
Acute renal failure
73
Dr. Suresh Singh;MCh Urology(std.) JIPMER;Puducherry
-
Upload
drvinitasingh -
Category
Documents
-
view
40 -
download
7
Transcript of Acute renal failure

Dr. Suresh Singh;MCh Urology(std.)JIPMER;Puducherry

Definition ARF is a sudden and usually reversible decrease in
the glomerular filtration rate (GFR) occurring over a period of hours to days
.The term “Acute Kidney Injury” now replaces the
term ARF; the term ARF should now be restricted to patients who have AKI and “need renal replacement therapy”.

Acute kidney injury classification -ADQI

RIFLE criteria

STAGING OF AKI



ACS:PRE-OP PREDICTORS OF AKIAge>= 56Male sexEmergency SurgeryIntraperitoneal SurgeryDM needing OHA or Insulin therapyActive CHFAscitesHypertensionMild to moderate renal insufficiency.

Serum Creatinine as a marker for AKI and GFR
Normal S.Creatinine is 0.6-1.2mg/dl and is the most commonly used parameter to assess renal function.
Unfortunately the correlation between S.Creatinine concentration and GFR may be confounded by several factors.

Ser
um
Cre
atin
ine
(mg
/dl)
GFR (ml/min per 1.73m2)
1.0
0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
40 60 80 100 120 140 160 180200

There is abrupt drop in GFR but the S.Cr. does not start going up for 24 or 36 hours after the acute insult .
40
80
0
GFR(mL/min)
0 7 14 21 28
4
Days
2
0
6
Serum Creatinine(mg/dL)
Relationship between GFR and serum creatinine in ARF

Creatinine is not an ideal marker
1. Creatinine excretion is dependent on renal factors independent of function:Certain medications such as cimetidine and
trimethoprim interfere with proximal tubular creatinine secretion and may cause rise in S. creatinine without fall in GFR.

2. S.Creatinine is dependent on nonrenal factors independent of renal functionS.Creatinine is dependent on muscle mass,
infection, volume of distribution, age, gender, race, body habitus, diet, presence of amputations.
Eg. S. Creatinine of 1.2mg/dl in a 40kg elderly signifies severe reduction of GFR while the same value in a 100kg represents a normal renal function
3. Creatinine production and excretion must be in a steady state before creatinine may be used in any formula for the estimation of GFR.

NEW MARKERCystatin C –protein
Produced by nucleated cells
Filtered and completely reabsorbed
Changes in serum levels occur sooner

NOVEL BIOMARKERS1. IL- 18
2.KIM-1
3.Gro α/KC
4.NGAL-neutrophil gelatinase associated lipocalin
5.NHE-3

Spectrum of AKIPrerenal : renal hypoperfusion
Renal (Intrinsic) :GlomerularTubularVascular Interstitial
Post renal: obstruction
InjuryInjury

Generalized or localized reduction in RBF
HaemorrhageHaemorrhageVolume depletionVolume depletion
( vomiting,( vomiting,diarrhoea,diarrhoea,
inappropriate inappropriate diuresis, burns)diuresis, burns)
Cardiogenic shockCardiogenic shockDistributive Distributive shockshock
(sepsis, (sepsis, anaphylaxis)anaphylaxis)
Cardiac failureCardiac failureHepatic cirrhosisHepatic cirrhosis
Nephrotic syndromeNephrotic syndrome
NSAIDs NSAIDs ACEI / ARBsACEI / ARBs
AAAAAARAS /occlusionRAS /occlusion
Reduced GFR
PRE-RENAL (Hemodynamic) AKI
PRERENAL AKI

Pre renal AKI characteristics:Decreased RBF and GFR
Increased Na and H2O reabsorption
Oliguria
High Uosm (>500), low UNa ( FeNa <1%)
Elevated BUN / S.Cr. Ratio
Bland urinary sediments

