Acute Respiratory Distress Syndrome Has management changed in the last Decade? Ram E. Rajagopalan,...
50
Acute Respiratory Distress Syndrome Has management changed in the last Decade? Ram E. Rajagopalan, MBBS, AB (Int Med) AB (Crit Care) Head, Department of Critical Care Medicine SUNDARAM MEDICAL FOUNDATION
-
Upload
barbara-oconnor -
Category
Documents
-
view
214 -
download
0
Transcript of Acute Respiratory Distress Syndrome Has management changed in the last Decade? Ram E. Rajagopalan,...

Acute Respiratory Distress SyndromeHas management changed in the last Decade?
Ram E. Rajagopalan,MBBS, AB (Int Med) AB (Crit Care)
Head, Department of Critical Care MedicineSUNDARAM MEDICAL FOUNDATION
Chennai

CT Ratio <.55
X-Ray in Early ARDS
Homogeneous pulmonaryinfiltrates
Non-central distributionof oedema
Normal cardiac size
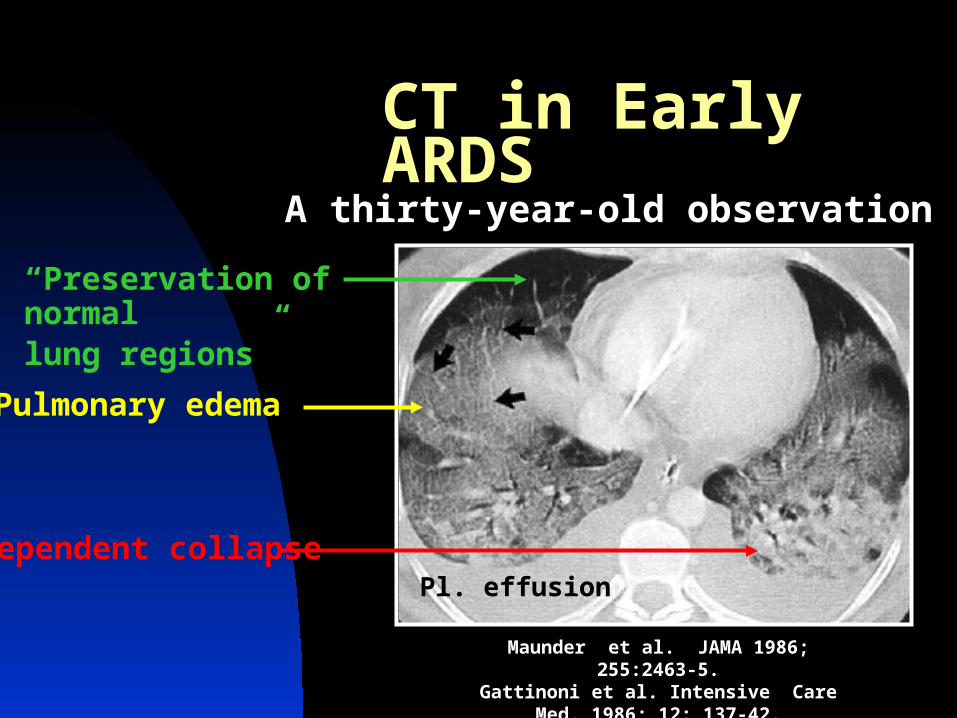
Pl. effusion
CT in Early ARDS
Maunder et al. JAMA 1986; 255:2463-5.Gattinoni et al. Intensive Care Med. 1986; 12: 137-42.
“Preservation of normallung regions”
Pulmonary edema
Dependent collapse
A thirty-year-old observation

“It is Sponge Lung!!”
“Sponge Lung”* Gravity dependent atelectasis
Lung superimposedpressure
Density x h
h
*Int Care Med 1986; 12: 137-42.**AJRCCM 2002; 165: 1647–53.

