Addressing Behaviors that Undermine Safety...
27
Addressing Behaviors that Undermine Safety Culture 1 ©2015 Vanderbilt Center for Patient and Professional Advocacy IHI National Forum December, 2015 December 6, 2015 Addressing Behaviors that Undermine Safety Culture Gerald B. Hickson, MD Sr. Vice President for Quality, Safety and Risk Prevention Assistant Vice Chancellor for Health Affairs Joseph C. Ross Chair in Medical Education & Administration Jay Banerjee, MBBS, MSc, FRCS, FCEM Emergency Physician/Associate Director Quality Improvement University Hospitals of Leicester NHS Trust Kevin Stewart, MB, MPH, FRCP, FRCPI Clinical Director, Clinical Effectiveness Unit Royal College of Physicians Session Code: L10 Presenters have nothing to disclose 27th Annual National Forum on Quality Improvement in Health Care 1. Appreciate the spectrum of behaviors that undermine a culture of safety; 2. Articulate an evidence-based approach to addressing behaviors that undermine a culture of safety; and 3. Understand how to deliver Cup of Coffee and Espresso conversations. Session Objectives
Transcript of Addressing Behaviors that Undermine Safety...

Addressing Behaviors that Undermine Safety Culture
1
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
December 6, 2015
Addressing Behaviors that Undermine Safety Culture
Gerald B. Hickson, MD
Sr. Vice President for Quality, Safety and Risk Prevention
Assistant Vice Chancellor for Health Affairs
Joseph C. Ross Chair in Medical Education & Administration
Jay Banerjee, MBBS, MSc, FRCS, FCEM
Emergency Physician/Associate Director Quality Improvement
University Hospitals of Leicester NHS Trust
Kevin Stewart, MB, MPH, FRCP, FRCPI
Clinical Director, Clinical Effectiveness Unit
Royal College of Physicians
Session Code: L10
Presenters have nothing to disclose
27th Annual National Forum on Quality
Improvement in Health Care
1. Appreciate the spectrum of behaviors that
undermine a culture of safety;
2. Articulate an evidence-based approach to
addressing behaviors that undermine a
culture of safety; and
3. Understand how to deliver Cup of Coffee
and Espresso conversations.
Session Objectives
Addressing Behaviors that Undermine Safety Culture
2
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
The content and materials related to the following
presentation are the sole property of Vanderbilt University and
the Vanderbilt Center for Patient and Professional
Advocacy. The presentation shall not be reproduced in any
form, or stored in any format or on any medium (e.g. video,
website, server, etc.) that is available to the general public or
others not attending this conference. The presentation, in any form, may not be used to produce a commercial product for
sale.
Copyright Disclosure Pursuing Reliability
Definition: “Failure free operation over time…
effective, efficient, timely, pt-centered, equitable”
Requires:
– Vision/goals/core values
– Leadership/authority (modeled)
– A safety culture = willingness to report and address
–Psychological safety
–Trust
Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National
Academies Press; 2001; Nolan et al. Improving the Reliability of Health Care. IHI Innovation Series. Boston: Institute for
Healthcare Improvement; 2004; Hickson et al. Chapter 1: Balancing systems and individual accountability in a safety culture.
In: Berman S., ed. From Front Office to Front Line. 2nd ed. Oakbrook Terrace, IL: Joint Commission Resources;2012:1-36.

Addressing Behaviors that Undermine Safety Culture
3
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
� Professionals are willing to engage in all aspects of the
job – tedious or otherwise – to the best of their ability.
� Professionals commit to:
• Technical and cognitive competence
AND
• Clear and effective communication
• Being available
• Modeling respect
• Self-awareness
� Professionalism demands self- and group regulation
Professionalism and Self-Regulation
Hickson GB, Moore IN, Pichert JW, Benegas Jr M. Balancing systems and individual accountability in a safety
culture. In: Berman S, ed. From Front Office to Front Line. 2nd ed. Oakbrook Terrace, IL: Joint Commission
Resources;2012:1-36. Reason, James. The Human Contribution: Unsafe Acts, Accidents and Heroic Recoveries.
