Adenomyosis: diagnostics andtreatmentAdenomyosis: diagnostics andtreatment...
6
Der Gynäkologe Leitthema Gynäkologe 2020 · 53:683–688 https://doi.org/10.1007/s00129-020-04655-7 Published online: 15 September 2020 © The Author(s) 2020 Redaktion L. Kiesel, Münster W. Janni, Ulm Harald Krentel 1 · Rudy Leon De Wilde 2 1 Clinic of Gynecology, Obstetrics, Gynecological Oncology and Senology, Bethesda Hospital Duisburg, Academic Teaching Hospital, Duisburg, Germany 2 Clinic of Gynecology, Obstetrics and Gynecological Oncology, University Hospital for Gynecology, Pius- Hospital Oldenburg, Medical Campus University of Oldenburg, Oldenburg, Germany Adenomyosis: diagnostics and treatment Adenomyosis can cause dysmen- orrhea, dyspareunia, bleeding disorders and pelvic pain and has a negative impact on fertility. The benign uterine disease can be found in almost 50% of patients with deep endometriosis, but also can appear without additional endometriosis. Adenomyosis is still underestimated and underdiagnosed and an exact in- cidence, especially related to patient age, is still not known. This might be related to the difficulties in diag- nosing adenomyosis, although the diagnostic tools have a high accuracy in the hands of the skilled examiner. Considering adenomyosis allows the individualization of medicinal and surgical treatment in symptomatic and/or infertile patients. e uterus is the central organ of the female pelvis and plays an indispensable role in reproduction. Adenomyosis is a benign disease of this important or- gan and knowledge about the impact of adenomyosis on symptomatology and fertility and its relation to additional peri- toneal or deep endometriosis has been increasing over the years. Although the exact incidence of adenomyosis re- mains unclear, the disease seems to affect women from adolescence to menopause. Many patients with adenomyosis are symptomatic and report dysmenorrhea, dyspareunia, central pelvic pain and bleeding disorders. e negative impact of adenomyosis on fertility is still un- der discussion but several publications have shown reduced pregnancy and birth rates and higher abortion rates in patients with adenomyosis undergoing reproductive treatment [1]. A risk for obstetric complications in patients with adenomyosis has recently been reported regarding premature birth, premature rupture of membranes, uterine rupture, postpartum hemorrhage, placentation failure and intrauterine fetal growth reduction [2]. It has been reported in various publications that medicinal and surgical treatment of adenomyosis may improve fertility [3] and reduces symptoms, although a standard for the treatment of infertile women with ade- nomyosis has not yet been established [4]. Hence it is of importance to con- sider adenomyosis as a possible factor in the diagnosis and treatment of all pa- tients withendometriosis, corresponding symptoms or infertility. e identifica- tion of patients with adenomyosis allows individualized treatment approaches in relation to family planning status. From anamnesis to transvaginal ultrasound—The diagnosis As always, the clinical diagnosis starts with a detailed anamnesis. e clinical symptoms can lead to the suspicion of adenomyosis as most of the patients have typical symptoms, such as dysmenor- rhea, bleeding disorders, chronic pelvic pain and dyspareunia. Adenomyosis might also be the reason for persistent symptoms aſter surgical interventions for peritoneal and deep endometrio- sis [5]. e gynecological examination may reveal a dolorous enlarged uterus and an additional palpable deep en- dometriosis of the retrocervical area [6]. Almost 50% of patients with deep endometriosis also have an involvement of the uterus. e most important di- agnostic tool in the daily gynecological practice is the transvaginal ultrasound [7]. Several typical ultrasound signs have been described in the literature: myometrial cysts, subendometrial mi- crocysts, question mark sign, heteroge- neous myometrium, uterine asymmetry, hyperechoic myometrial lesions, suben- dometrial thickening, disruption of the junctional zone, subendometrial linear striae and uterine enlargement (. Fig. 1). » The most important diagnostic tool in daily gynecological practice is transvaginal ultrasound Although the meaning of the particu- lar signs is not yet clear and a score system does not yet exist, the overall accuracy of 2D transvaginal ultrasound in the diagnosis of adenomyosis is high with a pooled sensitivity of 83.8% and a pooled specificity of 63.9% [8]. e 10- year meta-analysis [8] described the fea- ture heterogeneous myometrium as the sign with the highest pooled sensitivity, while globular uterine enlargement was the most specific sign. e combination with the feature question mark sign in- creased the accuracy. A similar review showed comparable results pointing out the high heterogeneity between the in- cluded studies and the missing consensus in adenomyosis classification [9]. Differ- ent publications showed a high variation Der Gynäkologe 10 · 2020 683
Transcript of Adenomyosis: diagnostics andtreatmentAdenomyosis: diagnostics andtreatment...
