Depot Injections in Treatment of Hay-fever and Pollen Asthma*
Upload
ike-ismi-zCategory
view
219download
0
Administration of depot and long-acting
antipsychotic injections
Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
This guide was commissioned and funded by Janssen-Cilag Ltd. Janssen-Cilag Ltd has beeninvolved in the development of the content, but did not have editorial control.
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 1

The Heights, 59-65 Lowlands RoadHarrow, Middlesex HA1 3AW
To subscribe call 0845 772 6100mentalhealthpractice.rcnpublishing.co.uk
Further information: [email protected]
Cover photograph: Alamy
3 Working within a recovery approach
6 Informed choice
7 Pharmacology
13 Physical health
14 Follow up
15 Maintaining knowledge and skills
15 Conclusion
16 References
Contents
2 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
MENTAL HEALTH PRACTICE ESSENTIAL GUIDE
© Copyright RCN Publishing Company Ltd 2008. All rights reserved. No part of thisbook may be reproduced, stored in a retrieval system, or transmitted in any form or byany means, electronic, mechanical, photocopying, recording or otherwise, without priorpermission of the publisher.
This guide was written by John Crowley, Professor Matt Griffiths,
Sheila Hardy, Mark Vincent, Jacquie White and Andrew Voyce.
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 2

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
october :: vol 12 no 2 :: 2008 3MENTAL HEALTH PRACTICE
It is essential for healthcare professionals toshare good practice and information inpartnership with those who use health and socialcare services (National Institute for MentalHealth in England 2008). The aim of this guide isto inform all practitioners, managers, serviceusers and carers about the use of intramuscular(IM) depot and long-acting injectable (LAI)antipsychotic medication. The recognition ofservice users’ need for privacy, safety and dignitywhen receiving these injections will beemphasised.
Fourteen years ago Good Practice in theAdministration of Depot Injections (Royal Collegeof Nursing (RCN) 1994) failed to mention thehumane aspects of the procedure ofadministering injections in terms of privacy,dignity and the environment. However, importantissues of dissatisfaction with the experience ofreceiving injections were highlighted by serviceusers (RCN 1994):�The reason for having an injection had not
been explained.�They were receiving too much medication.�They received too little information on side
effects.The group responsible for writing this guide in2008, aware of the development of moremeaningful service user/patient and carerinvolvement, reviewed a large number ofprotocols, guides and procedures from across theUK. Findings showed that the majority focusedon technical aspects and generally omitted theimportance of the relationship between thehealthcare professional and the service user. Arecent publication highlighted good practice inthe technical administration of all IM injections,
but did not address important differences in theadministration of depot or LAI antipsychotics(Hunter 2008).
In support of the principle of incorporating therecovery approach into every aspect of mentalhealth nursing practice (Department of Health(DH) 2006a), this guide emphasises theimportance of a partnership between thehealthcare professional and service users, usingtechnical information to illustrate, educate andencourage good practice. The working group hasconsidered the principles of working within arecovery framework, the environment, working inpartnership, informed choice, pharmacology,technique, monitoring and maintainingcompetence and knowledge. In each section thereader is signposted to a number of usefulpublications and good practice points arehighlighted.
Please note: where possible the term serviceuser has been adopted; the term patient has beenused interchangeably where it seemedappropriate or when it is citing a direct reference. Cartoons The cartoons featured throughout thisguide (© Andrew Voyce 2008) have beencreated by a user of mental health services andare a representation of the reported experiencesof people receiving depot injections in the 1980s.The illustrations are presented without comment;readers are encouraged to draw their ownconclusions of the nursing practice depicted.
Working within a recovery approach ‘Recovery is a deeply personal unique process ofchanging one’s attitudes, values, feelings, goals,skill and or roles’ (Kelly and Gamble 2005).
‘Offering help, treatment and care in an
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 3

atmosphere of hope and optimism’ is the first andoverarching principle in the National Institute forHealth and Clinical Excellence (NICE) guidelineson the treatment of people with schizophrenia(NICE 2002).
Recovery means different things to differentpeople (Kelly and Gamble 2005). In mental health,the notion of recovery is not about a ‘cure of acondition of biological origin’; it is about therecovery of the whole person. A way of living asatisfying, hopeful and contributing life, even withthe limitations caused by illness. Recovery involvesthe development of new meaning and purpose inlife as the individual grows beyond the catastrophiceffects of mental illness (Anthony 1993).
The values and principles of recovery shouldunderpin everything we do, every word we speakto colleagues and service users, and everyintervention we offer. At the core of the recoveryapproach is the absolute belief that there are ‘nolimits’ to the potential for recovery after adiagnosis of mental illness.
The basic principles and values of the recoveryapproach will inform the nurse administering thedepot medication to ‘work in partnership with thepatient and offer meaningful choice’ (DH 2006a).
What service users and carers should expectfrom a service:�That their aims are valued.�Partnership working that offers meaningful
choice.�Optimism, hope and the possibility of positive
change.�The promotion of social inclusion.Health and social care staff should provide(Roberts and Wolfson 2004):�An understanding of recovery principles.�Recognition of, and support for, the individual’s
personal resources.�An understanding of, and accommodation for,
the diverse views on mental illness, treatments,services and recovery.
�Awareness and skills to communicaterespectfully and develop good relationships.
�An understanding and active protection ofservice users’ rights.
�An understanding of discrimination and socialexclusion; how these may affect lifestyle andknowledge of how they can be reduced.
�Acknowledgement of the importance ofcultural beliefs and values.
�Comprehensive knowledge of communityservices and resources.
�Knowledge of patient groups and movementsand support in accessing them.
�Knowledge of family, friends and carers’ viewsand a willingness to support them.
The environment of administration Serviceusers have a right to care that actively promotes(DH 2001a):�Privacy – freedom from intrusion.�Dignity – being worthy of respect.The decision on which environment is chosen to
4 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
‘...but I have been by a Japanese one.’‘Paul! It’s your injection today!’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 4