Ashgate Publishing Limited 2008
Checklists: The Keys to the Kingdom…
Addressing Behaviors that Undermine Safety Culture
4
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
� Conclusions:
Adjusted risk of death; surgical
complications; SSIs; wound
complications, 30-day mortality…
But wait…
Urbach DR, et al. Introduction of surgical safety checklists in
Ontario, Canada. N Engl J Med. 2014 Mar 13;370(11):1029-38.
Reames BN, et al. A Checklist-Based Intervention to Improve Surgical
Outcomes in Michigan: Evaluation of the Keystone Surgery Program. JAMA
Surg. 2015 Jan 14. doi: 10.1001/jamasurg.2014.2873. [Epub ahead of print].
No Difference…No Difference…
Hickson GB, Moore IN, Pichert JW, Benegas Jr M. Balancing systems and individual accountability in a safety
culture. In: Berman S, ed. From Front Office to Front Line. 2nd ed. Oakbrook Terrace, IL: Joint Commission
Resources; 2012:1-36.SIU
Intentionally Designed Systems
Professional Accountability
The Right Balance
Addressing Behaviors that Undermine Safety Culture
5
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
� A safety culture is the overarching goal
� Disruptive behavior is counter to…
� Individuals are accountable to
promote and protect the safety culture
of the organization…
Transition from “Disruptive” to “Behaviors
that Undermine a Culture of Safety”Case: Whistling a Tune
The following event was reported to you through your
electronic event reporting system:
� “Dr. Surgeon was scheduled to perform procedure.
Once in the OR, the team attempted to perform a
‘time out’. Dr. Surgeon asked everyone to ‘listen
carefully,’ then as the process started Dr. Surgeon
began whistling a tune. ‘We believe it was the
Mickey Mouse Club theme song.’”

Addressing Behaviors that Undermine Safety Culture
6
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Represents a threat to safety?
1. Strongly Agree
2. Agree
3. Uncertain
4. Disagree
5. Strongly Disagree
1. 2. 3. 4. 5.
0% 0% 0%0%0%
10
1. 2. 3. 4. 5.
0% 0% 0%0%0%
1. 0%-20%
2. 20%-40%
3. 40%-60%
4. 60%-80%
5. 80%-100%
If this event occurred in your org, what % of the
time would it be reported?
10
Addressing Behaviors that Undermine Safety Culture
7
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
1. 2. 3. 4. 5.
0% 0% 0%0%0%
1. 0%-20%
2. 20%-40%
3. 40%-60%
4. 60%-80%
5. 80%-100%
If reported, what % of the time would a medical
leader have a conversation with Dr. Surgeon?
10
What are behaviors that undermine a culture of safety?
Why are we so hesitant to act?

Addressing Behaviors that Undermine Safety Culture
8
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
15

Addressing Behaviors that Undermine Safety Culture
9
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Interfere with ability
to achieve intended
outcomes
Definition of Behaviors That Undermine a Culture of Safety
Excerpts from Vanderbilt University and Medical Center Policy #HR-027, 2010
Create intimidating,
hostile, offensive (unsafe)
work environment
Threaten safety
(aggressive or violent
physical actions)
Violate policies (including
conflicts of interest and
compliance)
It’s About Safety

Addressing Behaviors that Undermine Safety Culture
10
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015

Addressing Behaviors that Undermine Safety Culture
11
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
To “do something” requires more than a commitment to
professionalism and personal courage.
It requires a plan(people, process and systems).
Essential Elements to Promote Reliability

Addressing Behaviors that Undermine Safety Culture
12
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Hand
Hygiene
Performance
What Are “Surveillance Tools”?
Hickson GB, Moore IN, Pichert JW, Benegas Jr M. Chapter 1: Balancing systems and individual accountability in a
safety culture. In: Berman S, ed. From Front Office to Front Line. 2nd ed. Oakbrook Terrace, IL: Joint Commission
Resources;2012:1-36.
