Adipocytes, Obesity, Bariatric Surgery and its Complications · Adipocytes, Obesity, Bariatric...
56
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine
Transcript of Adipocytes, Obesity, Bariatric Surgery and its Complications · Adipocytes, Obesity, Bariatric...
Adipocytes, Obesity, Bariatric Surgery
and its Complications
Daniel C. Morris, MD, FACEP, FAHA
Senior Staff Physician
Department of Emergency Medicine
Objectives
Basic science of adipocyte
Adipocyte tissue as an endocrine organ
Inflammatory response of obesity
Types of bariatric surgery
Complications and treatments
Too many calories in…………….
Not enough calories out.
Morbidity and Mortality
• Type 2 diabetes
• Hypertension
• Cardiovascular and Kidney disease
• Bone and Joint problems
• Increased risk of Cancer

Gene-Environment
Adipocyte
The classic function of the adipocyte is to store and
release lipid fuel.
Adipocytes can vary in size from 20 to 200 µm.
Adipose tissue can be divided into brown and white.
Brown adipose tissue is thermogenic whereas white
adipose tissue is primarily for storage.
Adipose deposits can be intracellular,
interorgan and subcutaneous.
Adipocyte
Approximately 90% of the adipocyte is triglyceride
storage.
The remaining 10% consists of nucleus, cytoplasm,
mitochondria and other organelles.
Hyperplastic obesity
Hypertrophic obesity

Classification of obesity
increase in adipocytes
juvenile onset obesity
Adipocytes are increased in
number rather than in size. The
number of cells can never be
reduced making it difficult to
reduce body fat. Critical times
are:
last trimester of mother's
pregnancy
first year of life
puberty
increase in adipocyte size
