
Added value, decreased cost: The evolving role of the cytotechnologist for preliminary screening and...
4
Added Value, Decreased Cost: The Evolving Role of the Cytotechnologist for Preliminary Screening and Triage of Thyroid Aspirates Angelean L. Wotruba, B.S., C.T., A.S.C.P., 1 * Jimmie Stewart III, M.D., 2 Thomas Scheberl, B.S., S.C.T., A.S.C.P., 1 and Suzanne M. Selvaggi, M.D. 2 Immediate adequacy assessment for thyroid fine-needle aspirations (FNAs) is standard practice in many cytopathology laboratories. A pathologist is usually present for these time consuming assessments. The purpose of this 5 month study (January 2008–May 2008) was to show that cytotechnologists can accurately provide the majority of immediate adequacy assessments for thyroid FNAs, saving both time and money for pathologists, clinicians, and patients. The study consisted of 167 thyroid nodule FNAs performed in twice weekly thyroid FNA clinics. A comparison was made of the immediate assessments by five participating cytotechnologists and the prelimi- nary and final diagnoses by three pathologists. The cytotechnologist prepared the slides, assessed the air-dried Hema-Diff TM stained slides for adequacy, and the pathologist viewed the slides remotely via real-time video streaming. Results were recorded in an Excel spreadsheet. There was a discordance rate of 1.2% when compar- ing the cytotechnologist’s adequacy interpretation and the patholo- gist’s preliminary diagnosis; both clinically insignificant. By cyto- technologist assessment, 79.0% of the cases were benign and 6.6% were nondiagnostic. 14.4% of the cases were assessed as cellular nodule or neoplastic lesion; all requiring pathologist’s preliminary diagnosis. Utilizing a cytotechnologist to provide adequacy, instead of a pathologist, saved $464.10/case (2.38 passes/case) based on current gross technical and professional charges. On the basis of our findings, cytotechnologists can accurately provide immediate onsite adequacy assessments for thyroid nodule FNAs. Affording cytotechnologists the opportunity to preliminarily assess FNAs for adequacy also creates a new role in the laboratory. Furthermore, cost-savings are realized for patients and the health care system. Diagn. Cytopathol. 2011;39:896–899. ' 2010 Wiley Periodicals, Inc. Key Words: thyroid; fine-needle aspiration; cytotechnologist; adequacy assessment Cytopathologic diagnosis of fine-needle aspirations (FNAs) of the thyroid gland has become routine clinical management of thyroid nodules. 1 FNA is an accurate cost-effective method to diagnose nodules, and it has sig- nificantly reduced the number of unnecessary thyroid sur- geries. 1 FNA can determine the diagnosis of thyroid nod- ules with a sensitivity of between 65 and 98% and a spec- ificity of 72 and 100%. 1 Most nodules in the thyroid are benign (69%) with only a small percentage of nodules diagnosed as malignant (4%). 1 Nondiagnostic rates that vary from 2 to 21% 1 are related to the experience of the aspirator. 2 To reduce the nondiagnostic rate, immediate adequacy assessments/preliminary diagnoses have been used to determine when an adequate amount of material has been obtained. 2–7 This in turn saves health care dol- lars by avoiding repeat procedures. 8 Currently, a cytopa- thologic evaluation at the time of aspiration is standard practice in many cytopathology laboratories, particularly in academic medical centers. Some authors believe that any preliminary diagnosis or assessment should be performed by a pathologist. 8 This is difficult for many hospital laboratories in that it removes the pathologist from the laboratory for long periods of time. A reasonable alternative is to have a well-trained cytotech- nologist provide an immediate assessment with triage to a pathologist of any patient’s case that is cellular or has any other neoplastic features. Cytotechnologists are highly skilled individuals with extensive training in cellular mor- phology and are well suited to the task of providing on-site immediate assessments. Enabling cytotechnologists to rou- tinely provide immediate assessments affords the patholo- gist time to spend on other tasks, gives the cytotechnologist a new role in the laboratory, and is a cost saving. 1 Department of Cytopathology, University of Wisconsin Hospital and Clinics, Madison, Wisconsin 2 Department of Pathology and Laboratory Medicine, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin *Correspondence to: Angelean L. Wotruba, B.S., C.T., A.S.C.P., Cytopa- thology Laboratory/D4-259d, University of Wisconsin Hospital and Clinics, 600 Highland Avenue, Madison, WI 53792. E-mail: [email protected] Received 16 December 2009; Accepted 3 June 2010 DOI 10.1002/dc.21487 Published online 14 October 2010 in Wiley Online Library (wileyonlinelibrary.com). 896 Diagnostic Cytopathology, Vol 39, No 12 ' 2010 WILEY PERIODICALS, INC.
