Addiction Medicine: Closing the Gap between Science and Practice
56
A Report by CASAColumbia ® October 17, 2012 ADDICTION MEDICINE: CLOSING THE GAP BETWEEN SCIENCE AND PRACTICE
-
Upload
casacolumbia -
Category
Health & Medicine
-
view
16.989 -
download
1
description
These slides accompany CASAColumbia's report, Addiction Medicine: Closing the Gap between Science and Practice, published in June 2012, which found that, despite the prevalence of addiction, the enormity of its consequences, the availability of effective solutions and the evidence that addiction is a disease, both screening and early intervention for risky substance use are rare, and only about 1 in 10 people with addiction involving alcohol or drugs other than nicotine receive any form of treatment.
Transcript of Addiction Medicine: Closing the Gap between Science and Practice

© CASAColumbia 2013
A Report by
CASAColumbia®
October 17, 2012
ADDICTION MEDICINE:
CLOSING THE GAP
BETWEEN SCIENCE AND
PRACTICE

© CASAColumbia 2013
Drew E. Altman, PhD (Chair) President and Chief Executive Officer,
The Henry J. Kaiser Family Foundation
Harvey V. Fineberg, MD, PhD President, Institute of Medicine
Mark S. Gold, MD University of Florida College of Medicine and
McKnight Brain Institute
Departments of Psychiatry, Neuroscience, Anesthesiology,
Community Health & Family Medicine
Chairman, Department of Psychiatry
Shelly F. Greenfield, MD, MPH Chief Academic Officer, McLean Hospital
Professor of Psychiatry, Harvard Medical School
Director, Clinical and Health Services Research and Education
Division on Alcohol and Drug Abuse, McLean Hospital
Elizabeth R. Kabler President, Rosenstiel Foundation
Myles V. Lynk, JD Peter Kiewit Foundation, Professor of Law and the
Legal Profession; Faculty Fellow, Center for Law, Science &
Innovation’s Program in Public Health Law and Policy
University, Sandra Day O’Connor College of Law
Arizona State University
2
June E. Osborn, MD President Emerita, Josiah Macy, Jr. Foundation
Manuel T. Pacheco, PhD President Emeritus, University of Arizona
and University of Missouri System
The Honorable Jose R. Rodriguez Circuit Judge, Ninth Judicial Circuit of Florida
Reverend Msgr. Stephen J. Rossetti, PhD, DMin Clinical Associate Professor
Associate Dean for Seminary and Ministerial Programs
The Catholic University of America, The School of Theology and Religious
Studies
Former President and Chief Executive Officer
Saint Luke Institute, Inc.
Leonard D. Schaeffer Judge Robert Maclay Widney
Chair & Professor
University of Southern California
Steven A. Schroeder, MD Distinguished Professor of Health and Health Care, Department of Medicine
Director, Smoking Cessation Leadership Center
University of California, San Francisco
Louis W. Sullivan, MD President Emeritus, Morehouse School of Medicine
National Advisory Commission
on Addiction Treatment

© CASAColumbia 2013
Funders
• The Annenberg Foundation
• The Diana, Princess of Wales Memorial Fund and The Franklin Mint
• The New York Community Trust
• Adrian and Jessie Archbold Charitable Trust
3

© CASAColumbia 2013
Methodology
• Review of more than 7,000 scientific articles, reports, books
• Secondary analysis of 5 national data sets
• 176 key informants
• Focus groups/national population survey of attitudes and beliefs of
1,303 adults
• New York State surveys
83 treatment program directors
141 staff treatment providers
4

© CASAColumbia 2013
Methodology (continued)
• National panel of treatment providers/online survey of 1,142
members of professional associations involved in addiction care
• Online survey of 360 individuals with history of addiction who are
managing the disease
• In-depth analysis of state/federal governments’ and professional
associations’ licensing and certification requirements for treatment
providers, facilities and programs; accreditation requirements for
facilities and programs
• Case study of addiction treatment in New York State and New York
City
5