The “Baby lung”
Unaerated segments distend poorly High pressure Slow response
Normal lung segments may be over-inflated when ventilated with traditional tidal volumes
ARDS Lung has “normal” & unaerated / partially aerated alveoli
“Normal” segments inflate easily

Tidal Volume in ARDSLow (6cc / Kg) vs. ‘traditional’ (12 cc/Kg)
N Engl J Med 2000; 342: 1301-8.
n = 432 vs. 429

P-V relationship in ARDS
Pressure
Volume
LIP
UIP
Beside avoiding large Vt……
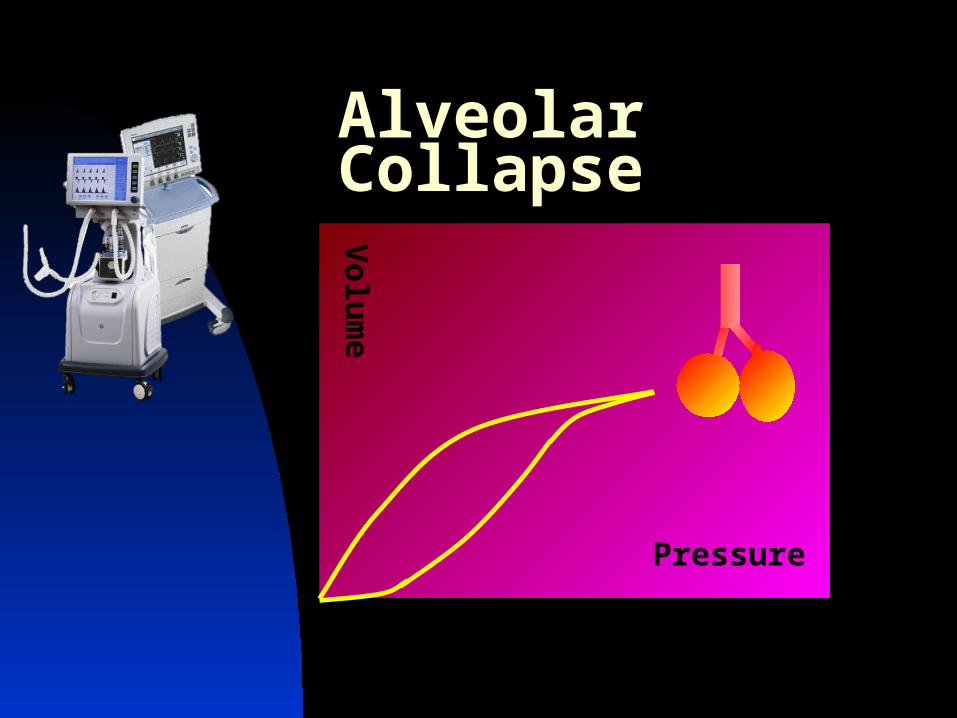
Alveolar Collapse
Pressure
Volume

“Volutrauma & Atelectrauma”
Non-dependent bullae areprobably due to alveolaroverdistension
Dependent bullae are dueto alternating opening &closing of the airway
Gattinoni et al. AJRCCM 2001; 164: 1701-11.
Pressure
Volume PEEP LIMIT Pr. or Vol.
Limiting Injury: “Lung Protective Ventilation”

ARDSnet: High vs. Low PEEP
NEJM 2004; 351: 327-36.
FiO2 LoPEEP HiPEEP0.3 5 140.4 5 14-160.5 8-10 15-18-200.6 10 200.7 12-14 200.8 14 20-220.9 14-18 221.0 18-24 22-24
1.0
0.5
00 10 20 30 40 50 60
Prob
abili
ty
Days
Survival
Discharge
1.0
0.5
00 10 20 30 40 50 60
1.0
0.5
00 10 20 30 40 50 60
Prob
abili
ty
Days
Survival
Discharge
n = 549

Variability in Recruitable Lung
*AJRCCM 2005; 171: 1002-1008.
The “anatomical” (CT) extent of potentially recruitable lung is very variable
Supports prior physiological studies*
A B
0
5
10
15
20
25
-5 0 5 10 15 20 25 30 35 40 45 50 55 60
A B
n
Recruitable lung (% of total)
N Engl J Med 2006;354:1775-86.