TubularTubularGlomerularGlomerular VascularVascularInterstitialInterstitial
ATNATN
Ischemia (50%)Ischemia (50%)Toxins (30%)Toxins (30%)
Ac. Interstitial Ac. Interstitial nephritisnephritis
Drug inducedDrug induced - - NSAIDs,NSAIDs,
antibioticsantibioticsInfiltrative -Infiltrative -lymphomalymphoma
Granulomatous- Granulomatous- sarcoidosis, sarcoidosis, tuberculosistuberculosis
Infection relatedInfection related - - post-infective, post-infective, pyelonephritispyelonephritis
Vascular Vascular occlusionsocclusions
- - Renal artery Renal artery occlusion occlusion
- Renal vein - Renal vein thrombosisthrombosis
- Cholesterol - Cholesterol emboliemboli
Ac.GN Ac.GN
–post-infectious,post-infectious,– SLE,SLE,–ANCA associated,ANCA associated,–anti-GBM diseaseanti-GBM disease–Henoch-Schönlein Henoch-Schönlein purpurapurpura–Cryoglobulinaemia,Cryoglobulinaemia,–Thrombotic Thrombotic microangiopathy microangiopathy
•TTPTTP•HUSHUS
5%5%
85%85%
8 -12%8 -12%
< 2%< 2%

ATN
CAUSES:
1.Ischemia
2.Infection with or without sepsis
3.Toxins –exogenous- radiocontrast,ampho-B
aminoglycosides
-endogenous-rhabdomyolysis,
hemolysis

ATN cont…. Common sites –
S3 segment of the proximal tubule
Thick ascending limb (more glycolytic machinery for ATP synthesis)
Medullary blood flow -- 10% to 15% of total RBF
Relative hypoxia in the outer medulla ;

PaO2 50 mm of
Hg
PaO2 20 mm of
Hg
10 mm of Hg
PaO2


PATHOPHYSIOLOGY OF ISCHEMIC ARF


Phases of ATN Initiation : - hours to days GFR declines Extension :- continuing ischemic injury and
inflammation GFR low Maintenance:- 1-2 weeks GFR stabilises uremic complications may arise Recovery :- GFR rises

ATN characteristics:Decreased GFR, Oliguria
Decreased Na reabsorption
Low Uosm (< 350), High UNa (FeNa >1%)
Elevated BUN / S.Cr.
Urinary sediments- Muddy pigmented granular casts

MORTALITY PREDICTORS IN ATNMale genderOliguriaMechanical
ventilationAcute MICVAImmunosupression
Leading cause of Death being:
Bronchopulmonary infections,sepsis ,CV disease and bleeding disorders.

Intra-luminalIntra-luminal•Stone,Stone,•Blood clots, Blood clots, •Papillary Papillary necrosisnecrosis
•Pelvic Pelvic malignanciesmalignancies•Prolapsed uterusProlapsed uterus•Retroperitoneal Retroperitoneal fibrosisfibrosis
IntrinsicIntrinsic
Intra-mural Intra-mural •Urethral stricture, Urethral stricture, •BPH, BPH, •Carcinoma prostate,Carcinoma prostate,• Bladder tumour,Bladder tumour,• Radiation fibrosisRadiation fibrosis
ExtrinsicExtrinsic
Post-renal Urinary outflow tract obstruction

ComplicationsMETABOLIC:
hyperkalemia, hyponatremia,
hypocalcemia, hyperphosphatemia,
hyperuricemia, metabolic acidosisCVS:
pericarditis/effusion , hypertension ,MI,
arrhythmias, pulmonary edemaGIT:
nausea, vomiting, malnutrition ,GI hemorrhage
CNS:
asterixis ,mental changes ,seizures
INFECTIONS:
pneumonia ,sepsis

Approach to a patient with AKI
Differentiate acute or chronic renal failure
Distinguishing between acute and chronic renal
failure is important, as the approach to these
patients differs greatly.


