Adam Wells, MD Severe COPD - … · Anthonisen et al. Am J Respir Crit Care Med 2002;166(5)675-9....
21
4/6/2018 1 Faculty Disclosure Adam D. Wells, MD Dr. Wells has listed no financial interest/arrangement that would be considered a conflict of interest. Severe COPD: What Can Be Done When Everything Else Fails Adam D. Wells, MD CHI Creighton Health Pulmonary and Critical Care Medicine 4/12/18
Transcript of Adam Wells, MD Severe COPD - … · Anthonisen et al. Am J Respir Crit Care Med 2002;166(5)675-9....
4/6/2018
1
Faculty DisclosureAdam D. Wells, MD
Dr. Wells has listed no financial interest/arrangement that would be considered a
conflict of interest.
Severe COPD: What Can Be Done When Everything Else Fails
Adam D. Wells, MDCHI Creighton Health
Pulmonary and Critical Care Medicine4/12/18
4/6/2018
2
Objectives:
• Review recent updates to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines
• Discuss adjuvant therapies for those patients who traditional inhaled therapies have not medically stabilized
• Present future therapies of COPD
COPD Definition ‐ GOLD
• Airflow limitation (obstruction) that is NOT fully reversible• Usually both PROGRESSIVE and associated with an abnormal
response of lungs to noxious particles or gases
4/6/2018
3
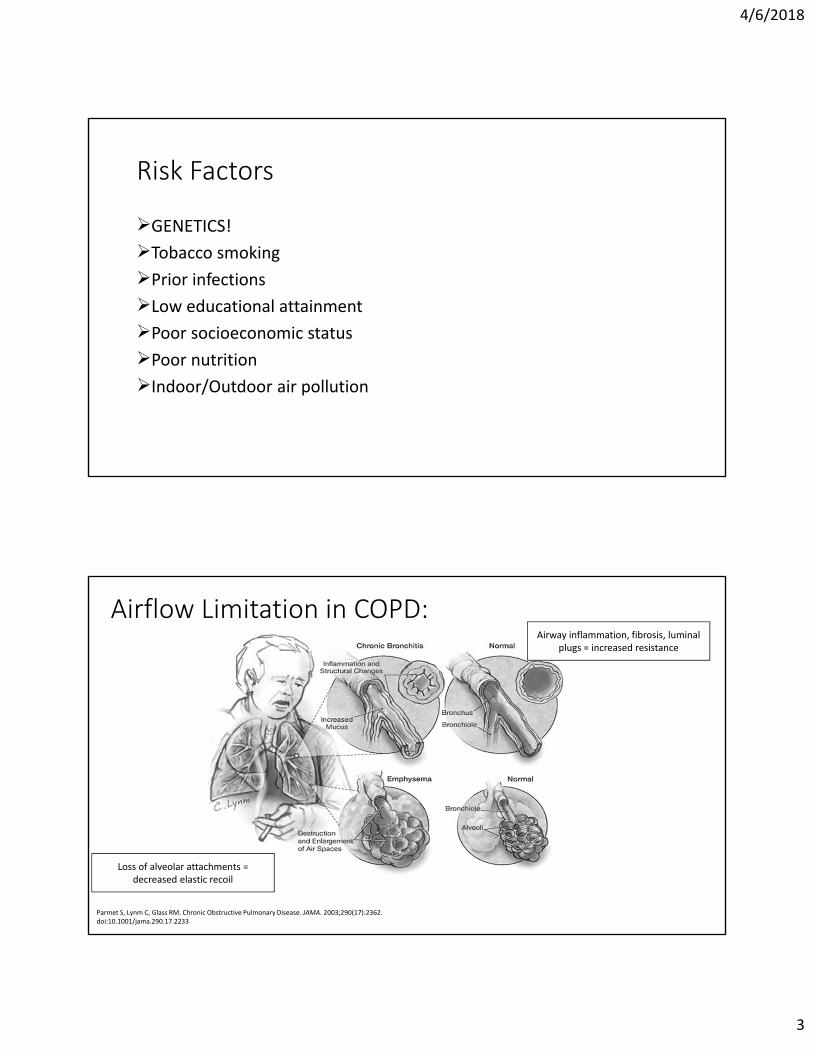
Risk Factors
GENETICS!Tobacco smokingPrior infectionsLow educational attainmentPoor socioeconomic statusPoor nutritionIndoor/Outdoor air pollution
Parmet S, Lynm C, Glass RM. Chronic Obstructive Pulmonary Disease. JAMA. 2003;290(17):2362. doi:10.1001/jama.290.17.2233
Airway inflammation, fibrosis, luminal plugs = increased resistance
Loss of alveolar attachments = decreased elastic recoil
Airflow Limitation in COPD:
4/6/2018
4
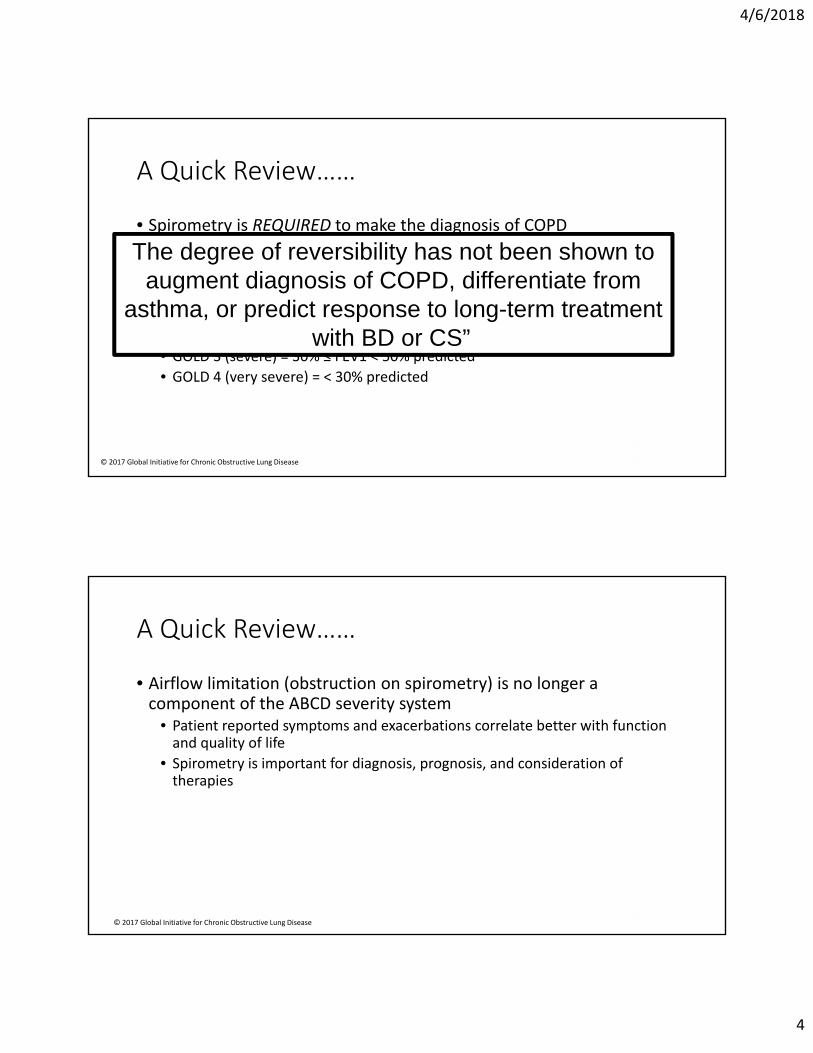
A Quick Review……
• Spirometry is REQUIRED to make the diagnosis of COPD• POST-bronchodilator FEV1/FVC ratio <0.70
• Disease is GRADED and GROUPED• GOLD Grade 1 = FEV1 ≤ 80% predicted• GOLD 2 (moderate) = 50% ≤ FEV1 < 80% predicted• GOLD 3 (severe) = 30% ≤ FEV1 < 50% predicted• GOLD 4 (very severe) = < 30% predicted
