Addictive behaviours and the family: Impacts, models and ...ictab+2015...Addictive behaviours and...
76
Addictive behaviours and the family: Impacts, models and interventions Professor Alex Copello, PhD School of Psychology, The University of Birmingham, UK ICTAB 2015 – Odense, Denmark
Transcript of Addictive behaviours and the family: Impacts, models and ...ictab+2015...Addictive behaviours and...

Addictive behaviours and the
family: Impacts, models and
interventions
Professor Alex Copello, PhD
School of Psychology,
The University of Birmingham, UK
ICTAB 2015 – Odense, Denmark

Acknowledgements

http://www.afinetwork.info/ AFINet Aims
Provide information
FM-centred research
Raise awareness of FMs & FM models
Influence policy
Evidence-based practice
Our Aims:

Plan
• Addiction in context • Families – extent and impacts • Evidence based family interventions • SSCS model - Helping family members in their
own right • Friends – Social support and outcomes -
interventions • Implementation • Working with families and social networks in
other generic settings

Addiction in Context

The particle vs the social paradigm…..Peter Adams (2008) Fragmented Intimacy: addiction in a social world, New York, Springer.
People as particles or people as relationships….

Individual vs. social view of addictions

Social Context
Family and Friends
Some Similarities....
Some differences....

SOCIAL NETWORKS

UKATT Research Team (Principal Investigators)
• Alex Copello West Midlands
• Christine Godfrey York
• Nick Heather Newcastle
• Ray Hodgson South Wales
• Jim Orford Birmingham
• Duncan Raistrick Leeds
• Ian Russell York/Bangor
• Gillian Tober Leeds

Participants entering the UKATT trial were asked about the people they had
spent most time with over the previous three months (aged at least 12 years
old). They named these ‘important’ people and described each of them using
demographic and drinking-related characteristics.
Overall 4677 important people were named. All 740 participants could name
at least 1 important person; the highest number named was 12. Participants
could most frequently name 10 people, and the mean number named was 6.5
(standard deviation 3.6).
This graph shows numbers of important people named by participants:
0
20
40
60
80
100
120
1 2 3 4 5 6 7 8 9 10 11 12
Important people
Pa
rtic
ipa
nts
Participants then decided which of these people were the four most important
and listed them in order.

The four most important people: how were they
related to the drinkers?
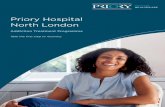
This graph shows how the participants were related to their four most
important people. Frequencies of relationship type are shown for the 1st, 2nd,
3rd and 4th most important people to the drinker.
The majority of people entering alcohol treatment named their partner as the
most important person, although family members were also a popular choice.
Very few drinkers named their partner as least important person of the four.
Members of close family were predominantly named as second or third most
important, and friends were commonly named as third or fourth.
0
100
200
300
400
500
1 2 3 4
important person no.
fre
qu
en
cy
s ignificant other
family
friend
other

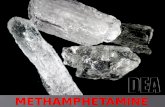
Who were the most important family members?
Relationships of important people to focal drinkers could be further broken
down into relationships of family members. This graph shows percentages
of type of family member (from overall relationship) who were named as
each important person:
0
5
10
15
20
25
1st 2nd 3rd 4th
children
parent
sibling
other/family
Parents were most frequently named as first and second most important,
children as second or third most important, and siblings as third most
important. Other family members were more likely to be named as the fourth
than as the most important person.


