Acyanotic Congenital Heart Disease Dr David Coleman Consultant Paediatric Cardiologist Our Lady’s...
27
Acyanotic Congenital Heart Disease Dr David Coleman Consultant Paediatric Cardiologist Our Lady’s Children’s Hospital, Crumlin Dublin
-
Upload
freddy-severn -
Category
Documents
-
view
226 -
download
2
Transcript of Acyanotic Congenital Heart Disease Dr David Coleman Consultant Paediatric Cardiologist Our Lady’s...

Acyanotic Congenital Heart
Disease
Dr David Coleman
Consultant Paediatric CardiologistOur Lady’s Children’s Hospital, Crumlin
Dublin

Common Shunt Lesions
♥ Ventricular septal defect (VSD)
♥ Atrial septal defect (ASD)
♥ Patent ductus arteriosus (PDA)
* All 3 lesions can lead to Eisenmenger’s Syndrome if a large lesion is not detected and treated early enough

Common Stenotic Lesions
♥ Pulmonary stenosis (PS)
♥ Aortic stenosis (AS)
♥ Coarctation of the aorta (CoA)

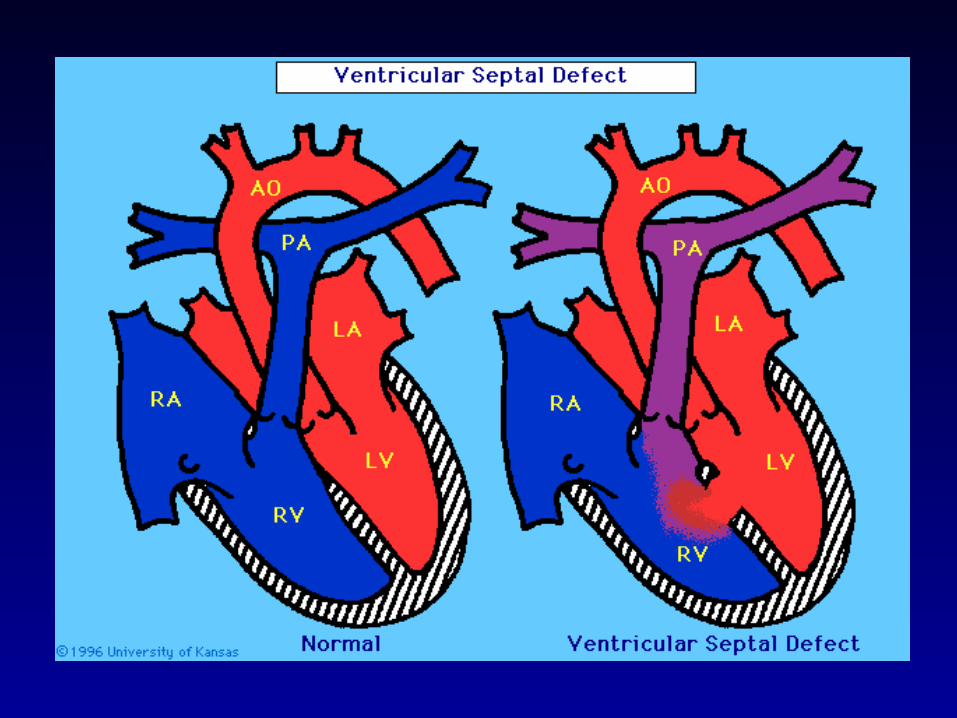
VSD’s
♥ Commonest form of CHD
♥ Commonest types:membranous (perimembranous)
~75%muscular
♥ Can be single or multiple
VSD’s
♥ Symptoms relate to the degree of shunt (VSD size, pulmonary vascular resistance)
if small: no symptoms
if large (high pulmonary blood flow, CHF):tachypnoeadyspnoeaslow feeding failure to thrivesweating

VSD’s
♥ Exam (smaller VSD):pinknormal pulsesnormal S1 and S2± systolic thrillharsh pansystolic murmur
LLSE
♥ ECG: normal (smaller VSD)or LVH ± RVH (larger VSD)

VSD’s
♥ Larger defect:
MDM @ apex (mitral flow murmur)
narrowly split S2 and loud P2
± S3
CXR: cardiomegaly increased pulmonary
vascularity
VSD’s
♥ Treatment options:
Nil (spontaneous closure)
Surgical closure
Device closure

ASD’s
♥ Three types: secundumprimumsinus venosus
♥ Commonest: secundum
♥ Primum: a form of atrioventricular septal (canal) defect



Secundum ASD
♥ Usually no symptoms in childhood
♥ Exam: pinknormal pulseswide ± ‘fixed’ split S2soft ESM @ ULSE
♥ ECG: incomplete RBBB (95%)
♥ CXR: often normal sometimes pulmonary
plethora