Factors that suggest chronicity :
Long duration of symptoms,
Absence of acute illness, anaemia,
hyperphosphatemia, and hypocalcaemia,
Previous Serum creatinine measurements
Small kidneys on ultrasound (except for in -Diabetes, PCKD, Urinary Tract Obstruction)

Exclude obstruction
Urological evaluation
Renal stones,
Symptoms of bladder outflow obstruction- Prostate
enlargement Prolapsed uterus
A palpable bladder.

CONTD ...
X-ray KUB
Renal ultrasonography – detect dilatation of the renal
pelvis and calyces
CT Scan

Evidence of renal parenchymal disease
(other than ATN)
History and examination (systemic features)
Urine dipstick
Urine microscopy (red cells, red cell casts,
eosinophils, proteinuria)

Signs of major “vascular occlusion”
Loin pain
Macroscopic haematuria
Anuria
Renal asymmetry

Assess the volume status of the patient:
Pulse,
JVP,
postural blood pressure,
daily weights,
fluid balance/fluid challenge

INVESTIGATIONS BiochemistryBlood urea, creatinine,
electrolytes,
Blood gas analysis.
Urine osmolality/sodium


Sr.Creatine kinase, myoglobin in urine
Markedly elevated CK and myoglobinuria suggests rhabdomyolysis
Serum immunoglobulins, serum protein electrophoresis, Bence Jones proteinuria
Monoclonal band on serum protein
electrophoresis, and Bence Jones proteinuria suggest multiple myeloma

Urine analysis:
Dipstick for blood, protein - Suggests a renal inflammatory process
Microscopy for cells, casts, crystals

RBC s Present in glomerulonephritis , vasculitis , HUS TTP scleroderma crisis

Casts:Hyaline –prerenal ARF
Granular –ATN (muddy brown)
Red blood cell casts –glomerulonephritis,vasculitis
malignant hypertension
WBC casts- AIN, pyelonephritis ,leukemic or
lymphomatous infiltrates

Crystals Urate crystals – acute urate nephropathy
Oxalate crystals –ethylene glycol ingestion /acyclovir/
indinavir
Eosinophiluria > 5 % of WBC s AIN ,atherothrombotic
disease

HaematologyFull blood count, blood film:
Eosinophilia may be present in acute interstitial nephritis,
cholesterol embolization, or vasculitis (CSS)
Thrombocytopenia and red cell fragments suggest thrombotic microangiopathy –TTP, HUS
Coagulation studies Disseminated intravascular coagulation associated
with sepsis

ImmunologyAntinuclear antibody (ANA) , Anti-double
stranded (ds) antibody - ANA positive in SLE and other autoimmune
disorders;DNA antibodies anti-ds DNA antibodies more specific for SLE
C3 & C4 complement concentrations-Low in SLE, acute post infectious
glomerulonephritis, CryoglobulinemiaASO and anti-DNAse B titres
High after streptococcal infection

Immunology...ANCA
p-ANCA - Anti PR3 antibodies c-ANCA - Anti MPO antibodies
Associated with systemic vasculitis - Wegener’s granulomatosis; CSS, Microscopic polyangiitis.
AntiGBM antibodies Present in Goodpasture’s disease

SerologyHepatitis B and C, HIV serology
Important implications for infection control within dialysis area
RadiologyRenal ultrasonography
For renal size, symmetry, evidence of obstruction

Management principles in ARF
Identify and correct pre-renal and post-renal factors
Optimise cardiac output and RBF :
Stop/adjust the dose of nephrotoxic drugs (ACEI, ARBs,
NSAIDs)

Management principles...
Accurately monitor fluid balance and daily body weight
Identify and treat acute complications
Hyperkalaemia,hypertensionAcidosis,Pulmonary oedema

