
Acute Pelvic Pain
21
Christopher R. Graber, MD Salina Women’s Clinic 15 April 2011
-
Upload
veronica-whitehead -
Category
Documents
-
view
159 -
download
12
description
Acute Pelvic Pain. Christopher R. Graber, MD Salina Women’s Clinic 15 April 2011. Overview. Definitions and Symptoms Acute OB/Gyn Pain Complication of pregnancy Acute infection Adnexal disorders Other GI, GU, Musculoskeletal, other. Definitions. Acute pain - PowerPoint PPT Presentation
Transcript of Acute Pelvic Pain
Christopher R. Graber, MDSalina Women’s Clinic
15 April 2011
Definitions and Symptoms Acute OB/Gyn Pain
• Complication of pregnancy• Acute infection• Adnexal disorders
Other• GI, GU, Musculoskeletal, other
Acute pain• Sudden onset, sharp rise, short course
Cyclic pain• Definite association with mestrual cycle• Dysmenorrhea – painful menstruation
Primary or secondary Chronic pelvie pain
• Greater than 6 months duration
Rapid onset• Perforation of hollow viscus or ischemia
Colic or severe cramps• Muscular contraction, obstruction of hollow
viscus such as uterus or intestines Entire abdomen
• Generalized reaction to irritating fluid within the peritoneal cavity
Complications of pregnancy• Ectopic, abortion, leiomyoma degeneration
Acute infections• Endometritis, PID, TOA
Adnexal disorders• Hemorrhagic functional cyst, ovarian
torsion, torsion of paratubal cyst• Ruptured cyst – functional or neoplastic
Ectopic pregnancy – implantation in a site other than the uterus (95% in tube)• Acute pain due to tubal dilation• If rupture localized changes to generalized
peritonitis (due to hemoperitoneum)• hCG less than expected or abnormal rise• Use ultrasound to locate pregnancy
Heterotopic pregnancy rare (both uterine and ectopic)
Treatment• Methotrexate
50 mg/m2 IM x1 Multiple-dose regimen an alternative
• Surgery Linear salpingostomy Partial salpingectomy
• Follow quant hCG if no fetal tissue recovered MTX: quant on days 4 and 7, expect 15% drop
Absolute contraindications• Breastfeeding, immunodeficiency• Chronic liver disease, active pulmonary disease• Leukopenia, thrombocytopenia, anemia• Peptic ulcer disease, renal dysfunction• Known sensitivity to methotrexate
Relative contraindications• Gestational sac >3.5 cm, embryo cardiac
motion• Elevated hCG quant
Abortion (loss of pregnancy <20w)• Threatened – any vaginal bleeding• Inevitable – bleeding plus dilation• Complete – spontaneous expulsion• Incomplete – passage of some tissue• Missed – no expulsion of tissue for 8w• Induced – medical or surgical
Degeneration of leiomyoma• Rapid growth during pregnancy, outgrowing
blood supply• If pedunculated, can cause torsion• Increased progesterone• Degeneration sometimes seen on imaging• Supportive care unless torsion or not