© CASAColumbia 2013
…addiction is not about drugs, it’s about brains. It is not the
substances a person uses that make them an addict; it is not even the
quantity or frequency of use. Addiction is about what happens in a
person’s brain when they are exposed to rewarding substances or
rewarding behaviors, and it is more about reward circuitry in the brain
and related brain structures than it is about the external chemicals or
behavior that “turn on” that reward circuitry.
--American Society of Addiction Medicine. (2011).
Definition of addiction: Frequently asked questions
6

© CASAColumbia 2013
Language Matters
Terms used to describe different levels of involvement with addictive
substances – experimentation, use, misuse, excessive use, abuse,
dependence:
• Lack precision
• Obscure important differences in nature and severity of illness
• Complicate ability to intervene and treat
7

© CASAColumbia 2013
Addiction Is a
Complex Brain Disease
• Nicotine, alcohol, controlled illicit drugs and prescription drugs all
affect pleasure and reward circuitry of brain in similar ways
• Continued use can physically alter structure and function of brain
• Significant behavioral characteristics, including compulsion to obtain
and use addictive substance even in the face of negative
consequences
8

© CASAColumbia 2013
Risky Use of
Addictive Substances
• Risky users are those who:
Currently use tobacco products
Exceed the USDA Dietary Guidelines for safe alcohol use
Misuse controlled prescription drugs
Use illicit drugs
Engage in some combination of the above
But do not meet the clinical criteria for addiction
• Risky use can result in devastating and costly health and social
consequences, including the disease of addiction
9
A Public Health Problem

© CASAColumbia 2013
How Big is the Problem?
• 15.9% (40.3 million) have the
disease of addiction – more than
have heart conditions (27.0
million), diabetes (25.8 million) or
cancer (19.4 million)
• 31.7% (80.4 million), while not
addicted, engage in use of
addictive substances in ways
that threaten health and safety
(risky users)
10

© CASAColumbia 2013
The Consequences
Are Enormous
Risky substance use and addiction:
• Account for 32.3% of all hospital inpatient costs
• Result in more than 20% of deaths
• Are causal and contributing factors in more than 70 other conditions
requiring medical care
• Drive a wide range of other costly social consequences
11

© CASAColumbia 2013
The Spending Gap
• In 2010, the U.S. spent:
$43.8 billion to treat diabetes (affecting 25.8 million)
$86.6 billion to treat cancer (affecting 19.4 million)
$107.0 billion to treat heart conditions (affecting 27.0 million)
$28.0 billion to treat addiction (affecting 40.3 million)
• 95.6 cents of every dollar spent by federal and state governments
on risky substance use and addiction go to pay for the
consequences; only 1.9 cents go to prevention and treatment
12

© CASAColumbia 2013
Clear Risk Factors
• Genetic predisposition
• Structural/functional brain vulnerabilities
• Psychological and environmental influences
• Age of first use: 96.5% of cases of addiction start with substance
use before age 21 when brain is still developing
13

© CASAColumbia 2013
Multiple Substances
Frequently Involved
• Among risky substance users, 30.6% use more than one substance
• Among those who are addicted, 55.7% are risky users of one or
more other substances and 17.3% have addiction involving multiple
substances
14

© CASAColumbia 2013
As With Other
Health Conditions…
• Addiction frequently co-occurs with other health problems
• Addiction can be a chronic disease
• Individually-tailored interventions and treatments are required
• Addiction should be addressed within the medical system
15

© CASAColumbia 2013
Screening and Intervention
for Risky Use
• Effective tools available
• Can be used in a variety of settings
and populations
• Can reduce risky use and prevent
addiction
16

© CASAColumbia 2013
Effective Treatment
Options Exist
• Pharmaceutical therapies
To reduce cravings/withdrawal
symptoms
To reduce reward of addictive
substances
Maintenance
17
• Psychosocial therapies
Motivational
Cognitive behavioral
Community reinforcement
Contingency management
Behavioral/couples/family
• Combined therapies

© CASAColumbia 2013
Best Treatment
Practices Require
• Diagnostic evaluation
• Comprehensive assessment
• Stabilization
• Acute care
• Chronic disease management
• Ancillary services and peer support
18

