Addiction Medicine - Inspire Malibu · Addiction Medicine: Closing the Gap between Science and...
586
Addiction Medicine: Closing the Gap between Science and Practice June 2012 Funded by: The Annenberg Foundation The Diana, Princess of Wales Memorial Fund and The Franklin Mint The New York Community Trust Adrian and Jessie Archbold Charitable Trust
Transcript of Addiction Medicine - Inspire Malibu · Addiction Medicine: Closing the Gap between Science and...
-
Addiction Medicine:
Closing the Gap between Science and Practice
June 2012
Funded by: The Annenberg Foundation The Diana, Princess of Wales Memorial Fund and The Franklin Mint The New York Community Trust Adrian and Jessie Archbold Charitable Trust
-
Board of Directors
Copyright ©2012. All rights reserved. May not be used or reproduced without the express written permission of The National Center on Addiction and Substance Abuse at Columbia University.
Lee C. Bollinger
President, Columbia University Ursula M. Burns
Chairman and CEO, Xerox Corporation Columba Bush
Former First Lady of Florida Joseph A. Califano, Jr.
Founder and Chairman Emeritus, CASA Columbia Kenneth I. Chenault Chairman and CEO, American Express Company Peter R. Dolan
Chairman, ChildObesity180 William H. Foster, Ph.D.
President and CEO, CASA Columbia Victor F. Ganzi
Chairman of the Board PGA Tour Melinda B. Hildebrand Ralph Izzo, Ph.D.
Chairman of the Board, CEO and President, Public Service Enterprise Group, Inc. (PSEG) Gene F. Jankowski
President, CBS Broadcasting, Retired David A. Kessler, M.D. Jeffrey B. Kindler Jeffrey B. Lane
Chairman, CASA Columbia Alan I. Leshner, Ph.D.
CEO, Executive Publisher, Science, American Association for the Advancement of Science
Rev. Edward A. Malloy, CSC
President Emeritus, University of Notre Dame
Doug Morris
CEO, Sony Music Entertainment
Bruce E. Mosler
Chairman, Global Brokerage, Cushman & Wakefield, Inc. Manuel T. Pacheco, Ph.D.
President Emeritus, University of Arizona and University of Missouri System Joseph J. Plumeri
Chairman and CEO, Willis Group Holdings PLC Jim Ramstad
Former Member of Congress (MN-3) Shari E. Redstone
President, National Amusements, Inc. E. John Rosenwald, Jr. Vice Chairman Emeritus, J.P.Morgan Michael I. Roth
Chairman and CEO, The Interpublic Group of Companies, Inc. Mara Burros Sandler Michael P. Schulhof
Chairman, GTI Holdings LLC Louis W. Sullivan, M.D.
President Emeritus, Morehouse School of Medicine John J. Sweeney Clyde C. Tuggle
Senior Vice President, Chief Public Affairs and Communications Officer, The Coca-Cola Company
Directors Emeritus James E. Burke (1992-1997) Jamie Lee Curtis (2001-2009) Jamie Dimon (1995-2009) Mary Fisher (1996-2005) Betty Ford (1992-1998) Douglas A. Fraser (1992-2003) Barbara C. Jordan (1992-1996) Leo-Arthur Kelmenson (1998-2006)
Donald R. Keough (1992-2010) LaSalle D. Leffall, Jr., M.D., F.A.C.S. (1992-2001) Nancy Reagan (1995-2000) Linda Johnson Rice (1992-1996) George Rupp, Ph.D. (1993-2002) Michael I. Sovern (1992-1993) Frank G. Wells (1992-1994) Michael A. Wiener (1997-2009)
-
The CASA Columbia National Advisory Commission on Addiction Treatment
Drew E. Altman, PhD (Chair) President and Chief Executive Officer The Henry J. Kaiser Family Foundation Harvey V. Fineberg, MD, PhD President Institute of Medicine Mark S. Gold, MD University of Florida College of Medicine and McKnight Brain Institute Departments of Psychiatry, Neuroscience, Anesthesiology, Community Health & Family Medicine Chairman, Department of Psychiatry Shelly F. Greenfield, MD, MPH Chief Academic Officer, McLean Hospital Professor of Psychiatry, Harvard Medical School Director, Clinical and Health Services Research and Education Division on Alcohol and Drug Abuse, McLean Hospital Elizabeth R. Kabler President Rosenstiel Foundation Myles V. Lynk, JD Peter Kiewit Foundation Professor of Law and the Legal Profession Faculty Fellow, Center for Law, Science & Innovation’s Program in Public Health Law and Policy Sandra Day O’Connor College of Law Arizona State University
June E. Osborn, MD President Emerita Josiah Macy, Jr. Foundation Manuel T. Pacheco, PhD President Emeritus, University of Arizona and University of Missouri System The Honorable Jose R. Rodriguez Circuit Judge Ninth Judicial Circuit of Florida Reverend Msgr. Stephen J. Rossetti, PhD, DMin Clinical Associate Professor Associate Dean for Seminary and Ministerial Programs The Catholic University of America, The School of Theology and Religious Studies Former President and Chief Executive Officer Saint Luke Institute, Inc. Leonard D. Schaeffer Judge Robert Maclay Widney Chair & Professor University of Southern California Steven A. Schroeder, MD Distinguished Professor of Health and Health Care, Department of Medicine Director, Smoking Cessation Leadership Center University of California, San Francisco Louis W. Sullivan, MD President Emeritus Morehouse School of Medicine
-
Table of Contents
Foreword and Accompanying Statement by Drew Altman, PhD ............................................. i I. Introduction and Executive Summary .....................................................................................1
The CASA Columbia Study.................................................................................................4 Key Findings ........................................................................................................................6
Addiction Is a Brain Disease..........................................................................................6 As with Other Health Conditions, There Are Clear Risk Factors for
the Development of Addiction .................................................................................7 Addiction Frequently Co-Occurs with Other Health Conditions ..................................7 Addiction Can Be a Chronic Disease.............................................................................7 A Lack of Standardized Terminology Compromises Effective Interventions ...............7 Multiple Addictive Substances and Behaviors Frequently Are Involved in
Risky Use and Addiction .........................................................................................7 Public Attitudes about the Causes of Addiction Are Out of Sync with the Science .....8 Physicians and Other Health Care Providers Should Be on the Front Line for
Addressing this Disease ...........................................................................................8 Screening and Intervention Are Effective at Addressing
Risky Substance Use and Forestalling Addiction ....................................................9 Effective Therapies to Treat and Manage Addiction Exist ............................................9 The Importance of Tailored Interventions and Treatment ...........................................10 Public Attitudes about Addiction Treatment Reflect the Prevailing
Non-Medical Approach to Addiction Care ............................................................10 Most People in Need of Treatment Do Not Receive It ................................................10 Most Referrals to Publicly Funded Treatment Come from the
Criminal Justice System .........................................................................................11 Less than Half of Treatment Admissions Result in Treatment Completion ................12 Patients Face Formidable Barriers to Receiving Addiction Treatment .......................12 The Spending Gap........................................................................................................12 Most Funding for Addiction Treatment Comes from Public Sources .........................13 The Education, Training and Accountability Gap .......................................................13 The Profound Disconnect between Evidence and Practice ..........................................13
Recommendations and Next Steps.....................................................................................14 Reform Health Care Practice .......................................................................................14 Use the Leverage of Public Policy to Speed Reform in Health Care Practice ............15
II. What Is Addiction? .................................................................................................................19 Addiction Is a Brain Disease..............................................................................................20 The Risk Factors for Addiction..........................................................................................22
Genetic Risks ...............................................................................................................22 Biological Risks ...........................................................................................................23 Psychological Risks .....................................................................................................23 Environmental Risks ....................................................................................................23 Early Initiation of Use ..................................................................................................24
Risky Use and Addiction Frequently Co-Occur with Other Health Conditions ................24 Addiction Can Be a Chronic Disease.................................................................................25
-
Models for Understanding Addiction ................................................................................26 Evolving Approaches to Addressing Addiction ................................................................26 Defining the Terms ............................................................................................................29
The Continuum of Substance Use................................................................................29 Public Attitudes about Addiction .......................................................................................34
Perceived Causes of Addiction ....................................................................................35 III. Prevalence and Consequences ..............................................................................................39
Defining the Problem .........................................................................................................40 Risky Substance Users .......................................................................................................41
Risky Tobacco Use ......................................................................................................43 Risky Alcohol Use .......................................................................................................44 Risky Illicit Drug Use ..................................................................................................46 Risky Use of Controlled Prescription Drugs ...............................................................47
Addiction............................................................................................................................48 Special Populations ............................................................................................................51
Pregnant Women ..........................................................................................................51 Adolescents and Young Adults ....................................................................................51 Older Adults .................................................................................................................52 Co-Occurring Disorders ...............................................................................................52 Members of the Military Exposed to Combat..............................................................53 Involvement in the Justice System ...............................................................................55
Consequences of Risky Substance Use and Untreated Addiction .....................................55 Tobacco ........................................................................................................................58 Alcohol .........................................................................................................................59 Illicit Drugs ..................................................................................................................60 Controlled Prescription Drugs .....................................................................................61
IV. Screening and Early Intervention ........................................................................................63 The Need for Patient Education, Screening and Intervention throughout the Lifespan ....64
Childhood and Adolescence ........................................................................................64 Young Adulthood.........................................................................................................65 Middle and Later Adulthood ........................................................................................65
Attending to Co-Occurring Conditions ..............................................................................66 Patient Education and Motivation ......................................................................................66 Screening............................................................................................................................66
