Administration of Intravesical Therapies - WA · PDF fileThis assessment includes both a...
12
Administration of Intravesical Therapies Self Directed Learning Package
Transcript of Administration of Intravesical Therapies - WA · PDF fileThis assessment includes both a...
Administration of Intravesical TherapiesSelf Directed Learning Package
2
© Department of Health, State of Western Australia (2010)
Copyright to this material produced by the Western Australian Department of Health belongs to the State of Western Australia, under the provisions of the Copyright Act 1968 (Commonwealth Australia). Apart from any fair dealing for personal, academic, research or non-commercial use, no part may be reproduced without written permission of the Health Networks Branch, Western Australian Department of Health. The Department of Health is under no obligation to grant this permission. Please acknowledge the WA Department of Health when reproducing or quoting material from this source.
Suggested citation
Department of Health, Western Australia. Administration of Intravesical Therapies: Self-directed Learning Package. Perth: Health Networks Branch, Department of Health, Western Australia; 2010.
Important Disclaimer
All information and content in this Material is provided in good faith by the WA Department of Health, and is based on sources believed to be reliable and accurate at the time of development. The State of Western Australia, the WA Department of Health and their respective officers, employees and agents, do not accept legal liability or responsibility for the Material, or any consequences arising from its use.
This package has been developed by the WA Cancer and Palliative Care Network Urology Tumour Collaborative.
The local implementation, training and evaluation of clinical staff remains the responsibility of the employing authority.
Date produced: November 2007
Date first reviewed: May 2008
Date reviewed: November 2010
Date for next review: November 2012
3
Intravesical TherapyCompetency Program
IntroductionThis policy applies to registered nurses and medical practitioners who are seeking to be trained and assessed as competent in delivering intravesical bladder cancer treatment.
Any practitioner who is intending to give intravesical treatment requires appropriate training and assessment. This assessment includes both a theoretical and practical component. On completion of this package, practitioners should be able to demonstrate an understanding of non-muscle invasive bladder cancer, associated health and safety issues regarding handling of cytotoxic and immunotherapeutic agents as well demonstrating safe practical skills relating to their administration.
Nurses, who are already certified as competent to administer chemotherapy but are unfamiliar with intravesical treatments, should complete this self directed learning package prior to undertaking any clinical practice to familiarise themselves with the specific requirements for delivering intravesical treatments.
All nurses administering intravesical cytotoxic drugs should be annually assessed and their assessor should record this as part of their performance management.
Bladder cancer epidemiologyApproximately 200 new cases of bladder cancer are diagnosed each year in Western Australia. Bladder cancer is a chronic illness and patients are required to undergo surveillance programs for many years following treatment. The cause of bladder cancer is not yet fully known but many diverse factors have been implicated, the most common being:
cigarette smoking
chemical used in the manufacture of rubber, plastics, insecticides, cables and dyes.
calculi
chronic inflammation and diverticulum
schistosomiasis.