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
october :: vol 12 no 2 :: 2008 5MENTAL HEALTH PRACTICE
administer the injection should be agreedbetween service users and clinicians involved intheir care. Irrespective of the setting, and indeedwho administers the injection, the good practicepoints in Box 1 should be followed.Working in partnership ‘It is important to notethat concordance is not a new, politically correct,way of referring to compliance. Compliancemeasures patient behaviour: the extent to whichpatients take medicines according to theprescribed instructions. However, concordancemeasures a two-way consultation process:shared decision-making about medicinesbetween a healthcare professional and a patient,based on partnership, where the patient’sexpertise and beliefs are fully valued’ (NationalPrescribing Centre (NPC) Plus 2007).
Creating a therapeutic alliance is dependenton the attitudes, values and corecommunication skills of the healthcareprofessional. Patel et al (2005) specificallyhighlight advocacy and treatment decisionmaking for enhanced nurse-patient interactionsas components of training and refreshercourses. Such training will help promote the
process of making shared decisions abouttreatment with the patient.
The act of administering a depot or LAIantipsychotic should not be seen as an isolatedbehaviour; it should be viewed as an importantand integral part of the individual service user’swhole matrix of care. While the administration ofthe injection is most likely to be carried out by anurse, it would be wrong to assume that otherdisciplines involved in the care should be divorcedfrom the process. Effective communicationbetween all professionals is essential in ensuringconsistent levels of care.
Gray and Robson (2005) have developed aflexible and adaptable toolkit that can be used byhealthcare workers to structure conversationswith service users about medication. This toolkitemphasises the service user’s rights, the need foran exchange of information and two-way
BOX 1
Good practice points
�Maintain a therapeutic environment byvaluing the nurse-patient relationship in thecontext of the injection-giving process.
�Create a safe and secure atmospherethrough provision of dependable andconsistent practitioners.
�Where possible, the same person shouldadminister the injection on each occasion.
�Exchange information about medicationand local resources.
�Create space in clinics for service users tomeet and interact with each other.(Adapted from Phillips and McCann (2007))
‘Shall we get it done now Paul?’‘Okay Marcia.’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 5

communication, and supports useful skills such asproblem solving and decision making. Box 2 listssome useful communication skills.
Informed choice Every adult must be presumed to have themental capacity to consent to, or refuse,treatment unless they are unable to (MentalCapacity Act 2005): �Understand the information relevant to the
decision. �Retain that information. �Use or weigh that information as part of the
process of making the decision.�Communicate their decision by talking, using
sign language or any other means. Obtaining consent is a process rather than a
6 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
Useful skills for good communication
BOX 2
�Using the service user’s own words. �Open-ended questions. �Reflective listening.�Summarising. �Eliciting and responding to feedback. �Working collaboratively. �Linking sessions together. �Setting an agenda. �Being flexible. �Building self-efficacy. �Taking an active therapeutic stance. �Emphasising personal choice and
responsibility. �Transparency.
one-off event (DH 2001b). The need to maintainthis continual process is necessary as treatmentchanges and the individual’s understanding andneeds fluctuates. Responding to changing needsfor information exchange as the patient movesalong a spectrum from a place where decisionsmay have been made for them towardsautonomy, shared decision making and informedchoice is important in supporting recovery.Healthcare professionals, patients and theircarers should communicate progress along thisspectrum on transfer to other teams to ensurethat work can be continued and lessons learntfrom each episode of care.
A meaningful exchange of information,discussion and choice depends on clearcommunication of the rationale for treatment,not just of the benefits and risks. This is mostuseful when framed in the language of theservice user, rather than the language ofpsychiatry, for example, what the medication isexpected to do for the problems experienced bythe service user. NPC Plus (2007), Usher andArthur (1997) and Rollnick et al (2000) suggestframeworks to guide this process in practice.
‘Advanced decisions’ to refuse medical treatmentare legally binding if they are valid and applicable,that is – the person had consent at the time theymade the decision and that the decision made isapplicable to the current decision. Advanceddecisions do not have to be made in writing,unless they are to refuse life-sustaining treatment(Mental Capacity Act 2005).
The law and professional bodies recognise thepower of advance directives, advance statementsor living wills. These are documents made in
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 6