Problems with ARDSnet approach
PEEP
Significant“Recruitable”Lung volume
Sparse“Recruitable”Lung volume
Opens alveoliBenefits patient
Hyperinflates lungHarms patient
No Effect; a l’ARDSnet
Identification ofthe potentiallyrecruitable ARDSlung becomes important

Heterogeneous effect of Paw Ptp (not Pairway ) correlates c EELV
A uniform airway pressure causes heterogeneous lung expansion because of pleural pressure D
The range of Ppleura J with lung injury
May result in significant over-distension of the ventral lung (A)
_

Homogenize the Lung!
If the alveolar distension is made more homogeneous……
…K PEEP induced asymmetrical expansion

The Prone Position
Supine Prone

Prone Position Improves Oxygenation
Rajagopalan et al; Ind. J. Crit. Care Med. 1999; 3(1): 73-5. 0
5 0
1 0 0
1 5 0
2 0 0
2 5 0
3 0 0
3 5 0
Pre P = 0.0232 Best Prone
83.8 + 27.3 torr 160.9 + 75.6 torr
PaO
2 / F
iO2 R
atio

Deforming Pressures in ARDS
LungSuperimposed
Pressure
But….Superimposed pressureis altered by…..

Deforming Pressures in ARDS
Heart & Mediastinum
Abdominal contents & caudal diaphragm;
“Pincers”

Effect of Heart & Mediastinum
AJRCCM 2000;161:1660-5
The weight of the heart and mediastinum exaggerates the gravitational collapse esp. on the left lung
In the prone position the entire mass is supported on the sternum and chest wall with no intervening lung

Chest Wall Compliance
Mobile anterior chest wall allows preferential ventilation
of ventral lung
Restriction of anterior chest makes wall compliance
homogeneous
Supine Prone

Uniform V/Q matching
Contrary to popular belief, pulmonary blood flow may not be gravity dependent (“C”)

Prone Positioning The Great Equalizer!
Decreases deforming forces (abdominal ‘pincers’ & heart)
Homogenizes chest wall compliance
Homogenizes ventilation & V/Q matching
AJRCCM 2000;161:1660-5AJRCCM1998; 157: 387-93AJRCCM 1998; 157: 1785-90

Gattinoni: Prone Trial 2001n = 152/ 152; 6-hours prone/day; 10 daysP/F <200 on 5 PEEP; <300 on 10 PEEP
No effect of Prone Positioning (?)
SUPINE
PRONE
Gattinoni et alN Engl J Med 2001; 345:568-73

Mancebo; Long ProningRCT of 136 patients76 were in prone position Aimed for 20 hrs/ day (obtained 17 hrs)Average duration of 10 days
Mortality K 58% to 43% (p=0.12)Multivariate analysis:
Higher SAPS II score, Days ventilated before studySupine posture J mortality
AJRCCM 2006; 173: 1233-9.
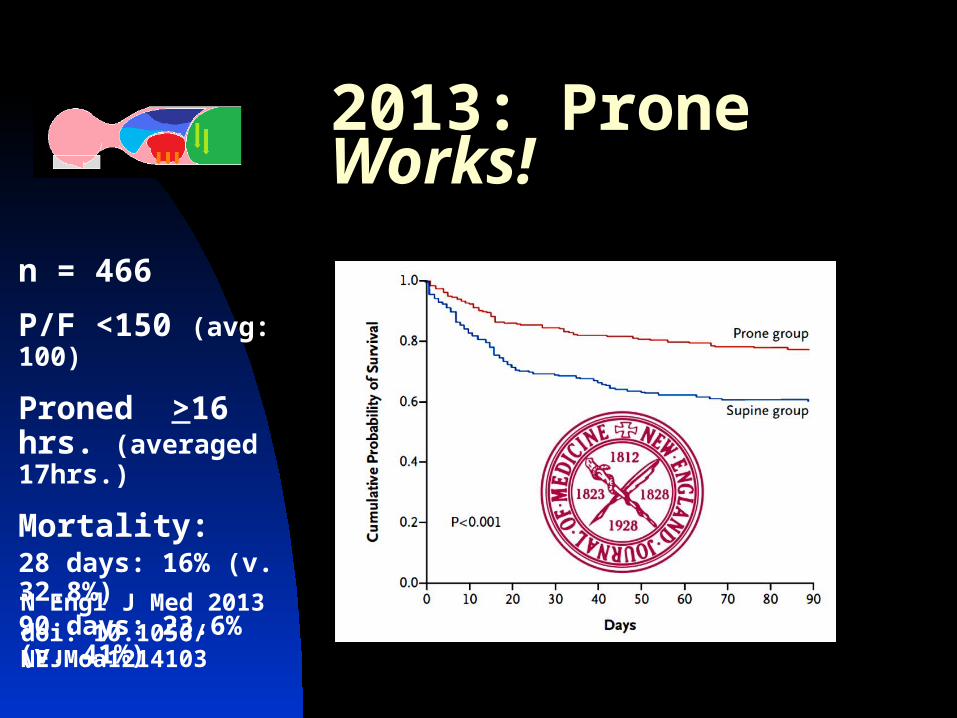
2013: Prone Works!
N Engl J Med 2013doi: 10.1056/ NEJMoa1214103
n = 466
P/F <150 (avg: 100)
Proned >16 hrs. (averaged 17hrs.)
Mortality:28 days: 16% (v. 32.8%)90 days: 23.6% (v. 41%)