It is now fairly well established that it is the metabolic products of the various chemicals that cause cancer, the exact mechanism being unknown.
4
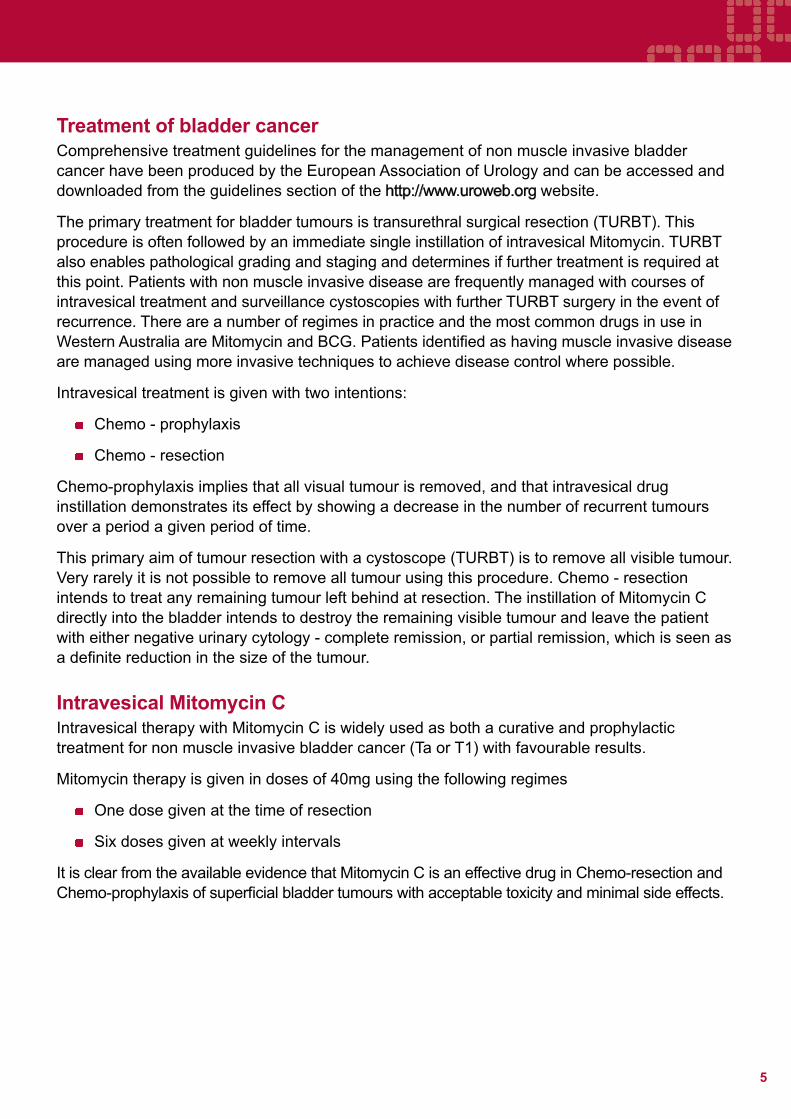
Clinical Grading and Staging of Bladder TumoursThe tumours develop in the epithelial lining of the bladder and quite often start as papillary growths. The majority of bladder cancers are transitional cell carcinomas. Without treatment, the tumours can invade by stages into the superficial muscle layer, the deep muscle and eventually into the surrounding tissues. This rate of growth is usually determined by how aggressive the tumour is, as shown by the grading definitions below.
Figure 1 Bladder Cancer Grading
Grading Definition
G1 Well differentiated (least aggressive)
G2 Moderately differentiated
G3 Poorly differentiated (most aggressive)
Treatment for bladder cancer is dependant on the stage of the disease at diagnosis or in the event of recurrence. Patients are classified as having either non muscle invasive disease (Carcinoma insitu, Ta or T1 disease) or have muscle invasive disease (T2 and above). Carcinoma in situ is a highly aggressive non muscle invasive type of bladder cancer. Staging is demonstrated further in the diagram below.
Figure 2 Staging of bladder cancer
FatMuscleConnective TissueBladder Lining
CISTaT1T2
T3
T4
Figure 2.
5
Treatment of bladder cancerComprehensive treatment guidelines for the management of non muscle invasive bladder cancer have been produced by the European Association of Urology and can be accessed and downloaded from the guidelines section of the http://www.uroweb.org website.
The primary treatment for bladder tumours is transurethral surgical resection (TURBT). This procedure is often followed by an immediate single instillation of intravesical Mitomycin. TURBT also enables pathological grading and staging and determines if further treatment is required at this point. Patients with non muscle invasive disease are frequently managed with courses of intravesical treatment and surveillance cystoscopies with further TURBT surgery in the event of recurrence. There are a number of regimes in practice and the most common drugs in use in Western Australia are Mitomycin and BCG. Patients identified as having muscle invasive disease are managed using more invasive techniques to achieve disease control where possible.
Intravesical treatment is given with two intentions:
Chemo - prophylaxis
Chemo - resection
Chemo-prophylaxis implies that all visual tumour is removed, and that intravesical drug instillation demonstrates its effect by showing a decrease in the number of recurrent tumours over a period a given period of time.
This primary aim of tumour resection with a cystoscope (TURBT) is to remove all visible tumour. Very rarely it is not possible to remove all tumour using this procedure. Chemo - resection intends to treat any remaining tumour left behind at resection. The instillation of Mitomycin C directly into the bladder intends to destroy the remaining visible tumour and leave the patient with either negative urinary cytology - complete remission, or partial remission, which is seen as a definite reduction in the size of the tumour.
Intravesical Mitomycin CIntravesical therapy with Mitomycin C is widely used as both a curative and prophylactic treatment for non muscle invasive bladder cancer (Ta or T1) with favourable results.
Mitomycin therapy is given in doses of 40mg using the following regimes
One dose given at the time of resection
Six doses given at weekly intervals
It is clear from the available evidence that Mitomycin C is an effective drug in Chemo-resection and Chemo-prophylaxis of superficial bladder tumours with acceptable toxicity and minimal side effects.