adult onset obesity
Adipocyte size increases when
lipid storage exceeds oxidation
release.
Hyperplastic obesity can be
reduced by increasing activity or
by reducing food intake.
Hyperplastic Morphology Hypertrophic Morphology
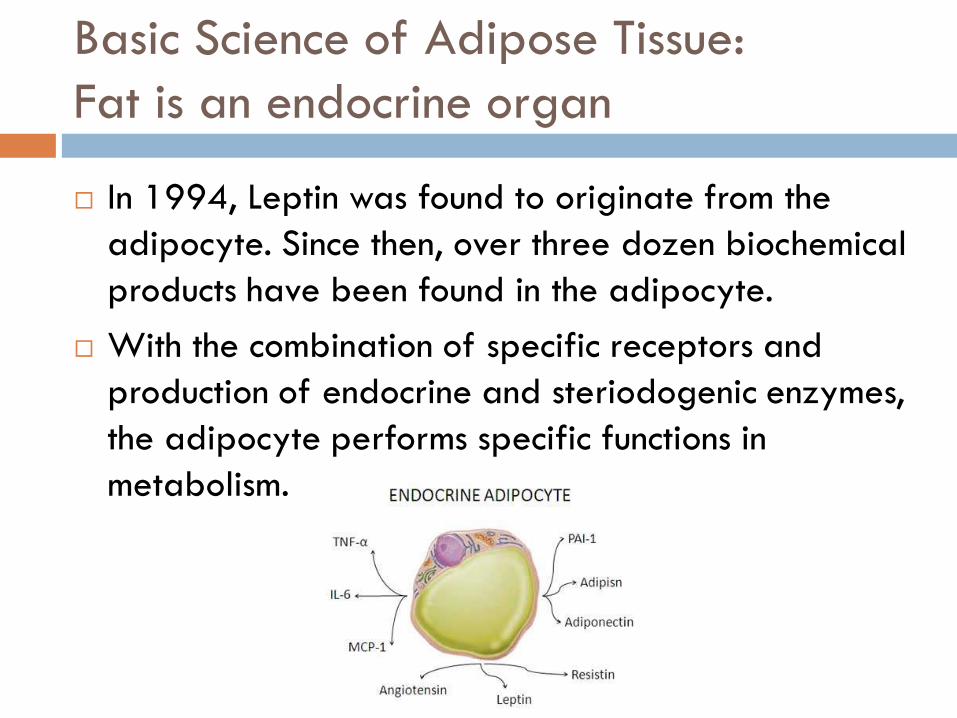
Basic Science of Adipose Tissue:
Fat is an endocrine organ
In 1994, Leptin was found to originate from the
adipocyte. Since then, over three dozen biochemical
products have been found in the adipocyte.
With the combination of specific receptors and
production of endocrine and steriodogenic enzymes,
the adipocyte performs specific functions in
metabolism.
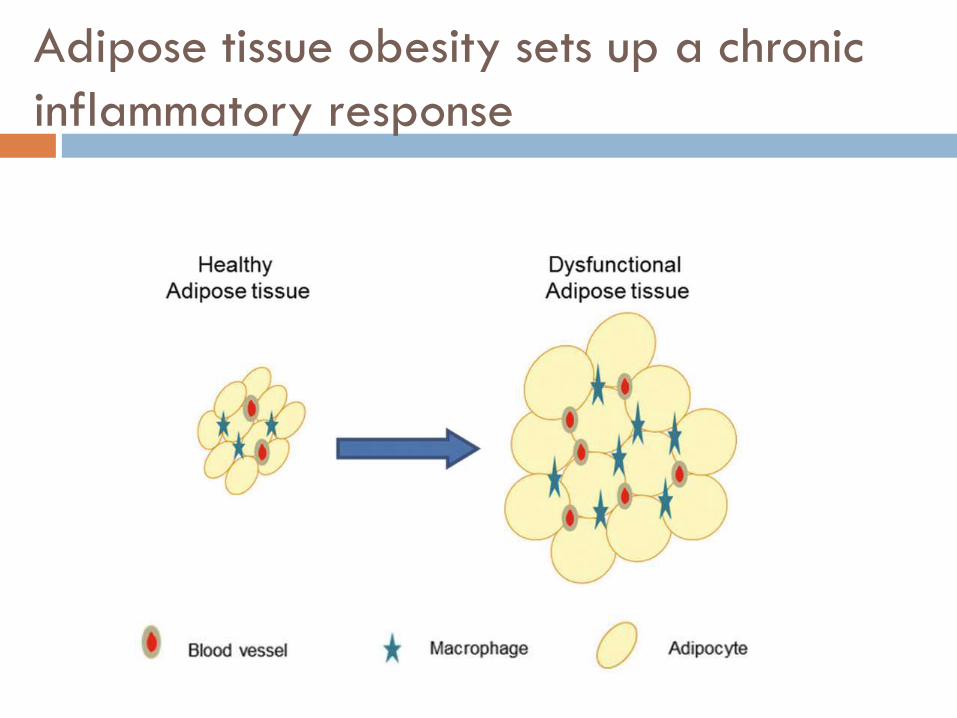
Adipose tissue obesity sets up a chronic
inflammatory response
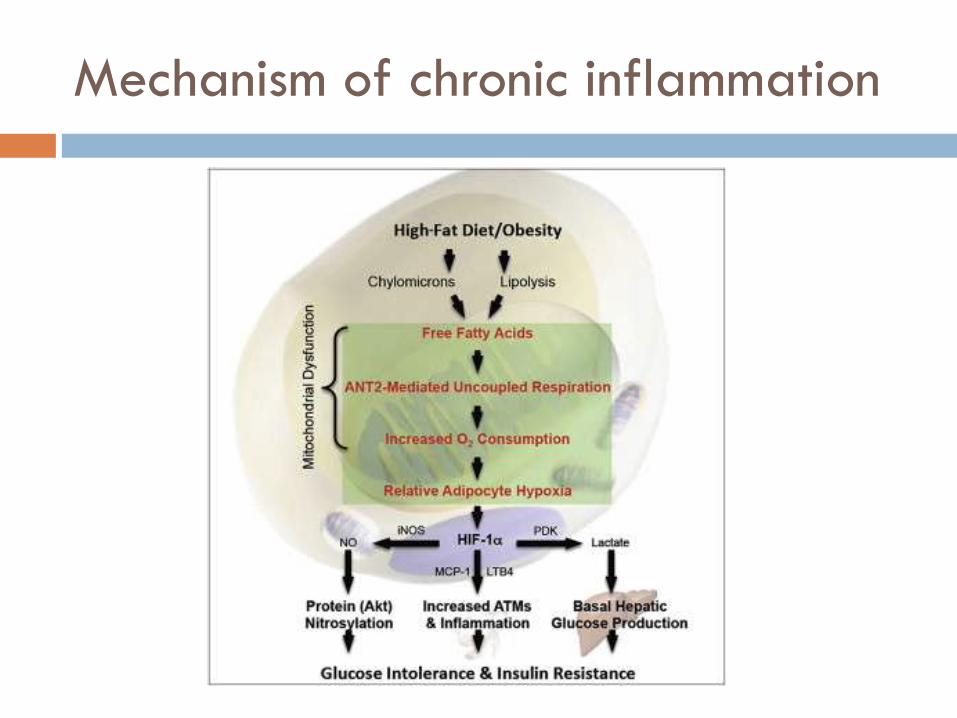
Mechanism of chronic inflammation
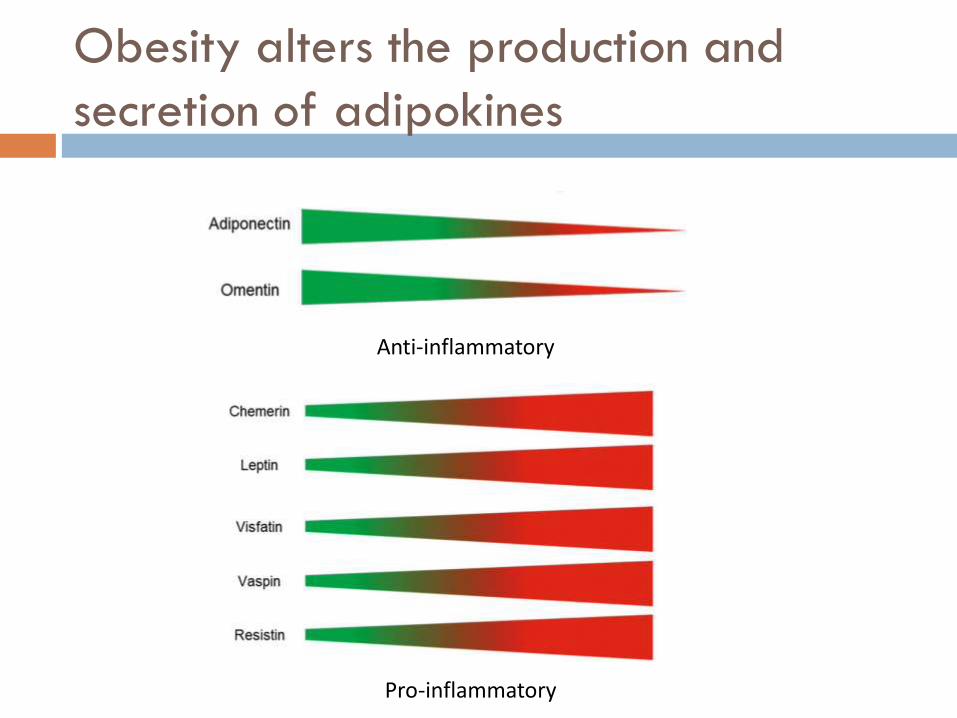
Obesity alters the production and
secretion of adipokines
Anti-inflammatory
Pro-inflammatory
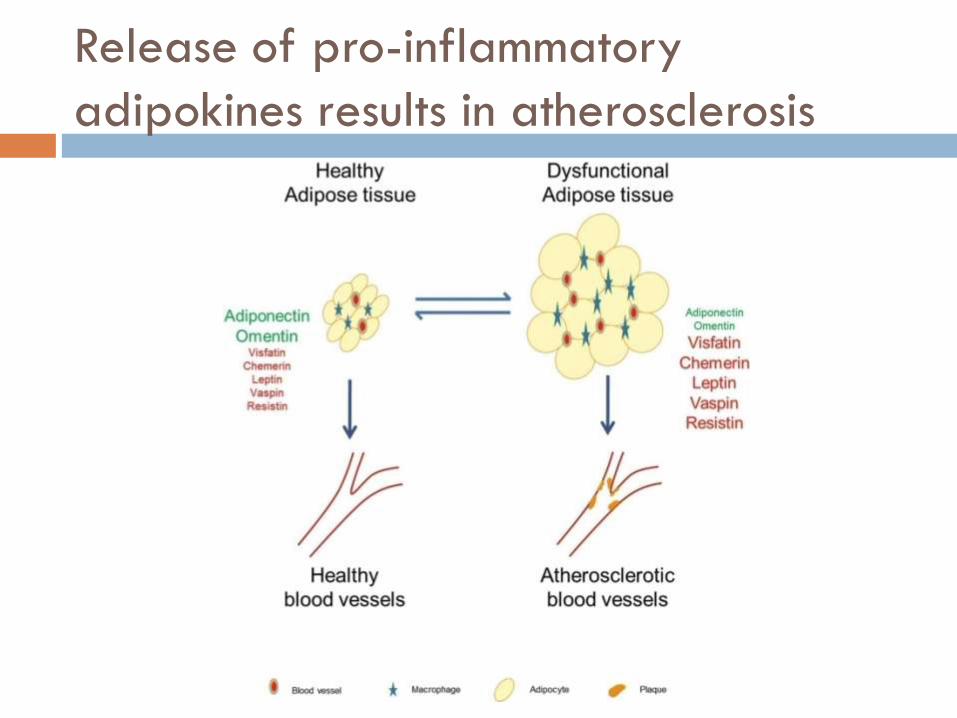
Release of pro-inflammatory
adipokines results in atherosclerosis
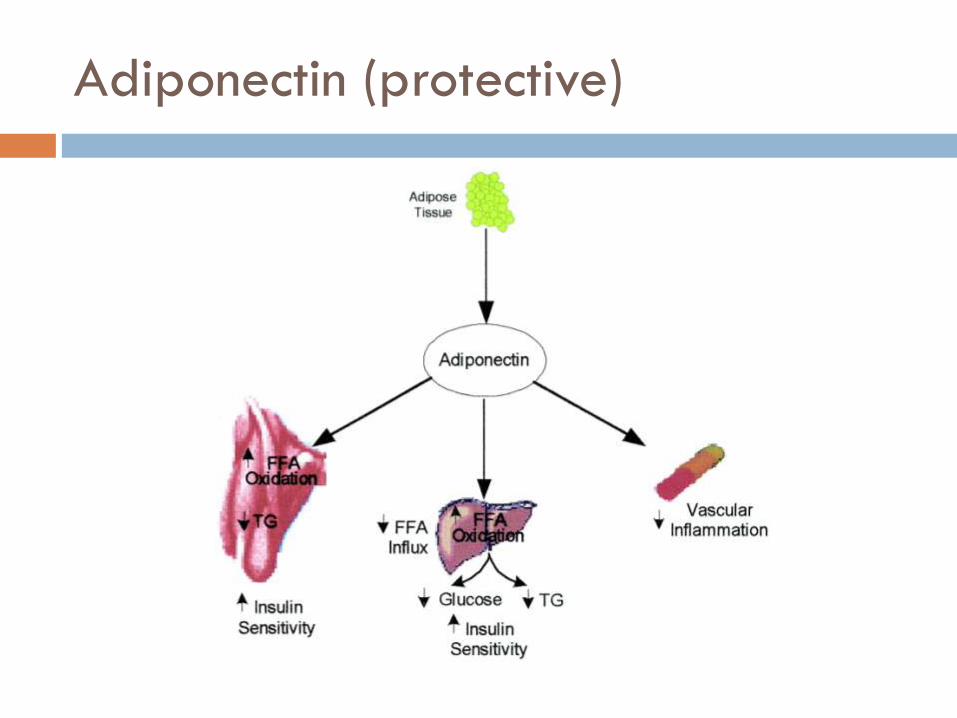
Adiponectin (protective)

Leptin (inflammatory)
Leptin enters the hypothalamus Activates the immune system

Leptin Mutation

Interleukin 6 (IL-6) and Tissue Necrosis
Factor (TNF)
Adipokine
Insulin resistance
Visceral adipose tissue
releases IL-6 directly
into the portal system
Adipokine
Development of type
2 diabetes
Insulin resistance
IL-6 TNF
Evolutionary Advantage?
Quickly store excess calories—Sedentary lifestyle?
Immune system is confused by modern diet
(pathological diet?) and activity levels
Metabolic disease is caused by lipids that are
stored in the wrong areas.