-
Upload
angelean-l-wotruba -
Category
Documents
-
view
212 -
download
0
Transcript of Added value, decreased cost: The evolving role of the cytotechnologist for preliminary screening and...

Added Value, Decreased Cost:The Evolving Role of the Cytotechnologistfor Preliminary Screening and Triage ofThyroid AspiratesAngelean L. Wotruba, B.S., C.T., A.S.C.P.,1* Jimmie Stewart III, M.D.,2
Thomas Scheberl, B.S., S.C.T., A.S.C.P.,1 and Suzanne M. Selvaggi, M.D.2
Immediate adequacy assessment for thyroid fine-needle aspirations(FNAs) is standard practice in many cytopathology laboratories. Apathologist is usually present for these time consuming assessments.The purpose of this 5 month study (January 2008–May 2008) wasto show that cytotechnologists can accurately provide the majorityof immediate adequacy assessments for thyroid FNAs, saving bothtime and money for pathologists, clinicians, and patients. The studyconsisted of 167 thyroid nodule FNAs performed in twice weeklythyroid FNA clinics. A comparison was made of the immediateassessments by five participating cytotechnologists and the prelimi-nary and final diagnoses by three pathologists. The cytotechnologistprepared the slides, assessed the air-dried Hema-DiffTM stainedslides for adequacy, and the pathologist viewed the slides remotelyvia real-time video streaming. Results were recorded in an Excelspreadsheet. There was a discordance rate of 1.2% when compar-ing the cytotechnologist’s adequacy interpretation and the patholo-gist’s preliminary diagnosis; both clinically insignificant. By cyto-technologist assessment, 79.0% of the cases were benign and 6.6%were nondiagnostic. 14.4% of the cases were assessed as cellularnodule or neoplastic lesion; all requiring pathologist’s preliminarydiagnosis. Utilizing a cytotechnologist to provide adequacy, insteadof a pathologist, saved $464.10/case (2.38 passes/case) based oncurrent gross technical and professional charges. On the basis ofour findings, cytotechnologists can accurately provide immediateonsite adequacy assessments for thyroid nodule FNAs. Affordingcytotechnologists the opportunity to preliminarily assess FNAs foradequacy also creates a new role in the laboratory. Furthermore,cost-savings are realized for patients and the health care system.Diagn. Cytopathol. 2011;39:896–899. ' 2010 Wiley Periodicals, Inc.
Key Words: thyroid; fine-needle aspiration; cytotechnologist;adequacy assessment
Cytopathologic diagnosis of fine-needle aspirations
(FNAs) of the thyroid gland has become routine clinical
management of thyroid nodules.1 FNA is an accurate
cost-effective method to diagnose nodules, and it has sig-
nificantly reduced the number of unnecessary thyroid sur-
geries.1 FNA can determine the diagnosis of thyroid nod-
ules with a sensitivity of between 65 and 98% and a spec-
ificity of 72 and 100%.1 Most nodules in the thyroid are
benign (69%) with only a small percentage of nodules
diagnosed as malignant (4%).1 Nondiagnostic rates that
vary from 2 to 21%1 are related to the experience of the
aspirator.2 To reduce the nondiagnostic rate, immediate
adequacy assessments/preliminary diagnoses have been
used to determine when an adequate amount of material
has been obtained.2–7 This in turn saves health care dol-
lars by avoiding repeat procedures.8 Currently, a cytopa-
thologic evaluation at the time of aspiration is standard
practice in many cytopathology laboratories, particularly
in academic medical centers.