Recruitment Homgenizes!
Recruitment, the application of a high Ptp, can make the alveolar distension more homogeneous
Can K PEEP induced asymmetry of distension

Lung Recruitment
No recruitment PEEP + 5 40 cm recruitment + PEEP above LIP 60 cm recruitment PEEP + 25AJRCCM 2006;174: 268 – 78.
26 patients
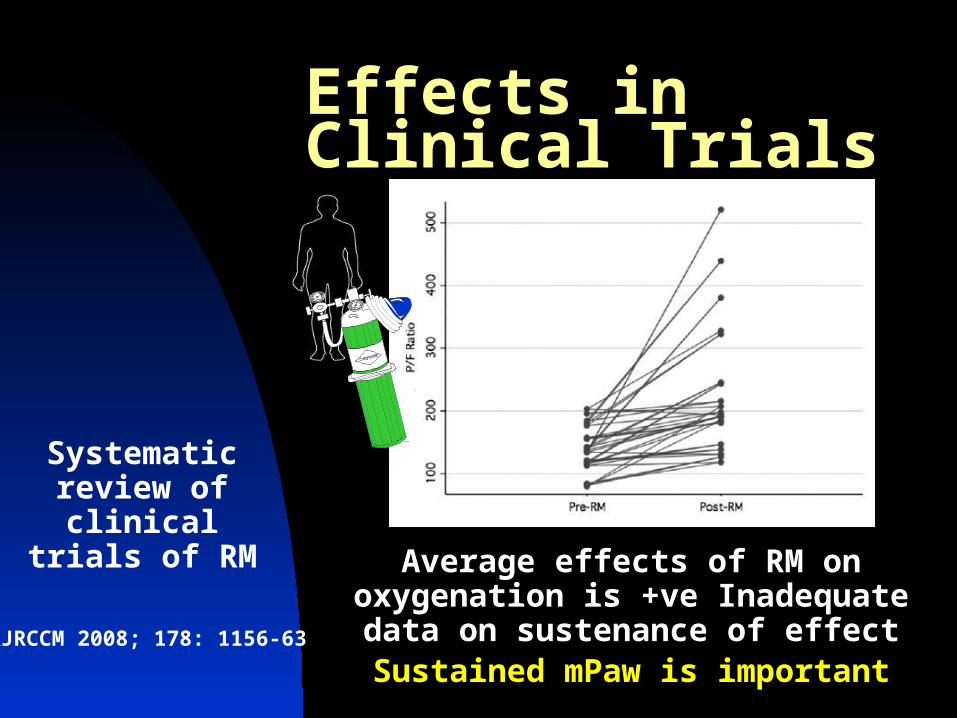
Effects in Clinical Trials
AJRCCM 2008; 178: 1156-63
Systematic review of clinical trials of
RMAverage effects of RM on oxygenation is +ve
Inadequate data on sustenance of effectSustained mPaw is important