Staff
Concerns
Risk Event
Reporting
System
Patient
Relations
Department
Surgical
Bundle
Compliance
Staff Professionalism ConcernsCalled Dr. __ re: change in pt status…came 25 min later,
looked at pt, publicly yelled at me, “you lied… pt okay…don’t
call again.”…felt threatened.
Called Dr. __ re: change in pt status…came 25 min later,
looked at pt, publicly yelled at me, “you lied… pt okay…don’t
call again.”…felt threatened.
Refused to do a time out before surgery, …. said, “we’re all
on the same page here.”
Refused to do a time out before surgery, …. said, “we’re all
on the same page here.”
Dr. __ refused to re-gown and re-glove during colorectal
surgery. Said, “I don’t agree with that part of the bundle.”
Dr. __ refused to re-gown and re-glove during colorectal
surgery. Said, “I don’t agree with that part of the bundle.”
Confidential and privileged information under the provisions set forth in T.C.A. §§ 63-1-150 and 68-11-272; not be disclosed to unauthorized persons.
Addressing Behaviors that Undermine Safety Culture
13
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Reports of Unprofessional Behavior
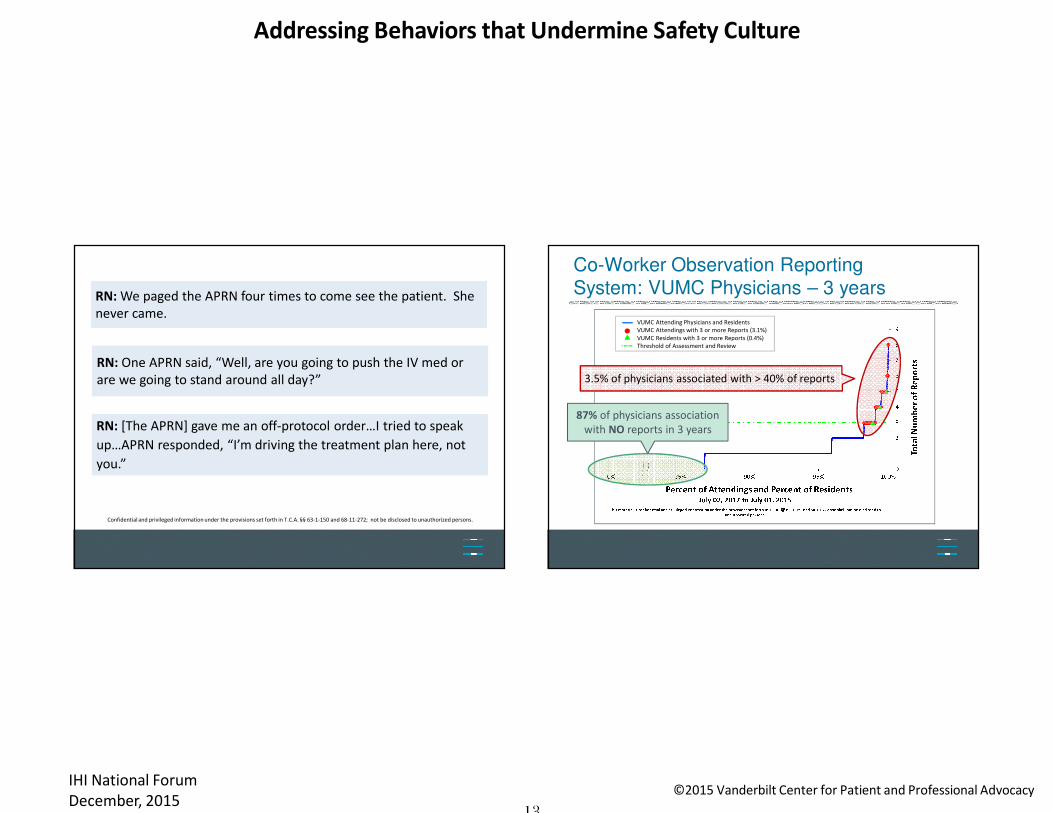
RN: One APRN said, “Well, are you going to push the IV med or
are we going to stand around all day?”
