Adult Liver Transplantation Michael J. Moritz, M.D. Drexel University College of Medicine.
42
Adult Liver Transplantation Michael J. Moritz, M.D. Drexel University College of Medicine
-
Upload
rhoda-walsh -
Category
Documents
-
view
216 -
download
0
Transcript of Adult Liver Transplantation Michael J. Moritz, M.D. Drexel University College of Medicine.

Adult Liver Transplantation
Michael J. Moritz, M.D.
Drexel University College of Medicine

Case Presentation:16yo HF transferred to HUH
• History
• 2 wks of lethargy, anorexia, nausea
• ? days of dark urine, light stools
• 2 days of jaundice

ER
• Encephalopathy
• Dense icterus, mild ascites, splenomegaly, edema
• Elevated LFT’s, total bilirubin 30mg/dL
• Anemia, thrombocytopenia, coagulopathy
• Oliguria and elevated creatinine

Diagnostic Testing
• 1) Ultrasound– Cirrhosis, patent portal vein with hepatopetal flow, edematous gall
bladder
• 2) Blood tests– Ceruloplasmin, serum copper
• 3) Specialty exam– Slit lamp with Kayser-Fleischer rings
• 4) Bx– Copper content per gram of liver tissue
• 5) Specific confirmatory testing– Urinary copper excretion, gene analysis

Wilson’s Disease
• Copper overload• Defective ATP7B copper transmembrane
transporter in the Golgi apparatus• Copper not appropriately transferred out of
hepatocytes to ceruloplasmin and bile• Accumulates in liver, CNS, red cells, bone• Fulminant (hepatic) vs. chronic (neuropsychiatric)
presentation• Gene frequency 1:90
Homozygosity 1:30,000

Wilson’s Disease Medical Treatment
• Copper chelation: trientene, D-penicillamine, tetrathiomolybdate
• Zinc supplementation
• Low copper diet (avoid organ meats, shellfish, dried beans, peas, whole wheat, chocolate,…)

Wilson’s DiseaseTransplantation
• Corrects the genetically defective liver
• Life long immunosuppression
• Indications: FHF or Chronic Liver Dz

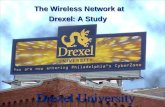
Explant—FHF Wilson’s Disease

Liver Transplantation
• Liver transplantation is the OPTIMAL treatment for end stage liver disease (ESLD)
• ESLD has 2 forms: Acute and Chronic
• Acute=Fulminant Hepatic Failure
• Chronic=Cirrhosis

Common Diagnoses in Liver Tplt. Pts. Last 118 Pts. 1°Dx 2°Dx
Hepatitis C 50%
Alcoholism 13% 12%
Cryptogenic 9%
FHF, Autoimmune 7%
PBC 4%
Hepatitis B 3% 4%
PSC 3%
HCC 7%

Less Common Diagnoses in Adults for Liver Transplantation
• Wilson’s Dz—acute and chronic
• Hemachromatosis
• Budd-Chiari Syndrome
• Congenital Hepatic Fibrosis
• Polycystic Disease
• Inborn errors of metabolism
• Familial Amyloidotic Polyneuropathy

Fulminant Hepatic Failure (FHF)
• Synonymous with Acute Liver Failure
• Definition: Development of encephalopathy within ~8 weeks of the onset of symptoms or within ~2 weeks of the onset of jaundice
• Pathology: Panlobular or Submassive necrosis

Causes of FHF
• Idiopathic
• Acetaminophen toxicity
• Hepatitis B, A, E, other viruses
• Drug reactions (INH, halothane, others)
• Wilson’s Disease
• Mushroom poisoning

FHF-Clinical Manifestations
• Encephalopathy
• Coagulopathy
• Hypoglycemia
• Cerebral edema
• Sepsis—Multiorgan Failure

FHF-Prognosis
• A race between progressive liver failure and its complications vs. liver regeneration
• Age
• Etiology
• Rapidity of onset

FHF-Treatment
• Supportive ICU care
• Support of renal fxn, plasmaphoresis
• ICP monitoring
• Transplantation

Chronic Liver Disease—Indications for Transplantation
• Ultimately, the decision to transplant is based upon the patient’s likelihood of survival
• Survival with transplantation:– One-year ~85-90%– Two-year ~80-88%– Five-year ~65-75%

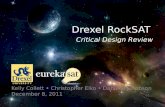
Patient Survival After Primary Liver Transplantation
0
10
20
30
40
50
60
70
80
90
100
0 12 24 36 48 60
Time (months)
Su
rviv
al (
%)
1984-2001 n=384
1991-2001 n=299
1995-2001 n=186

Chronic Liver Disease—Indications for Transplantation
• Ascites
• Encephalopathy
• Portal Hypertensive Bleeding
• Hepatocellular Carcinoma in the setting of Cirrhosis

