
Acute renal failure
29
Acute Renal Failure By: Dr.Leena Hafeez
-
Upload
leena-hafeez -
Category
Health & Medicine
-
view
31 -
download
4
Transcript of Acute renal failure
Acute Renal Failure
By:
Dr.Leena Hafeez
Definition
Sudden and usually reversible loss of renal function which develops over days or weeks accompanied by reduction in urine volume.

Etiology
The etiology of ARF can be divided into 3 categories.
PRE-RENAL RENAL POST RENAL
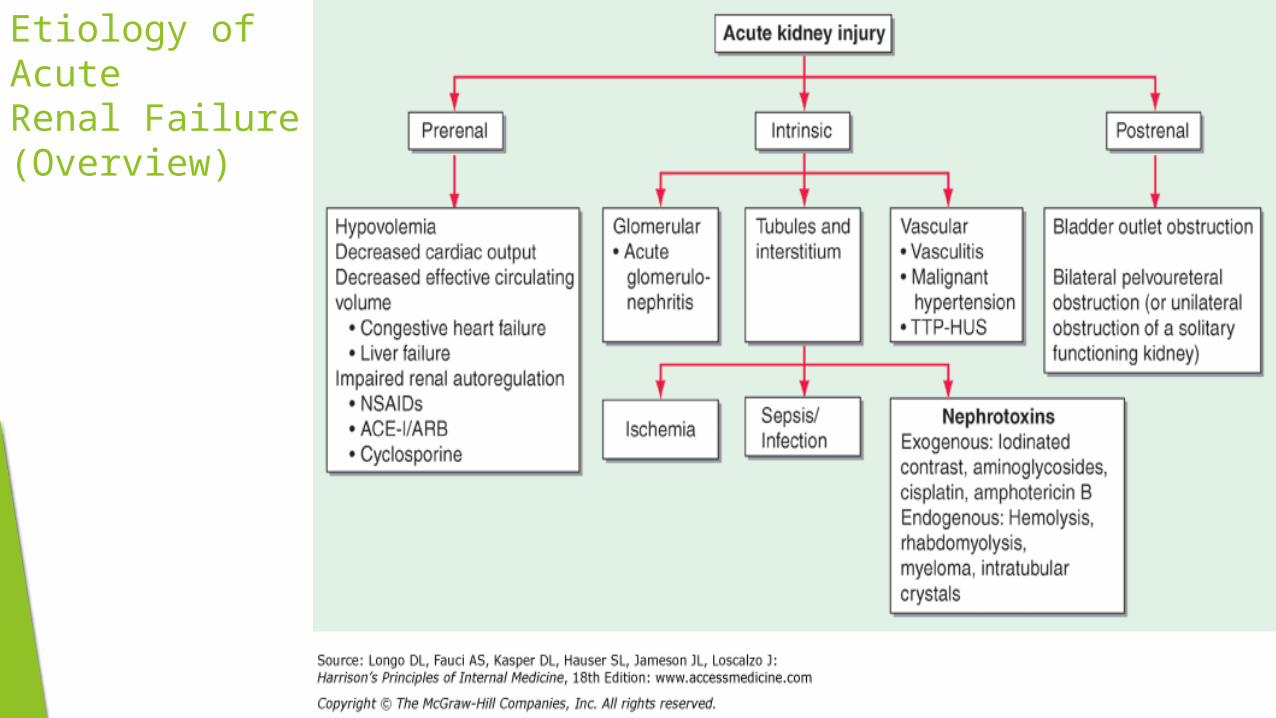
Etiology of AcuteRenal Failure(Overview)
Pre Renal Acute Renal Failure
Causes: Pre-renal causes of ARF include
Heart Failure.
Blood/Fluid loss as in major surgery,trauma,dehydration
sec. to severe diarrhea and vomiting.
Renal artery stenosis/Occlusion.
Diseases Affecting the arterioles.
Pathogenesis:
In circumstances which dec the perfusion pressure(Heart failure,Shock,Hypovolemia),Kidneys maintain their perfusion by constriction of renal vasculature and selective constriction of efferent arterioles
Drugs like NASIDs and ACE inhibitors affect these compensatory mechanisms.
Prolonged hypo perfusion and drug toxicity halt these compensatory mechanisms leading to acute decline in GFR
History and physical Examination
History: History of Vomiting,Diarrhea,Surgery or Trauma with blood loss and history of medications including diuretics,NSAIDs, ACE inhibitors, and ARBs may be present.