RN: One APRN said, “Well, are you going to push the IV med or
are we going to stand around all day?”
RN: [The APRN] gave me an off-protocol order…I tried to speak
up…APRN responded, “I’m driving the treatment plan here, not
you.”
RN: [The APRN] gave me an off-protocol order…I tried to speak
up…APRN responded, “I’m driving the treatment plan here, not
you.”
RN: We paged the APRN four times to come see the patient. She
never came.
RN: We paged the APRN four times to come see the patient. She
never came.
Confidential and privileged information under the provisions set forth in T.C.A. §§ 63-1-150 and 68-11-272; not be disclosed to unauthorized persons.
Co-Worker Observation Reporting
System: VUMC Physicians – 3 years
VUMC Attending Physicians and Residents
VUMC Attendings with 3 or more Reports (3.1%)
VUMC Residents with 3 or more Reports (0.4%)
Threshold of Assessment and Review
87% of physicians association
with NO reports in 3 years
3.5% of physicians associated with > 40% of reports

Addressing Behaviors that Undermine Safety Culture
14
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
97% of physicians are associated
with NO reports in 3 years
Co-Worker Observation Reports - National CORS℠ Database (n = 5,721)
Co-Worker Observation Reporting
System: National Comparison
1% of physicians associated with 61% of reports
Promoting Professionalism Pyramid
No ∆Level 3 "Disciplinary" Interv
Pattern persists Level 2 “Guided" Authority Interv
Apparent pattern Level 1 "Awareness" Interv
Single “unprofessional"
incidents (merit?)
Vast majority of professionals - no issues -
provide feedback on progress*includes CMS-defined “condition level” and “immediate jeopardy” safety-related complaints
"Informal" Cup of
Coffee Intervention
Mandated
Ray, Schaffner, Federspiel, 1985.
Hickson, Pichert, Webb, Gabbe, 2007.
Pichert et al, 2008.
Mukherjee et al, 2010.
Stimson et al, 2010.
Pichert et al, 2011.
Hickson & Pichert, 2012.
Hickson et al, 2012.
Pichert et al, 2013.
Talbot et al, 2013.
Mandated
Reviews
Addressing Behaviors that Undermine Safety Culture
15
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Back to the case: Whistling a tune
So what kind of conversation?
Dr. Surgeon asked everyone to ‘listen
carefully,’ then as the process started Dr.
Surgeon began whistling a tune. ‘We
believe it was the Mickey Mouse Club
theme song.’”
Informal ConversationRegular (Cup of Coffee)
(see handout)
For a single “event”…

Addressing Behaviors that Undermine Safety Culture
16
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
1. Model respect and seek to maintain trust
2. When possible share in a private area
3. Avoid tendency to downplay ‘event’
4. Balance empathy and objectivity
5. Anticipate range of responses (push-backs)
Principles for “Informal” Conversations
See Handout:
6. Your role (even as “the chief”): • To report a single “disturbance”
• To let the colleague know that the behavior/action was noticed
(surveillance)
7. It’s not a control contest
8. Don’t expect thanks
9. Know message and “stay on message”
10. Know your communication style (and your buttons)
Principles for “Informal” Conversations
See Handout:
Addressing Behaviors that Undermine Safety Culture
17
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
� Offer appreciation (if you can): “You’re important, if
you weren't, I wouldn't be here.”
� Use “I” statements: “I heard…,” “I saw…,” “I received…”
� Avoid “you” statements…
� Review incident, provide appropriate specifics
� Ask for colleague’s view…pause…
� Respond to questions, concerns…
Having the “Informal” Conversation
See Handout:
� Appreciation, affirmation
� Empathy: “Now I feel I understand..."
� Accountability: "But we've all got to respond
professionally..."
� Reminder of behavior standards: “incident did not appear
consistent with..."
� If asked what to do use phrases: "reflect on the issues,
think about ways to prevent recurrence."