© 2017 Global Initiative for Chronic Obstructive Lung Disease
The degree of reversibility has not been shown to augment diagnosis of COPD, differentiate from
asthma, or predict response to long-term treatment with BD or CS”
• Airflow limitation (obstruction on spirometry) is no longer a component of the ABCD severity system
• Patient reported symptoms and exacerbations correlate better with function and quality of life
• Spirometry is important for diagnosis, prognosis, and consideration of therapies
A Quick Review……
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
5
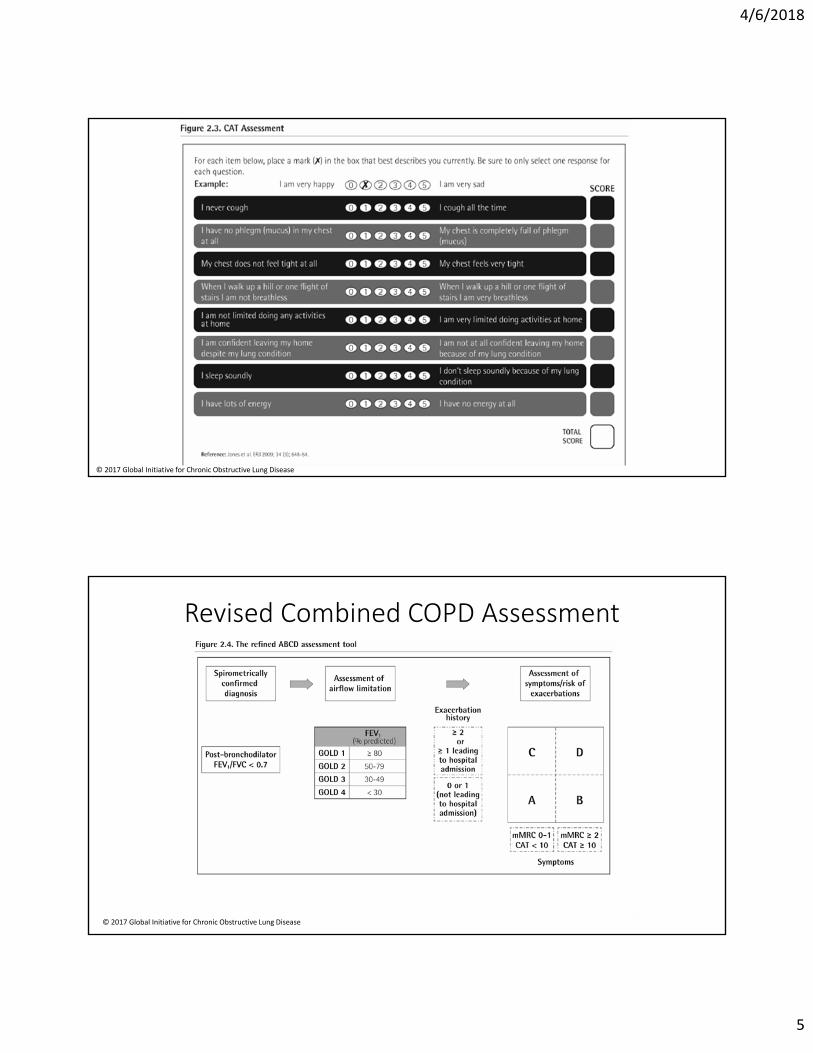
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Revised Combined COPD Assessment
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
6
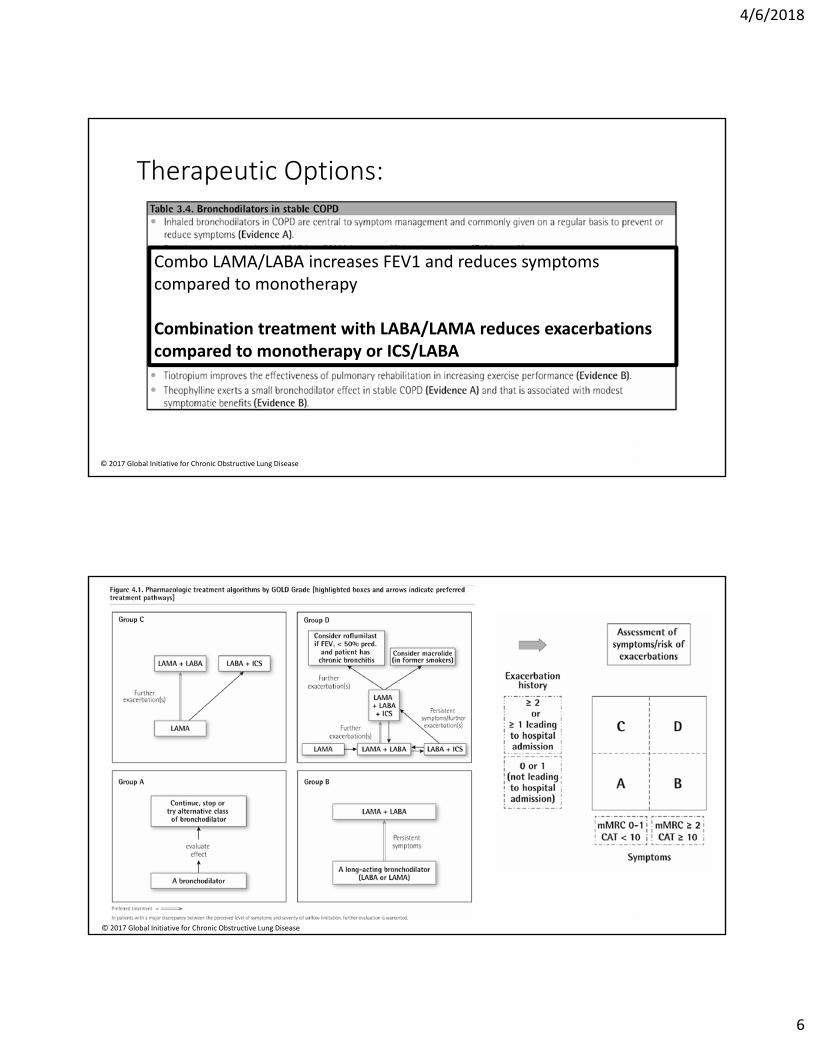
Therapeutic Options:
Combo LAMA/LABA increases FEV1 and reduces symptoms compared to monotherapy
Combination treatment with LABA/LAMA reduces exacerbations compared to monotherapy or ICS/LABA
© 2017 Global Initiative for Chronic Obstructive Lung Disease