Overproduction of adipokines have
wide systematic implications in overall
health of the individual
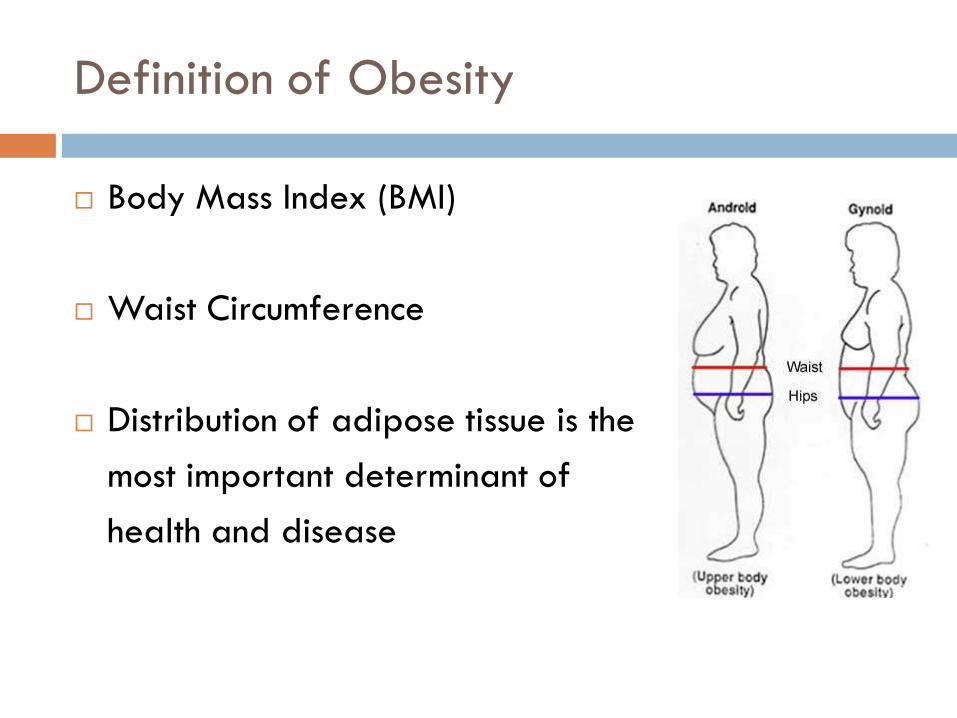
Definition of Obesity
Body Mass Index (BMI)
Waist Circumference
Distribution of adipose tissue is the
most important determinant of
health and disease
Treatment of Obesity
Diet and exercise
Pharmacologic management- Inadequate long-term
clinical efficacy or unacceptable side effects (anal
leakage?)
Bariatric Surgery- intervention that consistently
induces sustained weight loss
Bariatric Surgery
Roux-en-Y gastric bypass (common)
Sleeve gastrectomy (common)
Laparoscopic adjustable gastric band (uncommon)
Biliopancreatic diversion with duodenal switch (rare)

Indications for Bariatric Surgery
BMI > 40 kg/m² without comorbid conditions
BMI between 35 kg/m² and 40 kg/m² with
significant comorbidity (diabetes, HTN, apnea)
Candidates must have tried and failed nonsurgical
weight loss measures
Mechanisms of Weight Loss
Stabilizes glucose levels
Increases metabolism
Behavioral changes in eating habits through
alteration of gastro- and neuro- peptides
Alteration of gut microbes suggesting that metabolic
regulation begins in the gut.
Weight loss is not necessary due to smaller stomach
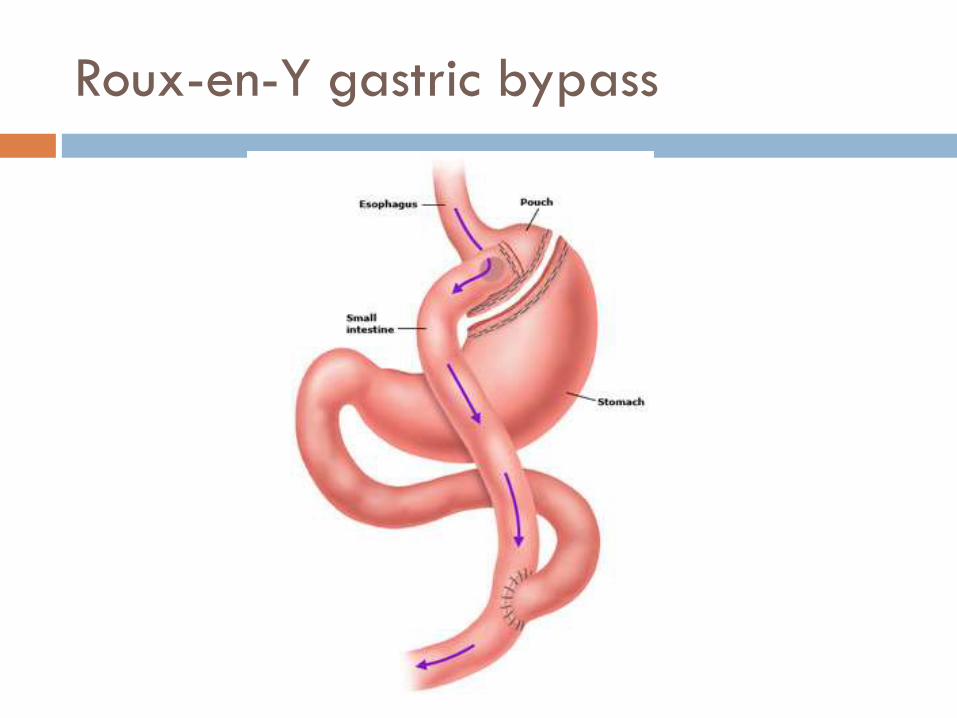
Roux-en-Y gastric bypass
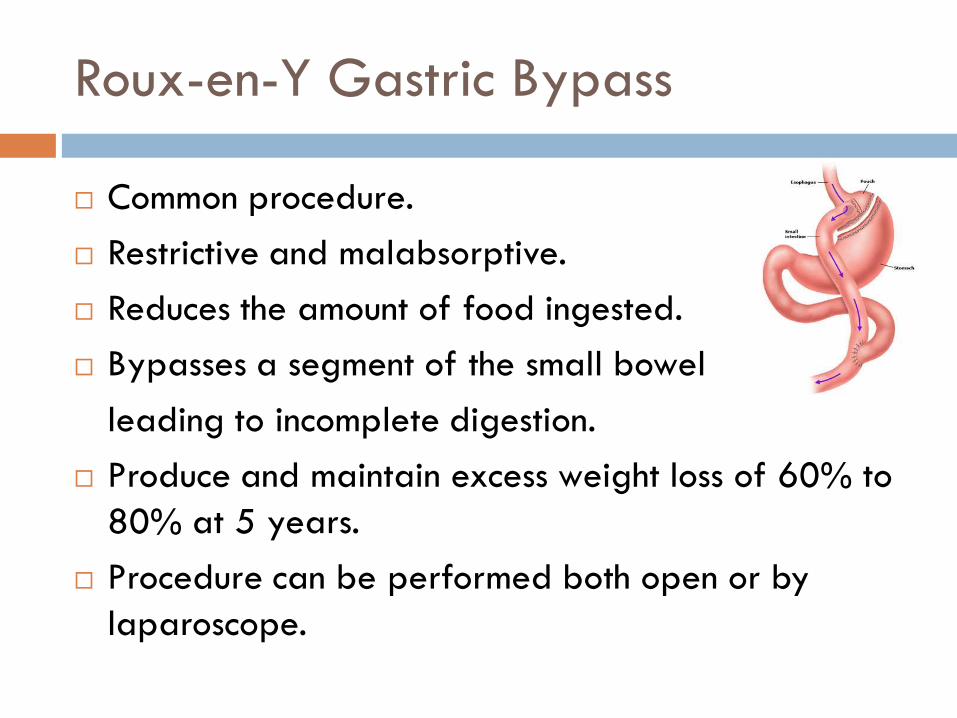
Roux-en-Y Gastric Bypass
Common procedure.
Restrictive and malabsorptive.
Reduces the amount of food ingested.
Bypasses a segment of the small bowel
leading to incomplete digestion.
Produce and maintain excess weight loss of 60% to
80% at 5 years.
Procedure can be performed both open or by
laparoscope.
Early Major Complications
Anastomotic leak with abscess: first few weeks
presenting with fever and tachycardia. Incidence in
Michigan < 1%. Common site is the
gastrojejunostomy.
Intra-abdominal or intraluminal bleeding: occurs at
the staple lines. Diagnosis is confirmed by
endoscope and most bleeding is treated
nonoperatively.
DVT or pulmonary embolism.
Abdominal Examination
Commonly unrevealing even with significant
pathology.
Obstruction in the bypassed segment will produce
vague symptoms.
Acute Abdominal Series will show no air fluid levels
and is of limited use.
