adderall presentation
29
Biopsychology Instructor- Janna Keefe Adam Schwartz
-
Upload
adam-schwartz -
Category
Documents
-
view
79 -
download
0
Transcript of adderall presentation

Biopsychology
Instructor- Janna Keefe
Adam Schwartz

Adderall IR (instant release)
Adderall XR (extended release)
Dextroamphetamine Saccharate, Amphetamine Aspartate, Dextroamphetamine Sulfate and Amphetamine Sulfate
Brand Names
Generic Name
Whether brand name or generic, this organic compound is a Psychostimulant½ Comprised of Amphetamine salts, and ½ Comprised of Dextroamphetamine salts.
These two stereoisomers (or optical isomers) combine to constitute a racemic mixture.

Carbon
Hydrogen
Nitrogen
Propan(Chain of 3 Carbons)
1-Phenyl (Benzene Ring)
-2 Amine(NitrogenAttached to 2nd Carbon)
1-phenylpropan-2-amine & 2S-phenylpropan-2-amine

To understand stereoisomers, think of any complimentary pair of gloves. They are mirror images of each other yet cannot be supper-imposed over each Other. Amphetamine is the, “right -hand glove,” and Dextroamphetamine isThe, “left-hand glove,” They do the same thing but must be differentiated by Organic Chemists for this difference.

“RIGHT-HANDED” STERIOISOMER
“LEFT –HANDED” STERIOISOMER
Amphetamine Dextroamphetamine
When synthesized in a laboratory there is an equal chance of producing either stereoisomer or enantiomer. Leaving them equally present as a racemic mixture influences the bodies ability to absorb, metabolize, and eliminate the drug.
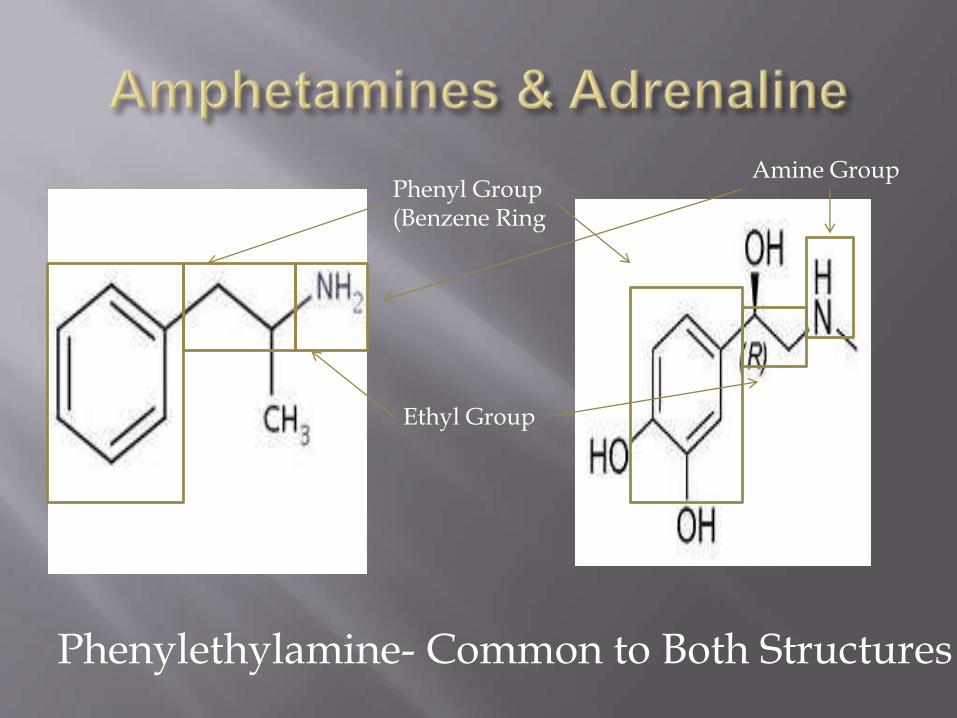
Phenyl Group(Benzene Ring
Ethyl Group
Amine Group
Phenylethylamine- Common to Both Structures

