients on maintenance therapy
ERA Starting Dose Target DoseDose
Reduction
Bosentan 62.5 mg PO BID x4 weeks
125 mg PO BID LFTs 3‐5x ULN
Ambrisentan 5 mg PO daily 10 mg PO daily Concomitant cyclosporine
Macitentan 10 mg PO daily 10 mg PO daily None
• All 3 ERAs may be taken with or without food
• Bosentan is a potent CYP 3A4 and 2C9/19 inducer
Lexicomp
FIXED DOSING
5 to <10 kg: 15.6 mg daily for 4 weeks; increase to 15.6 mg BID
10 to 20 kg: 31.25 mg daily for 4 weeks; increase to 31.25 mg BID
>20 to 40 kg: 31.25 mg BID for 4 weeks; increase to 62.5 BID
>40 kg: 62.5 mg BIDfor 4 weeks; increase to 125 mg BID
WEIGHT‐BASED DOSING
Children ≥2 years: Initial: 0.75 to 1 mg/kg/dose twice daily for 4 weeks (maximum dose: 62.5 mg); then increase to 2 mg/kg/dose twice daily
Lexicomp

2/20/2018
22
Wear gloves and mask when cutting and handling tablets.
Use a pill cutter to cut the tablet. Store the unused tablet pieces in the original bottle from the manufacturer for up to 4 weeks.
Bosentan tablets should not be crushed. Place the split tablet in 5 mL of water and allow to dissolve. Do not crush.
If women who are pregnant or may become pregnant do not handle the split tablets with bare hands.
www.tracleer.com [accessed 1/20/18]
Serious liver injury Bosentan: black box warning
Dose‐dependent and reversible hepatocellular damage and increased total bilirubin
Liver function tests (LFTs) prior to initiation and monthly thereafter
▪ Avoid initiation or dose adjust if AST/ALT >3x ULN
▪ D/C if AST/ALT elevated with symptoms (N/V, fever, abdominal pain, jaundice, lethargy) or bili ≥2x ULN
www.tracleer.com [accessed 1/20/18]
Peripheral edema (most common for all) Anemia
CBC at baseline, 1, and 3 months and Q3 months
Male infertility
Testicular tubular atrophy and infertility
Decreased sperm counts
Embryo‐fetal toxicity Pregnancy tests in women of childbearing potential
▪ Prior to initiation of therapy
▪ Monthly during therapy
Counsel to use 2 forms of contraceptives
www.tracleer.com [accessed 1/20/18]
2/20/2018
23
Embryo‐fetal toxicity ‐ likely to cause major birth defects
Pregnancy tests in women of childbearing potential
Prior to initiation of therapy (at least 11 days after last unprotected sexual intercourse)
Monthly during therapy
Counsel to use 2 forms of contraceptives
Hormonal methods less effective with bosentan
www.tracleer.com [accessed 1/20/18]
Two‐fold mechanism
Stimulate NO receptor
Increase sensitivity of soluble guanylate cyclase to endogenous NO
Improves exercise capacity, hemodynamics, and symptoms
Riociguat (Adempas®)
Syncope (most common) Headache, dizziness Hypotension (C/I with concomitant PDE‐5i or nitrate therapies)
Dyspepsia Peripheral edema Vomiting, diarrhea Embryo‐fetal toxicity

2/20/2018
24
Restores inadequate levels of prostaglandin I2 (prostacyclin)
Potent vasodilation of pulmonary vasculature Improve hemodynamics, functional class, and in IPAH patients also survival
IV
Epoprostenol (Flolan® or Veletri®)
Treprostinil (Remodulin®)
Subcutaneous
Treprostinil (Remodulin®)
Inhaled
Treprostinil (Tyvaso®)
Iloprost (Ventavis®)
Oral
Selexipag (Uptravi®)
Newer, more stable, longer half life Dosing
SQ (preferred) or IV therapy usually started at 1.25 ng/kg/min
Decrease to 0.625 ng/kg/min if not tolerated and do not re‐titrate for 4 weeks
Increase by ≤ 1.25 ng/kg/min weekly for first 4 weeks, then by ≤ 2.5 mg/kg/min
Transition from epoprostenol: start at 10% of epoprostenol dose and increase by 1.25 ng/kg/min but ≤ 2.5 ng/kg/min per week

2/20/2018
25
Alternative to parenteral in patients who refuse or cannot tolerate the complexity of those agents
Avoid in patients with pulmonary infections or lung disease
Dosing: Start with 3 breaths (18 mcg) 4 times daily while awake (~4 hrs apart)
Reduce to 1‐2 breaths if not tolerated
Increase by 3 breaths at 1‐2 week intervals
Goal dose is 9 breaths (54 mcg) 4 times daily
Alternative to parenteral in patients who refuse or cannot tolerate the complexity of those agents
WHO FC III [I‐A or B] or IV [IIa‐C] who have failed or are not candidates for CCBs
Avoids infectious complications associated with IV access for drug delivery
Start at 2.5 mcg inhaled 6 – 9 times daily (≥2 hour intervals while awake)
Increase to 5 mcg 6 – 9 times daily (max 45 mcg/day)
Must use AAD aerosolized device
Selective agonist of prostacyclin‐IP receptor Smooth muscle vasodilation, inhibition of smooth muscle proliferation, and inhibition of platelet aggregation
Easy to administer WHO Group 1 FC II‐III Decreased time to first event by 40%
First event: disease progression, hospitalization, PAH worsening, or all‐cause death
No current recommendation for use
2/20/2018
26
Pharmacokinetics
99% protein bound
Metabolized by CYP 3A4 and 2C8
Major active metabolite
Adult Dosing
Initially 200 mcg PO BID
Increase weekly in BID increments of 200 mcg
Max dose 1600 mcg PO BID
Re‐titration required if interrupted for ≥ 3 days
Once daily for mod hepatic impairment (CP Class B)
Similar to prostanoids… Headache
Diarrhea
Nausea
Jaw pain
Pain in extremities
Myalgia
Arthralgia
Flushing Avoid use with severe hepatic impairment (Child Pugh Class C)