� If appropriate: conversation confidential, known only to…
Having the “Informal” Conversation
Closing:
Addressing Behaviors that Undermine Safety Culture
18
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
� A control contest
� Therapy (for the individual or yourself)
� A hierarchical conversation
� An enabling conversation
� An opportunity to address multiple issues
Having the “Informal” Conversation
Conversation is NOT:
Now it’s your turn…
Addressing Behaviors that Undermine Safety Culture
19
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Essential Elements to Promote Reliability
But wait, does any of this really work?
Addressing Behaviors that Undermine Safety Culture
20
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
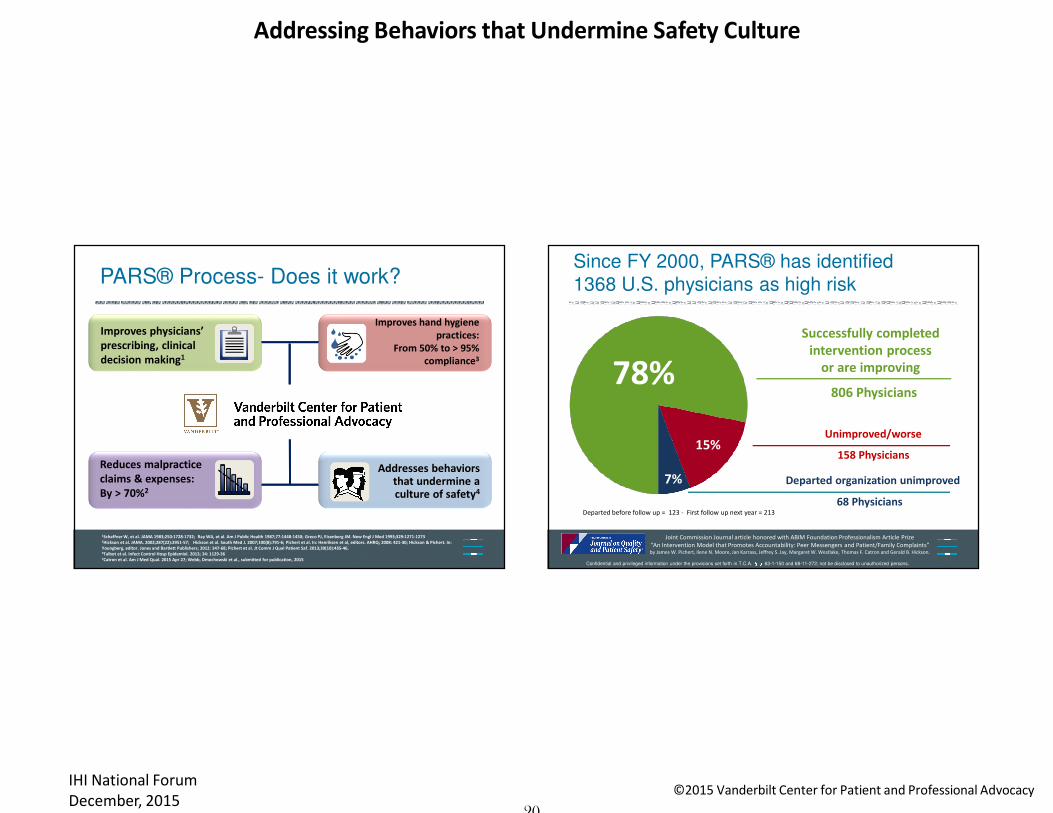
1Schaffner W, et al. JAMA 1983;250:1728-1732; Ray WA, et al. Am J Public Health 1987;77:1448-1450; Greco PJ, Eisenberg JM. New Engl J Med 1993;329:1271-12732Hickson et al. JAMA. 2002;287(22):2951-57; Hickson et al. South Med J. 2007;100(8):791-6; Pichert et al. In: Henriksen et al, editors. AHRQ; 2008: 421-30; Hickson & Pichert. In:
Youngberg, editor. Jones and Bartlett Publishers; 2012: 347-68; Pichert et al. Jt Comm J Qual Patient Saf. 2013;39(10):435-46. 3Talbot et al. Infect Control Hosp Epidemiol. 2013; 34: 1129-364Catron et al. Am J Med Qual. 2015 Apr 27; Webb, Dmochowski et al., submitted for publication, 2015
Reduces malpractice
claims & expenses:
By > 70%2
Improves hand hygiene
practices:
From 50% to > 95%
compliance3
Addresses behaviors that undermine a culture of safety4
Improves physicians’
prescribing, clinical
decision making1
PARS® Process- Does it work?