Dopamine-Catecholamine
Neurotransmitter that helps to regulate emotion and to reinforce reward-pathways. Acts on the sympathetic nervous system to stimulate heart rate and blood pressure.
Serotonin-Monoamine
Neurotransmitter derived from the amino acid tryptophan. Found mainly in the gastrointestinal tract and the central nervous system and contributes to well-being, feelings of happiness and the regulation of both appetite, and sleep.
Norepinephrine-Catecholamine Neurotransmitter released from sympathetic neurons. Increases heart rate, rate of glucose release, and blood flow. Synthesized from Dopamine and released into the blood stream where it acts on the Central Nervous System and the Sympathetic Nervous System.
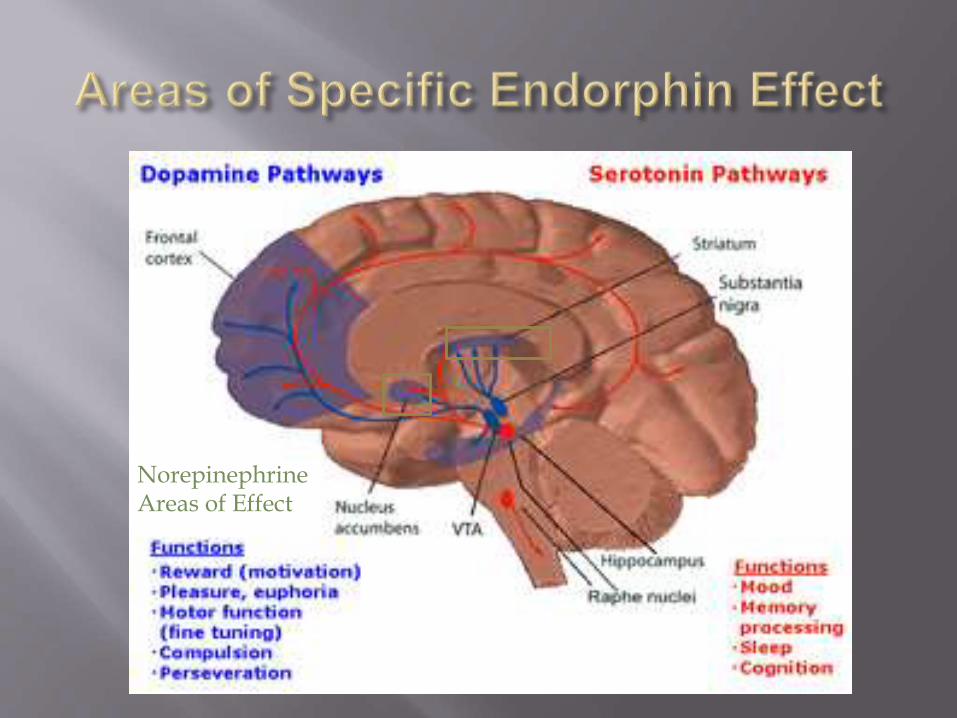
NorepinephrineAreas of Effect