SAMPLE
• 118 participants
• 93 (79%) men
• Mean age = 35.5 (20-60)
• Ethnicity:
– 73% white-British
– 14% south Asian
– 4% black
– 8% mixed
• Drug use in past 28 days:
• Heroin 56% (md 7 days)
• Cocaine 34% (md 6 days)
• BZ 8%
• Cannabis 39%
• Alcohol 48%
• 15% had injected

Day, Copello, Chohan et al., 2012. European Addiction Research Opiate Substitution Treatment in the UK 118 participants identified a total of 820 network members Mean network size was 6.9. Of this group, 47 (6%) were sexual partners 378 (46%) immediate family members 97 (12%) extended family members 189 (23%) friends 16 (2%) colleagues from work 51 (6%) treatment professionals or members
of self-help groups 42 (5%) others So, two thirds of the social network was made up of family members

'We are always in some form of contact': friendships among homeless drug and alcohol users living in hostels - J Neale, C
Brown - Health & social care in the community, 2015
Homeless drug and alcohol users have small friendship networks that are often undermined by arguments,
geographical mobility and imprisonment.
Homeless drug and alcohol users desire culturally normative friendships, underpinned by routine and regular contact.
Information and communication technologies are central to the friendships of many homeless drug and alcohol users, keeping
them connected to sources of social support and recovery capital outside homelessness and substance-using worlds.

• Most people entering treatment for alcohol and or drug problems in the UK are not isolated or lack potential sources of social support
• Also suggests that a number of people can potentially be affected by the impacts of the problem and resulting harms to others
• Despite some apparent differences between the two treatment groups, such as the higher number of partners proportionately reported by the alcohol treatment sample, the largest composition of the networks appears to comprise family members

Beyond treatment samples, wider estimates of the extent of affected
family members

How large is the (impact on family) problem?
It is estimated that there are approximately 15 million people with drug use disorders globally and 76 million with alcohol use disorders (Obot, 2005).
A cautious estimate of just one person seriously affected in each case suggests a minimum of 91 million affected family members
Most people would use a greater multiplier and produce a higher figure

What is the extent of the problem?
Drug treatment
population
General
population
50,373 partners
55,012 parents
35,208 ‘other’
573,671 partners
610,970 parents
259,133 ‘other’
Total = 140,593 Total =1,443,774
• Key findings from UK DPC study about adult family members of drug misusers.
• What about alcohol misuse?
• Up to 1 million children are affected by parental drug misuse & up to 3.5 million by parental alcohol misuse (Manning et al., 2009).
• It is estimated that the impact of drug misuse on the family costs the UK £1.8 billion but also brings a resource saving to the NHS of £747 million through the care provided.

In 2008 the ‘Harm to Others’ survey was conducted with 2600 people in Australia (Laslett et al. 2011) and 3068 in New Zealand (Casswell, You and Huckle 2011).
Just over a quarter (28%) of Australian adults reported being negatively affected by the drinking of someone they knew. Younger respondents were more likely to report that they had been affected, and compared to males; females were almost twice as likely. Seven percent of respondents reported living with a problematic drinker in the past year; often their partner or a family member. In New Zealand however this figure was considerably higher, with 1 in 4 reporting that the heavy drinker was part of their household (Casswell, You and Huckle 2011).

Percentages (and CIs) of respondents negatively affected in last 12 months by drinkers in various relationships
Laslett, Room, Ferris, Wilkinson, Livingston, & Mugavin (2011). Addiction, 106, 1603-1611.

We know it is a highly prevalent problem….

Stresses and Strains

THE UNIQUE SET OF STRESSFUL CIRCUMSTANCES FOR FAMILIES COPING WITH ADDICTION
Has the nature of severe stress, threat and abuse
Involves multiple sources of threat to self and family, including emotional, social, financial, health and safety
Can have significant impact on children
Worry for that family member is a prominent feature
There are influences in the form of individual people and societal attitudes that encourage the troubling behaviour
Attempting to cope creates difficult dilemmas, and there is no guidance on the subject
Social support for the family is needed but tends to fail
Professionals who might help are often at best badly informed and at worst critical

Symptoms of Ill Health
2
1
0
5
10
15
20
25
30
35
UK
Mex
ico
Wiv
es
P.C
are
P.C
are
Psy
ch
Co
ntr
ol
Family members; psychiatric out-pts. and
community controls
Family
members

Ray et al (2007) Compared family members of people with substance misuse problems with family members of similar persons without substance misuse. Samples: Family members n = 45,677 (male/female – 46/54%) Comparison group n = 141,722 (male/female – 46/54%) More likely to be diagnosed with medical conditions most commonly depression and other psychological problems Ray et al (2007) The excess medical cost… Medical Care

Population estimates of contact with law enforcement services and health-related services due to others’ drinking,
2008 (weighted data)
Mugavin, Livingston, & Laslett (2014). Drug and Alcohol Review, 33, 161-168.