6
Side effects from the treatment:
This is a local treatment affecting the bladder. Systemic absorption is rare.
The patient may feel the need to pass urine more frequently than normal for 2-3 days. This is due to mild irritation from the drug and also the site of the recently removed bladder tumour. Patients can help to relieve these symptoms by drinking 3 litres of fluid a day which will dilute the urine.
Because the drug is instilled into the bladder patient may notice that their urine is discoloured for about 12 hours following the treatment. This is due to the colour of the drug.
Although the drug used is a type of chemotherapy, patients will not experience the side effects associated with chemotherapy, such as hair loss, nausea or vomiting, because the effect of the drug is localised in the bladder.
BCG ImmunotherapyCarcinoma in situ and high grade bladder cancer (Grade 3) are considered to be high risk disease as if treated with surgery alone can progress to muscle invasive carcinoma. Intravesical treatment in addition to transurethral resection has shown a “complete response” rate in 50% of those treated in clinical trials with significantly improved prognosis amongst the respondents. Whist BCG therapy is the newer of the two treatments, clinical trials on the use of BCG therapy are also yielding positive results.
BCG treats on the premise of an immune response stimulation. It was introduced as a method of treatment following evidence that cell mediated immunity plays a role in the patients response to cancer. BCG was therefore employed in an attempt to control tumour recurrence.
Initial courses of BCG therapy are usually given on a weekly basis for 6 weeks. Whilst specific regimes do vary between different centres, maintenance treatment should be given to appropriate patients for a minimum period of 12 months if it is to be effective.
Side effects from the treatment:
Dysuria and frequency
Gross haematuria
Transient fever
Symptoms suggestive of BCG reaction (cough, persistent fever lasting more than 24 hours, joint pain and jaundice) should all be investigated without delay (Refer to guidelines for the administration of intravesical cytotoxic drugs within the hospital setting).
7
The following criteria have to be excluded prior to the instillation of BCG therapy
Urinary tract infection - treatment should be deferred until the patient is free of infection
Macroscopic haematuria or any urothelial wound
Presence of fever of unclear origin as well as any acute infectious diseases
Active TB (Tuberculosis)
Any immuno deficiency
Previous severe reaction to BCG
Traumatic catheterisation
Administration ProcedureRefer to WA Cancer and Palliative Care Network Guidelines for the Administration of intravesical cytotoxic drugs within the hospital setting
Part A: Instillation of a single post operative dose of an intravesical chemotherapy agent.
Part B: Instillation of a course of intravesical chemo / immunotherapy agents using pre mixed medication
Part C: Procedure for the instillation of a course of intravesical BCG using a closed system reconstitution kit
Post Treatment CareRefer to patient WA Cancer and Palliative Care Network patient information leaflets:
Information for patients undergoing intravesical Mitomycin therapy
Information for patients undergoing intravesical BCG therapy.
8
Competency Programme
Any nurse wishing to administer intravesical drugs should have a thorough understanding of the following issues and must be prepared to answer questions relating to these issues during the assessment period:
normal anatomy and physiology of the bladder
non-muscle invasive bladder cancer and its effects on the patient
how intravesical chemotherapy and immunotherapy acts on bladder cancer and the effects on the patient
be familiar with and understand the policy for the administration of intravesical chemotherapy
understand the safety issues surrounding the use of cytotoxic chemicals and their disposal and the reasons for such safety measures
be aware of what to do in the event of a spillage
understand the processes involved in the administration of intravesical drugs and the care patients require during and after treatment, and the reasons for such processes
be competent in delivering appropriate after-care advice to patients and carers.
Training and Assessment
Theoretical assessment – the learner should complete the following questionnaire and achieve 80% (minimum) correct responses prior to undertaking practical assessment.
Observation period - The learner will observe a qualified member of staff administering Intravesical Chemotherapy until such a time when the LEARNER feels competent enough to advance to supervised practice
Supervised practice - The learner should be observed throughout the entire process of preparation, delivering care, disposal of materials and after-care for the patient. The period of supervised practice has no fixed time period. Both the learner and assessor determine it, and the decision to allow independent practice should be mutually agreeable to both parties. The assessor should ensure that the learner has a thorough understanding of the issues discussed above prior to acknowledging the learners competence to practice independently.
9
Theoretical Assessment for the Administration of Intravesical Therapies
What personnel should not handle cytotoxics and cytotoxic waste products?
Once the Mitomycin arrives on the ward, where should it be stored until required?
Who can administer cytotoxic drugs?
List the protective clothing that must be worn when administering cytotoxic agents?