-
Der Gynäkologe
Leitthema
Gynäkologe 2020 · 53:683–688https://doi.org/10.1007/s00129-020-04655-7Published online: 15 September 2020© The Author(s) 2020
RedaktionL. Kiesel, MünsterW. Janni, Ulm
Harald Krentel1 · Rudy Leon DeWilde2
1 Clinic of Gynecology, Obstetrics, Gynecological Oncology and Senology, Bethesda Hospital Duisburg,Academic Teaching Hospital, Duisburg, Germany
2 Clinic of Gynecology, Obstetrics and Gynecological Oncology, University Hospital for Gynecology, Pius-Hospital Oldenburg, Medical Campus University of Oldenburg, Oldenburg, Germany
Adenomyosis: diagnosticsand treatment
Adenomyosis can cause dysmen-orrhea, dyspareunia, bleedingdisorders and pelvic pain and hasa negative impact on fertility. Thebenign uterine disease can be foundin almost 50% of patients with deependometriosis, but also can appearwithout additional endometriosis.Adenomyosis is still underestimatedand underdiagnosed and an exact in-cidence, especially related to patientage, is still not known. This mightbe related to the difficulties in diag-nosing adenomyosis, although thediagnostic tools have a high accuracyin the hands of the skilled examiner.Considering adenomyosis allows theindividualization of medicinal andsurgical treatment in symptomaticand/or infertile patients.
The uterus is the central organ of thefemale pelvis and plays an indispensablerole in reproduction. Adenomyosis isa benign disease of this important or-gan and knowledge about the impact ofadenomyosis on symptomatology andfertility and its relation to additional peri-toneal or deep endometriosis has beenincreasing over the years. Althoughthe exact incidence of adenomyosis re-mains unclear, the disease seems to affectwomen from adolescence to menopause.Many patients with adenomyosis aresymptomatic and report dysmenorrhea,dyspareunia, central pelvic pain andbleeding disorders. The negative impactof adenomyosis on fertility is still un-der discussion but several publicationshave shown reduced pregnancy andbirth rates and higher abortion rates in
patients with adenomyosis undergoingreproductive treatment [1]. A risk forobstetric complications in patients withadenomyosis has recently been reportedregarding premature birth, prematurerupture of membranes, uterine rupture,postpartum hemorrhage, placentationfailure and intrauterine fetal growthreduction [2]. It has been reportedin various publications that medicinaland surgical treatment of adenomyosismay improve fertility [3] and reducessymptoms, although a standard for thetreatment of infertile women with ade-nomyosis has not yet been established[4]. Hence it is of importance to con-sider adenomyosis as a possible factorin the diagnosis and treatment of all pa-tientswithendometriosis, correspondingsymptoms or infertility. The identifica-tion of patients with adenomyosis allowsindividualized treatment approaches inrelation to family planning status.
From anamnesis to transvaginalultrasound—The diagnosis
As always, the clinical diagnosis startswith a detailed anamnesis. The clinicalsymptoms can lead to the suspicion ofadenomyosis asmost of the patients havetypical symptoms, such as dysmenor-rhea, bleeding disorders, chronic pelvicpain and dyspareunia. Adenomyosismight also be the reason for persistentsymptoms after surgical interventionsfor peritoneal and deep endometrio-sis [5]. The gynecological examinationmay reveal a dolorous enlarged uterusand an additional palpable deep en-dometriosis of the retrocervical area
[6]. Almost 50% of patients with deependometriosis also have an involvementof the uterus. The most important di-agnostic tool in the daily gynecologicalpractice is the transvaginal ultrasound[7]. Several typical ultrasound signshave been described in the literature:myometrial cysts, subendometrial mi-crocysts, question mark sign, heteroge-neous myometrium, uterine asymmetry,hyperechoic myometrial lesions, suben-dometrial thickening, disruption of thejunctional zone, subendometrial linearstriae and uterine enlargement (. Fig. 1).
