Endocrinal functions of hypothalamus and pituitary gland (2)
Upload
daniel-flowersCategory
view
214download
0
Adrenal gland disorders
Dr. Miada Mahmoud Rady
EMS/474
Endocrinal emergencies

Introduction
Supra renal gland or adrenal gland are paired gland located at
the upper pole of the kidneys.
It is divided into two parts an outter cortex and inner medulla ,
each secretes a different set of hormones.
Main function of the hormones secreted by adrenal glands
are :
1. Cortisol → Sugar → increase BMR using fat and
protein for energy.

Introduction
2. Aldosterone → Salt → Na and water reabsorption
(↑ Na ) , K excretion ( ↓ K ).
3. Androgens→ Sex → sex hormones .
4. Adrenaline and noradrenaline → Stress→
stimulates sympathetic nervous system .
4 S

Hypothalamopituitary adrenal axis
Hypothalamus secretes CRF.
Which stimulate anterior pituitary to secretes ACTH.
Which stimulate adrenal cortex to secrete cortisol.

Cortisol
1. Assist with the response to stress.
2. Maintain blood pressure and cardiovascular function.
3. Regulates the metabolism of carbohydrates, proteins, and
fats.
4. Regulates glucose levels by balancing the effects of
insulin.
5. Slows the inflammatory response.

Adrenal dysfunction
So abnormal adrenal cortical function produces:
1. Abnormalities in the metabolism of carbohydrates
and protein.
2. Disturbances in salt and water metabolism.

Adrenal insufficiency
Definition : decreased function of the adrenal cortex .
It may be Primary Or Secondary .
Decreased in hormone production result in :
1. Weakness.
2. Dehydration.
3. Impaired body ability to maintain adequate blood
pressure and respond to stress.



Primary Adrenal Insufficiency
Also known as Addison's disease .
It is caused by Decreased Function of The Adrenal Cortex
and consequent underproduction of cortisol and Aldestorone.
Clinical presentation:
1. Slow progressive onset (over several months) .
2. The symptoms are usually well tolerated except in
crises .

Clinical Presentation
1. Hypotension and salt craving .
2. Hypoglycemia .
3. Hyper pigmentation (skin pigmentation ).
4. Weakness .
5. Weight loss.
6. Fatigue .
7. Fainting .
8. Pain (musculoskeletal ) which is so sever during crises.
9. Diarrhea which is so marked during crises.


Secondary Adrenal Insufficiency
More common than the primary type.???
Caused by :
1. lack of adrenocorticotropic hormone (ACTH)
secretion from the pituitary gland.
2. Sudden withdrawal of chronic corticosteroid therapy.
About 25% of patients first experience symptoms during an
addisonian crisis.

Secondary Adrenal Insufficiency
Clinical presentation :
The same as primary adrenal insufficiency except:
1. Chief clinical manifestation is shock.
2. Hypoglycemia is more sever.
3. Gastrointestinal symptoms are less common.
4. Darkening of the skin and dehydration do not
occur.

Addisonian crises symptoms
1. Sudden, severe pain in back and abdomen.
2. Severe vomiting and diarrhea.
3. Dehydration (marked).
4. Hypotension and shock.
5. Syncopal attack and finally coma.
6. Can be fatal.


Laboratory Finding
1. Decreased serum cortisol .
2. Hyponatremia .
3. Hyperkalemia .
4. Hypoglycemia .

Management of Addisonian Crises
1. Maintain ABCs :
Maintain patent airway , guard against vomiting and be
ready for suction.
Advanced airway management may be indicated.
Maintain adequate oxygenation and ventilation
Follow the procedure for altered mental status or coma.
Continuously monitor cardiac rhythm.

Begin rehydrating the patient, and correct electrolyte and
acid-base abnormalities.
1. D5NS is the preferred IV fluid
2. Start an IV, and infuse up to 1 L of 0.9% NS.
3. If the patient is hypotensive, administer an NS
bolus at 20 mL/kg.
4. Check the patient’s glucose level and administer
25 to 50 g of D50 to correct the hypoglycemia.

Hydrocortisone, 100 mg IV, is indicated in the acute
management of a crisis.
1. Continuously reassess the vital signs and rapidly
transport the patient.


Cushing syndrome

Cushing syndrome
Caused by :
1. Excess cortisol production by the adrenal glands.
2. Excessive use of cortisol or other similar corticosteroid
hormones.

Characteristic Changes
Metabolism of carbohydrate, protein, and fat is disturbed.
a. Blood glucose level rises.
b. Protein synthesis is impaired so Body proteins are broken
down which Leads to :
loss of muscle fibers and muscle weakness
Bones become weaker and more susceptible to
fracture.

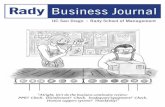
Clinical presentation
1. Weakness and fatigue
2. Increased thirst sensation and urination (hyperglycemia).
3. Obesity and weight gain at :
(a) Abdomen
(b) Face (“moon face”)
(c) Neck
(d) Upper back (“buffalo hump”)

Clinical presentation
4. Thinning of the skin leading to:
(a) Easy bruising.
(b) Pink or purple stretch marks (striae).
5. Darkening of skin of the neck





Cushing Syndrome Clinical Manifestation

Management
1. Patient with Cushing disease require long life treatment .
2. Emergency treatment is focused on addressing ABCs.

Home Work
• In a Table Compare Between :
1. DKA and HHNK.
2. Hypothyroidism and hyperthyroidism .
Any questio
ns?