© CASAColumbia 2013
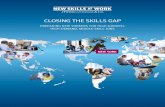
The Treatment Gap
19
77.2 72.9 71.2
10.9
Hypertension¹ Diabetes² Major Depression³ Addiction³(excluding
Nicotine*)
P
E
R
C
E
N
T
Individuals with Select Medical Conditions Who Receive Treatment
1 Ages 18 and older; Ostchega, Y., Yoon, S.S., Hughes, J. & Louis, T. (2008).2 All ages; Centers for Disease Control and Prevention. (2011).3 Ages 12 and older; CASA Columbia analysis of The National Survey on Drug Use and Health (NSDUH), 2010
* Due to data limitations.
No data exist on the treatment gap for those who are nicotine dependent.
Most People in Need of Treatment Do Not Receive It

© CASAColumbia 2013
Most Don’t Complete Treatment
The highest completion rates were from venues with the fewest
admissions:
• 14.8% of admissions were to short-term residential services
which had the highest completion rate of 54.8%
• 11.4% of admissions were to longer-term residential treatment
which had a completion rate of 45.5%
• 73.8% of admissions were to non-residential services which had
the lowest completion rate of 39.1%
20
Less Than Half (42.1%) of Treatment Admissions Result
in Treatment Completion

© CASAColumbia 2013
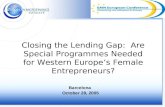
Treatment Referrals
21
0.6
1.4
5.7
10.6
12.1
25.3
44.3
Employers
Schools
Health Care Providers
Addiction Treatment Providers
Community Sources
Individuals
Criminal Justice System
P
E
R
C
E
N
T
Sources of Referral to Publicly-Funded Addiction Treatment (Excluding Nicotine)
Source: CASA Columbia analysis of The Treatment Episode Data Set (TEDS), 2009.
Most Referrals to Publicly-Funded Treatment Come
from the Criminal Justice System

© CASAColumbia 2013
Addiction Treatment Workforce
• Size of “treatment” workforce unknown
• Treatment providers include: physicians, physician assistants,
nurses, psychologists, mental health counselors and therapists,
social workers, acupuncturists and addiction counselors
22

© CASAColumbia 2013
Few Medical Professionals
Treat Addiction
• Little education required in addiction science, prevention and
treatment:
Separate courses in addiction medicine rarely taught in medical school
Required addiction-related content on board exams is minimal and often
identified only as possible sub-topics
• Of 985,375 active physicians, there are only about 1,200 practicing
addiction medicine specialists and 355 self-identified practicing
addiction psychiatrists
23

© CASAColumbia 2013
Treatment Providers Usually
Addiction Counselors No Medical Training Required
• 14 states: do not require all addiction counselors to be licensed or
certified
• 6 states: no minimum degree requirements
• 14 states: minimum requirement of high school degree or GED
• 10 states: minimum requirement of associate’s degree
• 6 states: minimum requirement of bachelor’s degree
• 1 state: minimum requirement of master’s degree
24

© CASAColumbia 2013
Regulatory Requirements
• Addiction treatment facilities and programs are not adequately
regulated or held accountable for providing treatment consistent with
medical standards and proven treatment practices
• Only 10 states require residential treatment programs to have a
physician either as medical director or on staff; 8 states require the
same of outpatient treatment programs
• Most regulators define medical care as detoxification, opioid
replacement therapy or treatment of co-occurring disorders only
25
Do Not Recognize Addiction Treatment as Medical Care

© CASAColumbia 2013
Addiction Care
• No national standards for who may provide addiction treatment in
the U.S.; varies by state and payer
• No other disease where appropriate medical treatment is available
is as neglected by the health care system
• Patients must turn to a broad range of practitioners largely exempt
from medical standards
26
Largely Disconnected from Mainstream Medical Practice