Laboratory Tests ..........................................................................................................68 Brief Interventions and Treatment Referrals .....................................................................69
Tobacco ........................................................................................................................69 Alcohol and Other Drugs .............................................................................................70
Effectiveness of Screening and Brief Interventions...........................................................71 Tobacco ........................................................................................................................72 Alcohol .........................................................................................................................72 Other Drugs ..................................................................................................................73
Implementing Screening and Brief Interventions in Health Care and Other Settings .......74 Primary Care ................................................................................................................74 Emergency and Trauma Care.......................................................................................76 Health Care for Pregnant Women ................................................................................77
-
Mental Health Care ......................................................................................................78 Dental Care ..................................................................................................................78 Pharmacies ...................................................................................................................78 High School, College and University Settings ............................................................78 Justice Settings .............................................................................................................79 The Workplace .............................................................................................................80 Government-Funded Social Service Systems ..............................................................81
Barriers to Effective Implementation of Screening and Brief Interventions .....................81 Insufficient Training ....................................................................................................81 Competing Priorities/Insufficient Resources ...............................................................82 Inadequate Screening Tools .........................................................................................83
V. Treatment and Management of Addiction ...........................................................................85 A Comprehensive Approach to Treatment ........................................................................86 Assessment .........................................................................................................................87 Stabilization .......................................................................................................................88
Cessation of Use ..........................................................................................................88 Detoxification ..............................................................................................................89
Acute Care .........................................................................................................................92 Pharmaceutical Therapies ............................................................................................92 Psychosocial Therapies ..............................................................................................102 Combined Therapies ..................................................................................................104 Nutrition and Exercise ...............................................................................................106
Chronic Disease Management .........................................................................................107 Medically Supervised Disease Management .............................................................107 Case Management ......................................................................................................108
Support Services ..............................................................................................................109 Mutual Support Services ............................................................................................109 Auxiliary Support Services ........................................................................................113
The Use of Technology in Addiction Treatment and Disease Management ...................114 Public Attitudes about Addictive Substances and the Need for Addiction Treatment ....114
Perceptions of the Relative Need for Treatment Based on Substance of Addiction .114 Perceptions of the Goals of Treatment .......................................................................115 Perceptions of the Types of Interventions that Constitute Treatment ........................116 Perceptions of the Effectiveness of Treatment ..........................................................116
VI. Tailored Treatment for Special Populations .....................................................................119 Co-occurring Medical Disorders......................................................................................119 Co-occurring Mental Health Disorders ............................................................................120
Tobacco Cessation .....................................................................................................121 Treatment for Addiction Involving Alcohol and Other Drugs ..................................121
Adolescents ......................................................................................................................122 Tobacco Cessation .....................................................................................................122 Treatment for Addiction Involving Alcohol and Other Drugs ..................................123
Women .............................................................................................................................124 Pregnant Women ........................................................................................................124
Older Adults .....................................................................................................................125 Racial and Ethnic Minorities ...........................................................................................126
-
Individuals of Minority Sexual Orientation .....................................................................126 Veterans and Active Duty Military ..................................................................................127 Individuals Involved in the Justice System ......................................................................128
Juvenile Offenders .....................................................................................................128 Adult Corrections .......................................................................................................128
VII. The Addiction Treatment Gap .........................................................................................131 Most People in Need of Treatment Do Not Receive It ....................................................133
Variations in the Treatment Gap by Primary Substance Involved ............................134 Variations in the Treatment Gap by Key Patient Characteristics ..............................135 Regional Variations in the Treatment Gap ................................................................137
Sources of Funding for Addiction Treatment ..................................................................137 Privately-Funded Treatment ......................................................................................138 Publically-Funded Treatment.....................................................................................138 Trends in Spending on Addiction Treatment .............................................................139 Expenditures by Providers and Types of Services .....................................................139
Treatment Admissions .....................................................................................................141 Treatment Referrals and Venues ......................................................................................142 Treatment Completion .....................................................................................................145
Variations in Treatment Completion by Source of Referral ......................................146 Variations in Treatment Completion by Primary Substance Involved ......................146 Variations in Treatment Completion by Key Patient Characteristics ........................146
Link between Funding Source, Type of Service Provided and Treatment Completion ..146 Barriers Patients Face in Accessing and Completing Addiction Treatment ....................147
Misunderstanding of the Disease ...............................................................................147 Negative Public Attitudes and Behaviors Toward People with Addiction ................148 Privacy Concerns .......................................................................................................150 Cost ............................................................................................................................151 Lack of Information about How To Get Help ...........................................................152 Limited Availability of Services ................................................................................152 Insufficient Social Support ........................................................................................153 Conflicting Time Commitments ................................................................................153 Negative Perceptions of the Treatment Process.........................................................153 Legal Barriers.............................................................................................................154
Barriers to Treatment Access and Completion in Special Populations ...........................154 Individuals with Co-Occurring Conditions ................................................................154 Pregnant and Parenting Women.................................................................................155 Adolescents ................................................................................................................155 Older Adults ...............................................................................................................156 The Homeless.............................................................................................................156 Veterans and Active Duty Military ............................................................................157 Rural Populations .......................................................................................................157 Native Americans.......................................................................................................158
-
VIII. The Spending Gap ............................................................................................................159 The Rational Approach to Risky Substance Use and Addiction .....................................159 Costs of Our Failure to Prevent and Treat Addiction as a Medical Condition ................160
The Largest Share of Costs Falls to the Health Care System ....................................160 Cost Savings of Addiction Screening, Intervention and Treatment ................................161
Screening and Early Intervention ...............................................................................162 Addiction Treatment and Disease Management ........................................................164
Insurance Coverage of Addiction Treatment is Limited ..................................................166 Parity Laws ................................................................................................................166 The Patient Protection and Affordable Care Act of 2010 ..........................................168 Gaps in Coverage within Public and Private Insurance Plans Continue to
Impede Comprehensive Addiction Care .................................................................169 IX. The Education, Training and Accountability Gap ...........................................................175
The Size and Shape of the Addiction Treatment Workforce ...........................................176 Licensing and Credentialing Requirements for Individuals who Provide