Some authors believe that any preliminary diagnosis or
assessment should be performed by a pathologist.8 This is
difficult for many hospital laboratories in that it removes
the pathologist from the laboratory for long periods of time.
A reasonable alternative is to have a well-trained cytotech-
nologist provide an immediate assessment with triage to a
pathologist of any patient’s case that is cellular or has any
other neoplastic features. Cytotechnologists are highly
skilled individuals with extensive training in cellular mor-
phology and are well suited to the task of providing on-site
immediate assessments. Enabling cytotechnologists to rou-
tinely provide immediate assessments affords the patholo-
gist time to spend on other tasks, gives the cytotechnologist
a new role in the laboratory, and is a cost saving.
1Department of Cytopathology, University of Wisconsin Hospital andClinics, Madison, Wisconsin
2Department of Pathology and Laboratory Medicine, University ofWisconsin School of Medicine and Public Health, Madison, Wisconsin
*Correspondence to: Angelean L. Wotruba, B.S., C.T., A.S.C.P., Cytopa-thology Laboratory/D4-259d, University of Wisconsin Hospital and Clinics,600 Highland Avenue, Madison, WI 53792. E-mail: [email protected]
Received 16 December 2009; Accepted 3 June 2010DOI 10.1002/dc.21487Published online 14 October 2010 in Wiley Online Library
(wileyonlinelibrary.com).
896 Diagnostic Cytopathology, Vol 39, No 12 ' 2010 WILEY PERIODICALS, INC.
The University of Wisconsin Cytopathology Section in
conjunction with the Endocrinology Division of Medicine
and the Endocrine Surgery Service provides a ‘‘one-stop
shopping’’ model for the workup and management of
patients with thyroid nodules. The endocrinologists and
their fellows perform the aspirations under ultrasound
guidance, a cytopathologist and/or a cytotechnologist im-
mediately reviews the Hema-DiffTM stained slides, and
the endocrine surgeons are available for evaluation of any
patient determined to possibly need surgery. No definitive
treatment is given until the entire specimen is evaluated;
however, the immediate assessment/preliminary diagnosis
provides critical information that allows appropriate triage
of patients. This study was performed to determine the ac-
curacy of the cytotechnologist as compared to the pathol-
ogist for the immediate adequacy assessment of thyroid
nodule FNAs.
Materials and Methods
All data were collected from January through May 2008 at
a twice weekly endocrine thyroid FNA clinic at the Univer-
sity of Wisconsin Hospital and Clinics, Madison, WI.
Three pathologists and five cytotechnologists were
involved in the project. Ultrasound-guided FNAs of thyroid
nodules were performed by an endocrinologist and/or endo-
crinology fellow. A total of 167 thyroid nodules were
sampled during this time period. The cytotechnologist pres-
ent at the procedure prepared the slides and made two
slides with each FNA pass. One slide was alcohol-fixed for
Papanicoloau staining, and the second slide was air-dried
and immediately stained with Hema-DiffTM stain. Needles
were rinsed in Hanks balanced salt solution for Thin-Prep
processing. Typically, three passes were made into each
nodule, and then the procedure was stopped to allow the
cytotechnologist time to review the air-dried slides for ade-
quacy. The specimen was deemed adequate when a mini-
mum of five to six groups of at least 10 follicular cells and
colloid were present.9 A specimen with fewer than five
groups of follicular cells or an absence of colloid was con-
sidered inadequate or nondiagnostic. This terminology was
used interchangeably. The cytotechnologist recorded their
assessment of the sample and then paged the pathologist on
service who viewed the specimen remotely via real-time
video streaming across the intranet using a high-resolution
camera (Fig. 1). The pathologist gave their adequacy
assessment/preliminary diagnosis and the cytotechnologist
also recorded their assessment. The data were recorded
onto an Excel spreadsheet.