© CASAColumbia 2013
Where is the Medical
Profession?
• 1956 – AMA declared alcoholism an illness that can and should
be treated within the medical profession
• 1989 – AMA adopted a policy declaring addiction involving other
drugs, including nicotine, to be a disease
• 47% of Americans would turn to a health professional if someone
close to them needed help for addiction
• Yet < 6% of referrals to publically-funded addiction treatment
come from a health care provider
27

© CASAColumbia 2013
Public-Private Spending
for Treatment Most Funding for Addiction Treatment Comes
from Public Sources
• Private payers (including private insurers and self-payers)
responsible for:
55.6% ($1.4 trillion) of medical expenditures in the U.S.
But only 20.8% ($5.8 billion) of addiction treatment spending
• Public spending concentrated in non-residential services operated
outside of mainstream health care
28

© CASAColumbia 2013
Public Attitudes about Addiction
CASAColumbia’s NABAS survey found that:
• The public does not recognize the role of genetics and biological
factors in the development of addiction
• 60% of respondents identify mutual support programs as a
“treatment” intervention
• Public perceptions do not distinguish between risky substance
use and the disease of addiction
29
Out of Sync with Science

© CASAColumbia 2013
Formidable Barriers to
Receiving Treatment Patients Face Obstacles to Addiction Treatment Due To:
30
• A misunderstanding of the disease
• Negative public attitudes and
behavior toward those with the
disease
• Privacy concerns
• Insufficient insurance coverage for
treatment
• Lack of information on how to get
help
• Limited availability of services
including a lack of addiction
physician specialists
• Insufficient social support
• Negative perceptions of the
treatment process
• Legal barriers

© CASAColumbia 2013
IT IS TIME FOR HEALTH CARE
PRACTICE TO CATCH UP WITH THE
SCIENCE
31

© CASAColumbia 2013
Recommendations
and Next Steps
• Reform health care practice
• Use leverage of public policy to speed reform
32

© CASAColumbia 2013
Reform Health
Care Practice
• Incorporate into routine medical practice screening and intervention
for risky substance use, and diagnosis, treatment and disease
management for addiction
• Incorporate screening and intervention for risky substance use into
routine practice for non-physician health professionals (physician
assistants, nurses, dentists, pharmacists, graduate-level clinical
psychologists, social workers, counselors)
33

© CASAColumbia 2013
Reform Health
Care Practice
• Develop core clinical competencies for physicians and for non-
physician health professionals in addressing risky substance use
and preventing and treating addiction
• Assure that core clinical competencies and specialized training are
required components of all:
Medical school curricula, residency training programs, licensing
exams, board certification exams and continuing medical
education (CME) requirements, including maintenance of
certification programs
Professional health care program curricula, graduate fellowship
training programs, professional licensing exams and continuing
education (CE) requirements
34

© CASAColumbia 2013
Reform Health
Care Practice
• Develop improved screening and assessment instruments
• Establish national accreditation standards for all addiction treatment
facilities and programs that reflect evidence-based care
Professional staffing: full time certified addiction physician specialist
and professional staff trained in core competencies
Intervention and treatment services: comprehensive assessment and
tailored, evidence-based treatment for addiction involving all
substances
Quality assurance: process and outcome measurements
35

© CASAColumbia 2013
Reform Health
Care Practice
• Standardize language used to describe the full spectrum of
substance use and addiction
36

© CASAColumbia 2013
Public Policy Leverage
to Speed Reform
• Condition government grants and contracts for addiction services on
provision of quality care
• Educate non-health government workers who come into contact with
significant numbers of individuals who engage in risky substance use
or who may have addiction about evidence-based practices
• Identify patients at risk in government programs and services where
costs of risky use and addiction are high and provide appropriate care
• Develop tools, practice guidelines and outcome measures to improve
quality of service delivery
• License addiction treatment facilities as health care providers
37

© CASAColumbia 2013
Public Policy Leverage
to Speed Reform
• Require adherence to national accreditation standards that reflect
evidence-based care
• Require that all insurers provide comprehensive coverage for
screening, intervention, diagnosis, treatment and disease
management for addiction, including specialty care
• Expand the addiction medicine workforce
• Implement a national public health campaign to educate the public
about all forms of risky substance use and addiction
• Invest in research and data collection to improve and track progress
and search for a cure
38

