Acute Pericarditis Emory Family Medicine Acute Pericarditis Emory Family Medicine Susan Schayes M.D....
32
Acute Pericarditis Acute Pericarditis Emory Family Medicine Emory Family Medicine Susan Schayes M.D. Susan Schayes M.D. Assistant Professor-CT Assistant Professor-CT Family Medicine, Emory Family Medicine, Emory University School of Medicine University School of Medicine
-
Upload
junior-fowler -
Category
Documents
-
view
229 -
download
2
Transcript of Acute Pericarditis Emory Family Medicine Acute Pericarditis Emory Family Medicine Susan Schayes M.D....
Acute Pericarditis Acute Pericarditis Emory Family Medicine Emory Family Medicine
Susan Schayes M.D.Susan Schayes M.D.
Assistant Professor-CTAssistant Professor-CT
Family Medicine, Emory University School Family Medicine, Emory University School of Medicineof Medicine

The PericardiumThe Pericardium
A fibroelastic sac composed of visceral and A fibroelastic sac composed of visceral and parietal layers parietal layers
Both these layers are separated by a pericardial Both these layers are separated by a pericardial cavity.cavity.
The cavity normally contains 15 to 50 ml of The cavity normally contains 15 to 50 ml of straw-colored fluid. straw-colored fluid.
Visceral layer is in contact with the Visceral layer is in contact with the epicardium (ST elevation)epicardium (ST elevation)

The Clinical problemThe Clinical problem
Can be an isolated entity or part of a systemic Can be an isolated entity or part of a systemic diseasedisease
0.1% of all hospitalized patients0.1% of all hospitalized patients 5% of ER visits for chest pain without an MI5% of ER visits for chest pain without an MI
Etiology-Acute PericarditisEtiology-Acute Pericarditis InfectiousInfectious
Viral : Coxsackie, Echo, EBV, Influenza, HIVViral : Coxsackie, Echo, EBV, Influenza, HIV Bacterial: TB, staph, hemophilus, pneumococcal, salmonellaBacterial: TB, staph, hemophilus, pneumococcal, salmonella Fungal/other: histo/blasto/coccidio, rickettsialFungal/other: histo/blasto/coccidio, rickettsial
RheumatologicRheumatologic SLE, Sarcoid, RA, Dermatomyositis, Ankylosing Spondylitis, Scleroderma, SLE, Sarcoid, RA, Dermatomyositis, Ankylosing Spondylitis, Scleroderma,
PANPAN NeoplasticNeoplastic
Primary: angiosarcoma, mesotheliomaPrimary: angiosarcoma, mesothelioma Metastatic: breast, lung, lymphoma, melanoma, leukemiaMetastatic: breast, lung, lymphoma, melanoma, leukemia
ImmunologicImmunologic Celiac sprue, Inflammatory Bowel DiseaseCeliac sprue, Inflammatory Bowel Disease
DrugDrug Hydralazine, ProcainamideHydralazine, Procainamide
OtherOther MI, MI, Dressler’sDressler’s, Post Pericardiotomy, Chest Trauma, Aortic dissection, Post Pericardiotomy, Chest Trauma, Aortic dissection UremicUremic, Post Radiation, Post Radiation IDIOPATHICIDIOPATHIC

Other PearlsOther Pearls
Viral and Autoimmune causes constitute > 50% of Viral and Autoimmune causes constitute > 50% of cases of acute pericarditiscases of acute pericarditis
Pericardial disease is the most frequent Pericardial disease is the most frequent cardiovascular manifestation of AIDScardiovascular manifestation of AIDS
The typical diffuse ST elevation is not seen in uremic The typical diffuse ST elevation is not seen in uremic pericarditis,in which there is fibrin deposition in the pericarditis,in which there is fibrin deposition in the parietal layer but no epicardial inflammation.parietal layer but no epicardial inflammation.