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
october :: vol 12 no 2 :: 2008 7MENTAL HEALTH PRACTICE
advance of a particular condition arising andshow the patient’s treatment choices. While notlegally binding, they can provide usefulinformation about the wishes of a patient who issubsequently unable to make a decision. There isclearly an opportunity immediately following anyrelapse or crisis to work with the patient andcarers to capture important information, whichcan inform advanced statements .
The law in relation to capacity, consent andmental health is fluid and complex. Dimond(2008) provides a comprehensive overview andincludes example scenarios from mental healthpractice. Further good practice points are shownin Box 3.
Pharmacology Although biological, social and psychologicalfactors are all important in the maintenance ofmental health, medication treatment focuses ontreating chemical imbalances in the brain tominimise distressing symptoms and provideprotection from relapse. Positive symptoms ofpsychosis are thought to be due to an excess ofthe neurotransmitter chemical dopamine in thesynapses between brain cells in the limbic areaof the brain. Cognitive symptoms and negativesymptoms are thought to be related to too littledopamine in the synapses of the cerebral cortex.Mood symptoms are thought to be related to adifferent neurotransmitter – serotonin.
However, dopamine and serotonin levels arefinely balanced, too much of one can affect thebalance of the other.
Medication for psychosis is now classified intothree types. The first generation, or typical
BOX 3
Good practice points
�Consent is an ongoing process.�Identify a rationale for the injection based
on the experience of the service user and inhis or her own language.
�Frameworks to guide interventions inprocess consent and reflect on one’s owncompetence are available (Usher andArthur 1997, NPC Plus 2007).
�The Elicit-Provide-Elicit model can be usedto exchange information based on needs atany one time (Rollnick et al 2000).
�Work with the service user and carer tocapture information to inform future riskand relapse plans and advanced statements.
�Careful documentation and communicationcan promote ongoing collaboration in aninformed choice process.
‘We can go in the empty side room Paul.’‘I was just saying to Alan how I saw this bloke ata bus stop in Woolwich once and he reminded...’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 7

antipsychotics were the first to be licensed andinclude most injections. Second- and third-generation, or atypical antipsychotics, includeproducts that have been licensed since clozapine.
All antipsychotic medications target dopaminereceptors in the brain. In addition, antipsychoticmedication can affect a range of other types ofreceptors including the receptors for serotonin,acetylcholine, noradrenalin (norepinephrine) andhistamine as well as several other types of dopaminereceptors. This action is largely responsible for sideeffects but can also be beneficial, for example, to aidsleep. Evidence suggests that the different productsare largely equal in their ability to treat symptoms ofpsychosis (efficacy) but their different side effectprofiles affect their acceptability, tolerability andoverall effectiveness in practice (Tandon and Jibson2003, Lieberman et al 2005, Jones et al 2006). Long-acting antipsychotic medications byintramuscular injection Intramuscular injectionsof antipsychotic medications were developed toallow the medicines to be delivered in a modifiedway, over time, following administration. This hasthe advantage of promoting a steady therapeuticconcentration of the drug, while minimising someof the side effects and variable effects onsymptoms that may result from the peaks andtroughs experienced when only tablets are taken.The achievement of a steady therapeutic levelfrom regular injections also affords protectionfrom relapse beyond the time the last injectionwas received. Specific information about eachproduct can be found in the individual summaryof product characteristics.
If lifestyle factors make regular taking of oralmedication difficult, or the service user has apreference for injections rather than tablets, this
can provide an important protection from stress,prevent relapse and maintain mental health inthe future.First-generation long-acting ‘depot’antipsychotic injections First-generationantipsychotic LAIs are commonly called ‘depot’injections. Depot refers to the way the drug isdeposited and stored in the muscle before beingabsorbed. Manufacturers formulated theseproducts in an oil base, which takes time to moveout of the muscle into the bloodstream. The oilsused include sesame and coconut and differbetween products. The injections are made deepinto the gluteus muscle.
Time to steady state, when optimal therapeuticdose is achieved, can take between eight and 12weeks after first administration of the full dose.Peak concentration occurs from seven to ten daysafter the injection and this is when side effectsare also likely to peak (Bazire 2007).
These medications take a long time to beeliminated from the body, so various benefits, andindeed side effects, can persist for some timefollowing the last injection. This is whyadministration of a small test dose isrecommended. A test dose also allows anassessment of any allergic response (for exampleto a nut oil diluent). The elimination effect shouldalso be taken into consideration when switchingfrom an oral product to an injection or betweendifferent types of injections, because side effectsrelated to the original drug can emerge in thisperiod.Second-generation long-acting antipsychoticinjections Risperidone was the first second-generation LAI to be licensed in the UK. Therisperidone LAI antipsychotic works in a different
8 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 8