How would you dispose of the used equipment after completion of the instillation?
If you were unable to administer the Mitomycin because the urine is still bloodstained, what would you do with the unused treatment?
A patient who has received Mitomycin into their bladder, is incontinent and contaminates Bed linen Their own pyjamas The floor
How would you deal with this and in what order?
You notice a patient has a skin rash after receiving Mitomycin, what would you do?
What information would you give a patient “after-care” following an instillation of Mitomycin?
How soon after TURBT should the single does of Mitomycin be given?
How do you recognise BCG septic reaction?
How would you deal with a patient you suspect of having BCG sepsis?
Where should BCG be reconstituted?
10
Administration of Intravesical Therapies Assessment Form
The following is checklist is a tool for assessors to use when determining whether a Registered Nurse has met the necessary skill requirement of the Intravesical Therapy Competency Programme.
Competency Yes No
Can identify rationale for use of intravesical chemotherapy agent
Can identify side effects from the treatment
Checks Intravesical therapy with second nurse
Identifies appropriate action in event of cytotoxic spillage
Identifies correct procedure for disposal of clinical waste and linen
Prepares equipment required for therapy
Explains procedure to patient
Administers treatment according to Area Specific Guideline: Administration of Intravesical Therapies
Labels and disposes of Cytotoxic material according to Hospital guidelines
Instructs patient regarding ongoing management post installation of therapy
Completes treatment regime and disposes of remaining waste material
Communicates with shift coordinator and peers cytotoxic therapy in progress
Completes accurate documentation of treatment and any side effects
Name:
Assessor:
Date competency attained: / / Date for next review: / /
11
References and Further ReadingAldousari, S. & Kassouf, W. (2010). Update on the management of non-muscle invasive bladder cancer. Canadian Urological Association Journal, 4(1):56-64.
Babjuk, M., Oosterlinck, W., Sylvester, R., Kaasinen, E., Böhle, A., Palou, J., Rouprêt, M. (2009). Guidelines on TaT1 (Non-muscle invasive) Bladder Cancer. European Association of Urology. Available from http://www.uroweb.org website. Accessed 02/03/2011
British Association of Urological Nurses [BAUN]. (2005). Guidelines for the administration of intravesical therapies. Bathgate, UK: Fitwise Management Ltd.
Green, K. (n.d.). The Administration of Intravesical Drugs (Theory Package). Royal Devon & Exeter Healthcare Trust.
Hall, R. R. (Ed.). (1999). Clinical Management of Bladder Cancer. Arnold, London: Oxford University Press.
Lamm, D. L., McGee, W. R., & Hale, K. (2005). Bladder cancer: current optimal intravesical treatment. Urologic Nursing, 25(5), 323-332.
Lamm, D. L. (1995). BCG immunotherapy for transitional-cell carcinoma in situ of the bladder. Oncology, 9(10), 947-956.
Mostofi, F. K., Sobin, L. H., & Torloni, H. (1973). Histological Typing of Urinary Bladder Tumours: International Histological Classification of Tumours; No. 10. Geneva, Switzerland: World Health Organization.
Nepple, K. G., & O’Donnell, M. A. (2009). The optimal management of T1 high-grade bladder cancer. Canadian Urological Association Journal, 3(Suppl4), S188-192.
O’Donnell, M. A. (2007). Advances in the Management of Superficial Bladder Cancer. Seminars in Oncology, 34(2), 85-97. doi:10.1053/j.seminoncol.2006.12.012
Sobin, L. H., Wittekind, C. H., & International Union Against Cancer [UICC] (Eds.). (1997). TNM classification of malignant tumors. (5th ed.). New York: John Wiley & Sons.
Solsona, E., Iborra, I., Ricos, J. V., Monros, J. L., Casanova, J., & Dumont, R. (1999). Effectiveness of a single immediate Mitomycin C instillation in patients with low risk superficial bladder cancer: short and long-term followup. Journal of Urology, 161(4): 1120-1123. doi: 10.1016/S0022-5347(01)61606-9
Threlfall, T. J., & Thompson, J. R. (2009). Cancer incidence and mortality in Western Australia, 2007. Department of Health, WA, Perth, Statistical series number 86. Available from: http://www.health.wa.gov.au/docreg/Reports/Diseases/Cancer/WACR_Cancer_incidence_mortality_main_2007.pdf
HP
1198
1 F
EB
’11This document can be made available in alternative
formats on request for a person with a disability.
Produced by WA Cancer and Palliative Care Network© Department of Health 2011