© CASAColumbia 2013
Ending Addiction
Changes Everything
www.casacolumbia.org

© CASAColumbia 2013
Speaker Notes Slide 6: • Addiction is a complex primary disease of the brains circuitry related to reward, motivation and
memory,
• Reflected in pathological pursuit of reward or relief by substance use and other behaviors.
• Not limited to the rewards provided by nicotine, alcohol and other drugs but extends to other
rewarding behaviors such as gambling, compulsive overeating, and sexual behaviors. • We tend to talk about addiction as if there are multiple diseases; in fact there are different
manifestations of one disease and those manifestations often co-exist or vary with circumstances. • Due to data limitations, this study focuses on addiction involving nicotine, alcohol and other drugs.
Slide 7: • There are many terms used to describe different levels of involvement with addictive substances
such as: experimentation, misuse, excessive use, abuse, dependence.
• This imprecision in our language:
• Obscures important differences in the nature and severity of illness
• And complicates our ability to intervene and treat effectively.
• Even the term “treatment” lacks precision with regard to addiction, since historically it has been
used to refer to a host of interventions, many of which are not based in the clinical and scientific
evidence as are treatments for other diseases.
40

© CASAColumbia 2013
Speaker Notes Slide 8: • This is consistent with the revisions recently published in the DSM-V for substance use disorders.
• All of these substances affect the brain’s reward circuitry in similar ways.
• Continued use can change both the structure and function of the brain.
• There also can be pre-existing structural and functional differences in the brain predisposing one
to the disease.
Slide 9: • It is essential to distinguish the disease of addiction from the public health problem of risky use of
addictive substances that does not meet the threshold for addiction.
• Risky users are those who do not meet clinical criteria for addiction but use addictive substances
in ways that threaten health and safety, including:
• Any tobacco/nicotine use
• Drinking in excess of the USDA dietary guidelines, and
• Any illicit drug use or misuse of controlled prescription drugs.
41

© CASAColumbia 2013
Speaker Notes Slide 10: • Risky substance use and addiction together constitute America’s largest health problem.
• About 16% of the U.S. population age 12 and over--40 million people--have addiction involving
nicotine, alcohol or other drugs:
• That is more than the number with heart conditions, diabetes or cancer
• Probably an undercount because, due to data limitations, we are only counting those who report
meeting behavioral criteria and not those who have the disease but who are managing it
effectively or who may not have yet displayed behavioral symptoms
• Nor does it include the institutionalized population.
• The population of risky users is double that size--about 80 million people.
Slide 11: • It also is our most costly health problem.
• For example, approximately 1/3 of all hospital inpatient costs are a result of risky substance use
and addiction.
• It accounts for at least 1/5 of all deaths and drives more than 70 other diseases requiring medical
attention
• And it is a major factor in a broad and devastating range of other health and social consequences
including:
• Motor vehicle crashes
• Homelessness, domestic violence
• Child abuse and neglect, a host of property and violent crimes.
42

© CASAColumbia 2013
Speaker Notes Slide 12: • Instead of paying for effective prevention and treatment services, we pay to cope with the
consequences.
• The tragedy is that less than 2 cents of every $1 federal and state governments spend on this
problem go to prevention or treatment
• While 96 cents go to cope with the consequences of our failure to prevent and treat it.
• This approach costs every person in America approximately $1500 every year.
Slide 13: • Like other diseases, there are clear risk factors for both risky use and addiction.
• Between 50-75% of the risk of moving from use to addiction appears to be governed by a range of
genetic factors.
• There also are significant influences exerted by:
• The families we grow up in
• Our peers and our communities
• Prescribing practices of health professionals
• And by advertising and media practices.
• Of critical importance is the age of first use of addictive substances.
• Addiction is, in most cases, a developmental disorder associated with the early use of addictive
substances while the brain is still developing.
43