» The most importantdiagnostic tool in dailygynecological practice istransvaginal ultrasound
Although the meaning of the particu-lar signs is not yet clear and a scoresystem does not yet exist, the overallaccuracy of 2D transvaginal ultrasoundin the diagnosis of adenomyosis is highwith a pooled sensitivity of 83.8% anda pooled specificity of 63.9% [8]. The 10-year meta-analysis [8] described the fea-ture heterogeneous myometrium as thesign with the highest pooled sensitivity,while globular uterine enlargement wasthe most specific sign. The combinationwith the feature question mark sign in-creased the accuracy. A similar reviewshowed comparable results pointing outthe high heterogeneity between the in-cluded studies and themissing consensusin adenomyosis classification [9]. Differ-ent publications showed a high variation
Der Gynäkologe 10 · 2020 683
https://doi.org/10.1007/s00129-020-04655-7http://crossmark.crossref.org/dialog/?doi=10.1007/s00129-020-04655-7&domain=pdf
-
Leitthema
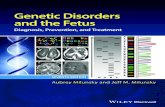
Fig. 18 Transvaginal ultrasound image of the uterus showing a suben-dometrialmicrocyst inadenomyosis(size4mm)withassociatedlinearstriae.(With permission©H. Krentel, all rights reserved)
Fig. 28 Transvaginal ultrasound image of the uterus showing a suben-dometrialmicrocyst inadenomyosis. Theadditional coloreddopplersonog-raphyhelps todistinguishbloodvessels (blue and red color) frommicrocystswith no color signal. (With permission©H. Krentel, all rights reserved)
Fig. 38Native tissue sample after hysterec-tomy showingmyometrial tissuewith suben-dometrial layer includingmicrocysts in adeno-myosis (3mm). (With permission©H. Krentel,all rights reserved)
in the most useful ultrasound features,varyingbetween linear striation,myome-trial cysts, question mark sign, hetero-geneous myometrium and asymmetri-cal myometrial thickening. Additionalsonographic techniques can help to con-firm the diagnosis of adenomyosis. Inthe examination of the junctional zoneand its typical irregularities in adeno-myosis, the 3D transvaginal ultrasoundseems to be superior to 2D sonography.Doppler sonography can be used to dis-tinguishadenomyosis (centralflow) fromfibroids (circular flow) by its typical flowcharacteristics and to differentiate smallmyometrial blood vessels from micro-cysts ([10]; . Fig. 2 and 3).
In combination with the clinical his-tory and gynecological examination,transvaginal ultrasound is a potent diag-nostic tool inthehandsoftheexperiencedexaminer. The consensus statement of
the morphological uterus sonographicassessment (MUSA) group on sono-graphic uterine features and the useof terminology summarized the actualstatus quo [11]. Specialized training anda standard ultrasound examination inall patients with typical symptoms mayhelp to detect adenomyosis.
» Magnetic resonance imagingis a potential diagnostic tool withhigh accuracy
Inorder todetect focal anddiffuse adeno-myosis and to presurgically localize andmeasure the affected uterine tissue, mag-netic resonance (MR) imaging is a poten-tial diagnostic tool with high accuracy.The most important diagnostic sign inMR imaging seems to be the irregular-ity of the junctional zone (JZ), followedby focal or diffuse thickening of the JZ,a JZ(max) to myometrial thickness ratio>40%, areas of myometrial low signal in-tensity and high signal intensity spots intheT2-weighted technique are the typicalfindings [12, 13]. Bazot et al. comparedtransvaginal ultrasound with MR imag-ing and reported no difference in accu-racy. In patients with additional uterinemyomas the sensitivity was higher inMRimaging [12].
Surgical diagnosis andhistological proof
Thenon-invasive diagnostic steps can becombined with operative diagnostic pro-cedures, such as diagnostic hysteroscopyand bipolar mini-resectoscopy. Thesetechniques allow the retrieval of biopsysamples and thus the histological proofof the presence of adenomyosis and canbe easily performed during surgery forendometriosis and infertility (. Fig. 4).In diagnostic hysteroscopy the uterinecavity and the endometrial layer can beinspected. Typical signs in adenomyosisare tiny openings in the endometrial sur-face, irregular endometrium, hypervas-cularization, strawberry pattern, fibrouscystic appearance of intrauterine lesionsand cystic hemorrhagic lesions [14]. Si-multaneously subendometrial adenomy-otic tissue resection and histopathologicexaminationcanbeperformed. Thediag-nostic specificity can be increased by thecombination of transvaginal ultrasoundand endomyometrial biopsy [15].
» Diagnostic findings canchange in relation to patientage, hormonal treatment andmenstrual cycle
Laparoscopic signs of adenomyosis canbe uterine enlargement, a pillowy resis-tance of the uterine wall, the blue signand cystic subseroushemorrhagic lesions
684 Der Gynäkologe 10 · 2020
-
(. Fig. 5). Laparoscopy-guided myome-trial biopsy techniques have been de-scribed as an accurate tool for obtaininga definitive diagnosis in patients with aclinical suspicion of adenomyosis [16].
The histologic proof can be helpful intherapeutic decisions, especially in casesof adenomyosis-related infertility. Theaccuracy of percutaneous, transvaginal,hysteroscopic and laparoscopic samplingtechniques varies in relation to exam-iner experience and quality of ultrasounddetection [17]. All diagnostic findingsin adenomyosis can change in relationto patient age, hormonal treatment andmenstrual cycle. In conclusion the di-agnosis or exclusion of adenomyosis bythe experienced gynecologist is possible.The individual combination of differentdiagnostic tools including imaging tech-niques and minimally invasive surgicalapproachesprovideahighaccuracy inthediagnosis of adenomyosis and in somecases even histological certainty.
