Acute rheumatic fever
12
Acute rheumatic fever Inflammatory disease following group A β-hemolytic streptococcal infection, due to cross-reactivity of antigens
-
Upload
puneet-shukla -
Category
Health & Medicine
-
view
139 -
download
5
description
a problem of the heart still seen among young in developing countries
Transcript of Acute rheumatic fever

Acute rheumatic fever
Inflammatory disease following group A β-hemolytic streptococcal infection, due to cross-reactivity of
antigens

Epidemiology Onset- ~2-3 weeks after streptococcal
infection Rate of development after untreated
infection- ~3% Recurrence with a subsequent
untreated infection- 5-50%, more in patients with RHD
Common in children- age 5-15, only 20% first attacks in adults

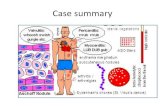
Pathogenesis Possible autoimmune disease Follows pharyngitis due to encapsulated GABH
streptococci A complex interplay of genetically determined host
susceptibility, pathogenic GABH streptococcal infection, in a susceptible environment
Best defined virulence factor- M protein Present on surface of bacteria Promotes bacterial adherence & resist phagocytosis Shares homology with cardiac myosin, tropomyosin, keratin,
laminin Types 1,3,5,6,14,18,19,24 associated with ARF Other- T cell activation by streptococcal superantigens,
leading to granuloma formation

Pathology Myocardial Aschoff body- a submiliary
granuloma, later forms scar Endocardial verrucous valvulitis, heals
with fibrous thickening & adhesions, causing stenosis or regurgitation
Serofibrinous pericarditis Joint- exudative arthritis Subcutaneous nodules- granuloma

Modified Jones’ criteria Used for diagnosis 2 major or 1 major+2 minor or
2 minor (in patient with RHD), with evidence of streptococcal infection
Evidence of s’coccal infection within last 45 days-
Elevated/rising ASO/anti-DNase B titres Positive throat culture Rapid Ag test for GABH s’cocci Recent scarlet fever

Jones’ criteria Major Migratory polyarthritis,
involves large joints Carditis- pancarditis Subcutaneous nodules-
painless, extensor Erythema marginatum-
over trunk/arms Sydenham’s chorea
Minor Fever Arthralgia Raised ESR/CRP ECG- heart-block-
prolonged PR interval
Previous e/o rheumatic fever

Acute carditis New murmur or change in pre-existing murmur Apical pansystolic murmur- MR ± Carey Coomb murmur-apical
MDM Basal early diastolic murmur- AR Tachycardia Soft heart sounds New onset CHF- gallop rhythm- S3 Pericardial rub or effusion Cardiomegaly Within 6 months of acute streptococcal infection

Course
90% attacks subside within 12 weeks
<5% persist >6 months

Recurrence
With new M-type streptococcal infectionMost common within first 5 years
Frequency decreases with time

GABH streptococcal pharyngitis
Age <15 years, high-grade fever, tonsillar
swelling/exudate, tender anterior Cxal LNE,
absence of cough

Treatment Acute streptococcal infection-
1.2 million units of benzathine penicillin G or amoxycillin/1st gen. oral cephalosporin x 10 days
Erythromycin, 500 BD x 10 days, if penicillin sensitive/allergic
Acute arthritis- ASA/NSAIDs Acute carditis- prednisolone, rest, diuretics, ACEI Chorea- diazepam, haloperidol, carbamazepine
Monitor ESR/CRP for duration of symptomatic Rx

Prophylaxis 1.2 million units of benzathine penicillin G,
IM q 3-4 weeks Sulfadiazine, 500 BD or Erythromycin, 250 BD,
if penicillin sensitive Duration- Without carditis- X 10 years or upto 21 years of age,
whichever is longer (WHO- x 5 yrs./upto 18 yrs. of age)
With carditis/RHD- upto 40 years of age (WHO- X 10 yrs./upto 25 yrs. of age)
Severe RHD/after valve Sx- lifelong Problem- compliance No recurrence with proper compliance