CT abdominal is test of choice
Patients can sip contrast over 3 hours (230-300 ml).
Deteriorate rapidly so early consultation is
preferred.
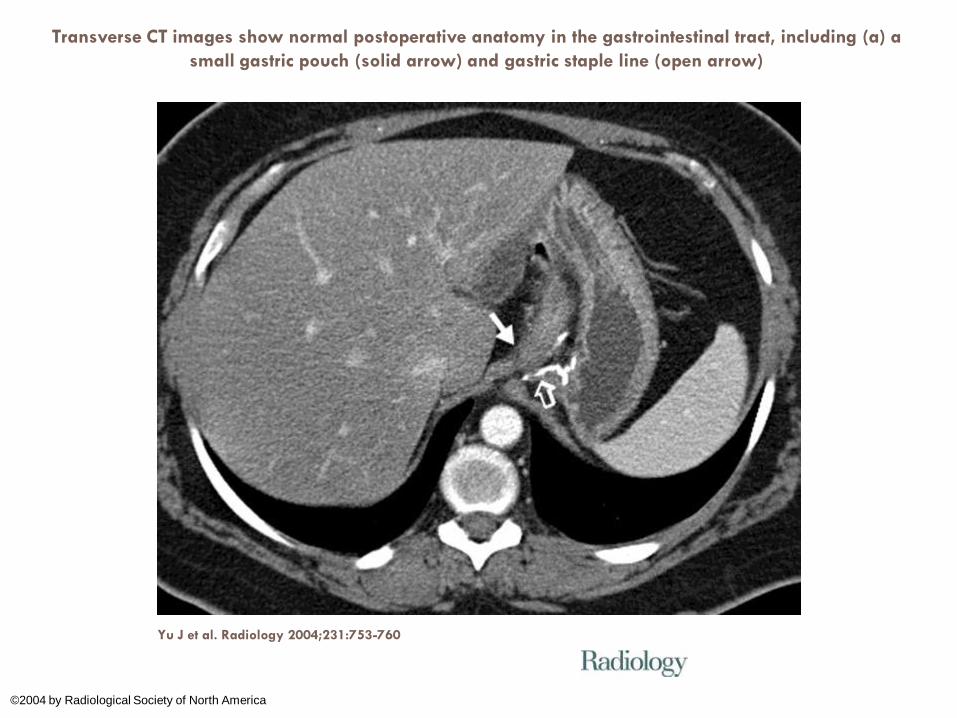
Transverse CT images show normal postoperative anatomy in the gastrointestinal tract, including (a) a
small gastric pouch (solid arrow) and gastric staple line (open arrow)
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
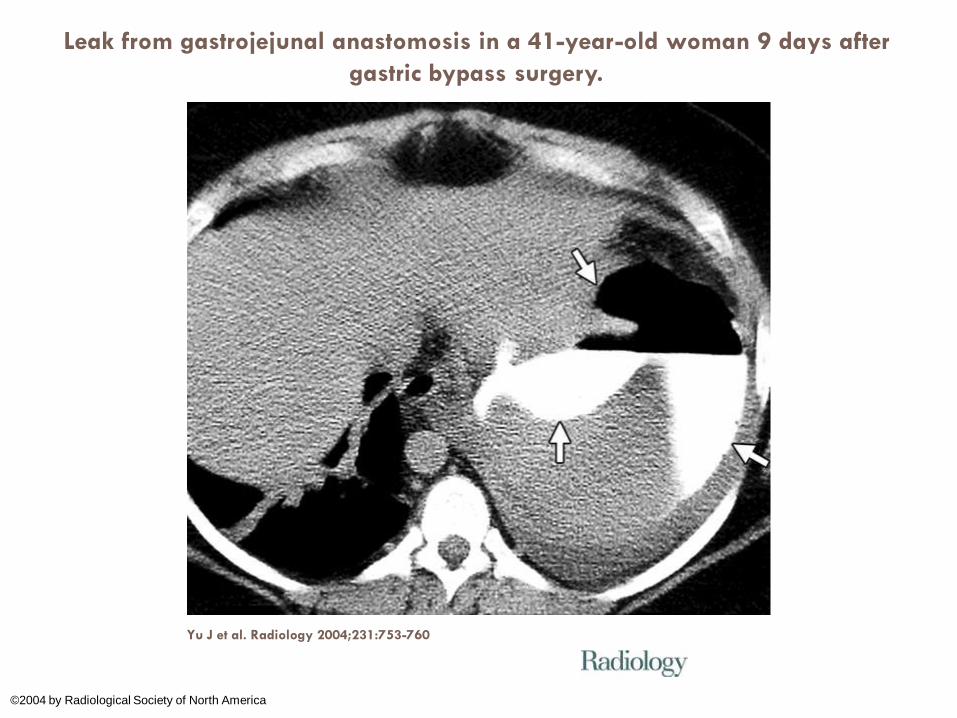
Leak from gastrojejunal anastomosis in a 41-year-old woman 9 days after
gastric bypass surgery.
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
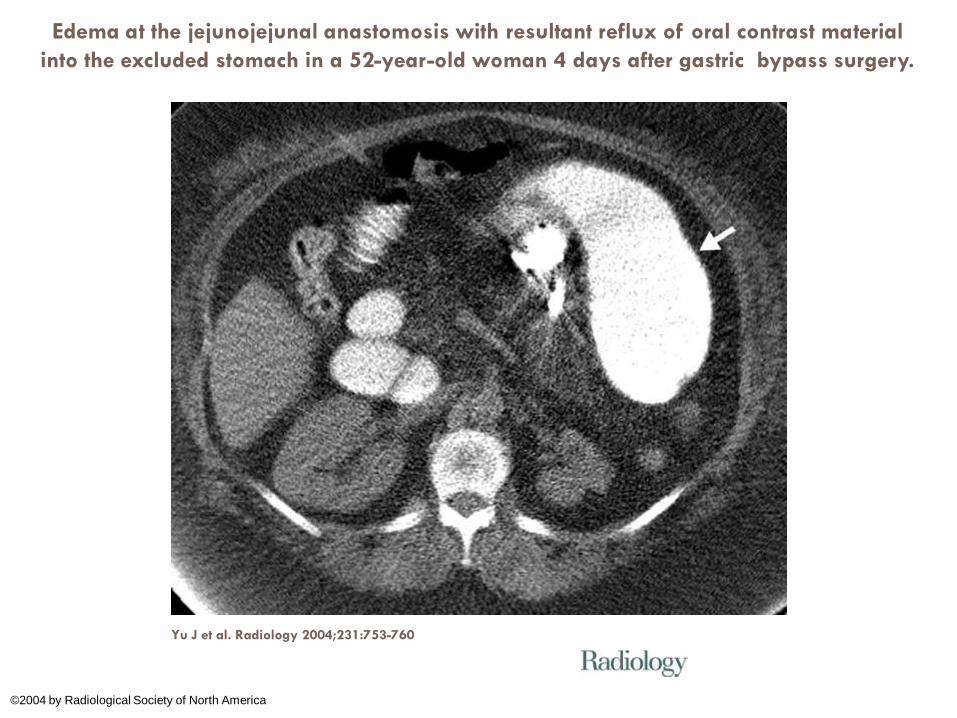
Edema at the jejunojejunal anastomosis with resultant reflux of oral contrast material
into the excluded stomach in a 52-year-old woman 4 days after gastric bypass surgery.