Surgical treatment when familyplanning is completed
Adenomyosis can be treated by medici-nal and/or surgical approaches includingreproductive techniques. The decisionon how to treat adenomyosis individ-ually depends on the following factors:type of symptoms, family planning sta-tus, additional peritoneal and/or deependometriosis and age. In patientswith completed family planning ade-nomyosis can be definitively treated bylaparoscopic total hysterectomy or la-paroscopic subtotal hysterectomy whenthe uterine cervix is free of adenomyosisor retrocervical deep endometriosis.The laparoscopic approach allows theinspection of the complete pelvis andthus the simultaneous resection of ad-ditional endometriosis. In cases ofsubtotal hysterectomy, laparoscopic inbag morcellation of the uterine cor-pus should be performed in order toavoid iatrogenic new onset intraperi-toneal or retroperitoneal adenomyosis,endometriosis, metastatic myomatosis,sarcoma or late onset malignant trans-formation of uterine tissue. Abdominal,laparoscopic or hysteroscopic adenomy-omectomy in focal or cystic adenomyosis
Abstract · Zusammenfassung
Gynäkologe 2020 · 53:683–688 https://doi.org/10.1007/s00129-020-04655-7© The Author(s) 2020
H. Krentel · R. L. De Wilde
Adenomyosis: diagnostics and treatment
AbstractBackground. Adenomyosis is a frequentadditional condition in patients withendometriosis and should be included indiagnostic and treatment concepts.Objective. Description of diagnostic andtherapeutic approaches in patients withadenomyosis in relation to patient age, familyplanning status, peritoneal and/or deependometriosis and symptoms.Methods. The current literature onadenomyosis including case reports wasanalyzed. Due to the lack of evidenced-basedapproaches the most probable trends indiagnostics and treatment are discussed.Results. Adenomyosis plays an importantrole in fertile patients with dysmenorrhea,dyspareunia and pelvic pain, with or withoutadditional peritoneal or deep endometriosis.
It has a negative impact on fertility and cancause a variety of symptoms. The diseasecan be diagnosed by a skilled examiner andtreatment concepts exist.Conclusion. Adenomyosis can be diagnosedby a combination of clinical history,gynecological examination, transvaginalultrasound and magnetic resonance imaging.Various medical and surgical treatmentapproaches are available to reduce symptomsand to increase fertility. The course of actiondepends on the family planning status of thepatient.
KeywordsEndometriosis · Infertility · Dyspareunia ·Dysmenorrhea · Transvaginal ultrasound
Adenomyose: Diagnostik und Therapie
ZusammenfassungHintergrund. Die Adenomyose ist einehäufig auftretende Begleiterkrankungbei Patientinnen mit Endometriose undsollte in Diagnostik und therapeutischenBehandlungskonzepte mit einbezogenwerden.Ziel. Beschreibung der diagnostischen undtherapeutischen Ansätze bei Patientenmit Adenomyose in Bezug auf Alter,Familienplanungsstatus, Peritoneal- und/odertiefe Endometriose und Symptome.Methoden. Die aktuelle Literatur zurAdenomyose einschließlich der Fallberichtewurde analysiert. Aufgrund mangelnderevidenzbasierter Ansätze werden diewichtigsten Entwicklungen in Diagnostik undTherapie diskutiert.Ergebnisse. Die Adenomyose spielt einebedeutende Rolle bei fruchtbaren Patien-tinnen mit Dysmenorrhö, Dyspareunie undBeckenschmerzen,mit oder ohne zusätzlichePeritoneal- oder tiefe Endometriose. Sie
wirkt sich negativ auf die Fruchtbarkeit ausund kann eine Vielzahl von Symptomenverursachen. Die Erkrankung kann von einemqualifizierten Untersucher diagnostiziertwerden. Für die Therapie stehen diverseBehandlungskonzepte zur Verfügung.Schlussfolgerung. Die Adenomyose kanndurch eine Kombination aus klinischerAnamnese, gynäkologischer Untersuchung,transvaginalem Ultraschall und Magnetre-sonanztomographie (MRT) diagnostiziertwerden. Zur Linderung der Symptome undzur Erhöhung der Fruchtbarkeit stehenverschiedene medizinische und chirurgischeBehandlungsansätze zur Verfügung. Dasweitere Vorgehen richtet sich nach demFamilienplanungsstatusder Patientin.