2/20/2018
27
Drug overdoses leading cause of accidental death
Opioid deaths in US 2015
▪ Heroin: 12,990 deaths
▪ Prescription opioids: 20,100 deaths
https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis [accessed 2/18/18]
CDC press release – November 11, 2001
Death toll tripled in previous decade
In US, 40 people die every day from opioid pain relievers
In 2010‐ 1:20 people ≥12 years old admits to using prescription pain medication non‐medically
5,500 people START to misuse pain medications EVERY DAY
78.5 BILLION dollar burden per year in US
https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis [accessed 2/18/18]
Opioid prescription fill rates
Illinois has lowest rate
Florida has highest rate
Overdose deaths
Nebraska has lowest rate
New Mexico has lowest rate
https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis [accessed 2/18/18]

2/20/2018
28
In 2016
3.9 million adult estimated in SC
5 million opioid prescriptions filled in SC
Equals 1.3 opioid prescriptions per adult
https://www.census.gov/quickfacts/SC [accessed 2/19/18]
Access
In 2012, 259 million prescriptions written for opioid pain reliever = enough to give every American adult a bottle
Doctor shopping “Pill mills” Sharing and saving
ASAM Opioid Addiction Facts and Figures 2016
In 2015
276,000 adolescents were current nonmedical users of pain reliever
122,000 addicted to prescription pain relievers
21,000 adolescents had used heroin in the past year, and 5,000 were current heroin users
ASAM Opioid Addiction Facts and Figures 2016
2/20/2018
29
Where does it come from?
Given to them for free by a friend or relative
Prescribing rates for prescription opioids among adolescents and young adults nearly doubled from 1994 to 2007
ASAM Opioid Addiction Facts and Figures 2016
Talk about it!
Pain medications in homes
Safe storage
Disposal
Prescribing
Only give enough supply for minimal pain
Promote distraction techniques
Set expectations
South Carolina Reporting and Identification Prescription Tracking Program
Monitors transactions to discourage abuse and diversion
Allows exchange of information with participating states

2/20/2018
30
December 18, 2017
SC Public Health Emergency declared by Gov. Henry McMaster
Effort to decrease opioid abuse in SC
Limit days supplies
Return to prescriber if additional supply needed
http://www.thestate.com/news/politics-government/article190314649.html [accessed 2/19/18]
https://www.scdhec.gov/Health/Opioids/ [accessed 2/18/18]
EMS and First responders in SC
Naloxone administration
4,600 times in 2015
6,400 times in 2016
Increase of 39% in just one year
https://www.scdhec.gov/Health/Opioids/ [accessed 2/18/18]

2/20/2018
31
2015 2016
https://www.scdhec.gov/Health/Opioids/ [accessed 2/18/18]
Prescription Auto –injector
Evzio®
Prescription Nasal Spray
Narcan®
https://www.evzio.com/patient/https://www.narcan.com/ [accessed 2/19/18]
Where to get naloxone
Retail pharmacies (including CVS and Walgreens)
Naloxone is available without a prescription in 41 states
AL, AK, AR, AZ, CA, CO, CT, FL, GA, IA, ID, IL, IN, KY, LA, MA, MD, MN, MO, MS, MT, NC, NH, ND, NJ, NM, NV, NY, OH, OR, PA, RI, SC, TN, TX, UT, VA, VT, WA, WI and WV
https://www.cvs.com/content/prescription-drug-abuse/save-a-life
2/20/2018
32
JAMA
60% report leftover opioids in the past year
20% report sharing medications with others
Do NOT flush down toilet to keep out of water supply
Mix with liquid or deterrant such as coffee grounds or cat liter
Place in regular household garbage for disposal
Unwanted medications (NOT controlled substances)
Retails pharmacies
▪ CVS 1‐888‐607‐4287
▪ Rite Aid 1‐800‐748‐3243
▪ Walgreens 1‐800‐925‐4733
Local government take back programs
Local hospitals
2/20/2018
33
Widely used opioid in pediatric patients for decades
In 2007: pediatric death reported attributed to cytochrome P2 CD6 polymorphism
In 2009: 2 year old previously healthy child die after tonsillectomy
In 2013: World Health Organization (WHO) removed codeine from pediatric pain guidelines

2/20/2018
34
2013: American, European, Canadian, and British warnings issued about use of codeine in pediatric patients
2015: Australia issues contraindication for patients <12 years of age
2016: American Academy of Pediatrics issues statement that further investigation needed
FDA summary memorandum. The safety of codeine in children 18 years of age and younger. Silver Spring, MD: Joint Pulmonary Allergy Drugs and Drug Safety and Risk Management Advisory Committee, 2015.www.AAP.org [accessed 11/18/17]
Codeine is metabolized to morphine through CYP2D6 enzyme
Altered metabolism may lead to respiratory depression
High risk patients
Breastfed babies
Post Tonsillectomy and Adenoidectomy
Ultra rapid CYP2D6 metabolizers
Crews KR. Clin Pharmacol Ther 2014;95(4):376-82.
http://www.aappublications.org/news/2017/04/20/Codeine042017 [accessed 11/18/17]

2/20/2018
35
Obesity
Gout
Hypertension Diabetes
Depression
Infection
Hyperlipidemia
Kidney disease