Caudate Nucleus + Lenticular Nucleus = Striatum
Nucleus Accumbens
Hippocampus
Frontal Cortex
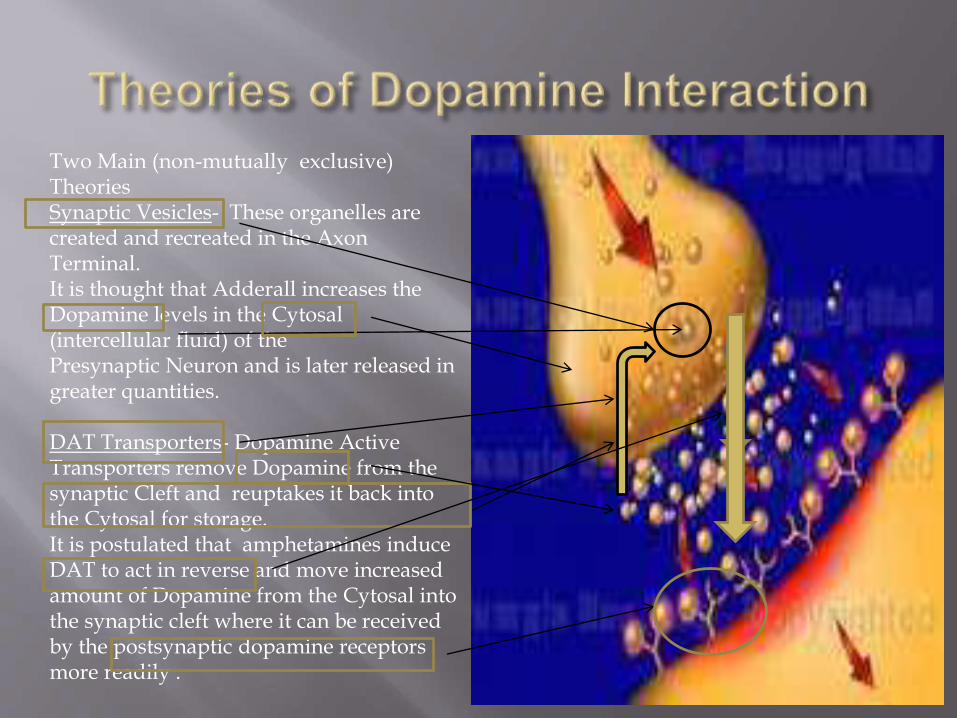
Two Main (non-mutually exclusive) TheoriesSynaptic Vesicles- These organelles are created and recreated in the Axon Terminal.It is thought that Adderall increases the Dopamine levels in the Cytosal(intercellular fluid) of the Presynaptic Neuron and is later released in greater quantities.
DAT Transporters- Dopamine Active Transporters remove Dopamine from the synaptic Cleft and reuptakes it back into the Cytosal for storage. It is postulated that amphetamines induce DAT to act in reverse and move increased amount of Dopamine from the Cytosal into the synaptic cleft where it can be received by the postsynaptic dopamine receptors more readily .

Serotonin Transporters (SERT)Seem to operate much like DAT. With the introduction of amphetamines an increased inhibitory response on SERT is seen affectingpathways associated with neural excitability. This may have implications for changes in locomotorstimulation seen in response to Amphetamines. So Amphetamines act in a way Similar to SSRI’s , leaving more Serotonin in the synaptic cleft to be taken up by Serotonin receptors in the postsynaptic Neuron. This increase increases Feelings of well-being, inhibits appetite, and disrupts sleep patterns.

Amphetamines also block the reuptake of Norepinephrine and interfere with the Norepinephrine Neural transport carrierResulting in increased concentrations being received by the postsynaptic neural receptors and in increased levels of Norepinephrine in the Brain and in the blood. This induces the Autonomic Nervous system to increase the heart rate and burning of glucose.
First Synthesized by Lazar Edeleanu in 1887 from Ma-Huang plant (Ephedra)
In 1927 a pharmacological use was first established for the compound as a synthetic form of ephedrine.
In early 1930’s was marketed as a decongestant under the trade name Benzedrine.
M.H. Nathanson conducted a subjective study on the effects of Amphetamines in 55 hospital workers in L.A. They reported well-being and decreased fatigue.

Used widely in WWII to decrease battle fatigue and increase alertness of soldiers.
After the emergence of significant abuse the FDA banned Benzedrine inhalers and mandated prescriptions to obtain Amphetamines.
The FDA classified Amphetamines as a schedule II drug as part of The controlled substance act of 1971.
By prescription to treat Attention-Deficit/Hyper-Active Disorder
By prescription to treat Narcolepsy
Occasionally used by prescription (off-label) to treat depression or obesity.
Illicitly used as a cognitive and athletic performance enhancer amongst students and professionals athletes.
According to the DSM-IV-TR, five criteria must be present for a person to be diagnosed with ADHD
Persistent pattern of inattention and/or hyperactivity and impulsivity more frequent and severe than others of same age or developmental level
Symptoms present before age 7 Symptoms present in more than one setting Symptoms cause problems in social, academic, or
work settings Rule out other psychological disorders may be
causing symptoms
http://www.drc.uga.edu/disabilities/adhdsub.php