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
7
Therapeutic Options:
• “Triple Therapy” improves lung function, symptoms, health status, and reduces exacerbation compared to ICS/LABA or LAMA monotherapy
• Inhaled corticosteroid therapy is associated with an increased risk of pneumonia
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Prevention:
• Vaccinate for influenza and pneumonia• Influenza vaccination decreases serious illness and death in COPD patients• PPSV23 decreased incidence of CAP in COPD patients <65 with FEV1 <40%
pred• PCV13 decreases bacteremia and invasive pneumococcal diseases
© 2017 Global Initiative for Chronic Obstructive Lung Disease

4/6/2018
8
In Summary……
- Make dang sure they know how to use the inhaler- Figure out what they can actually afford and access- Even though they say they know what they are doing, see what they
are actually doing – it’s probably wrong- Before you bail on a therapy, make sure the above.
When you've maximized inhalers:
4/6/2018
9
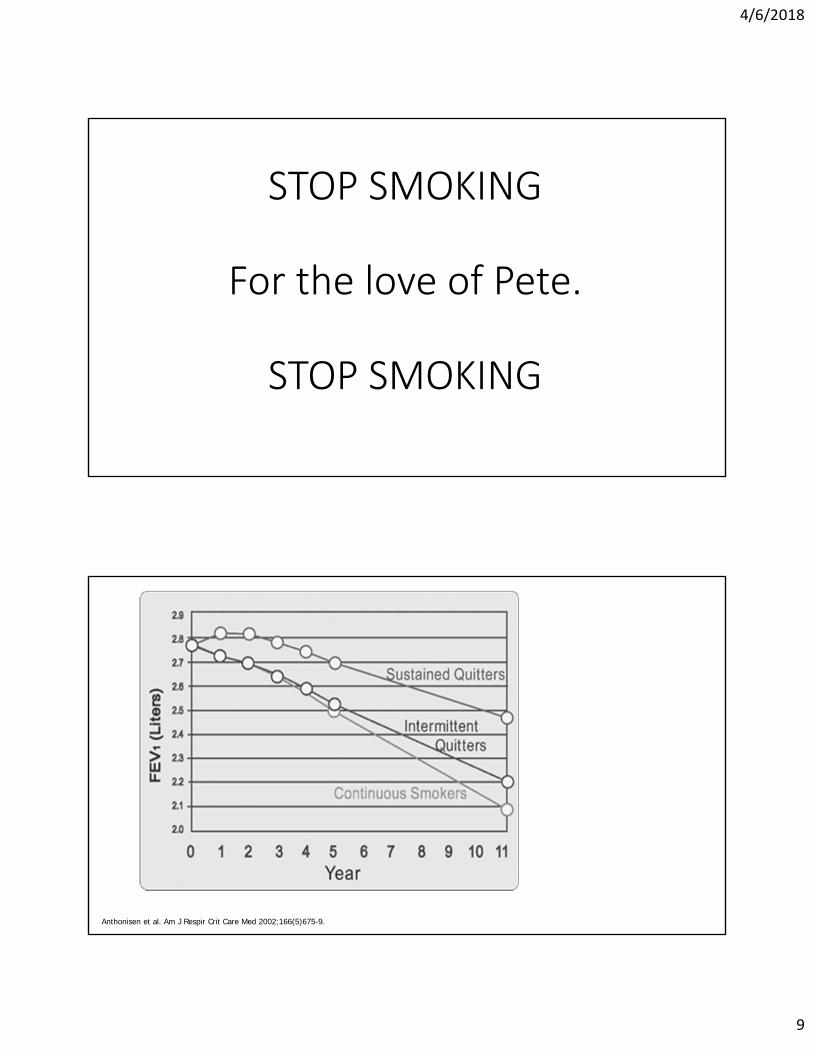
STOP SMOKING
For the love of Pete.