Sustaining high mPaw
Conventional ventilation translates into higher and prolonged peak Paw which may be more detrimental to normal alveoli
Paw
Time
mPaw HFO
mPaw PCVRationale for
HFOV

Gas exchange in HFOV
Oxygenation is determined by mean Paw
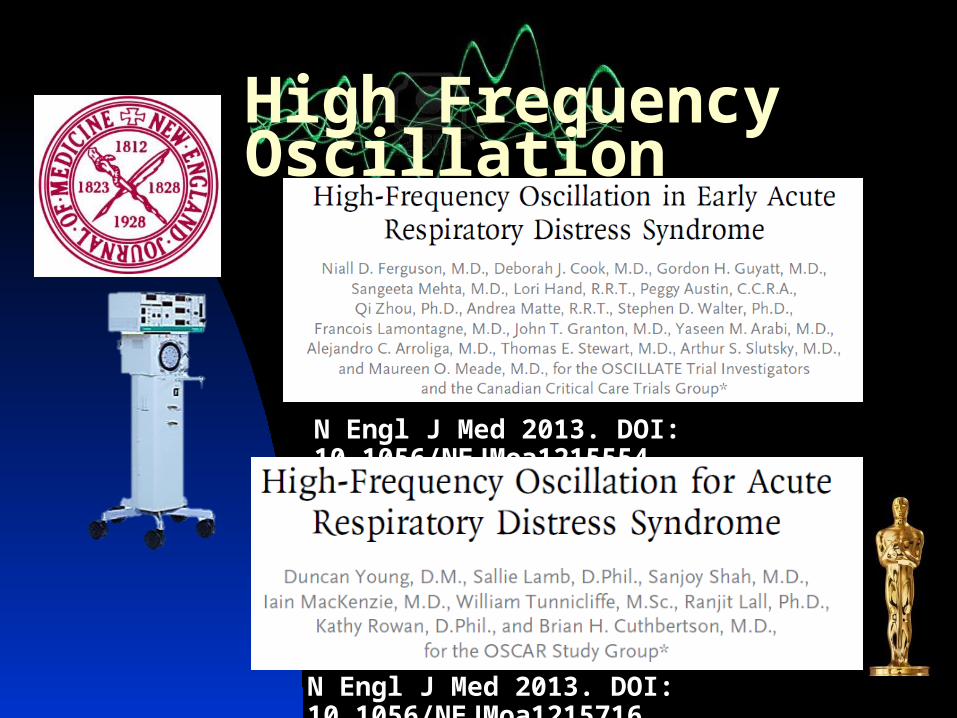
High Frequency Oscillation
N Engl J Med 2013. DOI: 10.1056/NEJMoa1215554
N Engl J Med 2013. DOI: 10.1056/NEJMoa1215716

OSCILLATE
Outcomes with HFOV
OSCAR
OSCILLATE stopped p 548 ptsOSCAR n=795

Is HFOV ineffective? One-size fits all approach No scope for titration in OSCILLATE No accounting of D in recruitability No prior recruitment in OSCAR
Were the patients ill enough to benefit? P/F ratio <200 for inclusion
Or too late; delayed inclusion in study
Greater need for sedation & HD issues
Study-related issues may account for the negative results, or…