SchlüsselwörterEndometriose · Infertilität · Dyspareunie ·Dysmenorrhö · Transvaginaler Ultraschall
and cytoreductive surgical procedures indiffuse adenomyosis can reduce symp-toms in patients who wish to preservethe uterus. Focal subendometrial or in-tramural cystic adenomyotic lesions andintracavitary polypoid adenomyoma canbe treated by hysteroresectoscopy. Newinstruments with a smaller diameter alsoprovide a minimally invasive approach
in very young nulliparous women. Thehysteroscopic resection of adenomyoticlesions improves symptoms. Larger in-tramural cystic lesions should be treatedby laparoscopic resection and uterinesuturing (. Fig. 6; [18]). The influenceof these procedures on patient fertilityshould by further investigated.
Der Gynäkologe 10 · 2020 685
https://doi.org/10.1007/s00129-020-04655-7
-
Leitthema
Fig. 48 Bipolarmini-hysteroresectoscopicbiopsytechnique. (Withpermission©H.Krentel,all rights reserved)
Endometrial ablation offers a less in-vasive treatment option in patients whowant to preserve the uterus; however, theefficacy in controlling bleeding decreasesover time [19].
Medical treatment options
Another treatment option is the useof a levonorgestrel intrauterine device(LNG-IUD), gestagens or combinedoral contraceptives. In the subgroup ofpatients with ongoing family planningthe medical treatment can only be anoption as a pretreatment before repro-ductive procedures or as a prophylactictreatment in very young women withadenomyosis and a pregnancy wish inthe future. In these cases a long-termtreatment with low complication ratesand the aim to prevent a worsening of theuterine situation is required. All med-ical therapeutic possibilities in patientswith adenomyosis have been recentlyreviewed by various authors [20, 21].The suppressive hormonal treatmentswith high dose progestins, oral con-traceptives, LNG-IUDs, gonadotropin-releasing hormone (GnRH) agonists,aromatase inhibitors, selective estrogenreceptor modulator (SERM) and selec-tive progesterone receptor modulator(SPRM) are able to reduce symptomsby reduction of adenomyosis; however,each of these treatments is related tospecific side effects. Currently, all med-ical approaches represent an off-labeluse as no medical solution is licensed inthe specific treatment of adenomyosis.
Dienogest is able to reduce adenomyosis-relatedpelvic pain anddysmenorrheabutis combined with a high risk of irregularuterine bleeding as the most commonadverse reaction. Therefore, patientstreated with dienogest have a certainrisk of treatment discontinuation espe-cially when they are of young age, haveanemia before treatment and/or havemildly supressed or unsuppressed estra-diol after starting dienogest treatment[22]. Also, progestins such as norethis-terone acetate or medroxyprogesteronacetate can reduce pain in patients withadenomyosis but are related to side ef-fects, such as acne, edema and reductionof libido causing high discontinuationrates. Combined oral contraceptivesrepresent another evidence-based ther-apeutic option. The data show a painreduction but also bleeding disordersas the main adverse effect. The LNG-IUD seems to be the most effectiveoption in reducing pain and menstrualblood loss [23]. The LNG-IUDs can beused in women with completed familyplanning instead of hysterectomy, and asamaintenance therapyafteradenomyosissurgery. In a retrospective analysis oftreatment with LNG-IUD in patientswith a large uterine adenomyosis andheavy menstrual bleeding, 10% under-went premature LNG-IUD removal and16.7% underwent subsequent hysterec-tomy [24]. The incidence of spontaneousexpulsion of the IUD is higher in pa-tients with adenomyosis and/or uterinefibroids than in women with a normaluterus and seems to depend on theinsertion technique and the placementtiming. The role of LNG-releasing in-trauterine systems in the treatment ofadolescent or very young women withadenomyosis, especially the use of low-dose IUDs should be investigated. Theuse of LNG-IUDs prior to assisted re-production also has been described buthas not yet been scientifically evaluated.Another medical treatment option isthe use of GnRH agonists or antago-nists. The application can be presurgical,postsurgical, prior to assisted repro-ductive techniques or as an individualapproach instead of other medical treat-ments. The presurgical treatment canreduce complications and bleeding in
adenomyosis surgery. The combina-tion of GnRH agonist application withconservative surgery seems to resultin longer symptom control and betterreproductive outcomes in symptomaticand subfertile patients with adenomyosiscompared with GnRH treatment alone.In infertile women with adenomyosisthe treatment with GnRH agonists isindicated before fertility treatment inorder to increase pregnancy and birthrates and decrease abortion rates [25].The efficacy of GnRH agonists in ado-lescents with refractory chronic pelvicpain, failed therapy with combined oralcontraceptives and positive MR imagingfor adenomyosis has been reported. Thetreatment improved symptoms and re-peated MR imaging showed regressionof the lesions [26]. As estrogen, estrogenreceptors and aromatase play a role inthe pathogenesis of adenomyosis, thetherapeutic use of aromatase inhibitorsis an additional option. The reductionof adenomyosis volume and symptomshas been shown; however only a fewpublications exist and further investiga-tions are needed. Selective progesteronereceptor modulators, selective estrogenreceptor modulators, valproic acid andantiplatelet treatment represent anothergroup of treatment options, which needsto be investigated before used in the dailyroutine. So far, the medical treatment ofadenomyosis especially in patients withongoing family planning is an individualrecommendation, while the situation inpatients with completed family planningis based on a large number of publi-cations, especially regarding the use ofLNG-IUDs.