STOP SMOKING
Anthonisen et al. Am J Respir Crit Care Med 2002;166(5)675-9.

4/6/2018
10
Pulmonary Rehabilitation
• Improves dyspnea, health status, exercise tolerance• Reduces hospitalization in those with recent exacerbation• Most effective therapeutic strategy to improve SOB, health status,
exercise tolerance• ***Home based pulm rehab MAY be equivalent
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Who gets oxygen?
• Severe chronic resting arterial hypoxemia ( pa02 < 55mmHg)• >15 hours of use per day
• Long term therapy does not affect outcomes for those with stable COPD and resting or exercise induced moderate arterial O2 desaturation
© 2017 Global Initiative for Chronic Obstructive Lung Disease

4/6/2018
11
Therapy you have heard of but don’t use…
• Macrolide Therapy• Azithromycin is best evidence• Reduces exacerbations over one year*
• Associated with increased incidence of bacterial resistance and hearing impairment• Dosed at 250mg/day or 500mg 3x/weekly• ***Less benefit in active smokers***
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Therapy you have heard of but don’t use…
• Roflumilast therapy• PDE4 inhibitor – increases intracellular cAMP and decreasing inflammatory
cell activity• Consider in patients with:
• FEV1 <50% and chronic bronchitis AND• 1+ hospitalizations in the previous year
• Improves lung function and decreases mod/severe exacerbations• Improves lung function and decreases exacerbation in patients already on
LABA/ICS
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
12
Therapy you have heard of but don’t use…