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
way to the first-generation depot injections. Tinypolymer beads impregnated with the activecompound are mixed with a diluent. After injectionthe diluent is quickly dissipated and the polymerbeads break down over a period of a few weeks,slowly releasing the drug as they do so (Ramstacket al 2003). The drug will not reach a therapeuticlevel for a few weeks after injection, therefore it isessential that the patient receive alternativeantipsychotic medication during the initial periodof treatment following the first injection.
Test doses are not required as long as theservice user has previously demonstratedtolerance to oral risperidone. Time to eliminationfrom the body can be quicker and fall off morerapidly after the last injection, than in comparisonwith the oil-based depot injections. Theimportance of accepting the injection at regularintervals to prevent relapse must be consideredwhen planning treatment. It is licensed for
october :: vol 12 no 2 :: 2008 9MENTAL HEALTH PRACTICE
administration into the gluteus muscle. Othersecond- and third-generation LAIs are indevelopment.Off-label and unlicensed medications Mostmedicines that healthcare professionals use arelicensed for a specific use and user group. This is astrict process, aimed at improving safety andensuring that medicines in use are proven in howthey work. However, some medicines are notlicensed for certain user groups and, therefore,their use is known as ‘off-label’. An example of off-label use is often seen in medicines for children orpeople with a learning disability, because it is notethical to undertake clinical trials on these groups.However, where these medicines are known to beeffective, have a good safety record, and it isconsidered best practice to use them, practitionerswill commonly prescribe and administer thesemedicines in the best interests of the patients totreat their condition.
Anyone who is to have a medicine that is off-label or unlicensed, for example, medicinethat has not been granted a product licence foruse in the UK, should be informed that themedicine is of a specific class, and made awareof the risks and benefits of such medicines sothat they can make an informed decision aboutwhether they wish to receive that particularmedicine (Nursing and Midwifery Council (NMC)2008a). Good practice points are listed in Box 4.
Details of an individual drug’s specific licensedindications are contained in its summary ofproduct characteristics (SPC). Please refer to theBritish National Formulary, published twice ayear and available online at www.bnf.org. SPCsand patient information leaflets are also availableonline via the electronic Medicines Compendium
‘... me of these two blokes I knew in thehospital, one of them used to look down incase there were any dog ends to pick up, andthe other one’s claim to fame...’‘You can put your jacket on the bed and getready Paul.’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 9

www.medicines.org.uk. Healy (2005), Bazire(2007) and Taylor et al (2007) each provideaccessible texts on pharmacology and moredetailed prescribing information. Injection technique Administering intramuscular injections should not be an isolatedbehaviour, but rather an important part of aprocess of medication management requiringthought and professional judgement (NMC2008a). Knowledge and skills in anatomy,physiology, patient assessment, patientpreparation and nursing intervention are allessential to fulfilling the role (Shepherd 2002).
Nurses need to be fully aware of theconsequences and, by default of their registration,be accountable for their clinical interventions.Practice must be evidence based anddemonstrate cogent understanding of theintervention and its context. Local protocols andprocedures should be followed. Core principles ofsafe practice and an exemplar standard operatingprocedure for prescribing, preparing andadministering injectable medicines are availablefrom the National Patient Safety Agency (2007).In addition the good practice points in Box 5should be noted.Monitoring All clinicians who prescribe oradminister medicines are accountable for the carethat they give, and are responsible for undertakinga comprehensive assessment of the patient undertheir care. It is also their responsibility to ensurethere is a valid prescription for the medicine theyare administering. As part of their assessment aclinician looking after any patient will need to beaware of other current medications to ensure thatmedications are not contraindicated (NMC 2008a).
All antipsychotic medication can give rise to
10 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
BOX 4
Good practice points
�Be clear about the licensed indication for the injection, including any contraindications,interactions, the maximum dose, frequencyand muscle for administration.
�Check allergy status of patients and staff,remembering that nut oil diluents are usedin depot antipsychotic injections (notrisperidone LAI).
�Use a test dose (not necessary withrisperidone LAI where tolerance to oralrisperidone is already demonstrated).
�Use the correct type of needle to make surethe active ingredient can travel down theneedle bore. With risperidone LAI, alwaysuse the needle supplied in the pack.
�Consider absorption and elimination effectswhen starting, switching or stoppingproducts.
unwanted effects. The purpose of this guide is notto list these verbatim, but nurses involved in thecare of service users receiving depot or LAIantipsychotic treatment need to be aware of whatunwanted symptoms might emerge. (See thepharmacology section for suggested resources.)Subjective experience of medication Data onside effects and efficacy of medicines come fromlarge clinical trial data sets and it should alwaysbe remembered that the experience of takingmedication is subjective. Although some effectsand side effects can be predicted from thepharmacology and can be measuredsystematically, the experience of the person taking
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 10