Addiction Treatment .....................................................................................................177 Medical Professionals ................................................................................................178 Mental Health Professionals ......................................................................................183 Acupuncturists ...........................................................................................................185 Addiction Counselors.................................................................................................186
Licensure, Certification and Accreditation Requirements for Addiction Treatment Programs and Facilities .................................................................................................187
State Licensing Requirements....................................................................................188 Federal Regulatory Requirements ..............................................................................189 Accreditation Requirements.......................................................................................190 Professional Staffing Requirements ...........................................................................191 Treatment Service Requirements ...............................................................................193 Quality Assurance Requirements ...............................................................................195
X. The Evidence-Practice Gap ..................................................................................................199 Current Approaches to Risky Substance Use and Addiction Are Inconsistent
with the Science and Evidence-Based Care ..................................................................199 Patient Education, Screening, Brief Interventions and Treatment Referrals .............200 Assessment, Stabilization and Acute Treatment ........................................................204 Tailored Treatment Services ......................................................................................208 Chronic Disease Management ...................................................................................210
Barriers to Closing the Evidence-Practice Gap ...............................................................212 The Addiction Treatment Workforce is Not Qualified to Implement
Evidence-Based Practices .......................................................................................212 Health Professionals do not Implement Evidence-Based Addiction Care Practices .216 Inadequate Use and Development of Pharmaceutical Treatments for Addiction ......219 Inadequate Quality Assurance ...................................................................................220 Inadequate Insurance Coverage .................................................................................222
No Overarching Organizing Body for Addiction Science and Treatment .................223 Efforts to Integrate Substance Use Prevention and Treatment into
Mainstream Medicine ...................................................................................................223
-
XI. Recommendations and Next Steps .....................................................................................227 Reform Health Care Practice ...........................................................................................228
Incorporate Screening and Intervention for Risky Substance Use, and Diagnosis, Treatment and Disease Management for Addiction into Routine Medical Practice ..............................................................................228
All Medical Schools and Residency Training Programs Should Educate and Train Physicians to Address Risky Substance Use and Addiction ......................229
Require Non-Physician Health Professionals to Be Educated and Trained to Address Risky Substance Use and Addiction ......................................................229
Develop Improved Screening and Assessment Instruments ......................................230 Establish National Accreditation Standards for All Addiction Treatment
Facilities and Programs that Reflect Evidence-Based Care .................................230 Standardize Language Used to Describe the Full Spectrum of Substance Use and
Addiction..............................................................................................................230 Use the Leverage of Public Policy to Speed Reform in Health Care Practice ................231
Condition Grants and Contracts for Addiction Services on the Provision of Quality Care .........................................................................................................231
Educate Non-Health Professionals about Risky Substance Use and Addiction ........231 Identify Patients at Risk in Government Programs and Services where Costs of
Risky Use and Addiction Are High .....................................................................231 Develop Tools to Improve Service Quality ...............................................................231 License Addiction Treatment Facilities as Health Care Providers ............................232 Require Adherence to National Accreditation Standards that Reflect Evidence-Based Care ..............................................................................232 Require that All Insurers Provide Coverage for Comprehensive Addiction Care .....232 Expand the Addiction Medicine Workforce ..............................................................232 Implement a National Public Health Campaign ........................................................233 Invest in Research and Data Collection to Improve and Track Progress in Addiction
Prevention, Treatment and Disease Management ................................................233 Implement the National Institutes of Health’s (NIH) Recommendation to Create a
Single Institute Addressing Substance Use and Addiction ..................................234 Appendix A-Methodology .........................................................................................................235 Appendix B-Key Informant Interview Guide and List of Key Informants ..........................245 Appendix C-National Addiction Belief and Attitude Survey (NABAS) ...............................253 Appendix D-Survey of New York State Addiction Treatment Directors .............................269 Appendix E-Survey of New York State Addiction Treatment Staff .....................................285 Appendix F- National Panel and National Online Survey of Members of Professional
Associations Involved in Addiction Care ...........................................................................297 Appendix G-Survey of Participants in Recovery ....................................................................305 Appendix H-Screening and Assessment Instruments .............................................................311 Notes ............................................................................................................................................325 Bibliography ...............................................................................................................................429
-
-i-
Accompanying Statement by Drew E. Altman, PhD, Chair, The CASA Columbia National Advisory Commission on Addiction Treatment
In homes, doctors’ offices, hospitals, schools, prisons, jails and communities across America, misperceptions about addiction are undermining medical care. Although advances in neuroscience, brain imaging and behavioral research clearly show that addiction is a complex brain disease, today the disease of addiction is still often misunderstood as a moral failing, a lack of willpower, a subject of shame and disgust. Addiction affects 16 percent of Americans ages 12 and older--40 million people. That is more than the number of people with heart disease (27 million), diabetes (26 million) or cancer (19 million). Another 32 percent of the population (80 million) uses tobacco, alcohol and other drugs in risky ways that threaten health and safety. Like other public health and medical problems, we understand the risk factors for addiction. We have effective ways of screening for risky use and intervening. While as of now there is no cure for addiction, there are effective psychosocial and pharmaceutical treatments and methods of managing the disease. But as this landmark report by CASA Columbia shows in sharp detail, this is where the comparison with other health conditions ends. Unlike other diseases, we do little to effectively prevent and reduce risky use and the vast majority of people in need of addiction treatment do not receive anything that approximates evidence-based care. The medical system, which is dedicated to alleviating suffering and treating disease, largely has been disengaged from these serious health care problems. The consequences of this inattention are profound. America’s failure to prevent risky use and effectively treat addiction results in an enormous array of health and social problems such as accidents, homicides and suicides, child neglect and abuse, family dysfunction and unplanned pregnancies. CASA Columbia estimates that risky substance use and
-
-ii-
addiction are this nation’s largest preventable and most costly health problems, accounting for one third of hospital inpatient costs, driving crime and lost productivity and resulting in total costs to government alone of at least $468 billion each year. In many ways, America’s approach to addiction treatment today is similar to the state of medicine in the early 1900s. In 1908, the Council on Medical Education of the American Medical Association turned to the Carnegie Foundation for the Advancement of Teaching to conduct a survey of Medical Education in the U.S. That survey, which became known as the Flexner Report, was led by Abraham Flexner who famously observed of the discrepancy among physicians’ qualifications, “there is probably no other country in the world in which there is so great a distance and so fatal a difference between the best, the average and the worst.” This CASA Columbia report identifies a similar gulf in the knowledge and practice skills of addiction treatment providers today. The education and training of persons providing addiction treatment vary considerably by state. In many cases, entry requirements for the profession are minimal in terms of education and are based on apprenticeship models rather than on science-based instruction. Flexner noted that the turn of the 19th to 20th century was a time of scientific progress in the understanding of disease and its treatment; however, due to the lack of a standardized and rigorous education for physicians, society reaped “but a small fraction of the advantage which current knowledge has the power to confer.” Similarly, 100 years later, advances in science and medicine have drawn a much clearer picture of addiction--including its causes, correlates and how to treat it--yet we are woefully unprepared to apply this evidence to practice. Our medical professionals are not trained to look for risky use and addiction or to intervene or treat the disease. Without medical attention, the disease progresses, forcing doctors to expend valuable resources treating the more than 70 other conditions requiring medical attention that result from substance use and addiction, while taxpayers shoulder the costs of these health and
other social consequences. This neglect by the medical system has led to the creation of a separate and unrelated system of addiction care that struggles to treat the disease without the resources or the knowledge base to keep pace with science and medicine. Because addiction affects cognition and is associated primarily with the difficult social consequences that result from our failure to prevent and treat it, those who suffer from the disease are poor advocates for their own health. And due in large part to the shame, stigma and discrimination attached to the disease, individuals with addiction and their family members too often are isolated in their struggle to understand the disease and find help. Only recently have we begun to see those affected by the disease working to raise awareness in ways, for example, that families of breast cancer victims have done. But these efforts are small, challenged by public misunderstanding and have failed to raise sufficient funding for needed research. Even individuals who can transcend the stigma face significant barriers to receiving effective care, and this report paints a dismal picture of a treatment ‘non-system.’ While almost half of Americans say they would go to their health care providers for help, most doctors are uninformed about this disease and rarely are equipped to offer a diagnosis, provide treatment or connect patients with appropriate specialty care. Insurance coverage varies widely. Services rarely are tailored to individual needs and are based primarily on an acute care model rather than recognizing the chronic nature of the disease. There are no national standards of care. Patients face a patchwork of treatment programs with vastly different approaches; many offer unproven therapies and little medical supervision. Some promise “one time” fixes; others offer posh residential treatment at astronomical prices with little evidence justifying the cost. Even for those who do have insurance coverage or can pay out-of-pocket, there are no outcome data reflecting the quality of treatment providers so that patients can make informed decisions.