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
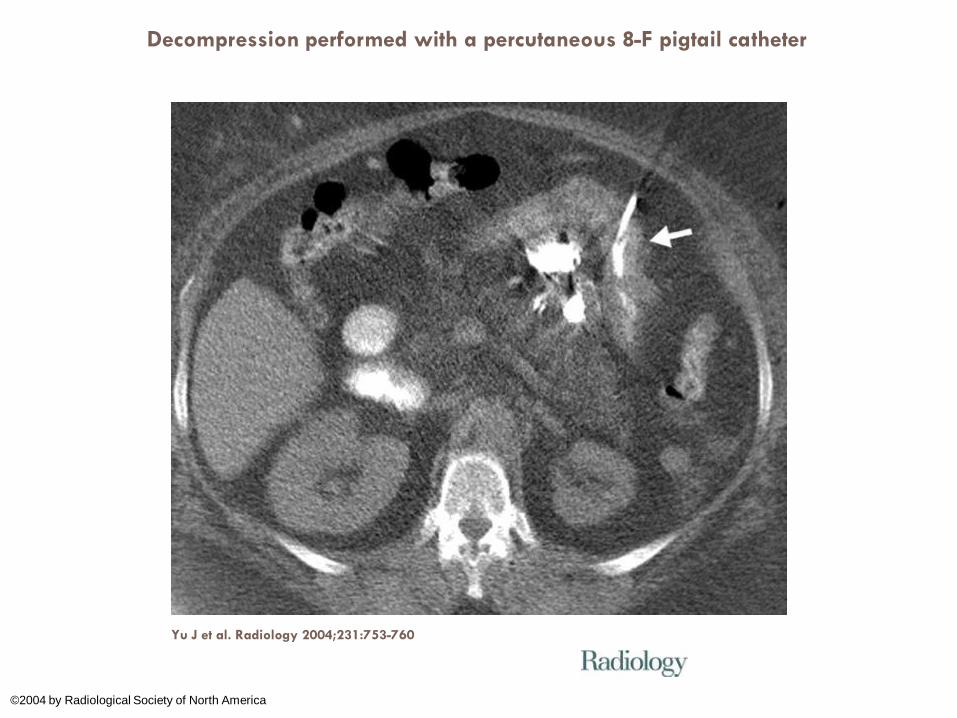
Decompression performed with a percutaneous 8-F pigtail catheter
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
Late Complications: Anatomic and Systemic
Anatomic: bowel obstruction, adhesions, strictures or
internal hernias.
Progressive inability to tolerate solids or liquids.
Anastomotic strictures can be managed
endoscopically with balloon dilatation.
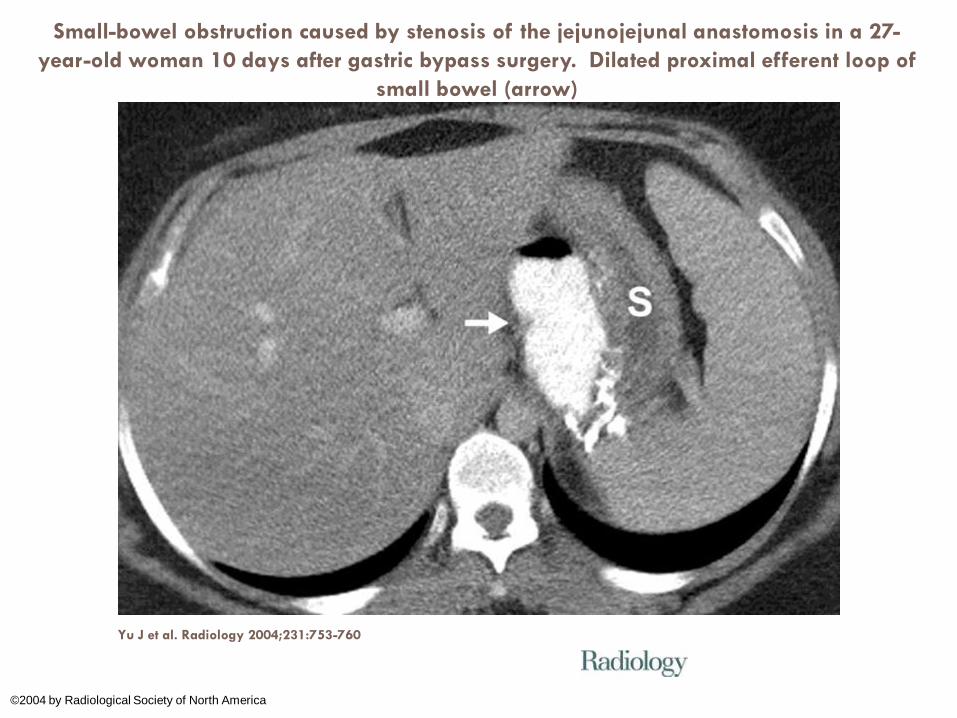
Small-bowel obstruction caused by stenosis of the jejunojejunal anastomosis in a 27-
year-old woman 10 days after gastric bypass surgery. Dilated proximal efferent loop of
small bowel (arrow)
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
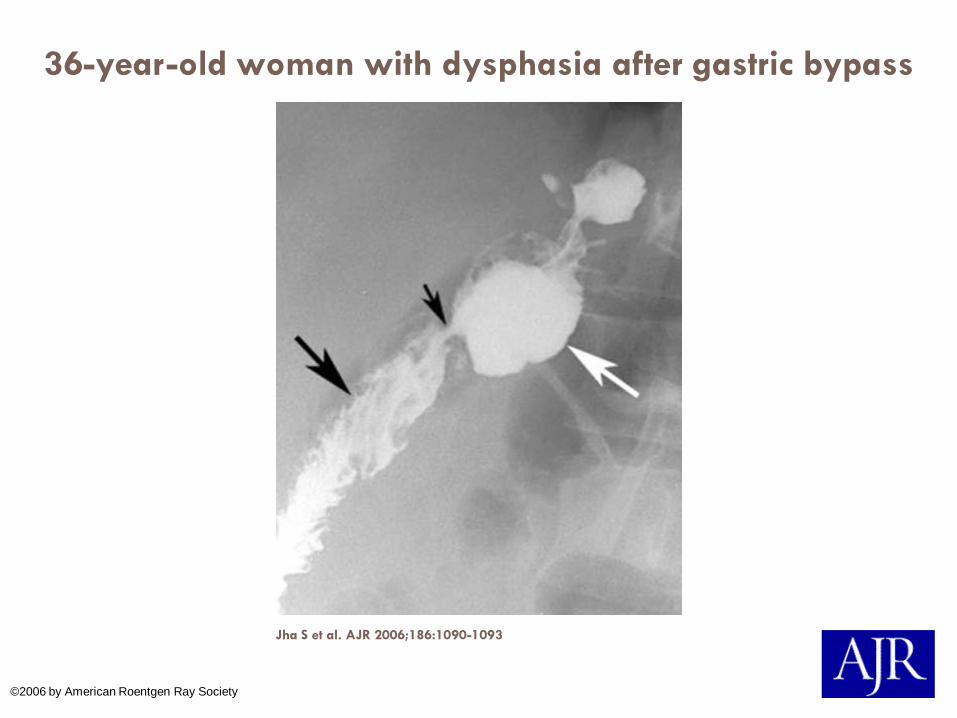
36-year-old woman with dysphasia after gastric bypass
surgery.
Jha S et al. AJR 2006;186:1090-1093
©2006 by American Roentgen Ray Society
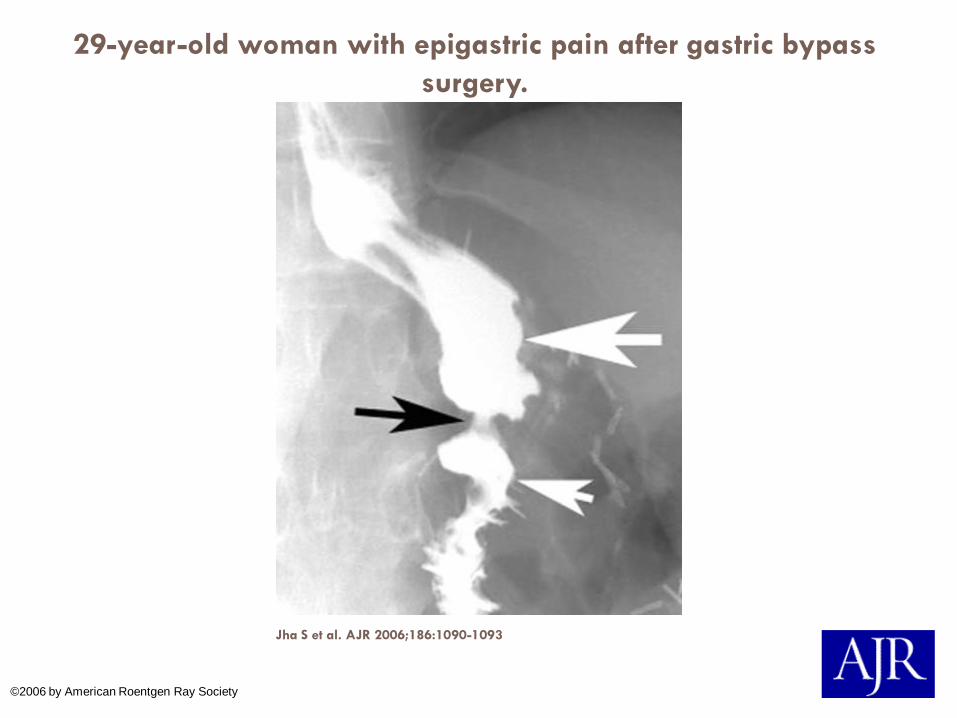
29-year-old woman with epigastric pain after gastric bypass
surgery.