Clinical PresentationClinical Presentation
Chest painChest pain Pericardial friction rubPericardial friction rub Diffuse ST segment elevation on EKGDiffuse ST segment elevation on EKG Pericardial effusionPericardial effusion
Presence of at least two of the above features is necessary to make the diagnosis

Chest PainChest Pain
Retrosternal in locationRetrosternal in location Sudden in onsetSudden in onset Pleuritic and sharp in naturePleuritic and sharp in nature Exacerbated by inspiration Exacerbated by inspiration Worsens when supine and improves upon sitting Worsens when supine and improves upon sitting
upright or leaning forward. upright or leaning forward. Can often radiate to the neck, arms, or left shoulder.Can often radiate to the neck, arms, or left shoulder. Radiation to one or both trapezius muscle ridges, Radiation to one or both trapezius muscle ridges,
suggests a probable pericarditis (phrenic nerve suggests a probable pericarditis (phrenic nerve traverses the pericardium)traverses the pericardium)

Pericardial Friction RubPericardial Friction Rub
Present in 85% of cases of pericarditisPresent in 85% of cases of pericarditis Highly specific with a variable sensitivityHighly specific with a variable sensitivity A high-pitched scratchy or squeaky sound best heard with the A high-pitched scratchy or squeaky sound best heard with the
diaphragm at the LSB with the patient leaning forward.diaphragm at the LSB with the patient leaning forward. Corresponds temporally to the movement of heart within the Corresponds temporally to the movement of heart within the
pericardial sac.pericardial sac. Has 3 components, which correspond to Has 3 components, which correspond to atrial systole, atrial systole,
ventricular systole, and early diastole.ventricular systole, and early diastole. Pericardial friction rub is audible throughout the respiratory Pericardial friction rub is audible throughout the respiratory
cycle, whereas the pleural rub disappears when respirations cycle, whereas the pleural rub disappears when respirations
are on hold.are on hold.

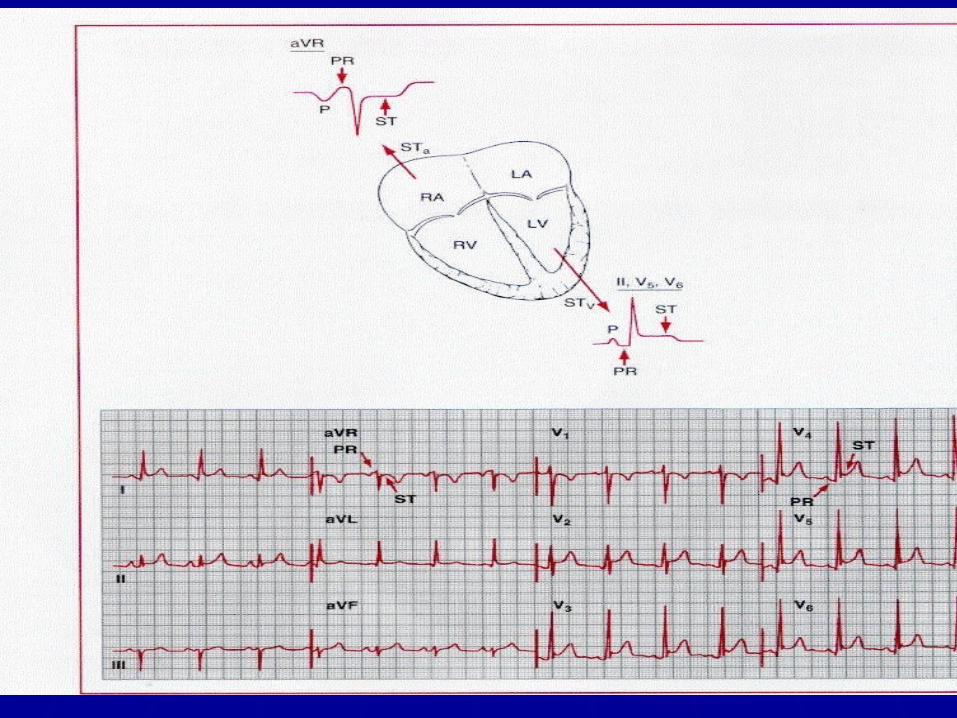
EKG in PericarditisEKG in Pericarditis
Widespread upward concave ST-segment Widespread upward concave ST-segment elevation and PR-segment depression elevation and PR-segment depression
If the ratio of ST-segment elevation to T-wave If the ratio of ST-segment elevation to T-wave amplitude in V6 > 0.24, acute pericarditis is amplitude in V6 > 0.24, acute pericarditis is almost always present.almost always present.
The EKG changes have 4 phases during the The EKG changes have 4 phases during the course of illnesscourse of illness

EKG StagesEKG Stages Stage IStage I
first few days first few days 2 weeks 2 weeks ST elevation, PR depressionST elevation, PR depression up to 50% of pt with symptoms / rub do NOT have or evolve into stage I up to 50% of pt with symptoms / rub do NOT have or evolve into stage I
Stage IIStage II last days last days weeks weeks Normalization of ST and PR segmentsNormalization of ST and PR segments ST returns to baseline, flat T wavesST returns to baseline, flat T waves
Stage IIIStage III after 2-3 weeks, lasts several weeksafter 2-3 weeks, lasts several weeks Widespread T wave inversionWidespread T wave inversion
Stage IVStage IV lasts up to several monthslasts up to several months gradual resolution of T wave changesgradual resolution of T wave changes