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
october :: vol 12 no 2 :: 2008 11MENTAL HEALTH PRACTICE
Good practice points
�The choice of injection site should bedetermined in conjunction with the serviceuser, however reference to the individualproduct’s SPC should be made to determinewhich sites are licensed because anydeviation from these means the drug is beingused off-label.
�Injection sites should be rotated at each visitand the previous site examined.
�Before administration, hands should bewashed thoroughly and protective glovesworn. A non-touch technique should be usedto prepare the injection according to themanufacturers’ information.
�The area in which medication is to beprepared should be as clean and unclutteredas possible and distractions andinterruptions should be avoided.
�Filter needles should not be used for drawing updepots, and only the needle supplied with thedose pack should be used for risperidone LAI.
�Needles should be long enough to reachmuscle and leave 5mm of the needle lengthclear of the skin. If the chosen needle is not
long enough to reach muscle, the injection maybe given into adipose tissue and this mayaffect the rate of absorption and potentiallyreduce the efficacy of the drug.. The choice ofneedle for administration is, therefore,important. Nisbet (2006) suggests that thetraditionally used green 21 gauge 35mmneedle may not be long enough to reachmuscle at the dorsogluteal site in manypatients. Females are likely to have a deeperfat layer at this dorsogluteal site. Individualclinical judgement should be used dependingon the size of the patient. A variety of lengthsof green 21 gauge needles are available.
�The site may be cleaned thoroughly for 30seconds with a 70 per cent isopropyl alcoholswab and allowed to dry for at least 30seconds before administering the injection(Lister and Sarpal 2004).
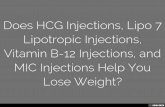
�The use of the Z-track method isrecommended as it reduces discomfort andprevents seepage back through the needletrack (Rodger and King 2000). See Box 6,page 12.
the medicine and the observations of carers areequally important and should form a central partof any assessment or review. Lifestyle factors andpersonal preference should also be consideredwhen making shared decisions about which drugis best to prescribe. Thus a patient with existingrisk factors for cardiovascular disease should
consider injections with a low propensity to causeweight gain. A patient in employment may wish toconsider an injection that is less likely to causesedation. Side effects Regular systematic monitoring ofside effects is essential using a validated tool,such as the Side Effect Scale/Checklist for
BOX 5
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 11
Antipsychotic Medication (SESCAM) (Bennett etal 1995) or the Liverpool University NeurolepticSide Effect Rating Scale (LUNSERS) (Day et al1995). Monitoring of physical health parametersis discussed in the next section.
Good practice dictates that monitoring shouldbe carried out on a three-monthly basis and atleast at every medication review. Both SESCAMand LUNSERS are broad scales and provide anindication of the presence of side effects. Morefocused outcome measures may be used to assessspecific adverse events, for example the AbnormalInvoluntary Movement Scale (for tardivedyskinesia) (National Institute of Mental Health
(NIMH) 1976), Barnes Akathisia Scale (Barnes1989). Cunningham-Owens (1999) describes indetail the assessment of extra pyramidal status.In a recent study, ability to manage side effectswas rated higher than the experience of sideeffects by patients – although the highest rateditem was efficacy (Kikkert et al 2006).
Assessment of positive effects is, therefore, asimportant as assessment of side effects. Datafrom assessments should be used to inform acollaborative dialogue with patients about theirexperiences. Importantly, information should beexchanged about current coping strategies andhow these may be enhanced. Using a problem-
12 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
BOX 6
The Z-track technique
�Immediately before injection, apply ashearing force with the non-dominant handto the skin, approximately 25mm from thechosen injection site, thus sliding the dermallayer over the muscle.
�Holding the needle at 90° to the skin,quickly insert the needle (leaving 5mm onthe outside). Pull back on the plunger; if noblood is aspirated continue. If blood isaspirated, discard the syringe and needleand start again using an alternative site.
�Slowly inject the contents of the syringe at arate of 1ml per 10 seconds.
�Withdraw the needle quickly andimmediately release the pressure on the skin.The natural elasticity of the skin returns thedermal layer to its former position, thussealing the needle track.
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 12
Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
solving approach to help patients identify andenhance their ways of coping with medicationproblems is important because these skills canoften be generalised to other areas of their lives.
Physical health Severe mental illness is associated with a higherincidence of physical illness and chronic disease(Brown 1997).
The most common physical conditions are: Cardiovascular disease People withschizophrenia are twice as likely to have someform of cardiovascular disease in comparison with people who do not have schizophrenia(Brown 1997). Diabetes The risk of diabetes in a person withschizophrenia is 14.9 per cent, compared with the1.2 per cent to 6.3 per cent risk observed in thegeneral population (Dixon et al 2000).
Obesity Evidence suggests excess weight gain canbe two to three times more prevalent in peoplewith schizophrenia than in the general population(Allison and Casey 2001). This may be due to highlevels of smoking, unhealthy diets and lack ofexercise – common lifestyle choices of people withschizophrenia (McCreadie 2003). However,antipsychotic medication can also exacerbateweight gain (Allison and Casey 2001). Thisantipsychotic treatment-induced weight gainincreases both the risk for hyperglycaemia and type2 diabetes, as well as the risk for hypertension andcardiovascular disease (Fontaine et al 2001).
These increased risks of physical disease maybe more prevalent because of the difficultyaccessing or receiving appropriate health carefrom primary and secondary services. Buntwal etal (1999) noted that 30 per cent of people withmental health problems using one mental healthunit had been struck off a GP’s list at some point.Despite evidence to suggest that people withschizophrenia have relatively high levels ofcontact with their GPs (Jablensky et al 2000),there appear to be inconsistencies in the waytheir problems are identified or managed. Forexample, studies have shown that patients withschizophrenia and heart disease have fewer bloodpressure or recent cholesterol tests (Hippisley-Cox and Pringle 2005).
The English government has producedguidelines (NICE 2002, 2006) recommendingthat physical health checks for people withsevere mental illness should normally be providedannually in primary care. To promote equality ofaccess and quality of services, there needs to besystematic disease prevention and healthpromotion programmes in place to challenge
october :: vol 12 no 2 :: 2008 13MENTAL HEALTH PRACTICE
‘...was that he’d been crossing a field inHailsham in 1942 and got machine-gunned bya German fighter. Escaped by jumpin’ in aditch. So this bloke in Woolwich was lookingdown at the gutter and I said to him...’‘Can you just hold your shirt up for me?’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 13