-
-iii-
This report focuses long overdue attention on the disease of addiction. It clarifies the important difference between this disease and risky use of addictive substances; identifies the human and economic costs of our current approach to these health problems; and documents the breadth of available knowledge on how to prevent risky use and treat addiction. As our nation struggles to reduce skyrocketing health care costs, there are few targets for cost savings that are as straightforward as preventing and treating risky substance use and addiction. This report shows that modest public health interventions and relatively inexpensive addiction therapies, compared with other medical treatments, would reduce this burden significantly. The report calls for modernizing addiction treatment--to harness the scientific knowledge we have acquired to prevent risky use and treat this disease. This report is a call to action. Like the Flexner Report a century ago, it shines a bright light on the problem and offers a roadmap for action. Addiction Medicine: Closing the Gap between Science and Practice represents more than five years of intensive research, and draws on policy and treatment research conducted by CASA Columbia over two decades and on a wide body of scientific, clinical and policy research conducted by others. This major undertaking was the result of the work of a large team of dedicated individuals and institutions and was conducted with the able advice and counsel of The CASA Columbia National Advisory Commission on Addiction Treatment which I had the privilege to chair. The Commission includes an impressive group of individuals knowledgeable about the many aspects of substance use and addiction in America today. We are grateful for their expert assistance. The project was made possible by the generous financial support of The Annenberg Foundation; The Diana, Princess of Wales Memorial Fund and The Franklin Mint; The New York Community Trust; and the Adrian and Jessie Archbold Charitable Trust.
Peter D. Hart Research Associates conducted the National Addiction Belief and Attitude Survey for this report; Survey Research Laboratory (SRL) of the University of Illinois at Chicago administered the survey of New York State addiction treatment providers. We are grateful to Karen Carpenter-Palumbo, former director of the New York State Office of Alcoholism and Substance Abuse Services (OASAS) for helping to make the New York State survey possible. We thank the following organizations which generously helped connect CASA Columbia with treatment providers who participated in a national online survey of members of professional associations involved in addiction care: The American Academy of Addiction Psychiatry (AAAP); the American Association for the Treatment of Opioid Dependence (AATOD); the American Psychological Association (APA); the American Society of Addiction Medicine (ASAM); the Association for the Treatment of Tobacco Use and Dependence (ATTUD); NAADAC, the Association for Addiction Professionals; the National Association of Addiction Treatment Providers (NAATP); the National Association of County Behavioral Health and Developmental Disability Directors (NACBHDD); the National Council for Community Behavioral Healthcare (National Council); the State Associations of Addiction Services (SAAS); and Treatment Communities of America (TCA). Also, we thank the following organizations for connecting us with individuals in long-term recovery for CASA Columbia’s online survey of this population: Hazelden, Freedom Institute, Faces and Voices of Recovery, Betty Ford Center, National Council on Alcoholism and Drug Dependence, Inc. (NCADD), Treatment Communities of America (TCA), Alcoholism and Substance Abuse Providers of New York State, Inc. (ASAP) and an anonymous treatment program alumni group. Finally, we are grateful to the 176 key informants who shared their insight and recommendations. Susan E. Foster, MSW, CASA Columbia’s Vice President and Director of Policy Research and Analysis, was the principal investigator and staff director for this effort. The senior research
-
-iv-
manager was Linda Richter, PhD, Associate Director of the Division and CASA Columbia Scholar. The data collection and analysis was conducted by CASA Columbia’s Data Analysis Center (SADACSM), headed by Roger Vaughan, DrPH, CASA Columbia Fellow and Professor of Clinical Biostatistics, Department of Biostatistics, Mailman School of Public Health at Columbia University, and associate editor for statistics and evaluation for the American Journal of Public Health. He was assisted by Elizabeth Peters and Sarah Tsai, MA. Emily Feinstein, JD, senior policy analyst, assisted with the research and writing. Other research staff members who worked on the project are: Nina Lei, Mark Stovell, Akiyo Kodera, Dina Feivelson, PhD, Gina Hijjawi, PhD, Harold Wenglinsky, PhD, Swapna Reddy, JD, Kristen Keneipp, MHS, Nabil Ansari and Sarah Blachman. David Man, PhD, MLS, is CASA Columbia’s librarian; he was assisted by Barbara Kurzweil. Jennie Hauser managed the bibliographic database and Jane Carlson handled administrative details. While many individuals and institutions contributed to this effort, the findings and opinions expressed herein are the sole responsibility of CASA Columbia.
-
-1-
Chapter I Introduction and Executive Summary
A large and growing body of scientific research has demonstrated clearly that addiction involving nicotine, alcohol, illicit drugs and controlled prescription drugs* is a complex brain disease.1 It affects 15.9 percent of the United States population ages 12 and older (40.3 million)† 2--more than the share of the population with heart disease,‡ diabetes or cancer.3 Another 31.7 percent of the population (80.4 million), while not addicted, engages in risky use§ of addictive substances in ways that threaten health and safety.4 * In this report, we have used the general term addiction to apply to those who meet criteria for past-month nicotine dependence based on the Nicotine Dependence Syndrome Scale (NDSS) and those who meet diagnostic criteria for past year alcohol and/or other drug abuse or dependence (excluding nicotine) in accordance with the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). (The DSM, the most widely accepted diagnostic system in the U.S. for such conditions, refers to substance abuse and substance dependence collectively as substance use disorders. The diagnostic criteria for nicotine dependence in the NDSS parallel those of the DSM-IV). This definition is consistent with the current move to combine abuse and dependence into an overarching diagnosis of addiction in the upcoming DSM-V. The term addiction also has been used in reference to compulsive behaviors involving eating, gambling and other activities that affect the brain’s reward system and which may develop independent of or in combination with other manifestations of addiction. This report, however, focuses only on addiction involving nicotine, alcohol and other drugs. † This estimate excludes the institutionalized population, for which rates of addiction are higher. ‡ Includes coronary heart disease, angina pectoris, heart attack or any other heart condition or disease, excluding hypertension and stroke. § Risky users of addictive substances are defined in this report as those who currently use tobacco products, exceed the U.S. Department of Agriculture (USDA) Dietary Guidelines for safe alcohol use, misuse controlled prescription drugs, use illicit drugs, or engage in some combination of these forms of substance use, but do not meet clinical diagnostic criteria for addiction. (See page 5.)