Unimproved/worse
Successfully completed
intervention process
or are improving
Departed organization unimproved
Since FY 2000, PARS® has identified
1368 U.S. physicians as high risk
68 Physicians
158 Physicians
806 Physicians
Confidential and privileged information under the provisions set forth in T.C.A. §§ 63-1-150 and 68-11-272; not be disclosed to unauthorized persons.
78%
7%
15%
“An Intervention Model that Promotes Accountability: Peer Messengers and Patient/Family Complaints”by James W. Pichert, Ilene N. Moore, Jan Karrass, Jeffrey S. Jay, Margaret W. Westlake, Thomas F. Catron and Gerald B. Hickson.
Joint Commission Journal article honored with ABIM Foundation Professionalism Article Prize
Departed before follow up = 123 - First follow up next year = 213
Addressing Behaviors that Undermine Safety Culture
21
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
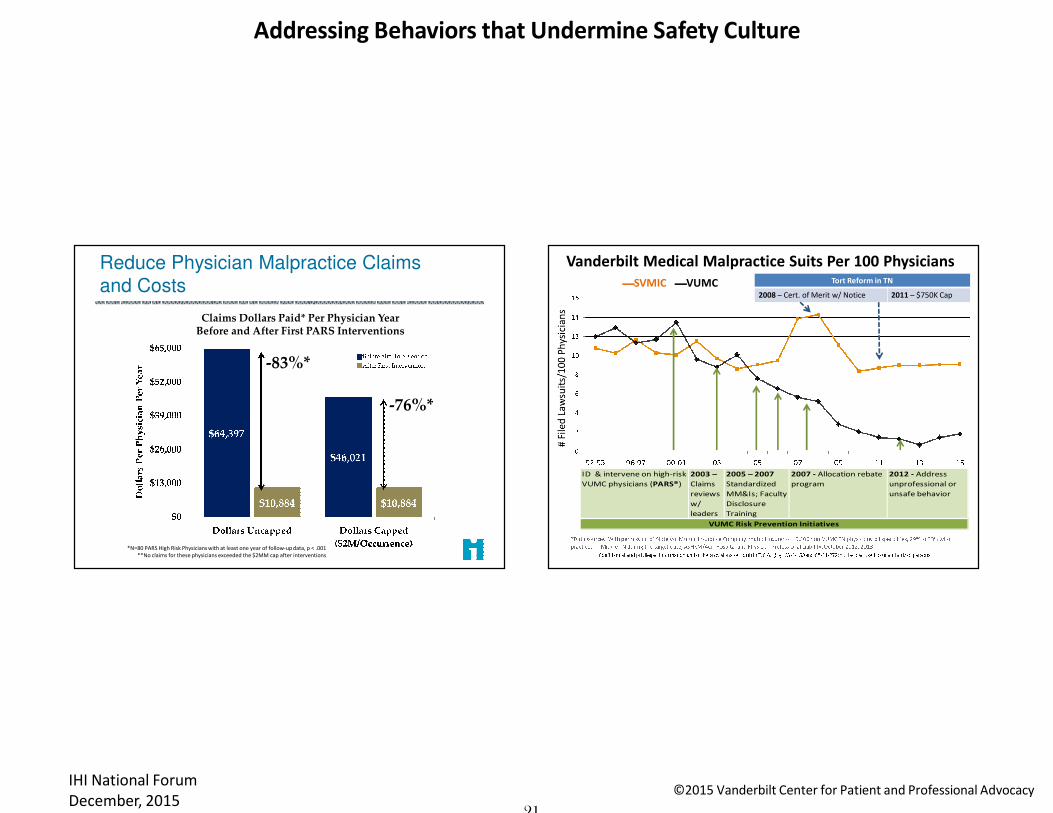
-76%*
-83%*
*N=80 PARS High Risk Physicians with at least one year of follow-up data, p < .001
**No claims for these physicians exceeded the $2MM cap after interventions
Reduce Physician Malpractice Claims
and Costs
Claims Dollars Paid* Per Physician Year Before and After First PARS Interventions
Vanderbilt Medical Malpractice Suits Per 100 Physicians
ID & intervene on high-risk
VUMC physicians (PARS®)
2003 –
Claims
reviews
w/
leaders
2005 – 2007
Standardized
MM&Is; Faculty
Disclosure
Training
2007 - Allocation rebate
program
2012 - Address
unprofessional or
unsafe behavior
VUMC Risk Prevention Initiatives
SVMIC VUMC Tort Reform in TN
2008 – Cert. of Merit w/ Notice 2011 – $750K Cap

Addressing Behaviors that Undermine Safety Culture
22
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Confidential and privileged information under the provisions set forth in T.C.A. §63-1-150 and §68-11-272; not to be disclosed to unauthorized persons.Threshold Target Reach VUMC YTD
Hospital Unit Hand Hygiene Compliance
July 1, 2010 – November 30, 2011VUMC Quarterly HH Compliance