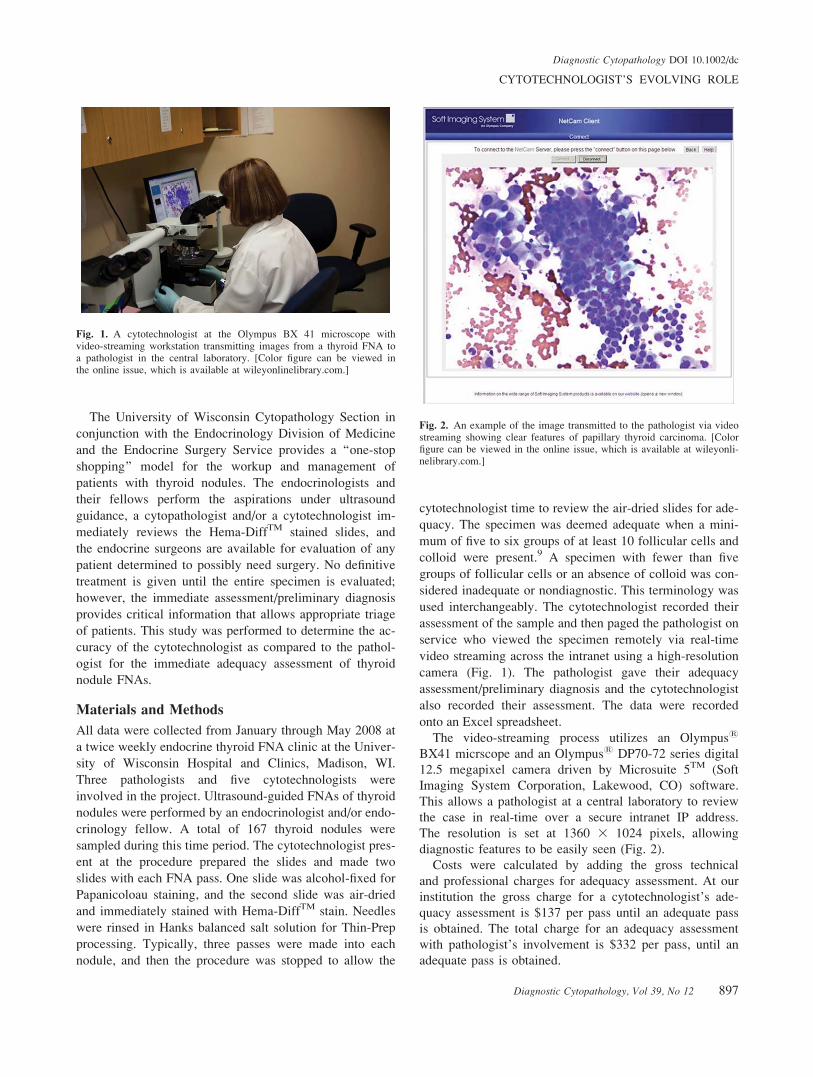
The video-streaming process utilizes an Olympus1
BX41 micrscope and an Olympus1 DP70-72 series digital
12.5 megapixel camera driven by Microsuite 5TM (Soft
Imaging System Corporation, Lakewood, CO) software.
This allows a pathologist at a central laboratory to review
the case in real-time over a secure intranet IP address.
The resolution is set at 1360 3 1024 pixels, allowing
diagnostic features to be easily seen (Fig. 2).