-
-2-
Addiction and risky use constitute the largest preventable and most costly health problems facing the U.S. today.5 It is estimated that more than 20 percent of deaths in the U.S. are attributable to tobacco, alcohol and other drug use.6 Addiction and risky use cause or contribute to more than 70 other conditions requiring medical care, including cancer, respiratory disease, cardiovascular disease, HIV/AIDS, pregnancy complications, cirrhosis, ulcers and trauma.7 They also drive and contribute to a wide range of costly social consequences, including crime, accidents, suicide, child neglect and abuse, family dysfunction, unplanned pregnancies and lost productivity.8 Costs of addiction and risky substance use to government alone total at least $468 billion each year.9 While both addiction and risky use of addictive substances contribute to these consequences, they are very different conditions. Addiction is a disease and, like other diseases, it can and should be diagnosed and treated in the context of the medical system,* using available evidence-based practices. Risky use of addictive substances is a public health problem and tools are available for a wide range of professionals in the health, social services, education, criminal justice and other sectors to screen for it and intervene to reduce it and its consequences, including the potential development of addiction. Despite the prevalence of these conditions, the enormity of the consequences that result from them and the availability of effective solutions, screening and early intervention for risky substance use is rare and the vast majority of people in need of addiction treatment do not receive anything that approximates evidence-based care. Nine out of 10 people (89.1 percent) who meet diagnostic criteria for addiction
* Involving interdisciplinary teams of physicians (of multiple medical specialties and subspecialties), nurses, physician assistants, nurses and nurse practitioners and graduate-level clinical mental health professionals (psychologists, social workers, counselors), working collaboratively with auxiliary and support personnel.
involving alcohol and drugs other than nicotine report receiving no treatment† at all;10 as a society, we do not even collect information on the number of people receiving treatment for addiction involving nicotine. There is no other disease that affects so many people, has such far-reaching consequences and for which there is such a broad range of effective interventions and treatments that is as neglected as the disease of addiction. This report documents the significant body of evidence defining and describing the disease of addiction and the risky use of addictive substances. It reveals the size and shape of the populations in need of screening, intervention and treatment. It reviews the evidence of effective screening, intervention, diagnostic, treatment and disease management tools and therapies. It outlines the consequences and costs of our failure to prevent risky substance use and treat addiction effectively. Finally, it examines the profound gaps between those who need treatment and those who receive it, and between the services they receive and what constitutes quality care. Key factors driving these gaps include: Inadequate Integration of Addiction Care
into Mainstream Medical Practice: Addiction prevention and treatment are for the most part removed from routine medical practice.11 In spite of the fact that about 80 percent of Americans‡ visited at least one physician or other health care professional in
† Treatment is defined in this report as psychosocial and pharmaceutical therapies. Detoxification, mutual support programs, peer counseling, other support services (including religious-based counseling) and services received in an emergency department are excluded from the definition. Services provided in prison or jail settings also are excluded since they cannot be identified in the data sources used for this analysis; furthermore, in CASA Columbia’s 2010 report (Behind Bars Update: Substance Abuse and America’s Prison Population), more than 70 percent of those receiving addiction-related services in prisons and jails received support services rather than any form of professional treatment. ‡ Ages 18 and older.
-
-3-
the past year,12 and more than two-thirds of people with addiction are estimated to be in contact with a primary or emergency care physician about twice a year,13 most physicians and other health professionals* do not identify or diagnose the disease or know what to do with patients who present with identifiable and treatable signs and symptoms. And, unlike other diseases, physicians too often lack access to available, trained and certified addiction physician specialists for consultation or referral. Instead of addressing addiction, the medical field primarily has focused its efforts on treating the secondary and tertiary complications of addiction, allowing the public health epidemic to advance unchecked. Furthermore, whereas the main criterion for determining whether health care services should be provided to patients in mainstream medicine is the principle of medical necessity,14 patients needing addiction treatment may face stringent eligibility criteria for treatment entry, including insurance benefit restrictions, limited availability of treatment slots, long waiting lists, lack of child care and the requirement to comply with all rules and treatment protocols.15 There simply is no other disease where appropriate medical treatment is not provided by the health care system and where patients instead must turn to a broad range of practitioners largely exempt from medical standards.
Inadequate Education and Training of
Addiction Treatment Providers: The majority of those who currently make up the addiction treatment provider workforce are not equipped with the knowledge, skills or credentials necessary to provide the full range of evidence-based services to treat the disease.
* The term “health professional” as used in this report includes medical professionals (physicians, physician assistants, nurses and nurse practitioners, dentists, pharmacists) and graduate-level clinical mental health professionals (psychologists, social workers, counselors).
Addiction counselors, who make up the largest share of providers of addiction treatment services, provide care for patients with a medical disease yet they are not required to have any medical training and most states do not require them to have advanced education of any sort.†
Physicians and other medical
professionals, who make up the smallest share of providers of addiction treatment services, receive little education or training in addiction science, prevention and treatment.
Inadequate Accountability for Addiction
Treatment Providers: Addiction treatment providers, facilities and programs are not adequately regulated or held accountable for providing treatment consistent with medical
† Only six states require a bachelor’s degree and only one state requires a master’s degree.
Published in the American Journal of Public Health
July, 1919 There is urgent need for widespread and early education of the medical profession, legislators, administrative authorities and laity into the facts of addiction disease… As a definite clinical entity of physical disease, addiction is practically untaught in the school and unappreciated by the average medical man… In the light of available clinical information and study and in the light of competent laboratory research we are forced as a profession to admit that we have not treated our addiction sufferers with sympathetic understanding and clinical competency and that the blame for the past failure to control the [narcotic] drug problem rests largely upon the educational inadequacy of our medical profession, and institutions of scientific and public health education.16
--Ernest S. Bishop, MD, FACP
-
-4-
standards and proven treatment practices. The credentials of treatment providers vary dramatically from state to state and from program to program. Compounding the problem, quality assurance standards that do exist focus more on administrative processes than on measureable patient outcomes.