Jha S et al. AJR 2006;186:1090-1093
©2006 by American Roentgen Ray Society
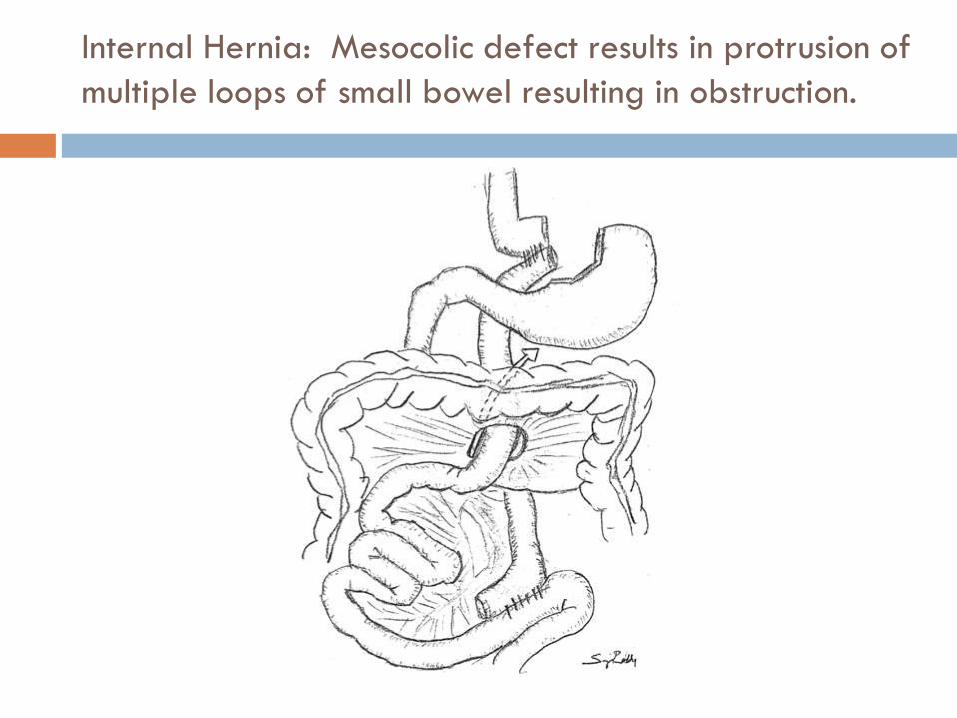
Internal Hernia: Mesocolic defect results in protrusion of
multiple loops of small bowel resulting in obstruction.
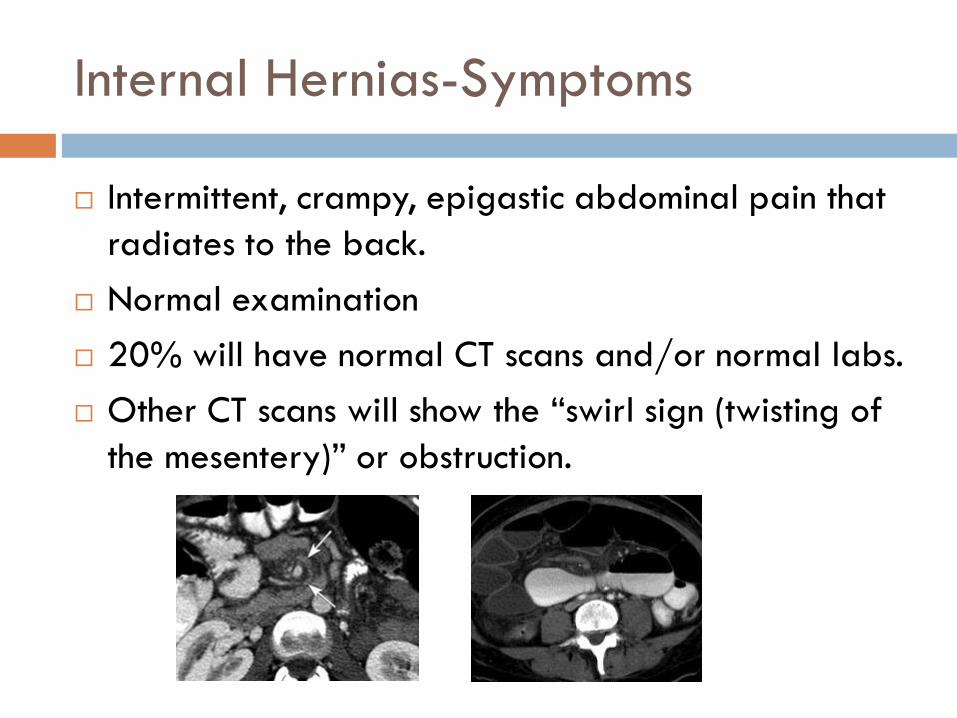
Internal Hernias-Symptoms
Intermittent, crampy, epigastic abdominal pain that
radiates to the back.
Normal examination
20% will have normal CT scans and/or normal labs.
Other CT scans will show the “swirl sign (twisting of
the mesentery)” or obstruction.
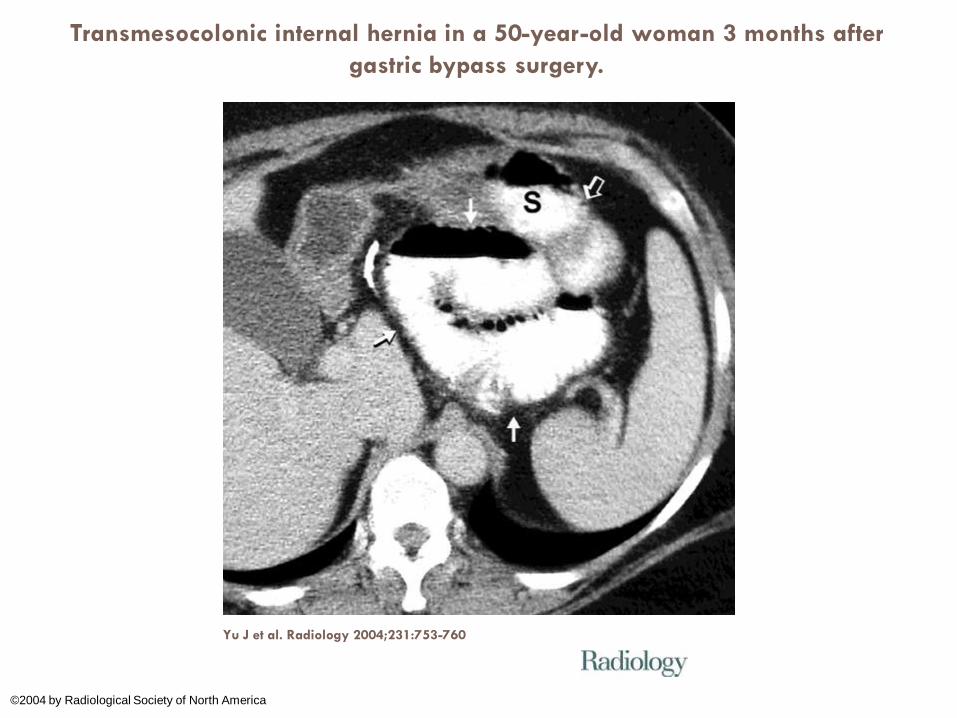
Transmesocolonic internal hernia in a 50-year-old woman 3 months after
gastric bypass surgery.
Yu J et al. Radiology 2004;231:753-760
©2004 by Radiological Society of North America
Systemic Late Complications
Nutritional deficiencies: Iron, Wernicke’s (B1),
vitamin B12, Vitamin D and calcium.
Secondary hyperparathyroidism: increased bone
turnover and decreased bone density.
Malabsorption of vitamin D leads to reduced
calcium absorption by the intestine leading to
hypocalcaemia and increased parathyroid hormone
secretion.