discrimination. This can be achieved by allorganisations working collaboratively to provideservices, which are fair, personal and responsiveto patients’ needs and wishes (DH 2006b).
The General Medical Services contract stipulatesthat these regular, physical health checks are partof the mental health review alongside regularreview of medication (British Medical Association2006). However, if the service user is not incontact with primary care then secondaryservices should monitor his or her physical health.
Effective communication between healthcareprofessionals in primary and secondary care willhelp the service user benefit from physicalassessment.
The Sainsbury Centre for Mental Health (2003)advocates that a physical health review for aperson receiving treatment with an antipsychoticinjection should include:�Advice about diet, exercise, smoking, and
substance and alcohol abuse. �Protection against influenza by offering annual
immunisation in view of increased occurrenceof cardiac and respiratory disorders, anddiabetes.
�Regular preventative care, for example cervicalcytology.
�Routine monitoring of weight and bloodpressure.
�Blood tests to measure glucose, cholesterol,and a full blood count.
�An electrocardiogram. The healthcare professional may also considerblood tests to monitor liver function, thyroidfunction, kidney function and creatinephosphokinase (Taylor et al 2007). More recently,measuring the waist-to-hip ratio has been
suggested as a method of measuring risk ofcardiovascular disease (Yusuf et al 2005). A newtool has been developed to help nurses assess 28physical health parameters and know what to donext if results are out of range (in print).
Follow up Any healthcare professional with theresponsibility of administering depot injectionsalso has a responsibility to ensure there is arobust system that identifies and follows upservice users who are not able to receive theirinjection on the due date.
Because of the pharmacokinetic profile ofrisperidone LAI, it is essential to follow up thoseservice users who have missed a dose. As there isat least a three-week lag between theadministration of the drug to effective dose level,the emergence of symptoms following a misseddose is not likely to be evident for at least threeweeks. However, as the drug is eliminated more
14 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
‘... I bet you’ve been machine-gunned by aGerman fighter. He turned round and said:No...’ ‘Just going in now...’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 14

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
quickly from the system than the older drugs, itis important to follow up the service user –ideally within a day of his or her missed dose.
With the slower time to elimination of the firstgeneration depot antipsychotics, there is a greaterwindow of opportunity for following up of thoseservice users who have missed a dose. Assertivefollow up is important, ideally within a few daysof the missed dose.
Maintaining knowledge and skills It is essential that all practitioners are aware of theirresponsibilities within the regulations and conductgoverning their profession (NMC 2008b). With thedevelopment of Agenda for Change and theKnowledge and Skills Framework (DH 2004a,2004b) implemented in most countries of the UK, itis incumbent on the practitioner to maintainprofessional knowledge and development. While theemployer has an obligation to support employeesduring the course of their work, it is the responsibilityof practitioners to maintain their contemporarypractice by formal and informal methods, using the
expertise of colleagues, patients, carers and othersinvolved in their day-to-day work.
Conclusion Antipsychotic medication remains a mainstay oftreatment for people experiencing serious mentalill health. It is the professional, legal and ethicalresponsibility of those administering themedication to be suitably skilled in contemporaryevidence-based techniques and to beacademically equipped to support the medicationmanagement of those under their care.
This guide is not intended to be either definitiveor exhaustive; it has been created to promotethinking and to stimulate further discussion.
Local protocols and governance arrangementsshould still be followed, as long as they reflectcurrent evidence; if they do not then it is theregistered nurse’s responsibility to challengethem. Where required, this guide might informthe review of such local arrangements, therebyencouraging a person-centred approach to LAIand depot management ■
october :: vol 12 no 2 :: 2008 15MENTAL HEALTH PRACTICE
‘...but I have been by a Japanese one – threetimes. I laughed. Turns out he’d been inMalaya, and it happened then.’‘There! That’s it. All over for now.’ ‘You can go back to the lounge now, Paul.’
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 15