Surgical or combined treatmentoptions in patients withongoing family planning
Patients with adenomyosis and infertil-ity have various treatment options; how-ever none of these options is evidencebased. Onewaycouldbe thedirect repro-ductive approach with or without med-ical pretreatment. Another way couldbe the combination with uterus-sparingsurgery, such as adenomyectomy or cy-toreduction. The questions are if surgeryhas an additional benefit for infertile pa-
686 Der Gynäkologe 10 · 2020
-
Fig. 58 Laparoscopic viewof subserous cystic adenomyosis. (Withpermis-sion,©H. Krentel, all rights reserved)
Fig. 68 Transvaginalultrasoundimageofanintramuralcysticadenomyosisin patientwith ongoing family planning. (With permission©H. Krentel, allrights reserved)
tients with adenomyosis and what wouldbe the right moment for surgery? Ina recent literature review these optionsincluding medical and surgical methods,highlightingtreatmentstrategies, butalsothe lack of knowledge and the difficultiesin suggesting evidence-based treatments,has been discussed [27]. An importantfactor in the patient selection for surgeryis the patients age, which should be lessthan 39 years [28]. Additional surgerymight be an option in symptomatic pa-tients, who are not able to undergo re-productive procedures, patients with in-fertility despite in vitro fertilization andintracytoplasmic sperm injection (IVF/ICSI) and as a last resort in extreme casesof diffuse adenomyosis. Surgery mightbe helpful in matters of fertility but theeffect of surgery needs to be proven inthe future [3].
» Important in patient selectionfor surgery is that patients shouldbe less than 39 years old
In a recent reviewanoverall clinical preg-nancy rate of 18.2% after surgical treat-ment of adenomyosis was described. Theadditional postoperative treatment withGnRH agonists increased the rate up to40%[29]. Therisksofsurgicalproceduresin adenomyosis should not be underes-timated. The surgery can be difficult andthe loss of organs due to severe intra-operative bleeding has been described.Adenomyosis surgery can cause uterine
rupture, postsurgical intrauterine and in-tra-abdominal adhesions and irregularplacentation. In order to minimize com-plications adenomyosis surgery shouldbe carried out in specialized centers withexperienced gynecological surgeons.
New minimally invasivetreatment options
High-intensityfocusedultrasound(HIFU)and radiofrequency ablation are alter-native treatment methods for focal anddiffuse adenomyosis. Both techniquesprovide symptom relief and a low rateof major and minor complications inpatients who wish to preserve the uterusor to conceive in the future. In recentpublications patients undergoing HIFUfor adenomyosis showed high concep-tion and live birth rates after treatment[30]; however, the role of HIFU in pa-tients who wish to conceive should befurther investigated. The transcervicalradiofrequency ablation for symptomaticadenomyosis has also been reported tobe a safe and effective method. Also,uterine artery embolization can reducesymptoms and improve the quality oflife in patients with symptomatic ade-nomyosis. The impact of uterine arteryembolization on fertility and pregnancyrequires further evaluation. The litera-ture describes awide range of therapeuticoptions, but none of them are evidencebased and in relation to effectiveness, fer-tility outcome, reliability and side effectsmany questions still remain unanswered.
Prospective randomized trials areneededin order to show if medicinal, surgical orreproductive treatment alone or a com-bination is the best way to improvefertility in patients with adenomyosis.Patients with adenomyosis need an indi-vidual approach with detailed diagnosisof the extent of the disease and an ac-curate planning of the medicinal and/orsurgical treatment.
Recommendations for dailypractice
4 Adenomyosis is a frequent benignuterine disease,
4 Dysmenorrhea, dyspareunia, pelvicpain and bleeding disorders aretypical symptoms,
4 Adenomyosis has a negative impacton fertility,
4 Adenomyosis can be diagnosed bya combination of clinical history,gynecological examination andtransvaginal 2D ultrasound,
4 MR imaging can be useful as anadditional diagnostic tool,
4 The treatment approach depends onthe patient’s family planning and thetype and localization of the disease,
4 Medicinal treatment and surgicalresection of adenomyosis can reducesymptoms,
4 Adenomyosis surgery should only beperformed in specialized centers.
Der Gynäkologe 10 · 2020 687
-
Leitthema
Corresponding address
Dr. Harald KrentelClinic of Gynecology,Obstetrics, GynecologicalOncology and Senology,Bethesda Hospital Duisburg,Academic Teaching HospitalDuisburg, [email protected]
Compliance with ethicalguidelines
Conflict of interest. H. Krentel andR.L. DeWildedeclare that theyhave no competing interests.