Chronic Liver Disease—Indications for Transplantation
• Ascites– Ascites has a two-year mortality of 50%– SBP has a two-year mortality of 80%
• Usual treatment-diuretics; when severe-Large Volume Paracentesis with Albumin Replacement
• At its end stage, ascites and resultant ARF is called HepatoRenal Syndrome

Requirements for Transplantation
• End stage liver disease
• Physiologic ability to tolerate surgery– Cardiac, pulmonary, renal, cerebral function
• Portal inflow
• Social support
• No extrahepatic infection or malignancy
• Alcohol abstinence for 6 months

Contraindications
• Age>70?
• Cardiac-pulmonary-renal-cerebral function
• Inability to safely be immunosuppressed
• Substance problems– EtOH, tobacco, opiate analgesics, illicit drugs
• Social problems

Hepatitis C-Natural History
• Approx. 3 million infected in the US
• Only 25% of infected individuals develop cirrhosis
• Median--innoculation to cirrhosis=20years
• Median—innoculation to HCC=30 years, prevalence of HCC unknown

Hepatitis C and Liver Transplantation
• Near universal recurrence of viremia at high levels, 40% with hepatitis at one-year (bx)
• 40% with or mild hepatitis-negligible risk
• 40% with moderate hepatitis-not in <5years
• 20% with severe hepatitis and cirrhosis within 5 years of transplantation

Hepatitis C and Liver Transplantation-New News
• The newest interferons (Pegylated interferon and consensus interferon) plus ribavirin have a 15-20% Sustained Viral Response in post-transplant patients!

Alcoholic Cirrhosis
• Alcoholics have a post-tplt prognosis no different from patients with other diagnoses
• Risk of Recidivist Drinking– 10% pathologic drinking within one year
• Predictors of Increased Risk Recidivism– Abstinence<6 months– Psychiatric dx, character disorder– Polysubstance abuse

Liver Transplant--Numbers
• UNOS Waiting List 17,231 (2/8/05)• 5,657 Cadaver donor liver transplants in
from 6,549 cadaver donors (2004)• 298 Living donor liver transplants (2004)• Waiting list mortality~15%
– Cirrhotic complications– Progression HCC– Substance and social issues

Donor Liver

Donor Liver

Diagram of Piggyback Orthotopic Liver Transplant

Schematic of Venovenous Bypass

Liver Transplantation: Outcomes
• Patient Survival at 1, 3, and 5 years86% 78% 72%
• Graft Survival81% 71% 64%
• Immunosuppression/Tolerance
• Recurrent Dz
• Immunosuppressive risks

Review—Liver Transplantation
• Diagnoses—acute, chronic
• Indications and contraindications
• Hepatitis C, Alcohol
• Insufficient numbers of cadaver donors to meet demand



Conclusions
• With appropriately selected patients, Liver Transplantation offers an excellent chance for long-term, good quality of life survival for patients facing death from ESLD
• Post-transplant Recurrent Hepatitis C is the largest clinical problem at present
• Donors are in short supply

Organ Allocation for Adults
• Status 1– FHF, Acute Wilson’s Disease– Early Post-transplant Complications:
PNF, HAT <7 Days– Allocated by Waiting Time, Blood Group
• Status 2– All Others– Allocated by MELD Score– Waiting Time at that score as tie breaker

MELD Score
• R=9.57ln(creat)+3.78ln(bili)+11.2ln(INR)+6.43
• Scale from 6-40
• Validation, c=0.82 for 90-day mortality for cirrhotics, almost the same as Child-Turcotte-Pugh score (c=0.84)

MELD Special Cases
• Hepatocellular Carcinoma• Hepatopulmonary Syndrome• Familial Amyloidosis• OTC Deficiency, Crigler-Najjar Syn., etc.• Currently Special Cases constitute:
– 0 of 19 Status 1 0%– 52 of 138 with MELD >30 38%– 214 of 807 with MELD 20-29 26%– 7 OF 6844 with MELD 10-19 0.1%– 0 of 6228 with MELD <10 0%

MELD
UNOS: Transplanted 3/02-7/02 1786+570• HCC 428• Hepatopulmonary Syndrome 24• Portopulmonary Hypertension 2• Familial Amyloidotic Polyneuropathy 2• Oxalosis 3• Hepatoblastoma 1• Other Special Cases 105• Total 570

MELD & HCC
Evaluation of # and size of tumors (US, CT or MR of abdomen and chest, bone scan) and– Enhancing tumor >1cm, or– AFP >200, or– + arteriogram, or– + biopsy, or– Have had treatment with PEI, RITA, cryo, or TACE,
and
• Not be a candidate for resection

Conclusions
• Liver transplantation is the optimal treatment for many end stage liver diseases
• Allocation of deceased donor organs is driven by acuity (MELD) and exceptions
• Survival outcomes are steadily improving, hampered by
• Donor limitations
• Recurrent disease