June 2009 – June 2015
Reach
Threshold
Period of intensified HH program utilizing shared
accountability
Talbot TR, et al. Sustained improvement in hand hygiene adherence: Utilizing shared accountability
and financial incentives. Infect Control Hosp Epidemiol. 2013; 34(11, Nov): 1129-1136

Addressing Behaviors that Undermine Safety Culture
23
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Hand Hygiene Improvement Strongly
Correlates with Low Infection Rates
Talbot TR, et al. Sustained improvement in hand hygiene adherence: Utilizing shared accountability
and financial incentives. Infect Control Hosp Epidemiol. 2013; 34(11, Nov): 1129-1136
Case: House call
The following event was reported to you through
your electronic event reporting system:
� Nurse reports: Attempted to page Dr. ___ about one of his
patients, 56 y/o with progressive renal failure and BP
elevation…BPs continued to rise so I paged again and called
his office…Office said they would give him a message…After
30 more min we called the RRT...shortly after the team
arrived Dr.___ shows up...clearly...declares "I will fix this
problem"...Returns with a poster with his name and pager
number...pulls out a roll of tape and...

Addressing Behaviors that Undermine Safety Culture
24
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
Promoting Professionalism Pyramid
No ∆Level 3 "Disciplinary" Interv
Pattern persists Level 2 “Guided" Authority Interv
Apparent pattern Level 1 "Awareness" Interv
Single “unprofessional"
incidents (merit?)
Vast majority of professionals - no issues -
provide feedback on progress*includes CMS-defined “condition level” and “immediate jeopardy” safety-related complaints
"Informal" Cup of
Coffee Intervention
Mandated
Ray, Schaffner, Federspiel, 1985.
Hickson, Pichert, Webb, Gabbe, 2007.
Pichert et al, 2008.
Mukherjee et al, 2010.
Stimson et al, 2010.
Pichert et al, 2011.
Hickson & Pichert, 2012.
Hickson et al, 2012.
Pichert et al, 2013.
Talbot et al, 2013.