Reduced medical costs in family members of individuals who are abstinent after addiction treatment
Weisner, Parthasarathy, Moor, & Mertens (2010). Addiction, 105, 1226-1234.

Embarrassment when illness strikes a close relative: A multi-site study
Ahmedani et al., 2013 Psychological Medicine Investigated social stigma: family members’ embarrassment by relative’s mental health or alcohol or drug problem. 16 sites across various countries with a combined n= 81144 Looked at burden and the experience of embarrassment

Embarrassment when illness strikes a close relative: A multi-site study
Family members experienced embarrassment:
24.9% of FMs experiencing General Medical Conditions 49.5 % of FMs of Alcohol and Drug Conditions 36.6 % of FMs of both conditions above combined Also found that embarrassment was not a function of burden Implications for early intervention and treatment entry delay

Interventions involving families
and wider networks

A narrow individual focus on treatment and help fails to consider some facts:
• That living with a significant alcohol or drug problem is a highly stressful experience
• That the stress experienced leads to physical and psychological
symptoms for family members
• That family members use generic and primary care services to seek help
• That family members provide significant care
• That family members can improve outcomes for the substance user

Addiction and the family: is it time for services to take notice of the evidence? (Copello and Orford, Addiction, 2002)
POTENTIAL BARRIERS
•Theoretical
•Practical •Treatment focus needs to be broadened
•Commissioners and service providers recognition of broader sets of outcomes

Group treatment
Al-Anon / Families Anonymous
Supportive stress management counselling
Parent coping skills training
5-Step Method
Working With FMs to engage relative in treatment
Joint involvement of FM and their relatives in treatment
Responding to Needs of FM in their own rights
Community reinforcement & family training
Unilateral Family therapy
Cooperative counselling
Pressure to change
Johnson Intervention
Conjoint family group therapy
Alcohol behavioural couples therapy
Family therapy
Network therapy
Social behaviour & network therapy (SBNT)
An Overview of ways of involving family members (FMs)

Despite the available evidence and potential gain, shifting the emphasis from individualised treatment approaches to those focused on the substance user’s family and social environment presents a number of significant challenges
(Copello, 2006)

Family members in their own right
SSCS model & 5 Step Method

‘Despite the recognition of carers’ needs and the growth of carer organisations, however, there is a rather limited evidence base assessing the impact on carers and families of people who misuse drugs and on interventions intended to support them, and even less attention given to the needs of families and carers in their own right.’ National Institute of Clinical Excellence (NICE) 2008.

Relative’s addiction problem
Stress on family member
Family member strain
Social support for family member
Ways the family member copes
The stress-strain-coping-support model
40
Understanding

Families in three contrasting cultures

Putting up
Withdraw-
ing
Variations by length
of time coping;
relationship to the
relative; culture
Family
strain
or
resilience
Ways family
member copes
Variations by
problem severity;
family disharmony;
living arrangements;
material resources.
Informal
(kin/non-kin)
Professional
(as available)
Own
demoralisation
and ill-health
Child and
family
disturbance and
ill-health
Stress on family
member
Relative's
addiction
problem
Social support for
family member
Information
and under-
standing
Affected
by the
relative
Worried
for the
relative
Standing up

Derives from the Stress Strain Coping Support (SSCS) model and what family members have told us in a number of research studies.
The 5-Steps are:
1. Let the family member tell their story.
2. Provide information.
3. Discuss ways of responding.
4. Explore sources of support.
5. Arrange further help if needed.
The 5-Step Method

on
e Listen, reassure and explore concerns
two
Provide relevant, specific and targeted information
th
ree
Explore coping responses
fou
r Explore and enhance social support
five
Discuss and explore further needs
The 5 steps
44


• Several research studies in the UK and Italy,
including one randomised controlled trial.
• Research in primary care, and also statutory and
non-statutory drug and alcohol services.
• Mixed method research, involving both
questionnaires and interview data.
• Data from over 250 family members.
• Pilot studies with groups, and of online support.
How does the 5-Step Method help
FMs?