‘Baby lung’ & Recruited lungThey are not ‘normal’
AJRCCM 2009; 180: 415 - 23Regional heterogeneity will persist even after “opening” the lung
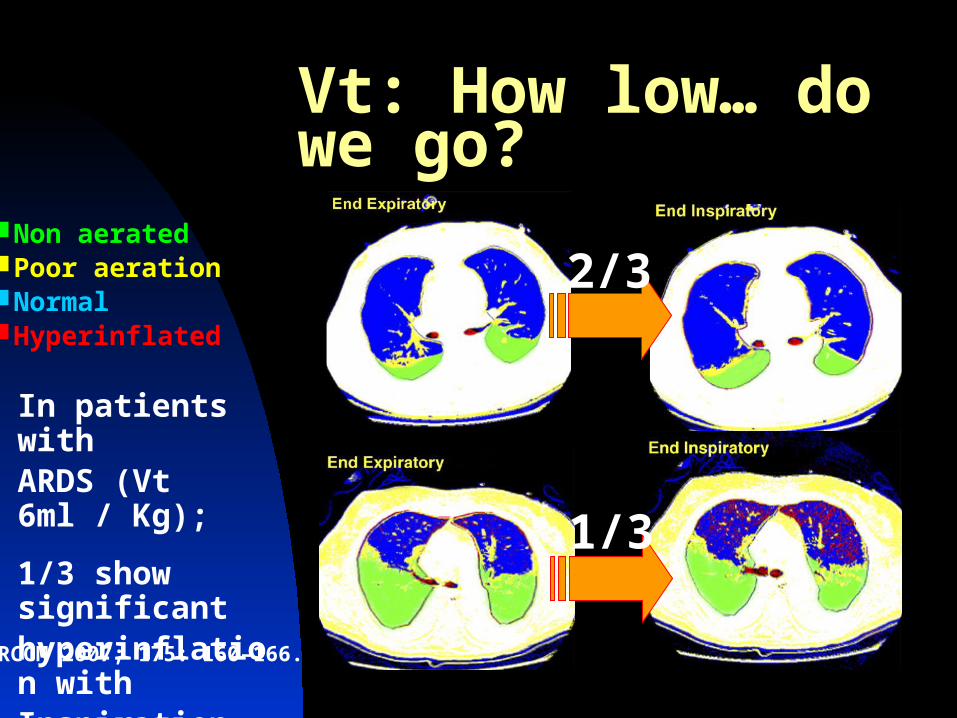
Vt: How low… do we go?
Non aeratedPoor aerationNormalHyperinflated
2/3
1/3
AJRCCM 2007; 175: 160–166.
In patients withARDS (Vt 6ml / Kg);
1/3 show significanthyperinflation with Inspiration (tidal)
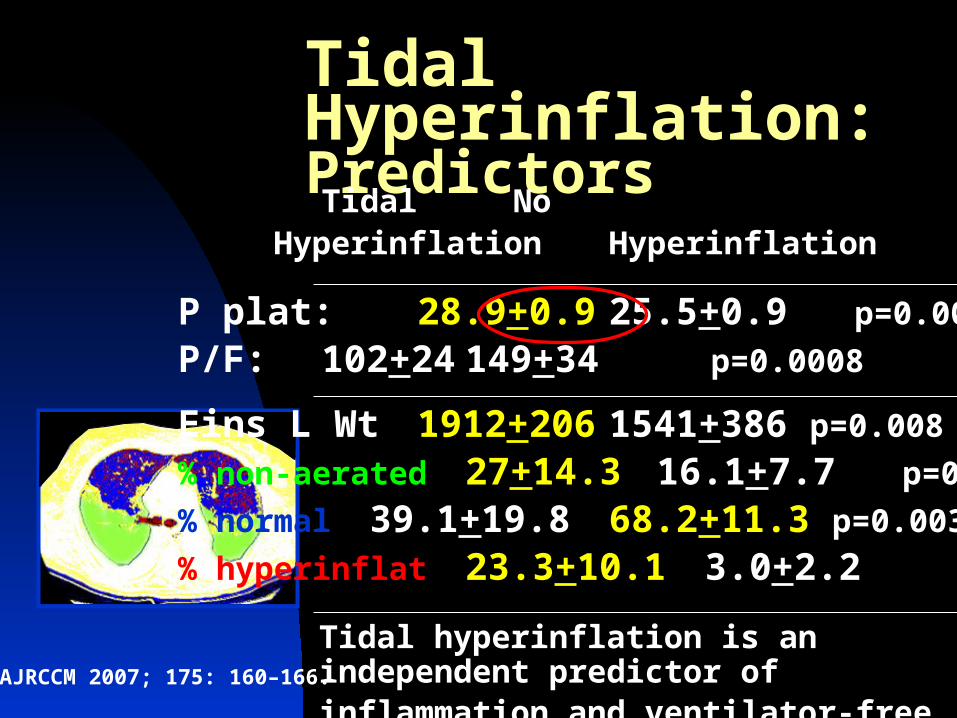
Tidal Hyperinflation: Predictors
AJRCCM 2007; 175: 160–166.