Examination: Physical signs of poor peripheral perfusion may be present. Orthostatic hypotension,Tachycardia,Reduced jugular venous pressure, decreased skin turgor, and dry mucous membranes are often present in prerenal azotemia
Intrinsic Acute Renal Failure
CausesIntrinsic causes of Acute renal failure include
Acute tubular necrosis:
May occur as a result of Ischemia,sepsis or
Nephrotoxic drugs.
Glomerular diseases:
Primary or Secondary glomerulonephritis
Vascular diseases:
E.g. Vasculitis or malignant hypertension
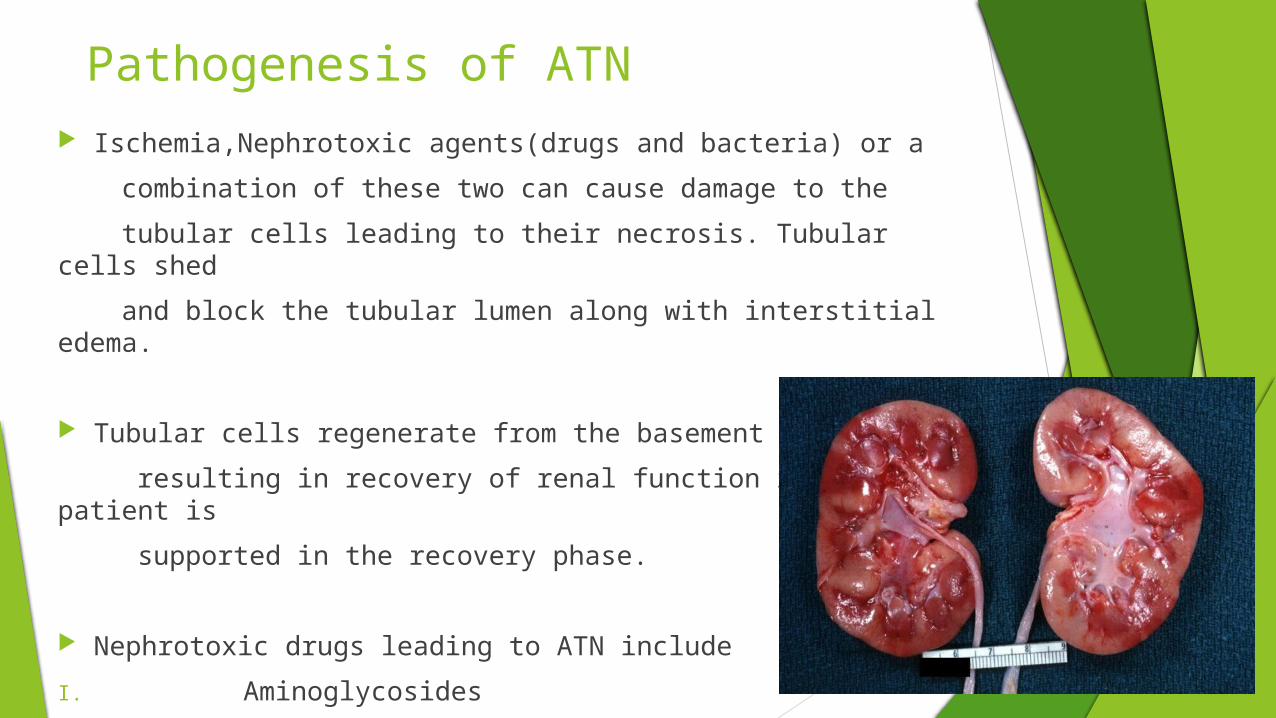
Pathogenesis of ATN Ischemia,Nephrotoxic agents(drugs and bacteria) or a
combination of these two can cause damage to the
tubular cells leading to their necrosis. Tubular cells shed
and block the tubular lumen along with interstitial edema.
Tubular cells regenerate from the basement membrane
resulting in recovery of renal function if the patient is
supported in the recovery phase.