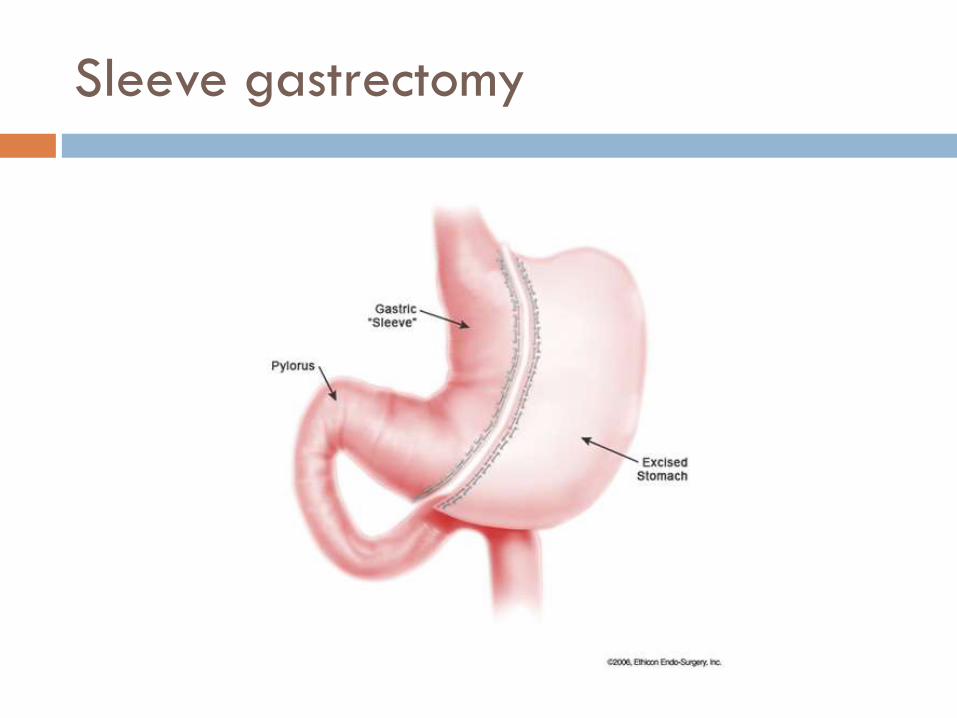
Sleeve gastrectomy

Sleeve gastrectomy
Equal with bypass. Restrictive and resective.
Longitudinal gastric resection, initially performed as
a treatment for peptic ulcer disease. Creates a
gastric tube by resecting the greater curvature of
the stomach. Performed open or by laparoscope.
Less risk of nutritional deficiencies.
Weight loss ranged from 33 to 85%.
Lower rate of resolution of diabetes mellitus and
hypertension.
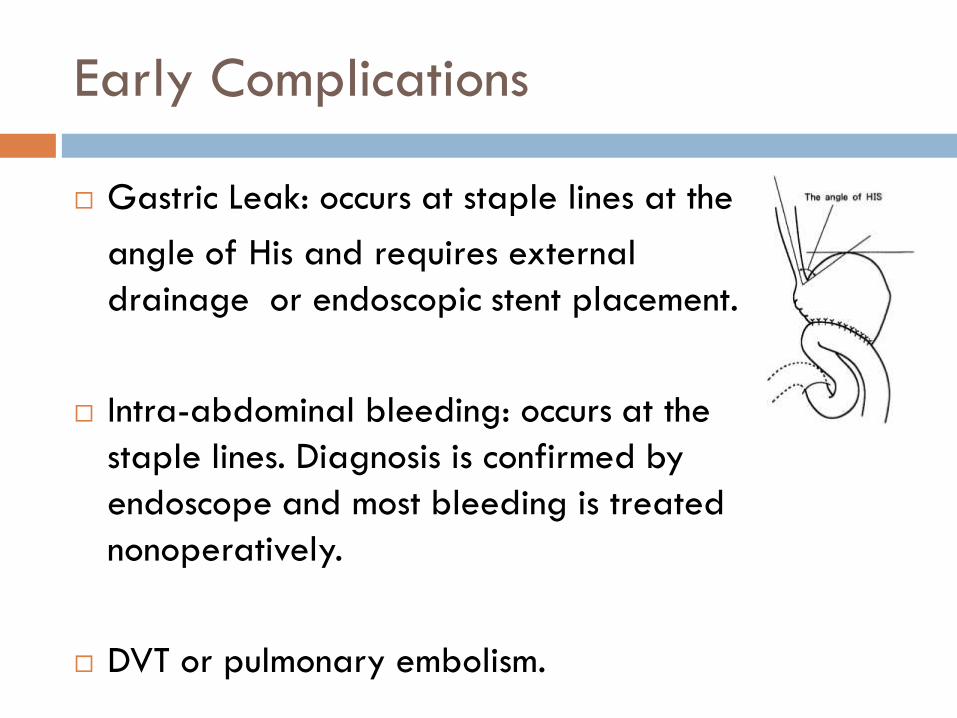
Early Complications
Gastric Leak: occurs at staple lines at the
angle of His and requires external
drainage or endoscopic stent placement.
Intra-abdominal bleeding: occurs at the
staple lines. Diagnosis is confirmed by
endoscope and most bleeding is treated
nonoperatively.
DVT or pulmonary embolism.
Late Complications
Bowel obstruction and adhesions. Rare with
laparoscopically performed procedures.
Gastroesophageal reflux disease (GERD): is
temporary and is gone by 3 months. Most GERD is
related to undiagnosed hiatal hernia. Surgeons
explore for hiatal hernia and repair at surgery.
Comparison of Bypass and Sleeve
Sleeve Gastrectomy has improved safety profile
compared to Bypass.
Lower rate of resolution of diabetes mellitus and
hypertension.
Mean excess weight loss approaches that of bypass
Laparoscopic adjustable gastric band
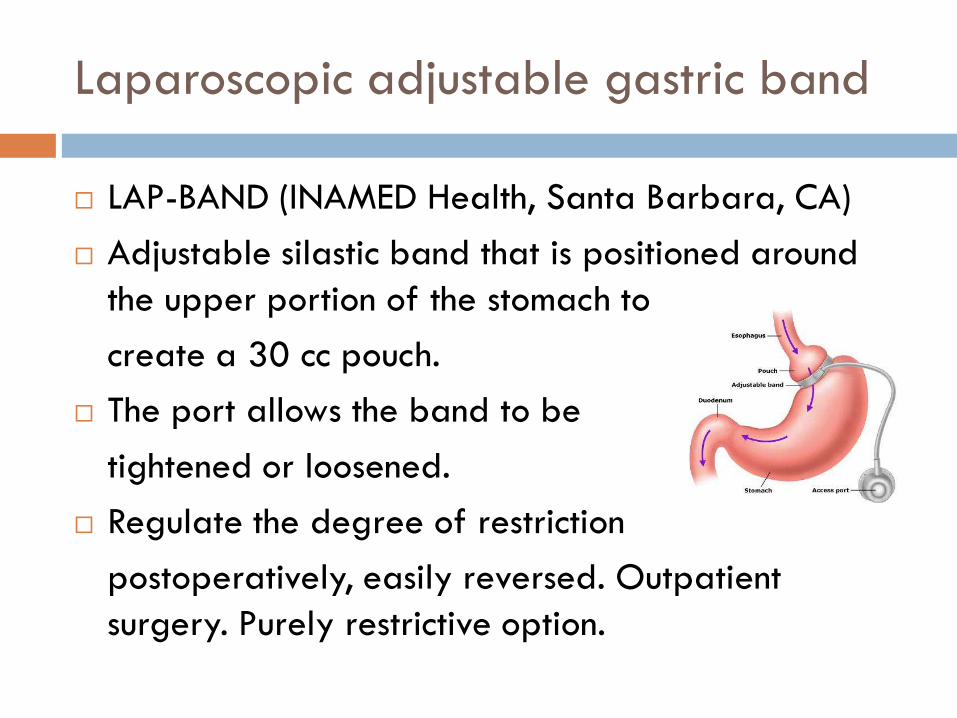
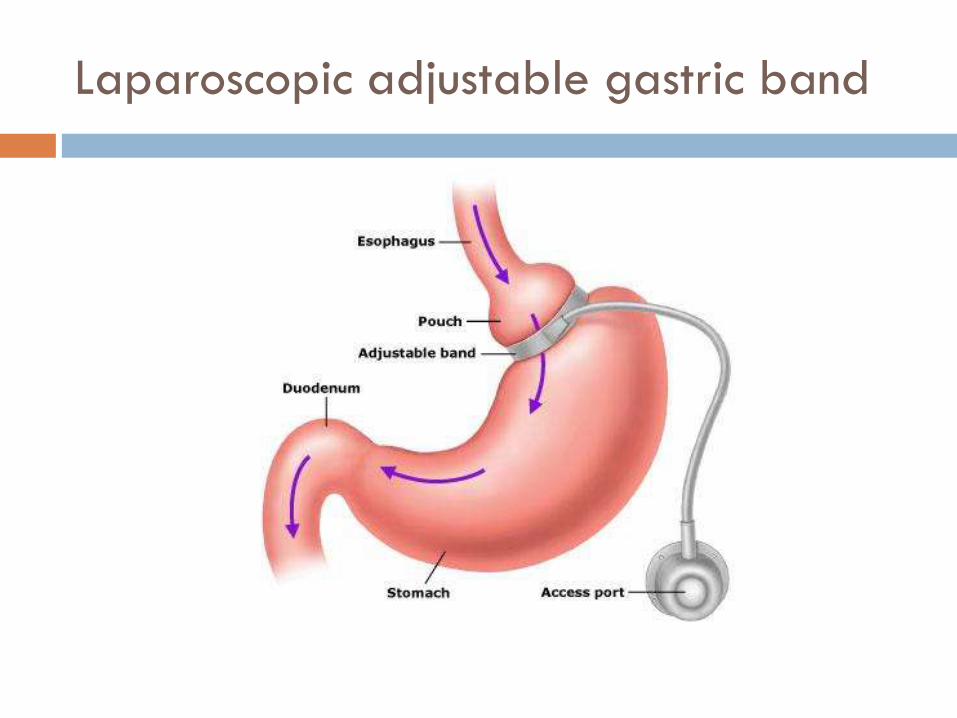
Laparoscopic adjustable gastric band
LAP-BAND (INAMED Health, Santa Barbara, CA)
Adjustable silastic band that is positioned around
the upper portion of the stomach to
create a 30 cc pouch.