© CASAColumbia 2013
Speaker Notes Slide 14: • People often display multiple manifestations of risky use.
• It makes no sense to only screen for risky use or treat addiction involving 1 or 2 substances. We
must address all--including nicotine.
Slide 15: • As with other health conditions:
• Addiction frequently co-occurs with other health problems that also must be addressed.
• It can become a chronic disease and require long-term management.
• A one size fits all approach to treatment does not work.
• Like other diseases, addiction requires medical attention.
• Like treatment for other diseases, proven pharmaceutical and specific behavioral treatments must
be provided in accordance with established treatment protocols and integrated into treatment for
other health conditions.
44

© CASAColumbia 2013
Speaker Notes Slide 16: • For risky use, there are effective and tested tools available to screen for this public health problem
• And provide brief interventions as needed.
• They can be used in a variety of settings with different populations.
• Training in the administration of screening and interventions is critical.
• We must screen for all substances and ideally for other risky behaviors.
• We must better calibrate our screening instruments to appropriate definitions of risky use.
Slide 17: • Similarly, a range of treatments have proven efficacy, including:
• Different types of pharmaceutical therapies, and
• Multiple psychosocial therapies.
• In many cases, best results are achieved by a combination of these therapies.
• Again, these treatments must be tailored to the needs of individual patients.
45

© CASAColumbia 2013
Speaker Notes Slide 18: • The elements of best practice in addiction treatment are:
1. A diagnostic evaluation to determine the presence of the disease.
2. If the disease is present, a comprehensive assessment of the stage and severity of disease, co-occurring
conditions, and personal circumstances that may affect the treatment.
3. The patient must be stabilized. This means managing cessation of use. Sometimes this can be achieved
with guidance, monitoring and social support, but other times pharmaceutical therapies and/or
hospitalization is required.
4. Then there is the acute phase of treatment, involving pharmaceutical, psychosocial or combined therapies
and treatment for co-occurring conditions that may be offered in a range of office based, outpatient or
inpatient settings, again depending on need.
5. Disease management is critical because as yet there is no cure for addiction.
6. Throughout the process, peer support and ancillary services can be deciding factors in the success of
treatment and disease management.
46

© CASAColumbia 2013
Speaker Notes Slide 19: • Only about 11% of those with the disease involving alcohol and drugs other than nicotine receive
any form of treatment at all.
• In this country, we don’t even know the number of people who receive treatment for addiction
involving nicotine.
• Compare that 11% with the 70-80% of people with other diseases like major depression, diabetes
and hypertension who do receive care.
• And of that 11% who receive some form of care, we also know that most do not receive anything
that approximates evidence-base services.
47

© CASAColumbia 2013
Speaker Notes Slide 20: • Of those who do receive some form of treatment, less than ½ actually complete the treatment
process recommended.
• The highest rates of completion were from treatment venues to which there were the least
referrals.
Slide 21: • Most referrals to treatment come from the criminal justice system--
• Illustrating how we fail to prevent and treat until a crisis occurs.
48

© CASAColumbia 2013
Speaker Notes Slide 22: • Unlike other health conditions, we have no reliable estimate of who is providing addiction
treatment.
• CASAColumbia identified a range of providers (listed), but there are others offering ‘treatment’ that
are even outside this wide range,
• Including religious-based providers and simply entrepreneurs.
Slide 23: • Unlike other diseases, most medical professionals who should be providing treatment are not
sufficiently trained to do so.
• Physicians and other medical professionals make up the smallest share of providers of addiction
treatment.
• Thanks to the work of the American Board of Addiction Medicine, there are efforts underway to
expand capacity, but the gap remains staggering.
49