Tidal NoHyperinflation Hyperinflation
P plat: 28.9+0.9 25.5+0.9 p=0.006
P/F: 102+24 149+34 p=0.0008
Eins L Wt 1912+206 1541+386 p=0.008
% non-aerated 27+14.3 16.1+7.7 p=0.002
% normal 39.1+19.8 68.2+11.3 p=0.003
% hyperinflat 23.3+10.1 3.0+2.2 p=0.01
Tidal hyperinflation is an independent predictor of inflammation and ventilator-free days
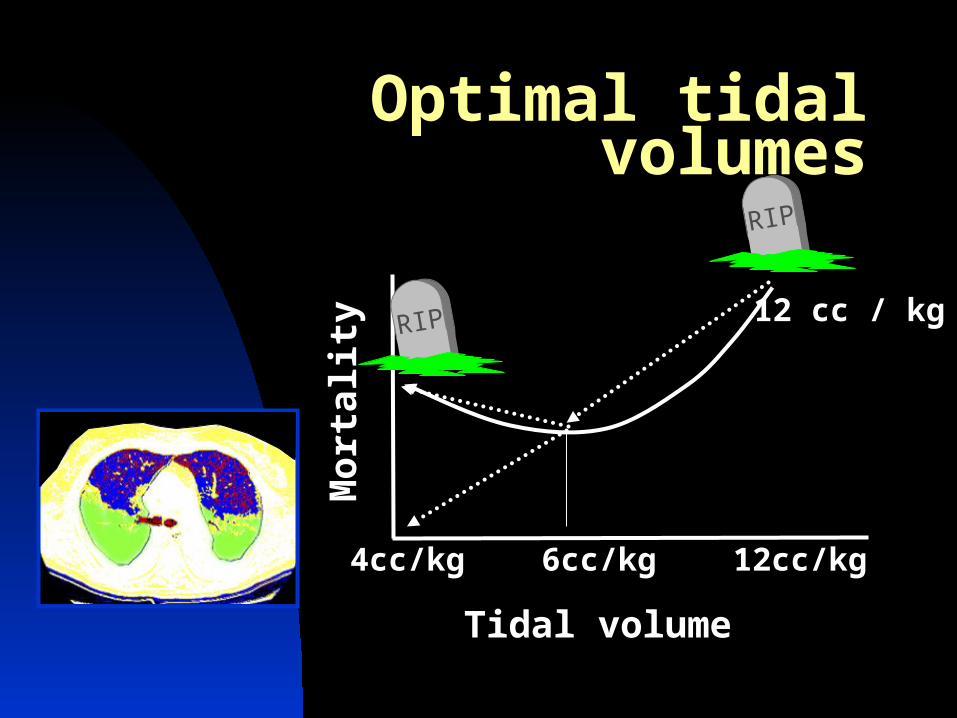
Optimal tidal volumes
12 cc / kg
RIP
Mor
talit
y
Tidal volume
4cc/kg 6cc/kg 12cc/kg
RIP