Some Findings
FMs mainly female and mothers or partners. Users tend to be male and alcohol or drug (heroin) misusers.
FMs have been living with the situation for an average of 8-10 years, feel generally isolated with low levels of support and previous negative experiences of help-seeking.

Some findings
• For family members:
• A positive and significant change in coping behaviour.
• Reduction in symptoms (physical and psychological).
• Lessening of the impact of the problem.
• For practitioners:
• Confidence in working with family members.
• Awareness of the importance of working with family members.

Examples of how the 5-Step Method can
influence coping responses
Increased focus on own life and needs (gaining
independence).
Increased assertiveness over the misuse
(resisting and being assertive).
Taking a calmer approach towards the misusing
relative (reduced emotional confronting).
Increased awareness of the relative’s misuse
problem and its effects on family members
(cognitive change).



Wider social networks including friends supporting
substance users


Social Networks and Addiction Problems
• Structure of networks
• Problem recognition and help-seeking
• Treatment outcome
• After treatment

Social Support and Outcomes
•General social support
•Alcohol-specific social support
•Drinking behaviour of the social network members
All unique predictors of alcohol treatment outcomes

The addition of just one alcohol abstinent person to the social network
may increase the likelihood of abstinence by 27% (Litt et al., 2007).

010
2030
4050
6070
8090
opposes
treatment
mixed neutral supports but
prefers
alternative
supports
treament in
this program
doesn't
know
1st
2nd
3rd
4th
How did they feel about the focal drinker getting alcohol
treatment?
Important people rarely opposed treatment. The most important person was
particularly supportive (78.89% supported treatment), and even fourth most
important people were predominantly supportive (53.18%). Just over 10% of all
important people felt neutral towards treatment. The third and fourth most
important people were more likely than the first/second not to know about
treatment.
This graph shows the percentages of important people (1st, 2nd, 3rd and 4th who fell
into each category:

The 4 most important people who have daily contact with the focal drinker
0
50
100
150
200
250
300
350
400
450
500
1st IP 2nd IP 3rd IP 4th IP
Diagramtitel
heavy drinkers
Non-heavy drinkers

Overall....
• Participants recruited to UKATT had people in their social networks
• Based on participants’ reports, most had people in their networks that did not have alcohol problems
• Most had people in their networks that were supportive of the focal client’s treatment

Social Behaviour and Network Therapy (SBNT)
• Built upon the premise that social network support for change is central to the resolution of addictive behaviour
• Integrates effective strategies from other treatment approaches
• Initially targeted at alcohol problems – UK Alcohol Treatment Trial
(UKATT)

SBNT: Key Principles
• Always ‘think network’.
• Draw a network diagram.
• Invite members of the network.
• Strengthen the network.
• Discuss themes of: communication, coping, information, joint activities.
• Work with any part of the network.
• Plan for the future.

SBNT content
Core topics
• Communication.
• Coping.
• Enhancing social support
networks.
• Developing a network-
based relapse
management plan.
Elective topics
• Basic education on
drugs/alcohol.
• Increasing pleasant
activities.
• Employment.
• Minimising support for
drug/alcohol use.

SBNT adapted for use with primary opiate users •20 therapists from Birmingham CDTs trained to deliver SBNT, supported by a treatment manual and a two-day workshop followed by video supervision •12 therapists delivered SBNT to 24 patients, and 3-month outcomes showed reductions in drug use and improved family and social relationships

How about service provision and delivery of evidence based family
and network interventions?