pregnant
Complications of pregnancy• Ectopic, abortion, leiomyoma degeneration
Acute infections• Endometritis, PID, TOA
Adnexal disorders• Hemorrhagic functional cyst, ovarian
torsion, torsion of paratubal cyst• Ruptured cyst – functional or neoplastic
Endometritis (postpartum uterine infection)• Fever, abdominal pain, leukocytosis• Vaginal delivery
Overall risk 1%, increased after prolonged labor or rupture of membranes
13 % risk if chorioamnionitis during labor• Cesarean delivery
Decreased by single-dose pre-op abx Increased risk with manual extraction of placenta
• Treatment – Abx: amp, gent, clinda
Pelvic inflammatory disease• Acute salpingo-oophoritis• Pain, fever, purulent vaginal/cervical
discharge• Cervical motion tenderness, adnexal
tenderness• Outpatient vs. inpatient mgmt
Inpatient if: acute abdomen, pregnancy, vomiting, no response to PO abx, TOA
• http://www.cdc.gov/std/treatment/2010/STD-Treatment-2010-RR5912.pdf
Tuboovarian abscess (TOA)• Sequela to PID• May be palpated on exam, seen on imaging• Treatment with IV abx• Exploratory surgery may be needed,
especially if rupture occurs
Complications of pregnancy• Ectopic, abortion, leiomyoma degeneration
Acute infections• Endometritis, PID, TOA
Adnexal disorders• Hemorrhagic functional cyst, ovarian
torsion, torsion of paratubal cyst• Ruptured cyst – functional or neoplastic
An ovarian cyst that is not torsing, rapidly expanding, infected, or leaking does not cuase acute pain
Ovarian cysts – leaking, hemorrhagic• May be mittleschmertz• Similar symptoms as a ruptured ectopic
Increasing abd pain, dizziness if hemoperitoneum
May be a surgical abdomen• Diagnosis: hCG, CBC, ultrasound• Treatment: supportive or surgical
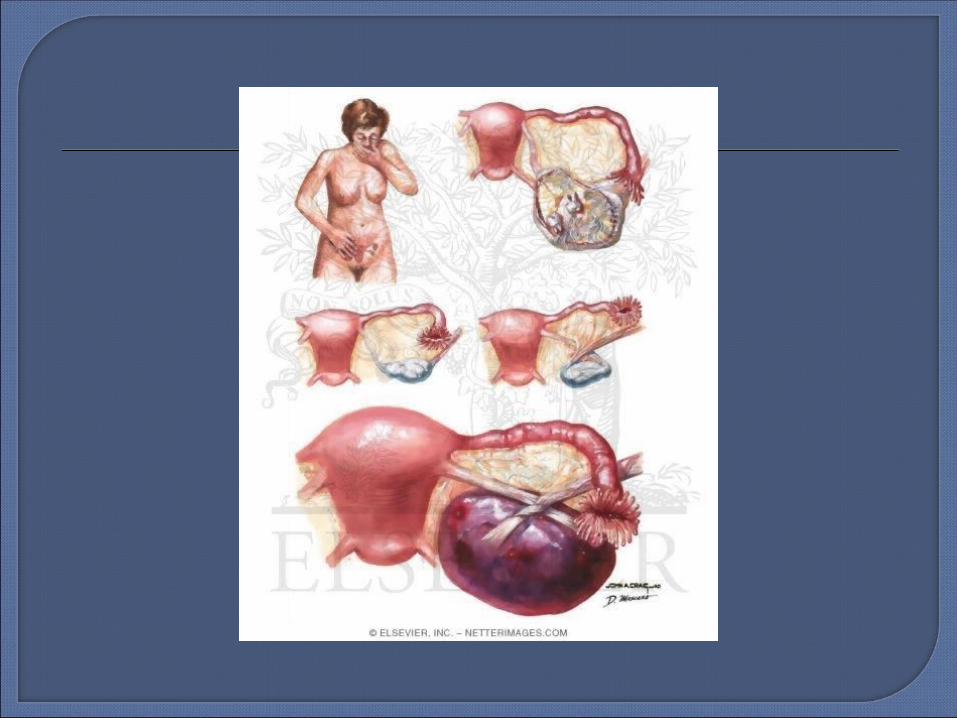
Adnexal torsion• Ischemia from twisting of the vascular
pedicle of an ovary, tube, or paratubal cyst• May be constant or intermittent pain• Onset may coincide with physical activity• Diagnosis – sono: rapidly increasing mass• Treatment – surgery, with possible removal• Benign cystic teratoma is most common
neoplasm to undergo torsion
GI• Gastroenteritis, appendicitis (can be similar
to PID), bowel obstruction, diverticulitis, IBS GU
• Cystitis, pylonephritis, ureteral lithiasis Musculoskeletal
• Abdominal wall hematoma, hernia Other
• Acute porphyria, pelvic thrombophlebitis, aneurysm, abdominal angina

Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2010. MMWR 2010;59.
Comprehensive Gynecology. Stenchever MA editor. Mosby Inc., St. Louis, MO. 2001.
Novak’s Gynecology – 13th edition. Berek JS editor. Lippincott, Williams, and Wilkins, Philadelphia, PA. 2002.
Williams Obstetrics – 22nd edition. Cunningham FG editor. McGraw-Hill, New York, NY. 2005.


