Pump-driven veno-venous ECMO
Lung “rested”:
Peak Paw = 20-25 cm H2OPEEP = 10-15 cm H2ORR = 10FiO2 = 0.3
CESAR trial

ECMO: The CESAR study90 randomized to transfer to ECMO site90 left on conventional Rx
Not ARDS only (~90%)
“Murray score” >3ph <7.20 (J CO2)
Death or severe disability at 6 months
Power adjustments made post-hoc; reduced n from 240 to 180!
Lancet 2009; 374; 1351-63

ECMO: The CESAR study
“ECMO group” “Control”Survival: 82% vs. 59% vs. 54%
63% vs. 47% (p=0.03)
Lancet 2009; 374; 1351-63
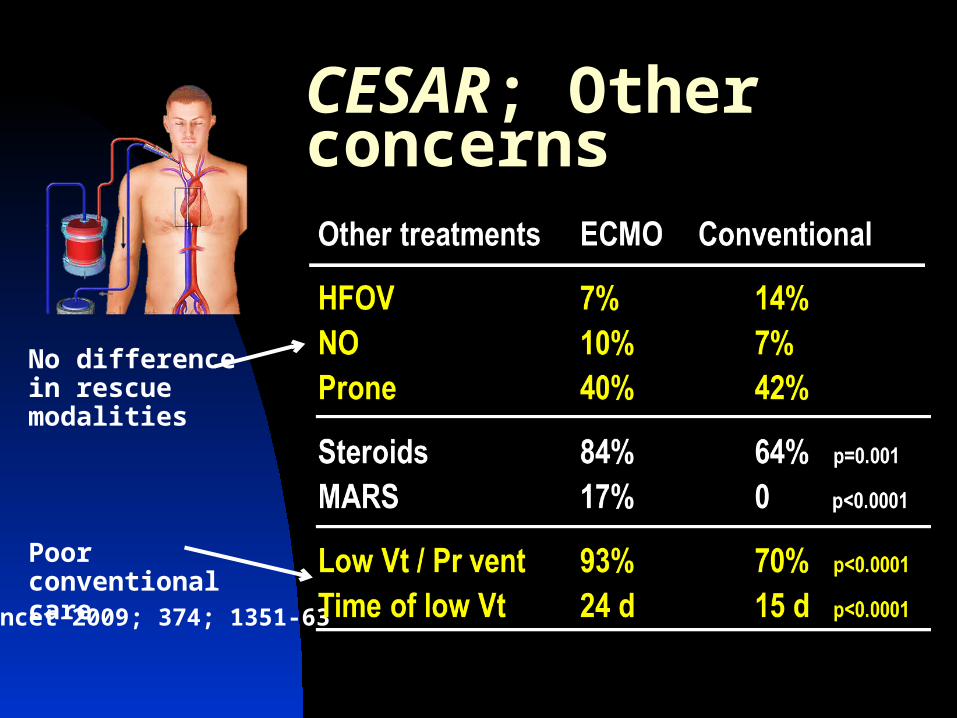
CESAR; Other concerns
Lancet 2009; 374; 1351-63
No difference in rescue modalities
Poor conventional care

CESAR; Sensitivity Analysis
Lancet 2010; 375: 550-1
Considering poor baseline care even a small J in survival in the conventionally treated patients would “annul” benefits of ECMO
2 less deaths would make results NS
Conclusion: The benefits of ECMO not clearThe benefits of expert care is obvious

PECLA; A Caution
A lot of abuse of “pumpless” systems is on the rise
They are effective for CO2 removal, not oxygenation
“Pumpless Extra-corporeal Lung Assist”

Eicosanoid Metabolism
linoleic acid (LA) - linolenic acid (ALA)C18:2-6 C18:3-3
arachidonic acid (AA)C20:4-6
eicosapentanoic acid (EPA)C20:5-3
docosahexanoic acid (DHA)C22:6-3
cyclic endoperoxids LTA4 LTA5
TXA2 TXA3 PGI2 PGI3 LTB4 LTB5 LTC4 LTC5
linoleic acid (LA) - linolenic acid (ALA)C18:2-6 C18:3-3
arachidonic acid (AA)C20:4-6
eicosapentanoic acid (EPA)C20:5-3
docosahexanoic acid (DHA)C22:6-3
cyclic endoperoxids LTA4 LTA5
TXA2 TXA3 PGI2 PGI3 LTB4 LTB5 LTC4 LTC5
W-6 W-3
W-3 fatty acids produce
eicosanoids with lower
inflammatory potential

The Formula

W-3 Fatty Acids in ARDS
3 RCTs included (author’s own paper too)
K Mortality OR: 0.40 (0.24-0.68) ventilation SMD: 0.56 (0.32-0.79) new organ failure OR: 0.17 (0.08-0.34) ICU stay SMD: 0.51 (0.27-0.74)
Establishes efficacy of specific formula (Oxepa ®) JPEN 2008; 32: 596-605

ARDSnet: W-3 Fatty Acids
JAMA 2011; 306: 1574-81

W-3 FA Supplement
W-3 supplements trending to worse outcome compared to low-fat, high-CHO feed
JAMA 2011; 306: 1574-81
n=272(stopped for futility)

Thank you for your patient
listening!