Acute pericarditis – Stage IAcute pericarditis – Stage I

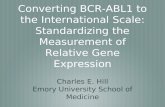
Pericarditis-Stage IIPericarditis-Stage II
60 y/o man with acute pericarditis on presentation and after 1 month of resolution of symptoms

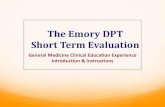
Pericarditis-Stage IIIPericarditis-Stage III
T wave inversions

Differential DiagnosesDifferential Diagnoses
ClinicalClinical
Myocardial InfarctionMyocardial Infarction MyocarditisMyocarditis Pulmonary embolismPulmonary embolism PneumothoraxPneumothorax PneumopericardiumPneumopericardium MusculoskeletalMusculoskeletal
EKG (ST elev)EKG (ST elev)
AMIAMI Early RepolarizationEarly Repolarization MyocarditisMyocarditis HyperkalemiaHyperkalemia Ventricular AneurysmVentricular Aneurysm Normal VariantNormal Variant

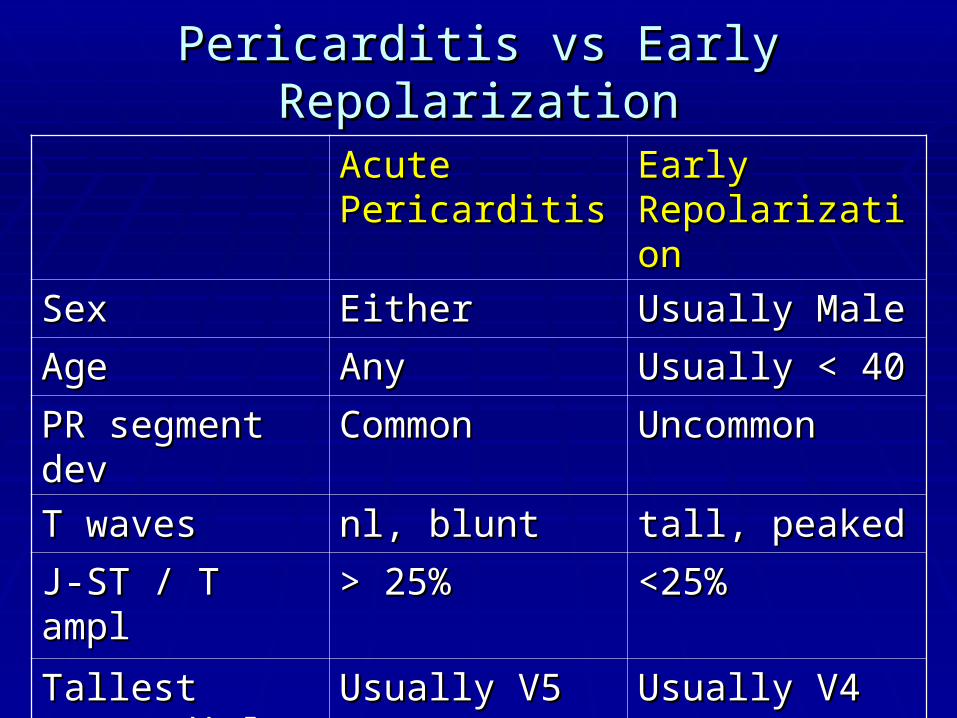
Pericarditis vs Early RepolarizationPericarditis vs Early Repolarization
Acute Acute PericarditisPericarditis
Early Early RepolarizationRepolarization
SexSex EitherEither Usually MaleUsually Male
AgeAge AnyAny Usually < 40Usually < 40
PR segment devPR segment dev CommonCommon UncommonUncommon
T wavesT waves nl, bluntnl, blunt tall, peakedtall, peaked
J-ST / T amplJ-ST / T ampl > 25%> 25% <25%<25%
Tallest Tallest precordial Rprecordial R
Usually V5Usually V5 Usually V4Usually V4