© CASAColumbia 2013
Speaker Notes Slide 24: • Most of those currently providing treatment for this disease are not medical professionals and are
not equipped with the knowledge, skills or credentials necessary to provide the full range of
evidence-based health care services.
• The largest group providing addiction treatment is the addiction counselors and
• In most states their minimum degree requirements are a GED or high school diploma.
• 14 states do not even require all addiction counselors to be licensed or certified.
• There simply are no national standards for who may provide addiction treatment in the U.S.
Slide 25: • Regulatory requirements for treatment providers vary dramatically by state and by payor.
• For the most part, providers are not required to be regulated as medical providers.
• Even if physicians are required to be on staff of treatment programs, they frequently are on call for
other ‘health problems’ and not to treat addiction.
• In fact, most regulators exclude addiction treatment from their definition of medical care--with the
exception of providing opioid replacement therapy which is not universally available.
• While about 30 states require a clinical or program director to oversee services, only 8 states
require a minimum of a master’s degree for the position--there is no medical degree requirement.
50

© CASAColumbia 2013
Speaker Notes Slide 26: • Much of what passes for “treatment” bears little resemblance to the treatment offered for other
health conditions, and much of what is offered in addiction “rehabilitation” programs has not been
subject to rigorous scientific study.
• This is inexcusable given decades of accumulated scientific evidence attesting to the fact that
addiction is a brain disease for which there are effective interventions and treatments.
• It also is unfair to the thousands of addiction counselors who struggle, in the face of extreme
resource limitations and no medical training, to provide help to patients with the disease of
addiction and numerous co-occurring medical conditions.
Slide 27: • This profound gap between the science of addiction and current practice is a result of decades of
marginalizing addiction as a social problem rather than treating it as a medical condition.
51

© CASAColumbia 2013
Speaker Notes Slide 28: • This gap between science and practice also is reflected in how we pay for treatment,
• With a concentration of public resources linked to the health and social problems that result from
our failure to prevent and treat the disease
• And in services operating outside of mainstream health care.
Slide 29: • Many outmoded attitudes about addiction reside in the public consciousness, although these
attitudes are changing.
• Recent surveys suggest that about 80% of Americans now recognize addiction as a disease,
• But, as you see here, they lack critical information to understand it.
52

© CASAColumbia 2013
Speaker Notes Slide 30: • What all this means for patients and their families is that they face enormous barriers in gaining
access to effective care
• Including how and where to get help
• And what help should entail.
Slide 31: • It is long past time for health care practice related to risky use and addiction to catch up with the
science.
• Failure to do so causes untold human suffering
• And it is a profligate waste of scarce taxpayer dollars.
53

© CASAColumbia 2013
Speaker Notes Slide 32: • Our full report has a wide range of recommendations to accomplish this transition.
Slide 33: • We must incorporate screening, intervention, diagnosis, treatment and disease management into
routine health care practice--in a sustainable way.
• Including both medical providers and the appropriate array of other health professionals.
• Backed by specialty care addiction physicians (addiction medicine physicians and addiction
psychiatrists).
• The team approach is the future of health care practice, but each team member must be highly
trained.
54

© CASAColumbia 2013
Speaker Notes Slide 34: • To assure appropriate training, we need to develop core clinical competencies for physicians
• And for the range of non-physician health professionals working as part of the team.
• And we need to assure that those clinical competencies are required components of the relevant:
• Educational curricula
• Residency and fellowship training programs
• Licensing and certification exams
• And continuing education requirements.
Slide 35: • We need to align our screening, assessment and diagnostic instruments with the science and with
definitions of risky use and addiction.
• We must establish national accreditation standards for addiction treatment facilities and programs
that reflect evidence-based care.
• We need to standardize our language as it relates to these health conditions and their prevention
and treatment.
55

© CASAColumbia 2013
Speaker Notes Slide 37: • The levers of public policy can be employed to speed this change.
• Examples include:
• Assuring appropriate screening, intervention and treatment for patients in government funded
programs where costs of not doing so are high--health care and justice
• Requiring that all addiction treatment facilities and programs be licensed as health care
providers
Slide 38: • Requiring adherence to national accreditation standards reflecting evidence-based care.
• Requiring expanded and comprehensive insurance coverage
• Jump-starting the addiction medicine workforce
• Implementing a national public health campaign to educate the public about:
• This disease
• Its risk factors
• What they can to prevent it, and
• When and where to get help.
• Developing ways to better measure outcomes and track progress
56