• N-acetylcystine (NAC) & carbocysteine (in those not on ICS)• Decreases exacerbations• Improvement in health status
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Therapy you have heard of but don’t use…
• A1AT Deficiency (ZZ)• ALL COPD patients, regardless of age should be tested• Replacement therapy MAY slow progression of disease in select
populations• Ex-smokers• FEV1 35-65% predicted• OR >65% but decline of 100mL/year or more in deficient patients
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
13
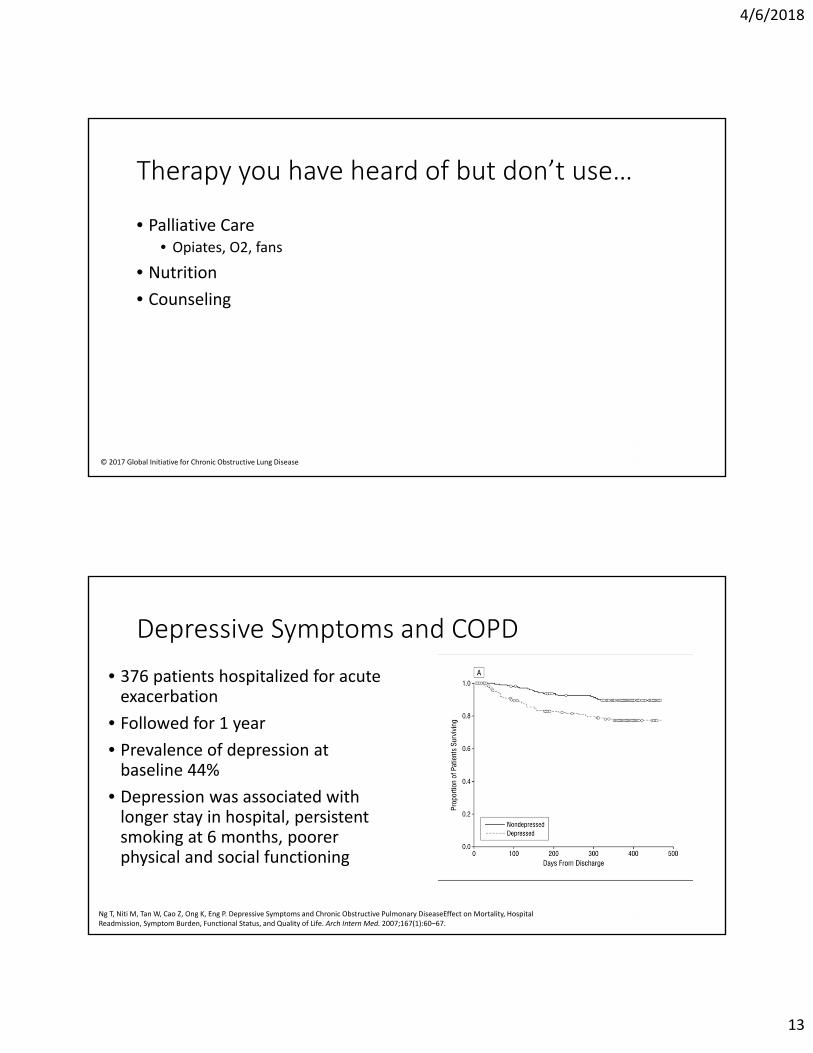
Therapy you have heard of but don’t use…
• Palliative Care• Opiates, O2, fans
• Nutrition• Counseling
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Depressive Symptoms and COPD
• 376 patients hospitalized for acute exacerbation
• Followed for 1 year• Prevalence of depression at
baseline 44%• Depression was associated with
longer stay in hospital, persistent smoking at 6 months, poorer physical and social functioning
Ng T, Niti M, Tan W, Cao Z, Ong K, Eng P. Depressive Symptoms and Chronic Obstructive Pulmonary DiseaseEffect on Mortality, Hospital Readmission, Symptom Burden, Functional Status, and Quality of Life. Arch Intern Med. 2007;167(1):60–67.
4/6/2018
14
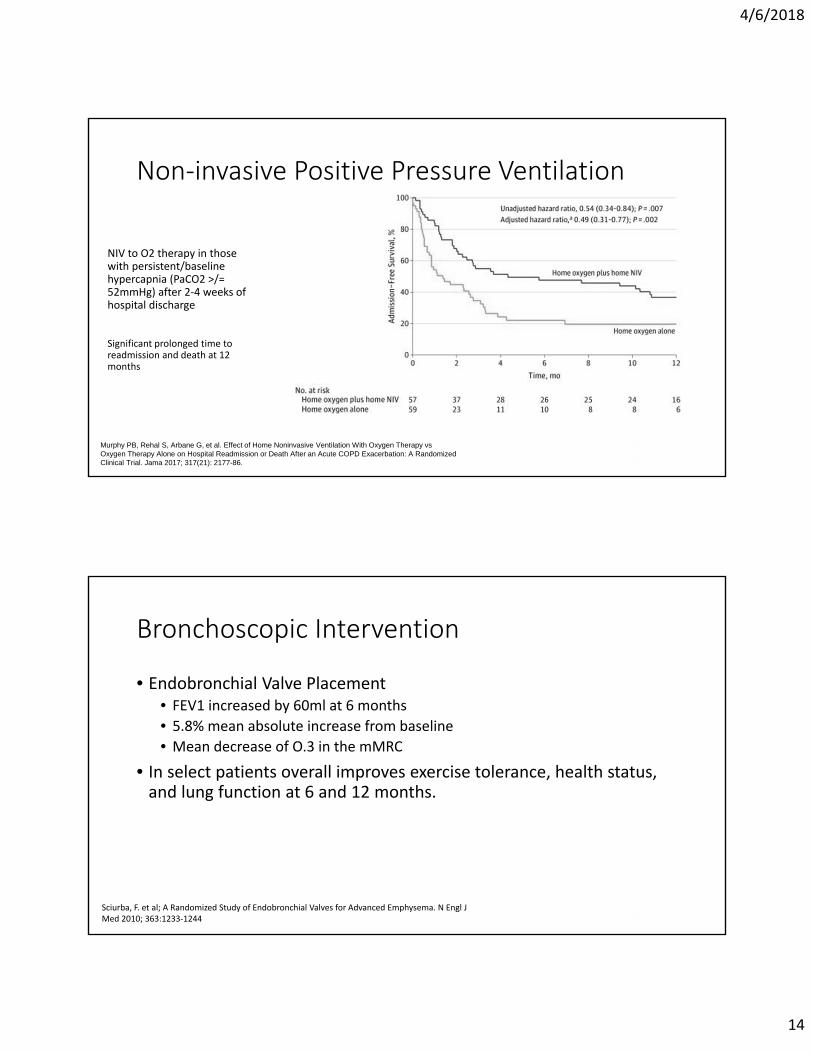
Non‐invasive Positive Pressure Ventilation
NIV to O2 therapy in those with persistent/baseline hypercapnia (PaCO2 >/= 52mmHg) after 2-4 weeks of hospital discharge
Significant prolonged time to readmission and death at 12 months
Murphy PB, Rehal S, Arbane G, et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. Jama 2017; 317(21): 2177-86.