Inadequate Allocation of Financial Resources: Financial investments in addressing addiction and risky substance use are aimed disproportionately at coping with their costly health and social consequences rather than at the effective implementation of available prevention, intervention and treatment approaches. In 2010, only 1.0 percent ($28.0 billion) of total health care costs went to treating the disease of addiction.17 Spending on addiction treatment disproportionately falls to the public sector. In contrast to the role of private insurance in general health care spending--where it covers 54.4 percent of costs--private insurers cover only 20.8 percent of the costs of addiction treatment, and the private share has been decreasing.18
This profound gap between the science of addiction and current practice related to prevention and treatment is a result of decades of marginalizing addiction as a social problem rather than treating it as a medical condition. Much of what passes for “treatment” of addiction bears little resemblance to the treatment of other health conditions. Much of what is offered in addiction “rehabilitation” programs has not been subject to rigorous scientific study and the existing body of evidence demonstrating principles of effective treatment has not been taken to scale or integrated effectively into many of the treatment programs operating nationwide. This is inexcusable given decades of accumulated scientific evidence attesting to the fact that addiction is a brain disease with significant behavioral components for which there are effective interventions and treatments. It also is unfair to the thousands of addiction counselors who struggle, in the face of extreme resource limitations and no medical training, to provide
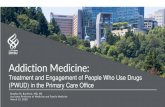
help to patients with the disease of addiction and numerous co-occurring medical conditions. America’s tendency to frame risky use of addictive substances and addiction as the same issue and as moral or social problems has resulted in an unmitigated failure on the part of policymakers and the health care community to educate the public about these health problems in ways that can help prevent them and to offer effective interventions and treatments that match those offered for other health conditions; instead the focus has weighed heavily toward law enforcement. The end result is that we have declared war on drugs rather than mounting a rational approach to prevention, treatment and finding a cure for the disease of addiction. We largely have punished rather than treated those in need of help even though treatment for a disease and accountability for behavior are not antithetic concepts. It is long past time for health care practice to catch up with the science. Failure to do so is a violation of medical ethics, a cause of untold human suffering and a profligate misuse of taxpayer dollars. The CASA Columbia Study Substance use can be understood as a continuum ranging from having never used tobacco, alcohol or another drug* at one end to having an unmanaged chronic, relapsing disease† at the other. (Figure 1.A)
* Including any use of illicit drugs or the misuse of controlled prescription drugs. † This continuum focuses on substance use; the category labeled addiction includes those individuals who meet current clinical criteria for this disease but does not include all individuals with addiction.
-
-5-
12.7 25.2 14.5 31.7 15.9
* Includes tobacco, alcohol, illicit drugs and misuse of controlled prescription drugs.Source: CASA Columbia analysis of The National Survey on Drug Use and Health (NSDUH), 2010.
Figure 1.AContinuum of Substance Use
Percent of Population Age 12+ by Level of Substance Use*
Never Used
No Current
Use
Non-Risky Use
RiskyUse
Addiction
While this report focuses primarily on those with the disease of addiction, it makes an important distinction between addiction and risky use of addictive substances: Those with the active disease of addiction*
are defined in this report as meeting the clinical diagnostic criteria for past month nicotine dependence or past year alcohol and/or other drug abuse or dependence. Individuals who meet diagnostic criteria for addiction are targets for appropriate, evidence-based clinical interventions by physicians and other health professionals. Addiction afflicts 15.9 percent of the U.S. population ages 12 and older (40.3 million people).19
Risky users of addictive substances are defined in this report as those who currently† use tobacco products, exceed the U.S. Department of Agriculture (USDA) Dietary
* Available data allow us to include only those who meet behavioral criteria in accordance with the diagnostic standards, meaning in most cases that their disease is not currently being managed. Individuals who have the disease of addiction but do not meet diagnostic criteria for past month (nicotine) or past year (alcohol and other drug) addiction are not included. † In the past 30 days.
Guidelines for safe alcohol use,‡ 20 misuse controlled prescription drugs,§ use illicit drugs** 21 or engage in some combination of these forms of substance use but do not meet clinical diagnostic criteria for addiction. Risky use can result in devastating and costly health and social consequences including the disease of addiction. Risky users are targets for public health efforts aimed at reducing risky use and for health professionals’ efforts to prevent risky use from progressing to the disease of addiction. Approximately one-third (31.7 percent) of the U.S. population ages 12 and older (80.4 million people) are risky substance users.22
‡ The U.S. Department of Agriculture Dietary Guidelines for safe alcohol use are no more than one drink a day for women, no more than two drinks a day for men and no alcohol consumption for: (1) persons under the age of 21; (2) pregnant women; (3) individuals who cannot restrict their drinking to moderate levels; (4) individuals taking prescription or over-the-counter medications that can interact with alcohol; (5) individuals with certain specific medical conditions (e.g., liver disease, hypertriglyceridemia, pancreatitis); and (6) individuals who plan to drive, operate machinery, or take part in other activities that require attention, skill or coordination or in situations where impaired judgment could cause injury or death (e.g., swimming). Due to data limitations, we were unable to include categories 4-6 in our calculation of risky drinkers. § For data analysis purposes, the national survey examined for this report defines misuse of controlled prescription medications more generally as “taking a controlled prescription drug not prescribed for you or taking it in a manner not prescribed for the experience or feeling it causes.” The misuse of over-the-counter medications also constitutes risky use; however, rates of risky use in this report do not include the misuse of these medications since they are not directly measured in the national surveys that were analyzed for this study. ** Substances controlled (either through prohibited or restricted use) through the federal Controlled Substances Act of 1970, which created a system for classifying illicit and prescription drugs according to their medical value and their potential for misuse. In this analysis, illicit drugs include marijuana/hashish, cocaine/crack, heroin, hallucinogens, Ecstasy, methamphetamine and inhalants.
-
-6-
To document the research on the causes, consequences and extent of risky substance use and addiction; the available tools for effective interventions and for treatment; the gap between the need for such interventions and treatments and the actual standard of care; the driving forces behind this substantial gap; and to develop concrete recommendations for minimizing it, CASA Columbia conducted:* A thorough review of more than 7,000
scientific articles, reports, books and other reference materials related to the science of addiction, the consequences of risky use and addiction, the prevention of risky use and treatment of addiction and barriers to improved care (see Appendix A);
Secondary analysis of five national data sets (see Appendix A);
Interviews with and suggestions from 176
leading experts in a broad range of fields relevant to the report, including researchers, physicians and other health professionals, other treatment providers, policymakers and members of professional associations, advocacy organizations, health insurers, pharmaceutical companies and organizations of people with the disease of addiction. Whereas the majority of these experts provided their thoughts in the context of an open-ended interview guide designed by CASA Columbia to explore key themes related to this project, some provided advice, suggestions and feedback about specific content to be included in this report (see Appendices A and B);
Focus groups and a national general
population survey assessing the attitudes and beliefs of 1,303 adults with regard to addiction and its treatment: the National Addiction Belief and Attitude Survey (NABAS) (see Appendices A and C);
Two statewide surveys of addiction
treatment providers in New York: one of 83 * See Appendix A for a more detailed description of the key methodological components of the study.
program directors and one of 141 staff treatment providers (see Appendices A, D and E);
A national panel of treatment providers and
an online survey of 1,142 members of professional associations involved in addiction care (see Appendices A and F);
An online survey of 360 individuals with a
history of addiction who are managing the disease (see Appendices A and G);
An in-depth analysis of state and federal
governments’ and professional associations’ licensing and certification requirements for individual treatment providers and addiction treatment facilities and programs, as well as accreditation requirements for facilities and programs (see Appendix A); and
A case study of addiction treatment in New
York State and New York City that drew from the research described above and the findings of which are incorporated into the report where relevant (see Appendix A).