Costs were calculated by adding the gross technical
and professional charges for adequacy assessment. At our
institution the gross charge for a cytotechnologist’s ade-
quacy assessment is $137 per pass until an adequate pass
is obtained. The total charge for an adequacy assessment
with pathologist’s involvement is $332 per pass, until an
adequate pass is obtained.
Fig. 1. A cytotechnologist at the Olympus BX 41 microscope withvideo-streaming workstation transmitting images from a thyroid FNA toa pathologist in the central laboratory. [Color figure can be viewed inthe online issue, which is available at wileyonlinelibrary.com.]
Fig. 2. An example of the image transmitted to the pathologist via videostreaming showing clear features of papillary thyroid carcinoma. [Colorfigure can be viewed in the online issue, which is available at wileyonli-nelibrary.com.]
CYTOTECHNOLOGIST’S EVOLVING ROLE
Diagnostic Cytopathology, Vol 39, No 12 897
Diagnostic Cytopathology DOI 10.1002/dc

Results
A total of 167 thyroid nodule FNAs were included in this
study. The cytotechnologist’s assessment did not agree
with the pathologist’s preliminary diagnosis in only two
cases. The discordance rate was just 1.20% (Table I). Both
discordant cases were clinically insignificant. In one case,
the cytotechnologist’s interpretation was rare atypical cells,
while the pathologist’s preliminary diagnosis was consist-
ent with a benign colloid nodule. In the second case, the
cytotechnologist’s interpretation was nondiagnostic, while
the pathologist’s preliminary diagnosis was consistent with
a benign colloid cyst. In five of the 167 (3.0%) cases the
pathologist’s preliminary diagnoses were discordant with
the final diagnoses (Table II). These cases were also clini-
cally insignificant and merely reflected the reclassification
of a benign diagnosis or unsatisfactory specimen. Some
may argue that these are not even true discordances; there
were no false positives or false negatives in this study.
By cytotechnologist assessment, most nodules (79.0%)
were benign entities including colloid nodules, Hashimo-
to’s thyroiditis, lymphocytic thyroiditis, and thyroid cysts
(Table III). A smaller fraction of nodules (14.4%) were
assessed as atypical or higher. These cases included diagno-
ses of cellular nodule, follicular neoplasm, Hurthle cell neo-
plasm, and papillary carcinoma. As stated previously, these
were the only cases that would require a pathologist’s pre-
liminary diagnosis. Only 6.6% of cases were considered
nondiagnostic by cytotechnologist’s assessment.
The cost incurred for the cytotechnologist’s immediate
adequacy assessment was less than the cost with the path-
ologist’s involvement. Costs were calculated by adding
the gross technical and professional charges for adequacy
assessment. Since the average number of passes to pro-
vide a diagnostic specimen in this study was 2.38 passes,
the cost savings by having a cytotechnologist render ade-
quacy was $464.10 per nodule. There were 145 benign or
nondiagnostic nodules in our study which would have
resulted in a cost savings of $67,294.50. In 2008, our
laboratory provided immediate adequacy on 771 thyroid
nodule FNAs. With an average of 85.7% of these nodules
not requiring pathologist assessment, this would amount
to a total savings of $306,652.68.
Discussion
Cytotechnologists are highly skilled in cytopathologic
morphology and are able to provide adequacy assessments
for thyroid FNAs to ensure that diagnostic samples are
obtained. In this study, adequacy assessments provided by
the cytotechnologists correlated with the preliminary diag-
noses of pathologists in 98.8% of the cases and all discor-
dances were clinically insignificant. Thyroid FNAs have
become part of the standard of care for patients with thy-
roid nodules, thus the demand for their immediate ade-
quacy is increasing. This creates a vital new role for the
cytotechnologists as a preliminary screener for these
specimens.