References
Allison D, Casey D (2001) Antipsychotic-induced weightgain. A review of the literature. Journal of ClinicalPsychiatry. 62, suppl 7, 22-31.
Anthony WA (1993) Recovery from mental illness: theguiding vision of the mental health system in the 1990s.Psychosocial Rehabilitation Journal. 16, 4, 11-23.
Barnes TR (1989) A rating scale for drug-induced akathisia.The British Journal of Psychiatry. 154, 672-676.
Bazire S (Ed) (2007) Psychotropic Drug Directory: TheProfessionals’ Pocket Handbook and Aide Memoire.HealthComm, Aberdeen.
Bennett J, Done J, Harrison-Read P, Hunt B (1995) Arating scale/checklist for the assessment of the side effectsof antipsychotic drugs. In Brooker C, White E (Eds)Community Psychiatric Nursing: A ResearchPerspective. Volume 3. Chapman & Hall, London.
British Medical Association (2006) GP Contract.www.bma.org.uk/ap.nsf/Content/GPcontractandworkload?OpenDocument&Highlight=2,gp,contract,workload(Last accessed: April 14 2008.)
Brown S (1997) Excess mortality of schizophrenia. Ameta-analysis. British Journal of Psychiatry. 171, 502-508.
Buntwal N, Hare J, King M (1999) The struck-off mystery.Journal of the Royal Society of Medicine. 92, 9, 443-445.
Cunningham-Owens DG (1999) A Guide to theExtrapyramidal Side-effects of Antipsychotic Drugs.Cambridge University Press, Cambridge.
Day JC, Wood G, Dewey M, Bentall RP (1995) A self-rating scale for measuring neuroleptic side-effects –validation in a group of schizophrenic-patients. BritishJournal of Psychiatry. 166, 650-653.
Department of Health (2001a) Essence of Care. TheStationery Office, London.
Department of Health (2001b) Reference Guide toConsent for Examination or Treatment. The StationeryOffice, London.
Department of Health (2004a) Agenda For Change: FinalAgreement. The Stationery Office, London.
Department of Health (2004b) The NHS Knowledgeand Skills Framework and the Development ReviewProcess. The Stationery Office, London.
Department of Health (2006a) From Values to Action: The Chief Nursing Officer’s Review of Mental Health Nursing. The Stationery Office,London.
Department of Health (2006b) Standards for BetterHealth. The Stationery Office, London.
Dimond BC (2008) Legal Aspects of Mental Capacity.Blackwell Publishing, Oxford.
Dixon L, Weiden P, Delahanty J et al (2000) Prevalence and correlates of diabetes in nationalschizophrenia samples. Schizophrenia Bulletin. 26, 4,903-912.
Fontaine KR, Heo M, Harrigan EP et al (2001) Estimatingthe consequences of anti-psychotic induced weight gainon health and mortality rate. Psychiatry Research. 101,3, 277-288.
Gray R, Robson D (2005) Concordance Skills.Collaboration. Involvement. Choice: A Manual forMental Health Workers. Institute of Psychiatry, King’sCollege, London.
Healy D (2005) Psychiatric Drugs Explained. FourthEdition. Churchill Livingstone, London.
Hippisley-Cox J, Pringle M (2005) Health InequalitiesExperienced by People with Schizophrenia and ManicDepression: Analysis of General Practice Data inEngland and Wales. Disability Rights Commission,London.
Hunter J (2008) Intramuscular injection techniques.Nursing Standard. 22, 24, 35-40.
Jablensky A, McGrath J, Herrman H et al (2000)Psychotic disorders in urban areas. Australian and New Zealand Journal of Psychiatry. 34, 2, 221-236.
Jones PB, Barnes TR, Davies L et al (2006) Randomizedcontrolled trial of the effect on quality of life of second-vs first-generation antipsychotic drugs in schizophrenia:cost utility of the latest antipsychotic drugs inschizophrenia study (CUtLASS 1). Archives of GeneralPsychiatry. 63, 10, 1079-1087.
16 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 16