Key Findings Addiction Is a Brain Disease Addiction is a complex brain disease with significant behavioral characteristics.23 Nicotine, alcohol, illicit drugs and controlled prescription drugs all affect the pleasure and reward circuitry of the brain in similar ways.24 Over time, continued use of these substances can physically alter the structure and function of the brain, dramatically affect judgment and behavior25 and drive a compulsion to obtain and use them, even in the face of mounting negative consequences.26 Growing evidence also points to structural and functional differences in the brain and to genetic factors that may predispose certain individuals to addiction.27
-
-7-
As with Other Health Conditions, There Are Clear Risk Factors for the Development of Addiction Risk factors for developing addiction include a genetic predisposition, structural and functional brain vulnerabilities, psychological factors and environmental influences. Whereas biological, psychological and environmental factors--such as impairments in the brain’s reward circuitry, compensation for trauma and mental health problems, easy access to addictive substances, substance use in the family or media and peer influences--play a large role in whether an individual starts to smoke, drink, or use other drugs,28 genetic factors are more influential in determining who develops the disease of addiction.29 A factor that is particularly predictive of risk, however, is the age of first use; in 96.5 percent of cases, addiction originates with substance use before the age of 2130 when the brain is still developing and is more vulnerable to the effects of addictive substances.* 31 Addiction Frequently Co-Occurs with Other Health Conditions Addiction frequently co-occurs with, contributes to or causes a wide range of medical conditions. Both risky substance use and addiction cause or contribute to more than 70 other conditions requiring medical care, such as heart disease and cancer,32 as well as mental health and behavioral disorders--including depression, anxiety, post-traumatic stress disorder, bipolar disorder, schizophrenia and other neuropsychiatric disorders.33 Addiction Can Be a Chronic Disease There is tremendous variation in the severity and course of the disease of addiction and of its symptoms. Some individuals may experience one episode in which their symptoms meet clinical diagnostic criteria for addiction and be non-symptomatic thereafter.34 In many cases, * These individuals also might have a predisposition to develop addiction, irrespective of their actual use of addictive substances.
however, addiction manifests as a chronic disease--a persistent or long-lasting illness--which requires ongoing professional treatment and management.35 However, very few people with addiction actually receive adequate, effective, evidence-based treatment,36 and the usual approach to treatment involves brief, episodic interventions rather than a model based on long-term chronic disease management. As a result, high rates of relapse, while comparable to other chronic diseases, may be due at least in part to inadequate or ineffective interventions and treatments.37 A Lack of Standardized Terminology Compromises Effective Interventions Terms used to describe different levels of involvement with addictive substances--such as experimentation, use, misuse, excessive use, abuse, dependence and addiction--lack precision, obscuring important differences in the nature and severity of the illness and complicating our ability to intervene and treat it effectively. Even the word “treatment” lacks precision with regard to addiction, since historically it has been used to refer to a host of interventions, many of which are not based in the clinical and scientific evidence as are treatments for other diseases. Multiple Addictive Substances and Behaviors Frequently Are Involved in Risky Use and Addiction Traditionally, risky substance use and addiction have been addressed largely on a substance-specific basis. Growing understanding of the nature of risky use and the disease of addiction--including the risk factors, symptoms and the neuropsychological effects of addictive substances--helps to explain the significant proportion of risky users and those who are addicted who are involved with more than one addictive substance. Among risky substance users who do not meet diagnostic criteria for addiction, 30.6 percent are risky users of more than one substance. Among those who are addicted, 55.7 percent are risky users of one or
-
-8-
more other substances and 17.3 percent have addiction involving multiple substances.38 Emerging research also suggests that other behavioral manifestations of addiction (e.g., obesity, gambling, sexual addiction) share common neuropsychological and genetic pathways with addiction involving substances,39 underscoring the importance of treating the antecedents, manifestations and consequences of addiction more generally. When treatments are too highly focused on a specific addictive substance or behavior, they may not be addressing the actual underlying disease of addiction or the possibility of addiction substitution, where a patient may replace one form of addiction with another.40 Public Attitudes about the Causes of Addiction Are Out of Sync with the Science CASA Columbia’s national survey of the attitudes and beliefs of adults in the U.S. with regard to addiction and its treatment (the NABAS) found that while there is public recognition of the role of genetics and biological factors in the development of addiction, approximately one-third of Americans continue to view addiction as a sign of lack of will power or self-control.41 Physicians and Other Health Professionals Should Be on the Front Line Addressing this Disease As with other diseases, addiction should be addressed within the medical system by physicians (including multiple medical specialties and sub-specialties) and a multi-disciplinary team of health professionals including physician assistants, nurses and nurse practitioners, and graduate level clinical psychologists, social workers and counselors. In order to treat addiction and reduce risky substance use and the related consequences, physicians and other health professionals must: Understand the risk factors, how these risks
vary across the lifespan, how risky
substance use that does not result in addiction has far-reaching adverse consequences and that addiction frequently co-occurs with other health conditions;
Educate patients, and their families if
relevant, about these risks, the nature of the disease of addiction and the adverse consequences of risky substance use;
Screen for risky substance use and symptoms of addiction and co-occurring health conditions using tools that have been proven to be effective;
Provide brief interventions when appropriate; and
Treat and manage the disease or provide referrals to specialty care if needed.
Non-laboratory-based screening for risky substance use can be conducted by a wide range of trained health professionals and brief interventions can be conducted by physicians and by appropriately trained clinicians, supervised as necessary. All aspects of stabilization and treatment--including laboratory-based screening, assessment, acute care and disease management--should be managed by a physician, as is the case with other medical illnesses. Highly-trained clinical mental health professionals can provide psychosocial therapies as part of a treatment plan established and managed by the patient’s physician. Case management can be provided by nurses and nurse practitioners, physician assistants and clinical mental health professionals if appropriately trained in addiction and if the services are performed under the supervision of a physician. Paraprofessionals and non-clinically trained and credentialed counselors can provide auxiliary services as part of a comprehensive treatment and disease management plan.
-
-9-
Referrals to specialty addiction care should be made to trained and credentialed addiction physician specialists.* 42 Screening and Intervention Are Effective at Addressing Risky Substance Use and Forestalling Addiction Screening and brief interventions have been found to be effective tools for addressing the risky use of tobacco,43 alcohol,44 illicit drugs and controlled prescription drugs45 in multiple settings and in many population groups.46 A range of screening tools exist and typically include written or oral questionnaires and, less frequently, clinical and laboratory tests. However, most screening tools are substance specific; an instrument that screens for risky use or addiction involving all substances as a unified dimension--and that makes appropriate distinctions for age, culture and gender--has yet to be developed. For those who screen positive for risky substance use that does not meet the threshold of clinical addiction, a brief intervention--typically involving motivational interviewing techniques and substance-related education--is an effective, low-cost approach to reducing risky substance use.47 Effective Therapies to Treat and Manage Addiction Exist For individuals showing signs of addiction, a comprehensive assessment of the stage and severity of the disease and the provision of treatment and disease management are critical to improving health and preventing further health and social consequences.48 As is true of other chronic diseases, while all patients with
* There are two major categories of addiction physician specialists: physician experts in addiction medicine--Diplomates of the American Board of Addiction Medicine (ABAM)--and physician experts in addiction psychiatry (psychiatrists with sub-specialty certification in addiction psychiatry)--Diplomates of the American Board of Psychiatry and Neurology (ABPN).
addiction will not respond equally well to treatment, the provision of evidence-based treatment does increase the odds of success. Addiction is a disease that can be treated and managed effectively within the medical profession using an array of evidence-based pharmaceutical and psychosocial approaches. In accordance with standard medical practice for the treatment of other chronic diseases, best practices for the effective treatment and management of addiction must be consistent with the scientific evidence of the causes and course of the disease. Best practices require:49 Comprehensive assessment of the extent
and severity of the disease, determination of a clinical diagnosis, evaluation of co-occurring health conditions and the development of a tailored treatment plan;
Stabilization of the patient’s condition via
cessation of substance use and medically supervised detoxification, when necessary, as a precursor to treatment;
Acute Care delivered by qualified health care professionals via evidence-based pharmaceutical and/or psychosocial addiction treatments, accompanied by treatment for co-occurring health conditions;
Chronic Disease Management to help the patient maintain the progress achieved during acute treatment and prevent relapse. The process should be medically supervised and should involve pharmaceutical and/or psychosocial therapies and continued management of co-occurring health conditions as indicated; and
Support Services including the provision of auxiliary services such as legal, educational, employment, housing and family supports, as well as nutrition and exercise counseling and connection to mutual support programs.