In our laboratory, cytotechnologists are an integral part
of the endocrinology thyroid clinic. Prior to clinic, the cyto-
technologist reviews the history of each patient and records
all relevant information including past history of thyroid
disease or thyroid cancer, as well as size and ultrasound
characteristics of each thyroid nodule. This information is
then given to the attending pathologist. The cytotechnolo-
gists also provide onsite immediate adequacy assessments
for all thyroid nodule FNAs. When sufficient material has
been collected to render a benign diagnosis, the cytotech-
nologist informs the endocrinologist that no further passes
are required. If the specimen is nondiagnostic, the cytotech-
nologist requests that additional passes be taken until an
adequate sample is obtained. The cytotechnologist is
required to call the pathologist for a preliminary diagnosis
only on those cases that have morphological criteria associ-
ated with an increased chance of malignancy. These fea-
tures include high cellularity, microfollicular arrangements,
Table I. Cytotechnologist Discordant Cases
Casenumber
Cytotechnologistadequacy assessment
Pathologistpreliminarydiagnosis
1 Nondiagnostic Colloid cyst2 Atypical nodule Colloid nodule
Table II. Pathologist Discordant Cases
Case number Preliminary diagnosis Final diagnosis
1 Cellular nodule Colloid nodule2 Colloid nodule Cellular nodule3 Cellular nodule Hashimoto’s thyroiditis4 Colloid nodule Hashimoto’s thyroiditis5 Nondiagnostic Colloid nodule
Table III. Immediate Assessments and Preliminary Diagnoses ofThyroid Nodules
Immediate assessment/preliminary diagnoses
Cytotechnologistnumber ofcases (%)
Pathologistnumber ofcases (%)
Finaldiagnoses
Nondiagnostic 11 (6.6%) 10 (6.0%) 9 (5.4%)Colloid nodule 108 (64.7%) 109 (65.3%) 109 (65.3%)Hashimoto’s thyroiditis 20 (12.0%) 20 (12.0%) 22 (13.2%)Lymphocytic thyroiditis 1 (0.6%) 1 (0.6%) 1 (0.6%)Negative: thyroid cyst 1 (0.6%) 2 (1.2%) 2 (1.2%)Negative: reactivelymph node
2 (1.2%) 2 (1.2%) 2 (1.2%)
Atypical nodulea 1 (0.6%) 0 (0.0%) 0 (0.0%)Cellular nodulea 10 (6.0%) 10 (6.0%) 9 (5.4%)Follicular neoplasma 5 (3.0%) 5 (3.0%) 5 (3.0%)Hurthle cell neoplasma 1 (0.6%) 1 (0.6%) 1 (0.6%)Papillary cancera 7 (4.2%) 7 (4.2%) 7 (4.2%)Total 167 (100%) 167 (100.0%) 167 (100%)
aDenotes immediate assessments that should be viewed by a pathologistfor a preliminary diagnosis whenever possible.
WOTRUBA ET AL.
898 Diagnostic Cytopathology, Vol 39, No 12
Diagnostic Cytopathology DOI 10.1002/dc

nuclear inclusions, etc. A cytotechnologist also may call a
pathologist for an evaluation of any case that they have dif-
ficulty in assessing. The pathologist’s evaluation is accom-
plished rapidly via video-streaming utilizing the NetCam
feature of Microsuite 5TM and ensures the proper triage of
patients to the endocrine surgeons.
It is important to note that no definitive surgical inter-
vention is performed until the final diagnostic report is
issued. Patients are merely triaged to a surgeon for evalu-
ation and scheduled for further pre-op appointments in
the event that the preliminary diagnosis becomes the final
one after review of all case materials. This ‘‘one-stop
shopping’’ model provides access to the appropriate heath
care provider in one clinic visit, eliminating delays in
appropriate patient care and management.
Utilizing a cytotechnologist as a preliminary screener
of thyroid FNAs saves pathologist’s time. The average
time for a pathologist to be present and provide adequacy
assessments on FNAs of thyroid nodules has been
reported as 35–57 minutes.3 In addition, immediate on-
site interpretations of FNAs by pathologists are insuffi-
ciently compensated by Medicare.10 Sending a cytotech-
nologist for immediate onsite adequacy saves time and
money, as illustrated in our study.