Nephrotoxic drugs leading to ATN include
I. Aminoglycosides
II. Cisplatin
III. Amphotericin B
Post renal Acute Renal Failure
Causes:
Post renal ARF occurs secondary to any obstruction in the urinary tract
which include:
Renal stones
Tumors
Benign prostatic hyperplasia
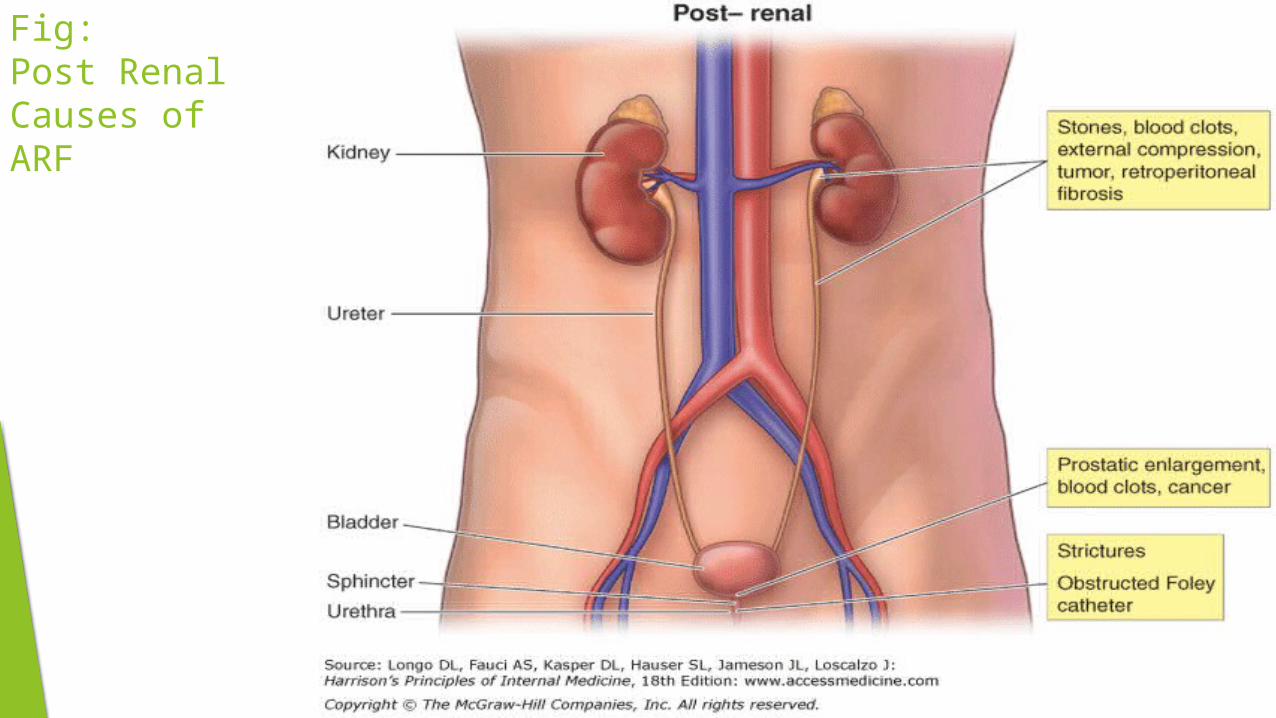
Fig:Post Renal Causes of ARF
History and Physical Examination
Colicky flank pain radiating to the groin suggests acute ureteric
obstruction.
Nocturia and urinary frequency or hesitancy can be seen in prostatic disease.
Abdominal fullness and suprapubic pain can accompany massive bladder enlargement.
Definitive diagnosis of obstruction requires radiologic investigations.
Phases of Acute Renal Failure
Phases Acute Renal Failure is divided into 4 phases
Initiation Phase:
Oliguric phase:
Lasts 7-14 days. Urine output <400ml/day.
Diuretic Phase:
Urine output can reach up to 2500ml/day. Adequate fluid replace
required for good recovery
Recovery Phase:
GFR returns to normal. Renal parameters decline towards the normal
range

Investigations
Blood Counts Full Blood Count:
Anemia may show CKD
Low platelets may indicate DIC and sepsis
Urea and Creatinine:
Daily raise may exceed up to 5mmole/day
Serum Electrolytes:
Hyperkalemia
Albumin:
Low Serum Albumin in nephrotic syndrome and sepsis
Urine Analysis
Proteinuria may indicate glomerular disease
Hematuria shows obstructive lesions, stone or glomerulonephritis
Leucocytes may show infection
Crystals can be specific of drugs or uric acid
Radiological Investigations
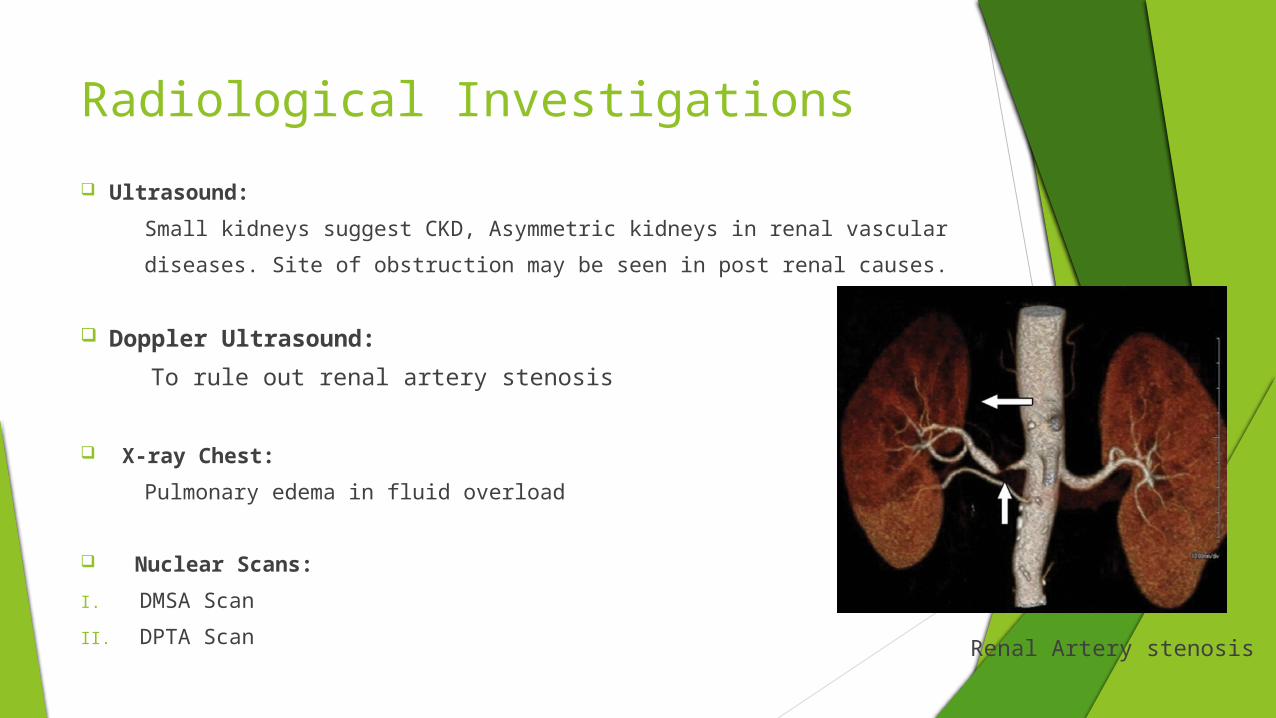
Ultrasound:
Small kidneys suggest CKD, Asymmetric kidneys in renal vascular
diseases. Site of obstruction may be seen in post renal causes.
Doppler Ultrasound:
To rule out renal artery stenosis
X-ray Chest:
Pulmonary edema in fluid overload