-
-10-
The Importance of Tailored Interventions and Treatment Each life phase presents unique vulnerabilities for risky substance use and the onset of the disease of addiction. Recognizing these differences as well as the basic risk factors for each is critical to reducing risky substance use and addiction. Certain populations--such as pregnant women,50 the young51 and the elderly52--are more vulnerable to the damaging and addictive effects of tobacco, alcohol and other drugs. Among members of the military exposed to combat,53 persons with co-occurring health conditions54 and individuals involved in the justice system55 the likelihood of addiction is significantly higher than in the general population. Treatment must be tailored to the particular stage and severity of the disease, a patient’s overall health status, past treatments and any other personal characteristics and life circumstances that might affect patient outcomes.56 These include patients with co-occurring health conditions, adolescents, women, older adults, racial and ethnic minorities, individuals of minority sexual orientation, veterans and individuals involved in the justice system. The research evidence clearly demonstrates that a one-size-fits-all approach to addiction treatment typically is a recipe for failure.57 Public Attitudes about Addiction Treatment Reflect the Prevailing Non-Medical Approach to Addiction Care CASA Columbia’s NABAS found that although the American public appears to be supportive of assuring that individuals with addiction receive effective addiction treatment, public views about what constitutes addiction treatment do not comport with the science: more than half (60.1 percent) of respondents to the NABAS spontaneously offered mutual support programs such as AA or NA as a “treatment” intervention when asked what kinds of treatment come to mind when they think about treatment for
addiction,58 despite the fact that such programs, while very helpful sources of support to many individuals with addiction, are not evidence-based treatments for the disease.59 The public also does not seem to distinguish between risky substance use and the disease of addiction. Most People in Need of Treatment Do Not Receive It As an indicator of the lack of attention afforded the disease of addiction, no single national data source exists to compare the proportion of the population in need of addiction treatment involving any addictive substance to the proportion that receives such treatment. While about seven out of 10 people with hypertension, major depression or diabetes get treatment for their medical conditions, only about one in 10 people with addiction involving alcohol or drugs other than nicotine do,* 60 (Figure 1.B), leaving a treatment gap of 20.7 million individuals.61 No data exist on the treatment gap for those with addiction involving nicotine. The proportion of individuals in need of addiction treatment involving alcohol and drugs other than nicotine who actually receive it has changed little since 2002, when 9.8 percent of those in need received treatment.62
* For this comparison, CASA Columbia examined the referenced national survey data to determine the proportion of the population with each disease--those with diagnosed or undiagnosed hypertension (59.3 million); those with diagnosed or undiagnosed diabetes (25.8 million); those who met clinical criteria for a major depressive episode in the past year and/or received professional treatment (saw a doctor, received medication, a combination thereof) (22.4 million); and those who met clinical criteria for addiction involving alcohol or other drugs excluding nicotine in the past year and/or received professional treatment for alcohol and/or other drugs in the past year (23.2 million)--who received treatment.
-
-11-
0.6
1.4
5.7
10.6
12.1
25.3
44.3
Employers
Schools
Health Care Providers
Addiction Treatment Providers
Community Sources
Individuals
Criminal Justice System
* Excluding nicotine.Source: CASA Columbia analysis of The Treatment Episode Data Set (TEDS), 2009.
PERCENT
Figure 1.C Sources of Referral to Publicly-Funded
Addiction* Treatment
77.2 73.2 71.2
10.9
Hypertension¹ Diabetes² MajorDepression³
Addiction³(excludingNicotine*)
PERCENT
Figure 1.B Individuals with Select Medical Conditions
Who Receive Treatment
1 Ages 18 and older; Ostchega, Y., Yoon, S.S., Hughes, J. & Louis, T. (2008).2 All ages; Centers for Disease Control and Prevention. (2011).3 Ages 12 and older; CASA Columbia analysis of The National Survey on Drug Use and Health (NSDUH), 2010* Due to data limitations.
Most Referrals to Publicly Funded Treatment Come from the Criminal Justice System CASA Columbia’s national survey conducted for this study found that 46.8 percent of respondents would turn to a health professional--such as their physician (27.8 percent), a health professional other than their primary care physician (19.7 percent) or a mental health professional (9.2 percent)*--if someone close to them needed help for addiction.63 However, only 5.7 percent of referrals to publicly funded treatment came from a health care provider. In contrast, a full 44.3 percent of the referrals to treatment were from the criminal justice system,64 highlighting the fact that this disease typically is addressed only at the point at which it results in profound social consequences. One-quarter (25.3 percent) of referrals came from individuals, including concerned family members, friends and the self-referred; 12.1 percent were referred by community sources such as social welfare organizations, religious organizations and mutual support programs; and 10.6 percent were referred by addiction treatment providers for additional treatment. Very few treatment referrals came from schools (1.4 percent) or from employers (0.6 percent).65 (Figure 1.C)
* Some respondents chose more than one response, so the 46.8 percent reflects those who chose either one of these health professionals.
-
-12-
Less than Half of Treatment Admissions Result in Treatment Completion In 2008,* less than half (42.1 percent) of discharges from formal addiction treatment services were of admissions in which treatment was completed.66 The highest completion rates were from venues to which there were the fewest admissions: 14.8 percent of admissions were to short-
term residential services which had the highest completion rate of 54.8 percent;
11.4 percent of admissions were to longer-
term residential treatment which had a completion rate of 45.5 percent; and
73.8 percent of admissions were to non-
residential services which had the lowest completion rate of 39.1 percent.67
No data are available on the extent to which referrals were based on matching providers with individual treatment needs. Patients Face Formidable Barriers to Receiving Addiction Treatment In addition to the lack of treatment referrals from the health care system, many other barriers stand in the way of individuals accessing and completing addiction treatment. These include: a misunderstanding of the disease, negative public attitudes and behavior toward those with the disease, privacy concerns, insufficient insurance coverage of the costs of treatment, lack of information on how to get help, limited availability of services including a lack of addiction physician specialists, insufficient social support, conflicting time commitments, negative perceptions of the treatment process and legal barriers. Rarely is there only one obstacle to a person receiving needed treatment.68 Although comparable national data for barriers to accessing smoking cessation treatment are not available, research indicates that barriers similar to those facing individuals
* Most recent available data on discharges.
seeking treatment for addiction involving alcohol or other drugs stand in the way of smokers accessing tobacco cessation services.69 The Spending Gap In 2010, the United States spent $43.8 billion to treat diabetes70 which affects 25.8 million people,71 $86.6 billion to treat cancer72 which affects 19.4 million people73 and an estimated $107.0 billion to treat heart conditions74 which affect 27.0 million people,75 but only $28.0 billion to treat addiction† which affects 40.3 million people.‡ 76 Looking just at government spending, CASA Columbia calculated that in 2005, risky substance use- and addiction-related spending accounted for 10.7 percent of federal, state and local spending, and that for every dollar federal and state governments spent, 95.6 cents went to pay for the consequences of substance use; only 1.9 cents was spent on any type of prevention or treatment.§ The taxpayer tab for government spending on the consequences of risky substance use and addiction alone totals almost $1,500 a y