Secundum ASD
♥ Haemodynamic significance of ASD is assessed to decide if closure appropriate
♥ Usually closed age 3-5 years (earlier if symptomatic) or when diagnosed if later
♥ Two options for closure:surgery - suture or patchinterventional catheter - device

Amplatzer ASD Occluder

PDA
♥ CHF symptoms if large ductus in very young infant, otherwise often asymptomatic
♥ Exam: pinkfull volume pulsesharsh systolic (1st few weeks) or continuous ‘machinery’
murmur loudest under left clavicle
♥ ECG: normal (small PDA)LVH ± RVH (large PDA)

PDA
♥ CXR: ± cardiomegaly, pulm plethora
♥ Options for closure:
surgery - ligationinterventional catheter - coil(s) or
device

Pulmonary Stenosis
♥ Usually asymptomatic
♥ Exam: pinknormal pulses± systolic ejection clickESM loudest @ ULSE if severe, S2 widely split (not
fixed)


Pulmonary Stenosis
♥ ECG:RAD, RVH
♥ CXR: normal ± prominent MPA (post-stenotic dilatation)
♥ Treatment of valvar PS (moderate/severe):balloon valvuloplasty preferreduncommonly surgical
valvotomy

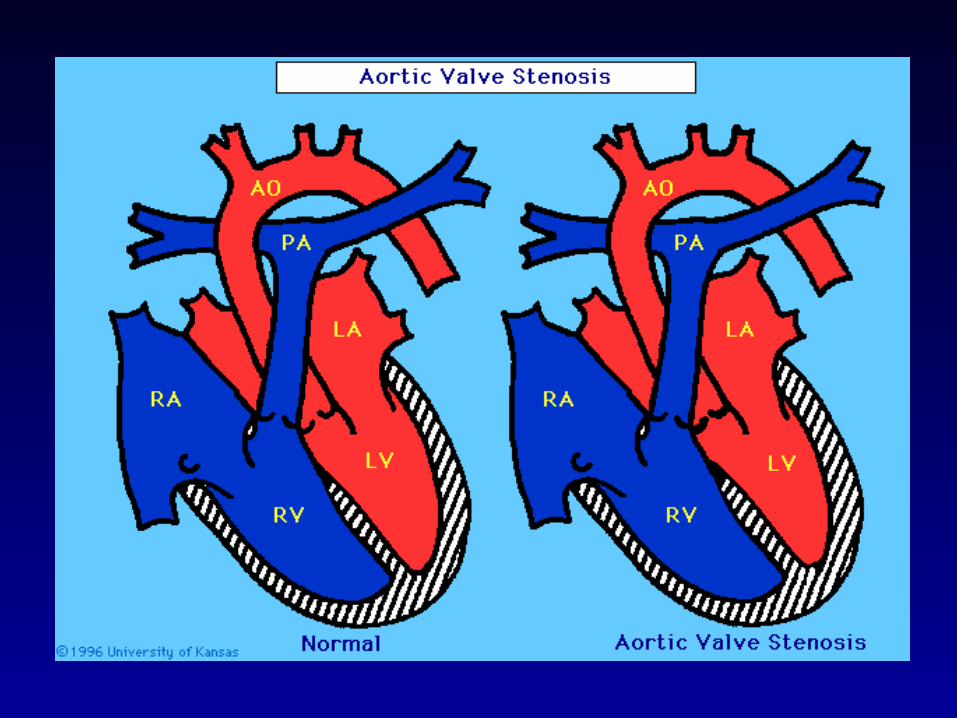
Aortic Stenosis
♥ Often asymptomatic; otherwise SOB, syncope or chest pain on exertion
♥ Exam: pinksmall volume pulse, small pulse pressure± LV lift± systolic thrill (suprasternal, URSE)± systolic ejection clickharsh ESM loudest @ URSE & radiating to carotidsif severe, narrow split S2 (even reversed)

Aortic Stenosis
♥ ECG:normal (mild AS)LVH ± strain (more severe AS)
♥ CXR: often normal± dilated ascending aorta
♥ Treatment of valvar AS (moderate/severe):balloon valvuloplastysurgical valvotomy

Coarctation of the Aorta
♥ CHF in neonate if severe CoA;often asymptomatic in older child
♥ Exam: pinkreduced or absent femoral
pulsessoft systolic murmur mid LSE and/or mid left back
♥ ECG:RVH in 1st few months of life,LVH if older


Coarctation of the Aorta
♥ CXR: cardiomegalyevidence of CHFrib notching (older child)
♥ Treatment:surgery for ‘native’ CoAballoon angioplasty for re-
CoA