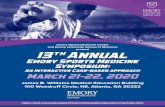
Early Repolarization
J point and ST segment elevation is most prominent in V4 to V6. The ST segment maintains its normal configuration and is slightly concave
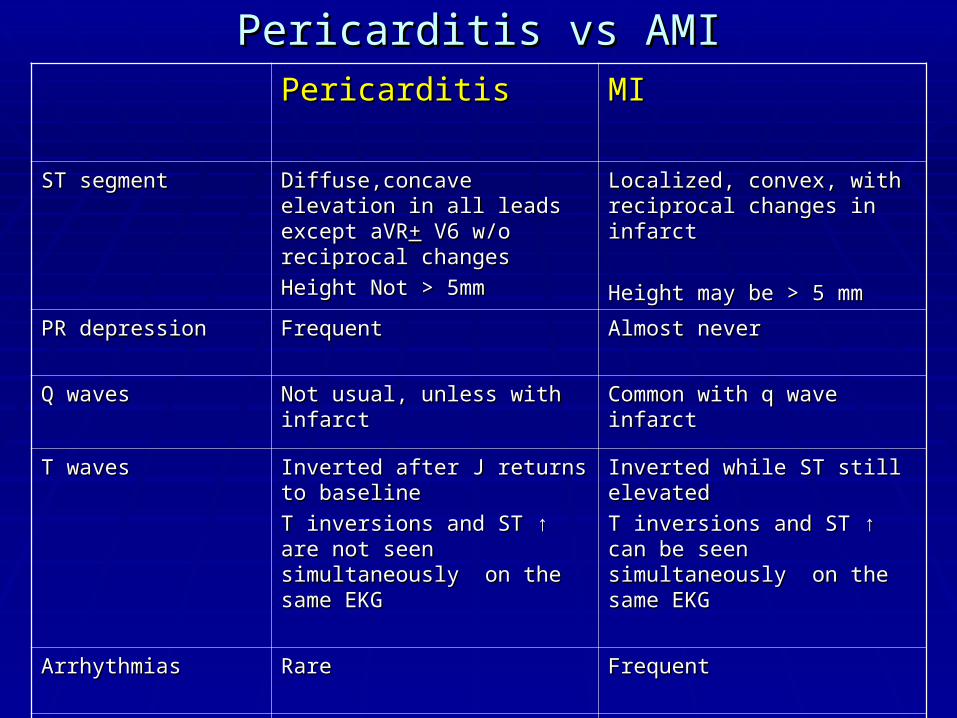
Pericarditis vs AMIPericarditis vs AMIPericarditisPericarditis MIMI
ST segmentST segment Diffuse,concave elevation in all Diffuse,concave elevation in all leads except aVRleads except aVR++ V6 w/o V6 w/o reciprocal changesreciprocal changes
Height Not > 5mmHeight Not > 5mm
Localized, convex, with Localized, convex, with reciprocal changes in infarctreciprocal changes in infarct
Height may be > 5 mmHeight may be > 5 mm
PR depressionPR depression FrequentFrequent Almost neverAlmost never
Q wavesQ waves Not usual, unless with infarctNot usual, unless with infarct Common with q wave infarctCommon with q wave infarct
T wavesT waves Inverted after J returns to Inverted after J returns to baselinebaseline
T inversions and ST T inversions and ST ↑ are not ↑ are not seen simultaneously on the seen simultaneously on the same EKG same EKG
Inverted while ST still elevatedInverted while ST still elevated
T inversions and ST T inversions and ST ↑ can be ↑ can be seen simultaneously on the seen simultaneously on the same EKG same EKG
ArrhythmiasArrhythmias RareRare FrequentFrequent
Conduction Conduction disturbancesdisturbances
RareRare frequentfrequent

Acute Anterior MIAcute Anterior MI

Laboratory testingLaboratory testing
Laboratory abnormalitiesLaboratory abnormalities CBC – very high WBC (purulent pericarditis)CBC – very high WBC (purulent pericarditis) ↑↑ESR ESR Chem-7 (uremic etiology)Chem-7 (uremic etiology) ↑↑CRPCRP HIV in selected casesHIV in selected cases ANAANA Rheumatoid factorRheumatoid factor Blood cultures if febrileBlood cultures if febrile Viral cultures and antibody testing not indicatedViral cultures and antibody testing not indicated
Cardiac Isoenzymes - ? helpfulCardiac Isoenzymes - ? helpful
MB fraction of CK and Troponin I are modestly elevatedMB fraction of CK and Troponin I are modestly elevated The rise in TnI is related to the extent of myocardial The rise in TnI is related to the extent of myocardial
inflammation.inflammation. Features associated with a rise in Tn I are younger age,male Features associated with a rise in Tn I are younger age,male
gender,presence of effusion and a recent infectiongender,presence of effusion and a recent infection Enzyme rise is transient,resolving within the first week, Enzyme rise is transient,resolving within the first week,
persistent persistent ↑ suggest myopericarditis↑ suggest myopericarditis Not reliable to differentiate MI vs pericarditisNot reliable to differentiate MI vs pericarditis
• Two studies that included 187 patients with idiopathic pericarditis ,TnI was detectable in 32-49% and in 8-22% it was >1.5 mcg/ml
• Another 2 year ER based study-Another 2 year ER based study-Out of 14 pts with 2/3 findings (typical CP, rub, and ECG changes)Out of 14 pts with 2/3 findings (typical CP, rub, and ECG changes) 71% had elevated Tn I with negative CAD workup71% had elevated Tn I with negative CAD workup