Me
nt
al
H
ea
lt
h
Pr
ac
ti
ce
E
ss
en
ti
al
G
ui
de
Kelly M, Gamble C (2005) Exploring the concept ofrecovery in schizophrenia. Journal of Psychiatric andMental Health Nursing. 12, 4, 245-251.
Kikkert MJ, Schene AH, Koeter MWJ et al (2006)Medication adherence in schizophrenia: exploringpatients’, carers’ and professionals’ views. SchizophreniaBulletin. 32, 4, 786-794.
Lieberman JA, Stroup TS, McEvoy JP et al (2005)Effectiveness of antipsychotic drugs in pateints withchronic schizophrenia. New England Journal ofMedicine. 353, 12, 1209-1223.
Lister S, Sarpal N (2004) Drug administration: generalprinciples. In Dougherty U, Lister S (Eds) The RoyalMarsden Hospital Manual of Clinical Procedures. Sixthedition. Blackwell Publishing, Oxford.
McCreadie R (2003) Diet, smoking and cardiovasculardisease risk in people with schizophrenia: descriptive study. British Journal of Psychiatry. 183,534-539.
National Institute for Health and Clinical Excellence (2002)Core Interventions in the Treatment and Management ofSchizophrenia in Primary and Secondary Care. ClinicalGuidance 1. NICE, London.
National Institute for Health and Clinical Excellence(2006) Bipolar Disorder. Clinical Guidance 38. NICE,London.
National Institute for Mental Health in England (2008)Medicines Management: Everybody’s Business. TheStationery Office, London.
National Institute of Mental Health (1976) AIMS.Abnormal Involuntary Movement Scale. In Guy W (Ed)ECDEU Assessment for Psychopharmacology. RockvilleMD.
National Patient Safety Agency (2007) Patient Safety Alert20: promoting safer use of injectable medicines.www.npsa.nhs.uk/patientsafety/alerts-and-directives/alerts/injectable-medicines/ (Last accessed: July 25 2008.)
National Prescribing Centre Plus (2007) A CompetencyFramework for Shared Decision Making with Patients:Achieving Concordance in Taking Medicines. NPC Plus,Keele.
Nisbet AC (2006) Intramuscular gluteal injections in theincreasingly obese population: retrospective study. BritishMedical Journal. 332, 7452, 637-638.
Nursing and Midwifery Council (2008a) Standards forMedicines Management. NMC, London.
Nursing and Midwifery Council (2008b) The NMC Codeof Professional Conduct: Standards of Conduct,Performance and Ethics. NMC, London.
Patel MX, De Zoysa N, Baker D, David AS (2005)Antipsychotic depot medication and attitudes ofcommunity psychiatric nurses. Journal of Psychiatric andMental Health Nursing. 12, 2, 237-244.
Phillips L, McCann E (2007) The subjective experiences ofpeople who regularly receive depot neuroleptic medicationin the community. Journal of Psychiatric and Mental HealthNursing. 14, 6, 578-586.
Ramstack M, Grandolfi G, Mannaert E, D’Hoore P,Lasser RA (2003) Long-acting risperidone: prolonged-release injectable delivery of risperidone using Medisorbmicrosphere technology. Abstracts of the IXthInternational Congress on Schizophrenia Research.Schizophrenia Research. 60 (Suppl), 1-401.
Roberts G, Wolfson P (2004) The rediscovery of recovery:open to all. Advances in Psychiatric Treatment. 10, 37-49.
Rodger MA, King L (2000) Drawing up and administeringintramuscular injections: a review of the literature.Journal of Advanced Nursing. 31, 3, 574-582.
Rollnick S, Mason P, Butler C (2000) Health Behavior Change:A Guide for Practitioners. Churchill Livingstone, Edinburgh.
Royal College of Nursing (1994) Good Practice in theAdministration of Depot Injections. Department ofHealth/Royal College of Nursing, London.
Sainsbury Centre for Mental Health (2003) Briefing 21. TheNew General Medical Services Contract for GPs.www.scmh.org.uk/pdfs/briefing+21.pdf (Last accessed: July22 2008.)
Shepherd M (2002) Medicines 2 – administration ofmedicines. Nursing Times. 98, 16, 45-48.
Tandon R, Jibson MD (2003) Efficacy of newer generationantipsychotics in the treatnment of schizophrenia.Psychoneuroendocrinology. 28, Suppl 1, 9-26.
Taylor D, Paton C, Kerwin R (2007) The South London andMaudsley NHS Trust & Oxleas NHS Trust PrescribingGuidelines. Ninth edition. Informa Health Care, London.
Usher KJ, Arthur D (1997) Nurses and neurolepticmedication: applying theory to a working relationshipwith clients and their families. Journal of Psychiatric andMental Health Nursing. 4, 2, 117-123.
Yusuf S, Hawken S, Ôunpuu S et al (2005) Obesity and therisk of myocardial infarction in 27,000 participants from 52countries: a case-control study. The Lancet. 366, 9497,1640-1649.
october :: vol 12 no 2 :: 2008 17MENTAL HEALTH PRACTICE
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 17

18 october :: vol 12 no 2 :: 2008 MENTAL HEALTH PRACTICE
This guide was prepared by:John Crowley, lecturer, University of Greenwich/Researcher Oxleas NHS FoundationTrust; Professor Matt Griffiths, independent nurse consultant – prescribing and medicinesmanagement, visiting professor of prescribing medicines management, The University ofNorthampton, senior nurse, medicines management University Hospitals of Leicester NHSTrust; Sheila Hardy, nurse practitioner, Park Avenue Medical Centre, Northampton; MarkVincent, principal lecturer, The University of Northampton; Jacquie White, lecturer,University Teaching Fellow, University of Hull; Andrew Voyce, service user
Address for correspondence: Sheila Hardy [email protected]
The views expressed in this guide are those of the authors and not those of Janssen-Cilag Ltd.
Footnote:
Many of the policy references in this guideapply to England. Despite this, it is intended
that the spirit of this guide should be equallyrelevant to readers in Scotland, Wales andNorthern Ireland.
Notes:
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 18

INFORMEDIN TOUCHONLINE
DIGITAL EDITIONS
Subscribers can also access the RCN Publishing Online archive which containsclinical and research articles, as well as access to exclusive web-only content
To subscribe to the digital edition or to switch your current print subscription to digital,visit www.mentalhealthpractice.co.uk
* Backdated to September 2007
MENTAL HEALTH PRACTICE AT YOUR FINGERTIPS
• Save on shelf space – just log in toaccess back issues
• Environmentally friendly – no packagingor distribution implications
• Search all archived editions, includingnews, features and clinical articles*
• Fully linked contents page – go directly toitems of interest with a single click
• Build your own Mental Health Practicedigital library
• Access immediately on the day ofpublication
• Link directly to relevant websites from within articles
PLUS
Fully searchable, interactive and easy to use:
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 19
To subscribe, visit www.mentalhealthpractice.co.uk
� Research and practice articles speciallycommissioned on the latest findings
� In-depth clinical features analysing a widerange of topics
� High-quality, practice-orientated editorialwritten by practising nurses and independentexperts in their field
� A round-up of key news, policy developmentsand guidelines from the mental health field
� Letters, resources and research round-up incorporating livelydebates, reviews and the latest research findings
The leading journal in mental health nursing
PLUS Subscribers can also accessthe RCN Publishing Online archivewhich contains clinical andresearch articles, as well as accessto exclusive web-only content
Mental Health Practice is available in print or digital format
MHP depot booklet THIS ONE 2 9/9/08 16:19 Page 20