ADHD-INATTENTIVE TYPE
ADHD-HYPERACTIVE/IMPULSIVE TYPE
Six (or more) symptoms of inattention (but fewer than six symptoms of hyperactivity-impulsivity) have persisted for at least six months. Hyperactivity may still be a significant clinical feature in many such cases, whereas other cases are more purely inattentive.
Characteristics: Often fails to give close attention to details or makes
careless mistakes in schoolwork, work, or other activities
Often has difficulty sustaining attention in tasks or play activities
Often does not seem to listen when spoken to directly
Often does not follow through on instructions and fails to finish school work, chores, or duties in the workplace
Often has difficulty organizing tasks and activities Often avoids, dislikes, or is reluctant to engage in
tasks that require sustained mental effort Often loses things necessary for tasks or activities Is often easily distracted by extraneous stimuli Is often forgetful in daily activities
Six (or more) symptoms of hyperactivity-impulsivity (but fewer than six symptoms of inattention) have persisted for at least 6 months. According to the DSM-IV-TR inattention may often still be a significant clinical feature in such cases.
Characteristics (hyperactivity): Often fidgets with hands or feet or squirms in seat Often leaves seat in classroom or in other situations
in which remaining seated is expected Often runs about or climbs excessively in situations
in which it is inappropriate (in adolescents and adults, may be limited to subjective feelings or restlessness)
Often has difficulty playing or engaging in leisure activities quietly
Is often "on the go" or often acts if "driven by a motor"
Often talks excessively
Characteristics (impulsivity): Often blurts out answers before questions have been
completed Often has difficulty awaiting turn Often interrupts or intrudes on others
http://www.drc.uga.edu/disabilities/adhdsub.php

ADHD-
COMBINED TYPE
ADHD- NOT OTHERWISE SPECIFIED TYPE
Six (or more) symptoms of inattention have persisted for at least six months.
Six (or more) symptoms of hyperactivity-impulsivity have persisted for at least six months.
Rarely used Diagnostically
Used for people who generally conform to ADHD symptoms but don’t sufficiently meet all clinical criteria and/or present with an atypical mixture of symptoms.
May be a label given to a child experiencing learning or executive functioning problems.

Concentration Relativity Theory
Stimulants by relative comparison cause the external world to slow down and provoke a ,“focusing,” response. This is akin to the fight or flight response which allows organisms increased focus and an impression of time slowing.
Dopamine Regulation TheoryInhibited Dopamine function in the Frontal Lobe can lead to hyperactivity, impulsivity, and distraction. A healthy amount of Dopamine in the Frontal Lobe helps with attention, focus, And decision-making. Adderall Promotes a higher level of Dopamine through it’s effect on Dopamine Active Transporters and/or through increased Dopamine in the Synaptic
Vesicles.
Dopamine in The Frontal Lobe

Possible Counter
Indications for
Adderall.
Heart Problems
High blood Pressure
Bipolar disorder and Schizophrenia
A history of seizures or Epilepsy
Tourette’s Syndrome
Hyperthyroidism
Glaucoma
If you are pregnant, thinking of becoming pregnant, or breastfeeding.

Further Limitation and
Concerns About
Adderall
Is an addictive substance with a potential to be abused or cause the user to build tolerance.
Has the potential to cause a slight slowing of growth (which is usually later made up) in children.
May effect your ability to drive or operate heavy machine until you acclimate to it properly after 2 weeks.
Do not use if you have used Nardil, Parnate, or Marplanin the last two weeks.

Increased heart rate or Arrhythmia
High blood pressure
Tremors, ticks, or confusion
Shortness of Breath
Anxiety or nervousness
Seizures
Euphoria or dysphoria
Burning during urination
NorepinephrineRelated
Dopamine andSerotonin Related
Stimulants can cause dehydration
Usually occurs in stimulant abusers but does rarely present in patients taking a therapeutic does of stimulants such as Adderall.
Presents like organic psychosis with primary symptoms including hallucinations, delusions, disordered thinking and (rarely) catatonia.
An Australia study found an 18% occurrence of stimulant psychosis in amphetamine users (this includes amphetamine abusers) A Japanese study observed a 64% recovery rate within 10 ten day of onset, increasing to 82% after 30 days of stimulant cessation. 5-15% did not make a full recovery by the time the study was published.

Insomnia
Dry mouth
Fever
Restlessness or irritability
Loss of appetite and weight loss
Sexual (libido, impotence, trouble achieving orgasm)
Diarrhea, stomach pain, constipation, nausea, vomiting
Atomoxetine (Strattera) is a non-stimulant that has been approved by the FDA to treat ADHD.
Some drugs such as Bupropion (Wellbutrin) and antihypertensives such as Clonidine (Catapres) and Guanfacine(Tenex) have been shown to be efficacious for some ADHD symptomology.
Diet high in dietary fiber and low in processed sugars. Behavioral interventions involving parental psycho-education,
parenting skills, and child safety. Interactive Metronome Training- Involves rhythmic kinesthetic
movement to strengthen the motor training/timing deficit thought to be associated with ADHD.
Neurofeedback Training- Uses an EEG to train the client to increase arousal in certain frontal cortex regions by increasing beta brain waves while decreasing theta waves through the use of focused cognitive tasks.