Other StudiesOther Studies
Tuberculin skin testingTuberculin skin testing EchocardiogramEchocardiogram
Normal unless there is an effusionNormal unless there is an effusion Presence of effusion supports the diagnosis, but absence Presence of effusion supports the diagnosis, but absence
does not exclude it.does not exclude it. The ACC/AHA/ASE all recommend to obtain an echo The ACC/AHA/ASE all recommend to obtain an echo
in any suspected pericardial diseasein any suspected pericardial disease
Chest X-rayChest X-ray Recommended in all casesRecommended in all cases Typically normal Typically normal Enlarged cardiac silhouette in effusion (with clear lung Enlarged cardiac silhouette in effusion (with clear lung
fields)fields)

Need for hospitalizationNeed for hospitalization Many physicians tend to admit them, but this may not be Many physicians tend to admit them, but this may not be
necessary. necessary. Uncomplicated acute pericarditis can undergo initial Uncomplicated acute pericarditis can undergo initial
evaluation in a same day hospital facility or clinic, with an evaluation in a same day hospital facility or clinic, with an outpatient follow-up outpatient follow-up
Features of high risk include:Features of high risk include: Subacute symptoms (eg, developing over several days or weeks) Subacute symptoms (eg, developing over several days or weeks) High fever (>38ºC [100.4ºF]) and leukocytosis High fever (>38ºC [100.4ºF]) and leukocytosis Evidence suggesting cardiac tamponade Evidence suggesting cardiac tamponade A large pericardial effusion A large pericardial effusion Immunosuppressed state Immunosuppressed state A history of oral anticoagulant therapy A history of oral anticoagulant therapy Acute trauma Acute trauma Failure to respond within seven days to NSAID therapy, a Failure to respond within seven days to NSAID therapy, a
generous allocation of time generous allocation of time Elevated cardiac troponin, suggestive of myopericarditisElevated cardiac troponin, suggestive of myopericarditis

ComplicationsComplications
Pericardial Effusion/ TamponadePericardial Effusion/ Tamponade Constrictive PericarditisConstrictive Pericarditis
can be “transient” – 10% may have transient can be “transient” – 10% may have transient within 1within 1stst month, resolves by 3 months month, resolves by 3 months
Recurrent Pericarditis (15-32%)Recurrent Pericarditis (15-32%) Recurrent sx after the initiating event is no longer Recurrent sx after the initiating event is no longer
activeactive Most likely an autoimmune etiologyMost likely an autoimmune etiology Rx : NSAIDS/ Colchicine +/- steroidsRx : NSAIDS/ Colchicine +/- steroids

TreatmentTreatment
Goals of acute therapy:Goals of acute therapy: Relieve PainRelieve Pain Treat the inflammationTreat the inflammation Prevent Cardiac tamponadePrevent Cardiac tamponade
Most viral infections are self-limitedMost viral infections are self-limited Treat the underlying disease processTreat the underlying disease process Drain purulent effusionsDrain purulent effusions Symptomatic therapySymptomatic therapy None of the treatments unfortunately, have not been None of the treatments unfortunately, have not been
proven to prevent the complications.proven to prevent the complications.

NSAIDsNSAIDs May require weeks to months of treatment with high doses of May require weeks to months of treatment with high doses of
NSAIDsNSAIDs The choice is usually empiric, based on the physician’s The choice is usually empiric, based on the physician’s
familiarity with the agent and/or its availability.familiarity with the agent and/or its availability. Rapidly titrate the dose within 1–2 days to achieve maximum Rapidly titrate the dose within 1–2 days to achieve maximum
symptomatic relief symptomatic relief Evaluate for a response within 1–2 wks,Sx usually subside in a Evaluate for a response within 1–2 wks,Sx usually subside in a
week.week.
If adequate clinical response,continue NSAIDs for 1 wk after If adequate clinical response,continue NSAIDs for 1 wk after
complete resolution of Sx and then taper in 2–3 dayscomplete resolution of Sx and then taper in 2–3 days. .