Ethical standards. For this article no studieswithhumanparticipants or animalswere performedbyanyof the authors. All studies performedwere inaccordancewith the ethical standards indicated ineach case.
Open Access. This article is licensedunder a CreativeCommonsAttribution 4.0 International License,whichpermits use, sharing, adaptation, distribution and re-production in anymediumor format, as long as yougive appropriate credit to the original author(s) andthe source, provide a link to the Creative Commons li-cence, and indicate if changesweremade. The imagesor other third partymaterial in this article are includedin the article’s Creative Commons licence, unless in-dicatedotherwise in a credit line to thematerial. Ifmaterial is not included in the article’s Creative Com-mons licence and your intendeduse is not permittedby statutory regulation or exceeds the permitteduse,youwill need toobtain permissiondirectly from thecopyright holder. To viewa copyof this licence, visithttp://creativecommons.org/licenses/by/4.0/.
References
1. Younes G, Tulandi T (2017) Effects of adenomyosison in vitro fertilization treatment outcomes:ameta-analysis. Fertil Steril 108(3):483–490
2. Buggio L, Monti E, Gattei U, Dridi D, Vercellini P(2017) Adenomyosis: fertility and obstetricoutcome. A comprehensive literature review.Minerva Ginecol. https://doi.org/10.23736/S0026-4784.17.04163-6
3. Dueholm M (2017) Uterine adenomyosis andinfertility, reviewof reproductive outcomeafter invitro fertilizationandsurgery. ActaObstetGynecolScand96(6):715–726
4. TamuraH, KishiH, KitadeM,Asai-SatoM, TanakaA,Murakami T, Minedishi T, Sugino N (2017) Clinicaloutcomes of infertility treatment for womenwith adenomyosis in Japan. Reprod Med Biol16(3):276–282
5. Ferrero S, Camerini G, Menada MV, Biscaldi E,RagniN, RemorgidaV (2009)Uterineadenomyosisin persistence of dysmenorrhea after surgicalexcision of pelvic endometriosis and colorectalresection. JReprodMed54(6):366–372
6. Krentel H, Cezar C, Becker S, Di Spiezio Sardo A,Tanos V, Wallwiener M, De Wilde RL (2017) From
clinical symptomstoMRimaging: diagnostic stepsinadenomyosis. BiomedRes Int2017:1514029
7. Graziano A, Lo Monte G, Piva I, Caserta D,Karner M, Engl B, Marci R (2015) Diagnosticfindings in adenomyosis: a pictorial review onthe major concerns. Eur Rev Med Pharmacol Sci19(7):1146–1154
8. Andres MP, Borelli GM, Ribeiro J, Baracat EC,AbraoMS, KhoRM (2018) Transvaginal ultrasoundfor the diagnosis of adenomyosis: systematicreview and meta-analysis. J Minim InvasiveGynecol25(2):257–264
9. Bazot M, Darai E (2018) Role of transvaginalsonography and magnetic resonance imaging inthe diagnosis of uterine adenomyosis. Fertil Steril109(3):389–397
10. Benagiano G, Brosens I, Habiba M (2015) Adeno-myosis: a life-cycle approach. Reprod BiomedOnline30(3):220–232
11. VandenBosch T, DueholmM, Leone FP, Valentin L,Rasmussen CK, Votino A, Van Schoubroeck D,Landolfo C, Installé AJ, Guerriero S, Exacoustos C,Gordts S, Benacerraf B, D’Hooghe T, De Moor B,Brölmann H, Goldstein S, Epstein E, Bourne T,Timmerman D (2015) Terms, definitions andmeasurements to describe sonographic featuresof myometrium and uterinemasses: a consensusopinion from the Morphological Uterus Sono-graphic Assessment (MUSA) group. UltrasoundObstetGynecol46(3):284–298
12. Bazot M, Cortez A, Darai E, Rouger J, Chopier J,Antoine JM, Uzan S (2001) Ultrasonographycompared with magnetic resonance imaging forthe diagnosis of adenomyosis: correlation withhistopathology. HumReprod16(11):2427–2433
13. Novellas S, Chassang M, Delotte J, Toullalan O,Chevallier A, Bouaziz J, Chevallier P (2011) MRIcharacteristics of theuterine junctional zone: fromnormal to the diagnosis of adenomyosis. AJRAmJRoentgenol196(5):1206–1213