PROPONENTS OPPONENTS
The overwhelming academic consensus is that ADHD is a real clinical disorder with genetic, environmental , and neurobiological components.
No real empirically supported behavioral therapy yet available for managing ADHD symptoms.
Untreated or ineffectively treated ADHD leads to poor school performance and difficulty in learning social skills.
At therapeutic levels, drugs like Adderall, consistently helps adults and children with concentration, impulse control, planning, and task completion and has not yet been correlated with increased propensity for chemical addiction later in life.
ADHD is over-diagnosed, misdiagnosed and possibly not a valid clinical condition.
There are non-stimulant medications and behavioral interventions that may show some promise.
There are few long term studies yet available to determine long term stimulant use effects in adults or growing children.
It has a potential for abuse and/or exacerbation of aggression, anxiety, and depression plus numerous uncomfortable and potentially dangerous side-effects

“ADHD is not a simple disorder to treat - and we must work to treat each individual, not just a diagnosis.”-Douglas Cowan Psy.D.
My own opinion regarding the use of amphetamine salts, specifically Adderall would mirror this sentiment. I think that careful and thorough evaluations are needed to ensure an accurate diagnoses which is not being confused with oppositional-defiance disorder or with developmental behavioral symptoms. Once a diagnoses is made medication such as Clonidine, Wellbutrin, and Strattera should be administered along with behavior interventions and monitored for efficaciousness before Adderall is considered. In cases where these measures involving non-addictive medications are found to be insufficient I believe that the carefully monitored use of low doses of Adderall and other amphetamine based drugs might be the difference between reaching normal academic and social milestones or an emerging pattern of anti-social behavior and developmental delays.

Sulzer D, Chen TK, Lau YY, Kristensen H, Rayport S, Ewing A (May 1995). "Amphetamine redistributes dopamine from synaptic vesicles to the cytosol and promotes reverse transport". J. Neurosci. 15 (5 Pt 2): 4102–8.
Del Arco A, González-Mora JL, Armas VR, Mora F (July 1999). "Amphetamine increases the extracellular concentration of glutamate in striatum of the awake rat: involvement of high affinity transporter mechanisms". Neuropharmacology 38 (7): 943–54.
Division of Student Affairs. Disability Resource Center. University of Georgia. Text-Only Version. 3/25/2013.
McKetin R, McLaren J, Lubman DI, Hides L. The prevalence of psychotic symptoms among methamphetamine users. Addiction 2006;101(10):1473–8.
Sato M, Numachi Y, Hamamura T. Relapse of paranoid psychotic state in methamphetamine model of schizophrenia. Schizophrenia Bulletin1992;18(1):115–22.
Drugs.com. Micromedex™ (updated Mar 12th, 2013), Cerner Multum™ (updated Mar 18th, 2013), Wolters Kluwer™ (updated Mar 6th, 2013). Electronic Text. 3/31/2013.
Rothman RB, Baumann MH (August 2006). "Balance between dopamine and serotonin release modulates behavioral effects of amphetamine-type drugs". Ann. N. Y. Acad. Sci. 1074: 245–60.
Sulzer, D.; Chen, T.; Lau, Y.; Kristensen, H.; Rayport, S.; Ewing, A. (1995). "Amphetamine redistributes dopamine from synaptic vesicles to the cytosol and promotes reverse transport". The Journal of neuroscience : the official journal of the Society for Neuroscience 15 (5 Pt 2): 4102–4108.
Jones S, Kauer JA (November 1999). "Amphetamine depresses excitatory synaptic transmission via serotonin receptors in the ventral tegmental area". J. Neurosci. 19 (22): 9780–7.
Sulzer D, Sonders MS, Poulsen NW, Galli A (April 2005). "Mechanisms of neurotransmitter release by amphetamines: a review". Prog. Neurobiol. 75 (6): 406–33