Some3,11 have advocated not providing immediate eval-
uations for FNAs, reporting that there is not a significant
enough decrease in the nondiagnostic rate to justify the
procedure time for the staff involved. However, our insti-
tution is academic and the training of house staff is a
major mission. By providing immediate adequacy assess-
ments, we also assist other departments to train their resi-
dents and fellows in the collection of thyroid FNA speci-
mens while ensuring an adequate sample is obtained. In
addition, patient satisfaction is greatest when an FNA is a
‘‘one-stop’’ procedure, obviating the need for a repeat
clinic visit with its incurred costs to the patient and the
healthcare system.
Our study has shown that cytotechnologists can provide
immediate adequacy assessments to nearly the same accu-
racy as a pathologist. This is a new role for many cyto-
technologists, but a role that once they are trained they
should readily accept. We recommend that institutions
routinely provide immediate on-site adequacy for all thy-
roid FNAs and provide the cytotechnologist the opportu-
nity to do so.
Acknowledgments
We thank the Cytopathology staff at the University of
Wisconsin Hospital and Clinics for their assistance with
this study.
References
1. Gharib H, Goellner J. Fine-needle aspiration biopsy of the thyroid:an appraisal. Ann Intern Med 1993;118:282–289.
2. Ghofrani M, Beckman D, Rimm DL. The value of onsite adequacyassessment of thyroid fine-needle aspirations is a function of opera-tor experience. Cancer (Cancer Cytopathol) 2006;108:110–113.
3. Eedes CR, Wang HH. Cost-effectiveness of immediate specimenadequacy assessment of thyroid fine-needle aspirations. Am J ClinPathol 2004;121:64–69.
4. Jing X, Michael CW, Pu RT. The clinical and diagnostic impact ofusing standard criteria of adequacy assessment and diagnostic termi-nology on thyroid nodule fine needle aspiration. Diagn Cytopathol2008;36:161–166.
5. Nguyen G, Lee MW, Ginsberg J, Wragg T, Bilodeau D. Fine-needleaspiration of the thyroid: An overview. CytoJournal 2005:2:12.
6. Redman R, Zalaznick H, Mazzaferri EL, Massoll NA. The impactof assessing specimen adequacy and number of needle passes forfine-needle aspiration biopsy of thyroid nodules. Thyroid2006;16:55–60.
7. Zhu W, Michael C. How important is on-site adequacy assessmentfor thyroid FNA? An evaluation of 883 cases. Diagn Cytopathol2006;35:183–186.
8. Nasuti JF, Gupta PK, Baloch ZW. Diagnostic value and cost-effec-tiveness of on-site evaluation of fine-needle aspiration specimens:Review of 5,688 cases. Diagn Cytopathol 2002;27:1–4.
9. Pitman MB, Abele J, Ali SZ, et al. Techniques for thyroid FNA: Asynopsis of the National Cancer Institute Thyroid Fine-Needle Aspi-ration State of the Science Conference. Diagn Cytopathol2008;36:407–424.
10. Layfield LJ, Bentz JS, Gopez EV. Immediate on-site interpretationof fine-needle aspiration smears. Cancer (Cancer Cytopathol)2001;93:319–322.
11. O’Malley ME, Weir MM, Hahn PF, Misdraji J, Wood BJ, MuellerPR. US-guided fine-needle aspiration biopsy of thyroid nodules: Ad-equacy of cytologic material and procedure time with and withoutimmediate cytologic analysis. Radiology 2002;222:383–387.
CYTOTECHNOLOGIST’S EVOLVING ROLE
Diagnostic Cytopathology, Vol 39, No 12 899
Diagnostic Cytopathology DOI 10.1002/dc


