14. Di Spiezio Sardo A, Calagna G, Santangelo F,Zizolfi B, Tanos V, Perino A, DeWilde RL (2017) Theroleofhysteroscopyinthediagnosisandtreatmentofadenomyosis. BiomedRes Int2017:2518396
15. Dakhly DM, Abdel Moety GA, Saber W, GadAllah SH, Hashem AT, Abdel Salam LO (2016) Theaccuracyofhysteroscopicendomyometrial biopsyin diagnosis of adenomyosis. J Minim InvasiveGynecol23(3):364–371
16. Jeng CJ, Huang SH, Shen J, Chou CS, Tzeng CR(2007) Laparoscopy-guided myometrial biopsyin the definite diagnosis of diffuse adenomyosis.HumReprod22(7):2016–2019
17. Movilla P, Morris S, Isaacson K (2019) A systematicreview of tissue sampling techniques for thediagnosis of adenomyosis. J Minim InvasiveGynecol. https://doi.org/10.1016/j.jmig.2019.09.001
18. Gordts S, CampoR, Brosens I (2014)Hysteroscopicdiagnosis and excision of myometrial cysticadenomyosis. GynecolSurg11(4):273–278
19. Philip CA, Le Mitouard M, Maillet L, de Saint-Hilaire P,HuissoudC, CortetM,DubernardG (2018)Evaluation of Novasure global endometrial abla-tion in symptomatic adenomyosis: a longitudinalstudy with a 36 month follow-up. Eur J ObstetGynecolReprodBiol227:46–51
20. Vannuccini S, Luisi S, Tosti C, Sorbi F, Petraglia F(2018) The role of medical therapy in themanagement of uterine adenomyosis. Fertil Steril109(3):398–405
21. Pontis A, D’Alterio MN, Pirarba S, de Angelis C,Tinelli R, Angioni S (2016) Adenomyosis: a sys-
tematic reviewof themedical treatment. GynecolEndocrinol32(9):696–700
22. Nagata C, Yanagida S, Okamoto A, Morikawa A,Sugimoto K, Okamoto S, Ochiai K, Tanaka T(2012) Risk factors of treatment discontinuationdue to uterine bleeding in adenomyosis patientstreated with dienogest. J Obstet Gynaecol Res38(4):639–644
23. Imai A, Matsunami K, Takagi H, Ichigo S (2014)Levonorgestrel-releasing intrauterinedeviceusedfor dysmenorrhea: five-year literature review. ClinExpObstetGynecol41(5):495–498
24. Park DS, Kim ML, Song T, Yun BS, Kim MK,Jun HS, Seong SJ (2015) Clinical experiences ofthe levonorgestrel-releasing intrauterine systemin patients with large symptomatic adenomyosis.TaiwanJObstetGynecol54(4):412–415
25. Streuli I, Dubuisson J, Santulli P, de Ziegler D,Batteux F, Chapron C (2014) An update on thepharmacological management of adenomyosis.ExpertOpinPharmacother15(16):2347–2360
26. MansouriR, SantosXM,Bercaw-Pratt JL,DietrichJE(2015) Regression of adenomyosis on magneticresonance imaging after a course of hormonalsupression in adolescents: a case series. J PediatrAdolescGynecol28(6):437–440
27. DueholmM(2018)Minimally invasivetreatmentofadenomyosis. BestPractResClinObstetGynaecol.https://doi.org/10.1016/j.bpobgyn.2018.01.016
28. Kishi Y, Yabuta M, Taniguchi F (2014) Whowill benefit from uterus-sparing surgery inadenomyosis-associated subfertility? Fertil Steril102(3):802–807
29. Rocha TP, AndresMP, Borelli GM, AbraoMS (2018)Fertility-sparing treatment of adenomyosis inpatients with infertility: a systematic review ofcurrentoptions. ReprodSci25(4):480–486
30. Zhang L, Rao F, Setzen R (2017) High intensityfocused ultrasound for the treatment of adeno-myosis: selection criteria, efficacy, safety andfertility. ActaObstetGynecolScand96(6):707–714
688 Der Gynäkologe 10 · 2020
http://creativecommons.org/licenses/by/4.0/https://doi.org/10.23736/S0026-4784.17.04163-6https://doi.org/10.23736/S0026-4784.17.04163-6https://doi.org/10.1016/j.jmig.2019.09.001https://doi.org/10.1016/j.jmig.2019.09.001https://doi.org/10.1016/j.bpobgyn.2018.01.016
Adenomyosis: diagnostics and treatmentAbstractZusammenfassungFrom anamnesis to transvaginal ultrasound—The diagnosisSurgical diagnosis and histological proofSurgical treatment when family planning is completedMedical treatment optionsSurgical or combined treatment options in patients with ongoing family planningNew minimally invasive treatment optionsRecommendations for daily practiceReferences