Management of complications Volume overload –salt restriction < 1 – 1.5 g/d water restriction -< 1
litre /d diuretics
Hyponatremia –restriction of oral & intravenous fluids
Hyperkalemia – K binding resins ,glucose + insulin
Ca gluconate ,soda bicarb.Metabolic acidosis – soda bicarb ., if < 15 meq Hyperphosphatemia – PO4 binders –sevalamer

Contd….Hypocalcemia –calcium carbonate
Nutrition –restriction of dietary protein < 0.8 g/kg /d
calories – 25-30 kcal / d enteral nutrition preferred

Contd …
Identify and aggressively treat infection;
Minimise indwelling lines
Identify and treat bleeding tendency:
Prophylaxis - proton pump inhibitor or H2 antagonist, transfuse if required

Absolute indication for dialysis Evidence of uremia ;
Intractable volume overload
Hyperkalemia
Severe metabolic acidosis refractory to medical
measures



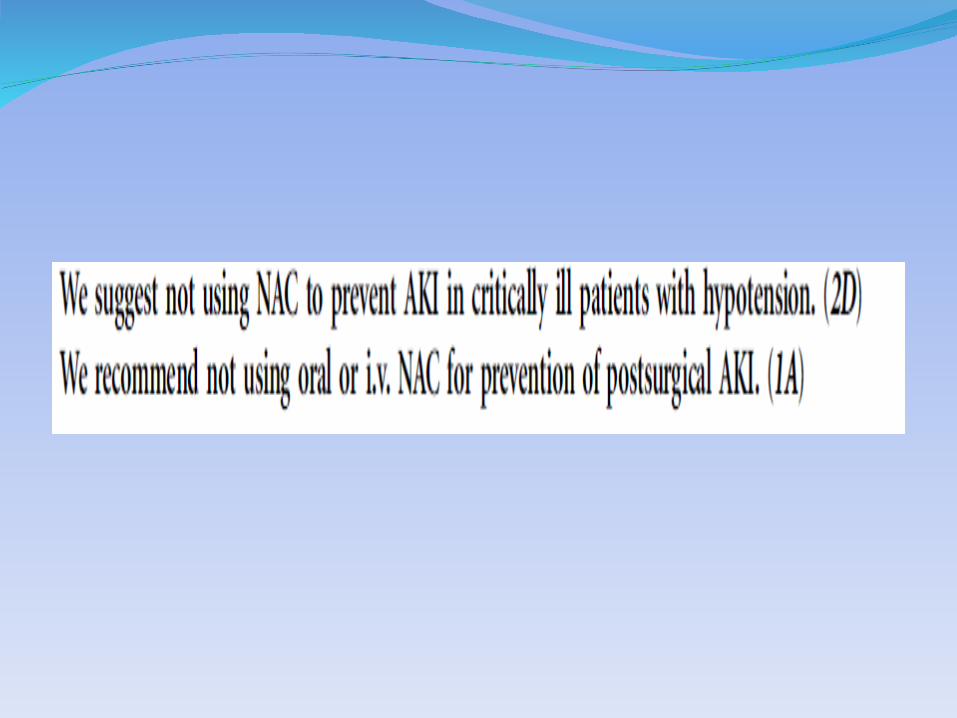
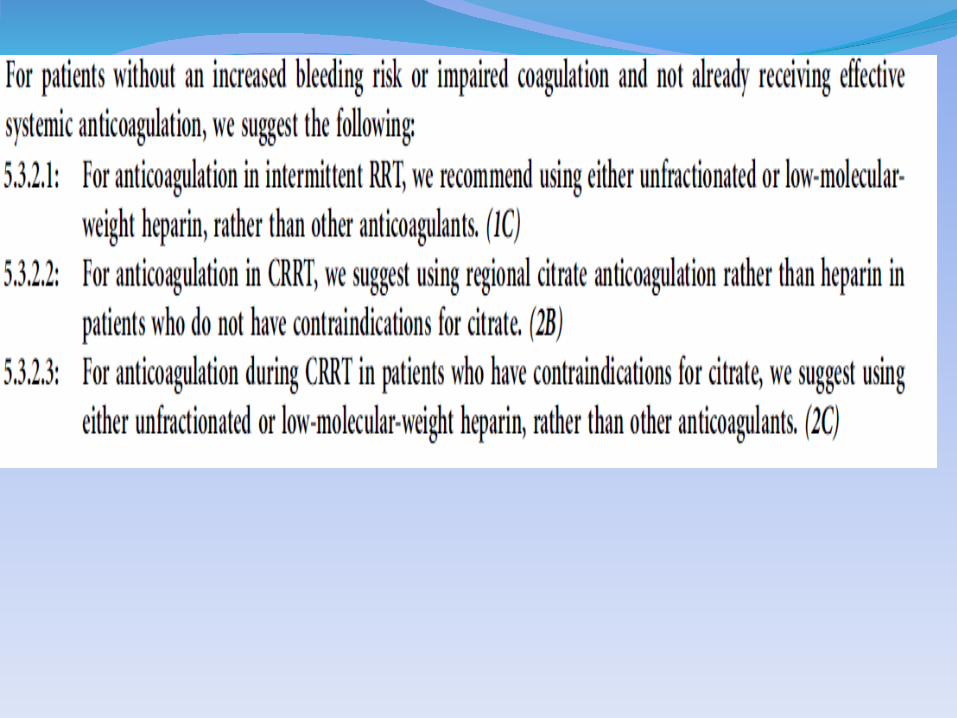
RECOMMENDATIONS