UKDPC research on adult family /carers
Phase 2: 2011-12
Aims
• To describe the extent and nature of support provision for adult family members / carers of people experiencing drug problems to highlight gaps and good practice to help improve provision.
Components:
• Review of policy & guidance in the UK
• Web survey of service providers in the UK
• In-depth study: 20 DAT areas in England & 8 ADPs in Scotland
Research team: Alex Copello, Lorna Templeton, Gagandeep Chohan & Trevor McCarthy

Current Service Provision in the
UK
• Patchy provision of family-focused drug and alcohol intervention services across the UK
• Often based on poor or insecure funding.
• A focus on treatment for the substance misuser mostly.
• Copello et al (2006) “the responsibility for increasing implementation for family-based services lies not only with service providers but also with policy makers and commissioners.”

Developing Family Focused Practice

Overall proportion of family-focused practice – increases after targeted
program of work within an organisation (from Claire Hampson’s PhD work)
19
26
34
Baseline (117/611) Training & Supervision period(108/410)
Post-intervention (257/765)
% family-focused practice
*
*^
*Significantly greater than baseline. ^Significantly greater than training period.

A need to improve outcomes for all “I had a session where a Mother and Daughter let some stuff out [in the session]. At the end of it they got up and hugged each other, apparently for the first time in 5 years”
Working creatively and flexibly ‘The confidentiality form is a useful tool rather than a formality…I ask them [focal client] if your brother called me, could I talk to him? I’m proactive in searching around”
Efficacious impact of the project “Nothing comes of a one-off model workshop. It needs a follow-up intervention.’ ‘The meetings are a useful as a constant reminder. It’s good having the contact”
Recognising changes needed in practice and policy ‘Admin will be amending the wording of the invitation letter to show clients that their FMs are welcome in the sessions’
Policy and procedures impeding family-focused practice “It doesn’t just fit into the cycle we’re funded for”
Limited family-focused practice within outside organisations “GPs only refer drinkers, they don’t think about the affected family members”
Perceiving and experiencing challenges and difficulties
“We’ve had it rammed down our throats careful of the confidentiality, careful not to give anything away”
Individualistic practices remain “A one-to-one can be quite precious and that’s my preference to working”
Qualitative analysis: Main themes IN
TERN
AL
EXTER
NA
L

Responding to families in other settings


Increasing access to Psychological Therapies (IAPT) services sit within primary care and aim to ensure that psychological interventions are offered as frontline to those with mild to severe presentations of depression and anxiety, alongside
treatment as usual by their General Practitioner.
The sample of 100 clients was made up of 40 men and 60 women. The mean age of the sample was 38.5 years
The first question asked of participants was: ‘At the time of entering the IAPT service did you/do you have a family member whose level of alcohol and/or drug use concerns you?’ (Yes, No).
Twenty-two responded with a Yes

• Thirteen participants reported having a family member whose alcohol use was of concern (59 %), five drugs (23%) and four both (18%).
• There was a significant difference between the mean depression scores of the 22 positive cases (19.2, s.d. 4.0) compared that for the remaining 78 clients (15.8, s.d. 6.1) (p < 0.05), but no significant differences in anxiety scores.
• This pilot study provides some indication that a large minority of IAPT clients may be seeking help partly because of substance misuse problems in the family suggesting the study deserves replication and extension.

Some tentative concluding thoughts
• Addiction is sufficiently stressful to cause pain and suffering to a very large but unaccounted number of adults and contributes to the global burden of adult ill-health
• The impact and cost of the care given by family members is significant.
• Alcohol and drug policies are increasingly recognising the needs of family members or how they can be involved in treatment.
• Specialist service delivery remains predominantly oriented towards the focal alcohol or drug client, although there is evidence of a wide range of interventions to support families, and some evidence that more services are becoming available.
• An effective response to the needs of family members has the potential to significantly reduce harm and health problems in this group and could be delivered in generic services
• Involving family members in supporting the treatment of the user can improve outcomes
• We need to develop flexible approaches, deal with implementation barriers and aim to understand better the mechanisms of change for both groups

Thank you for listening…