Nuclear Scans:
I. DMSA Scan
II. DPTA Scan
Renal Artery stenosis
Specific Investigations:
Renal Biopsy:
For glomerular diseases, interstitial nephritis
Serology:
For infections like post streptococcal glomerulonephritis,
Leptospirosis.

Management
Management1.Treat the underlying cause:
Pre renal failure:
Restore the blood volume by transfusing Blood, Plasma or isotonic
saline carefully monitoring CVP and PWP
Renal Cause of ARF:
I. ATN responds to restoration of renal perfusion
II. Immunosuppressive therapy for glomerulonephritis
Post renal cause:
Prompt relive of obstruction restores the renal functions.
Management2.Fluid and Electrolyte Balance:
Strict monitoring of Intake and output
Daily fluid intake should be equal to output+500ml
Additional replacement required in case of abnormal losses like Diarrhea and Vomiting.
3.Hyperkalemia:
Potassium concentration >6mmole/L can cause serious
arrthymias.Immediate intervention required
4.Metabolic Acidosis:
Restoration of blood volume will correct acidosis. Treat with sodium
bicarbonate(50ml of 8.4%) in severe cases.
Management5.Proteins and energy Intake:
Protein restriction to less than 40g/day.
Major source of energy should be fats and carbohydrates
Enteral and parenteral nutrition may be required in patients with hyper catabolic states(e.g. burns and sepsis)
6.Infection Control:
Prompt diagnosis and treatment with antibiotics required
7.Avoidance of nephrotoxic drugs:
NSAIDS and ACE inhibitors may prolong ARF and should be avoided.
8.Renal replacement therapy:
May be required as supportive management
Prognosis
Prognosis of ARF depends upon the severity of Underlying cause
In Uncomplicated ARF secondary to hemorrhage and Drugs mortality is low
ARF associated with Serious Infections and MOF mortality is 50-70%

Thank You