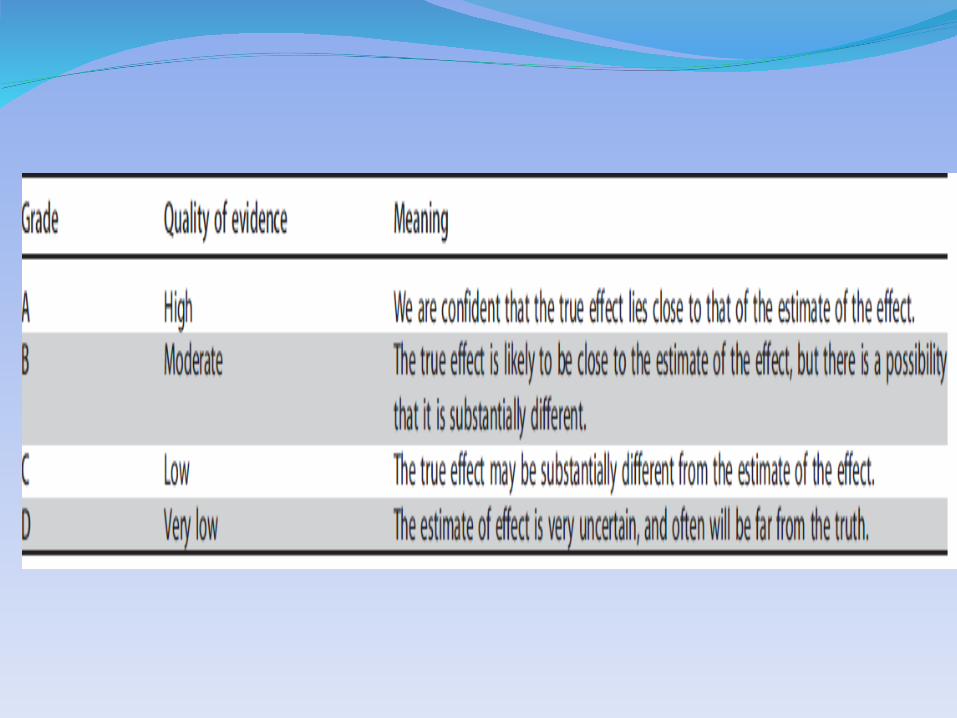

KIDGO RECOMMENDATIONS









Thank you Thank you