AspirinAspirin 2-6 gm daily2-6 gm daily650mg Q3-4 hrs650mg Q3-4 hrs Preferred in patients with CADPreferred in patients with CAD
IbuprofenIbuprofen 1600-3200 mg daily1600-3200 mg daily400-800 mg q 6-8 hrs400-800 mg q 6-8 hrs above average response rate and has a very good side above average response rate and has a very good side
effect profileeffect profile IndomethacinIndomethacin
75-225 mg daily75-225 mg daily Try to avoid, unless absolutely needed as it can Try to avoid, unless absolutely needed as it can ↓ ↓
coronary blood flow.coronary blood flow.
Nonsteroidal Anti-inflammatory Drugs in the Treatment of Pericarditis: Clinical ReviewSCHIFFERDECKER, BRANISLAV MD; SPODICK, DAVID H. MD, DScCardiology Review ; Volume 11(4), July/August 2003, pp 211-217
NSAIDs

ColchicineColchicine
A prospective, randomized, open-label design was used.A prospective, randomized, open-label design was used. 120 patients with a first episode of acute pericarditis 120 patients with a first episode of acute pericarditis
were randomly assigned to were randomly assigned to conventional treatment with aspirin (group I) or conventional treatment with aspirin (group I) or conventional treatment plus colchicine 1.0 to 2.0 mg for the first day and conventional treatment plus colchicine 1.0 to 2.0 mg for the first day and
then 0.5 to 1.0 mg/d for 3 months (group II). then 0.5 to 1.0 mg/d for 3 months (group II). Colchicine significantly reduced the recurrence rate (10.7% vs 32.3%; Colchicine significantly reduced the recurrence rate (10.7% vs 32.3%;
PP=0.004;) and presence of symptoms at 72 hours (11.7% vs 36.7%; =0.004;) and presence of symptoms at 72 hours (11.7% vs 36.7%; PP=0.003). =0.003).
Based upon this, addition of it to the Rx regimen for an initial episode of Based upon this, addition of it to the Rx regimen for an initial episode of acute pericarditis is an option for physicians.acute pericarditis is an option for physicians.
Colchicine in Addition to Conventional Therapy for Acute Pericarditis Results of the COlchicine for acute PEricarditis (COPE) Trial Circulation. 2005;112:2012-2016 10.1161/CIRCULATIONAHA.105.542738eeeeew
SteroidsSteroids
In patients refractory to NSAIDs and colchicineIn patients refractory to NSAIDs and colchicine Steroid therapy with initial episode is more likely Steroid therapy with initial episode is more likely
associated with recurrent episodes. associated with recurrent episodes. Evidence available argues against the routine Evidence available argues against the routine
administration of corticosteroids during a first administration of corticosteroids during a first episode of acute pericarditis episode of acute pericarditis
Specific conditions that will benefit:Specific conditions that will benefit: Acute pericarditis due to connective tissue diseasesAcute pericarditis due to connective tissue diseases Auto-immune pericarditisAuto-immune pericarditis Uremic pericarditisUremic pericarditis
Myocardial Infarction-Associated PericarditisMyocardial Infarction-Associated Pericarditis
Early post MI pericarditis is a consequence of transmural Early post MI pericarditis is a consequence of transmural infarction.infarction.
Aspirin is the drug of choice in this setting. (650 mg Aspirin is the drug of choice in this setting. (650 mg Q4h) Q4h)
Late MI associated pericarditis (Dressler syndrome), occurs Late MI associated pericarditis (Dressler syndrome), occurs days to months after infarction, days to months after infarction,
Autoimmune in etiology.Autoimmune in etiology. NSAIDs are the treatment of choice. NSAIDs are the treatment of choice. Colchicine seems to be the most effective if NSAIDs failColchicine seems to be the most effective if NSAIDs fail Corticosteroids seem to provide symptomatic benefit but do not Corticosteroids seem to provide symptomatic benefit but do not
prevent recurrence. prevent recurrence. Pericardiectomy is only rarely curative Pericardiectomy is only rarely curative

SummarySummary
Etiology of Acute PericarditisEtiology of Acute Pericarditis Clinical Presentation and EKG findingsClinical Presentation and EKG findings Differential DiagnosisDifferential Diagnosis EvaluationEvaluation TreatmentTreatment