Bronchoscopic Intervention
• Endobronchial Valve Placement• FEV1 increased by 60ml at 6 months• 5.8% mean absolute increase from baseline• Mean decrease of O.3 in the mMRC
• In select patients overall improves exercise tolerance, health status, and lung function at 6 and 12 months.
Sciurba, F. et al; A Randomized Study of Endobronchial Valves for Advanced Emphysema. N Engl J Med 2010; 363:1233-1244

4/6/2018
15
Surgical Treatments
• Lung Transplantation: In appropriately selected patients, improves quality of life and functional capacity
• Criteria for referral: FEV1<35% predicted PaO2<55-60mm Hg, PaCO2>50 mm Hg, and secondary pulmonary hypertension ***
• Lung Volume Reduction Surgery• Increases chance of improved exercise capacity • Survival advantage for patients with predominantly upper-lobe emphysema
and low base-line exercise capacity
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Things that probably don’t work…
• Anti-tussive therapy• Vasodilators
© 2017 Global Initiative for Chronic Obstructive Lung Disease
4/6/2018
16
High‐Risk Phenotypes
• Asthma COPD Overlap Syndrome (ACOS)• Encompasses different phenotypes
• Eosinophilic COPD• Severe asthma with incomplete airflow reversibility• Asthma with smoking
• More exacerbation and more symptoms than either alone• Evaluation is different –
• IgE, eosinophils, FeNO
Future Directions

4/6/2018
17
More liberal use of ICS (especially for group C or D) High dose ICS?
Omalizumab IL-5 therapy (Coming soon!) Benralizumab Mepolizumab Reslizumab
High‐Risk Phenotypes
- Maltby et al. Omalizumab treatment response in a population with severe allergic asthma and overlapping COPD. Chest 2017;151:78-89.- Bel et al. New Anti-Eosinophil Drugs for Asthma and COPD. Chest 2017; 152(6) 1276-1282
Self/Multi‐disciplinary Management
Rice KL, Dewan,N et al. Disease management program for COPD: A randomized controlled trial. AJRCCM 2010;182: 890-896.
- 41% reduction in rate of hospitalizations and emergency visits for COPD among the disease management patients
- 30% lower hospitalization rate after 1 year
- Group education- Smoking cessation- Inhaler use teaching- Vaccinations- Exercise options- Hand hygiene- Action Plans- Case manager- Telephone number

4/6/2018
18
What to do when nothing else works?
• How are you managing?• COPD is now managed according to group, not severity of obstruction
• Ensure inhaled therapies are correctly chosen• Do they have a SABA? Are they on a LAMA?
© 2017 Global Initiative for Chronic Obstructive Lung Disease

4/6/2018
19
What to do when nothing else works?
• Have you ensured the patient is using the inhaled therapy correctly?• Have you addressed smoking?• What preventative measures could you initiate?
• Vaccinations• Pulmonary Rehab• Nutrition• Depression
• Have you checked for A1AT?
What to do when nothing else works?
• Are they a candidate for on therapies?• NAC• Roflumilast• Azithromycin
• Are they a potential surgical candidate?• Upper lobe predominance• Transplant referral?

4/6/2018
20
What to do when nothing else works?
• Are you engaging the Patient? • Make an action plan
• Steroids, antibiotics in hand• Easy phone access• Written materials
Need more help?

4/6/2018
21
Questions?