The port allows the band to be
tightened or loosened.
Regulate the degree of restriction
postoperatively, easily reversed. Outpatient
surgery. Purely restrictive option.
Complications
Early: vomiting as a result of edema or proximal
movement of the band.
Late: Migration or slippage of the stomach resulting
in gastric dilatation. Gastric necrosis or perforation.
Deflation of the band can prevent obstruction.
Late: Gastric erosion occurs when band erodes the
stomach wall. Presents with sepsis, abscess or
fistulas.
Infection of the port site or device malfunction.
Comparison of Bypass and Band
Banding produces much less weight loss compared
to bypass (40.4% versus 74.6%). Better efficacy in
patients <40 years and BMI <50 kg/m².
Mechanical complications.
Patients prefer the device as the procedure is
outpatient.
Fewer metabolic derangements and lower mortality.
Long term outcomes show band device complications
and inadequate weight loss requiring removal of
the device (30%).

Biliopancreatic diversion with duodenal
switch
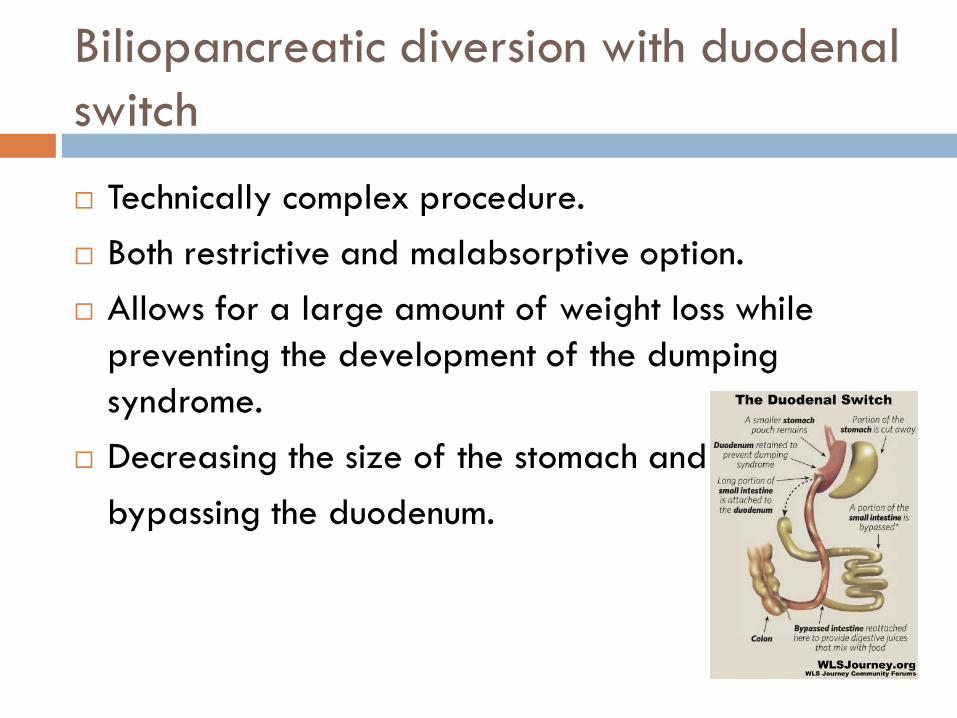
Biliopancreatic diversion with duodenal
switch
Technically complex procedure.
Both restrictive and malabsorptive option.
Allows for a large amount of weight loss while
preventing the development of the dumping
syndrome.
Decreasing the size of the stomach and
bypassing the duodenum.
Complications
Anastomotic leak with abscess.
Intra-abdominal bleeding
DVT or pulmonary embolism.
Bowel obstruction, adhesions, strictures or internal
hernias.
Nutritional deficiencies: Iron, Wernicke’s (B1),
vitamin B12, Vitamin D and calcium.
Fat-soluble-vitamin deficiencies. Selenium and zinc
deficiencies.
Hepatic dysfunction leading to jaundice and failure.
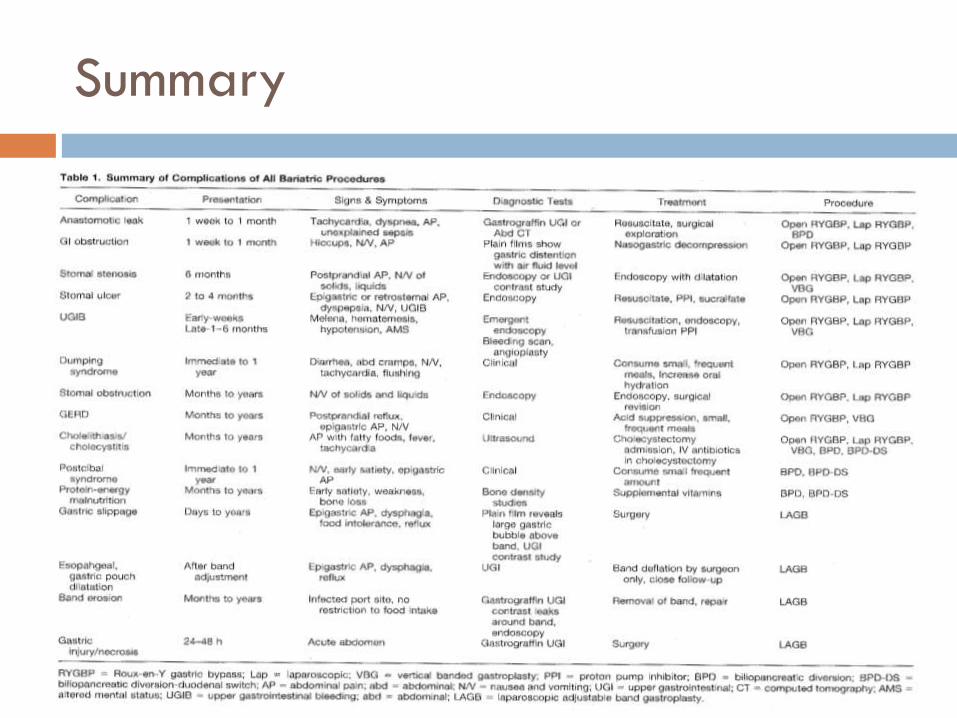
Summary
Conclusions
Obesity is a multifactorial disease with metabolic
consequences.
Adipocyte tissue (Fat) is an endocrine organ
Adipocytes have a limited lipid storage ability;
exceeding that limit sets up an inflammatory
response.
Bariatric surgery, specifically gastric bypass, is an
efficacious treatment for morbid obesity
Complications are common and can be life-
threatening.
Conclusions
High suspicion for complications when bariatric
surgery patients present to the ED.
Early complications are obstruction, leaks, bleeding
and PE.
Late complications are internal hernias, band slips,
erosions and strictures.
Eat your fruit and vegetables.




![Ophthalmic Complications of Bariatric Surgery · 2017-08-19 · ophthalmic complications have already occurred in patients after bariatric surgery [11, 13, 14]. Symptomatic vitamin](https://static.fdocuments.in/doc/165x107/5fab819e32d14352ae428938/ophthalmic-complications-of-bariatric-surgery-2017-08-19-ophthalmic-complications.jpg)