Mandated
Reviews
Informal Conversation
Espresso(see handouts for each)
For a single “event”…
Addressing Behaviors that Undermine Safety Culture
25
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
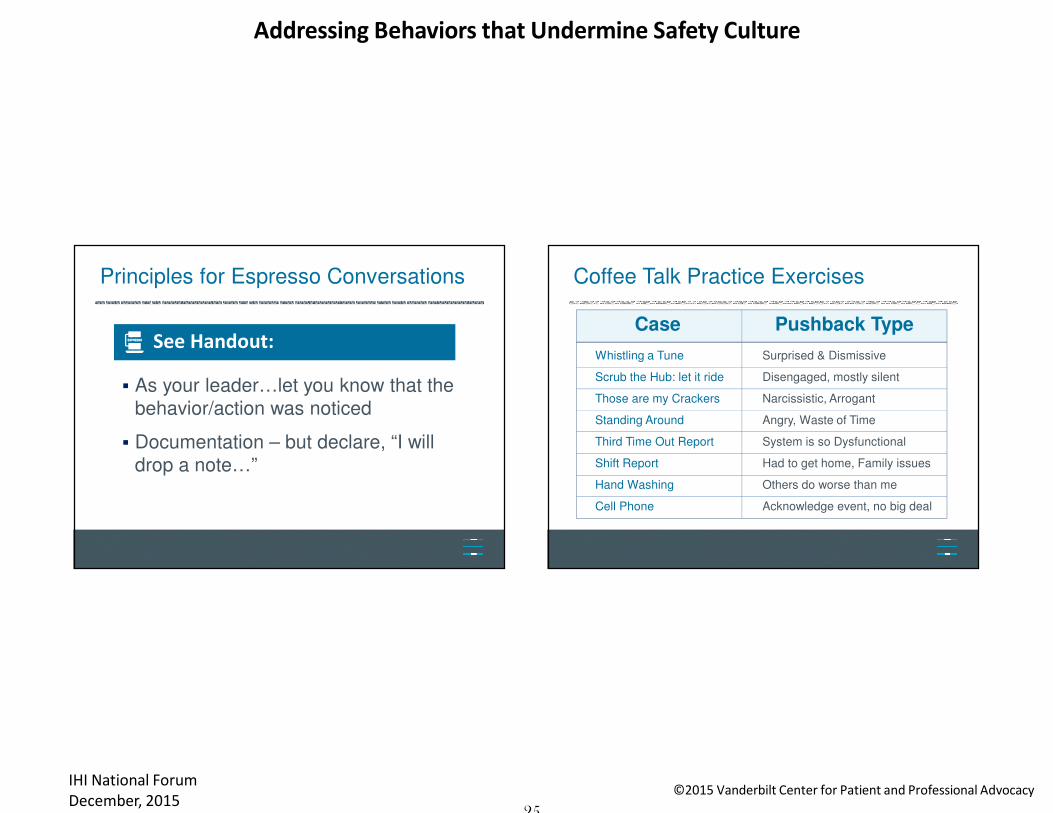
� As your leader…let you know that the
behavior/action was noticed
� Documentation – but declare, “I will
drop a note…”
Principles for Espresso Conversations
See Handout:ESPRESSOESPRESSOESPRESSOESPRESSO
Coffee Talk Practice Exercises
Case Pushback Type
Whistling a Tune
Scrub the Hub: let it ride
Those are my Crackers
Standing Around
Third Time Out Report
Shift Report
Hand Washing
Cell Phone
Surprised & Dismissive
Disengaged, mostly silent
Narcissistic, Arrogant
Angry, Waste of Time
System is so Dysfunctional
Had to get home, Family issues
Others do worse than me
Acknowledge event, no big deal

Addressing Behaviors that Undermine Safety Culture
26
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
What can I do?• Model professionalism
• Self-reflect on your own behavior
• Speak up or report when you see/experience
lapses in professionalism
• Commit to engage others in building a culture
of accountability
• Discuss what you’ve learned with your leader
I’m only one person…
What should I do?• Everything on the previous slide, plus
• Review your Gap Analysis
• Write down three things that will move you
closer to your goal
� Complete
� Repeat
I’m a Leader…
Addressing Behaviors that Undermine Safety Culture
27
©2015 Vanderbilt Center for Patient and Professional AdvocacyIHI National Forum
December, 2015
1. Cup of Coffee Handout
2. Espresso Handout
3. Gap Analysis
Takeaways from this Session
Now or Later
www.mc.vanderbilt.edu/cppa
Let Us Hear Your Comments and Questions